Amaranth Oil Increases Total and LDL Cholesterol Levels without Influencing Early Markers of Atherosclerosis in an Overweight and Obese Population: A Randomized Double-Blind Cross-Over Study in Comparison with Rapeseed Oil Supplementation

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
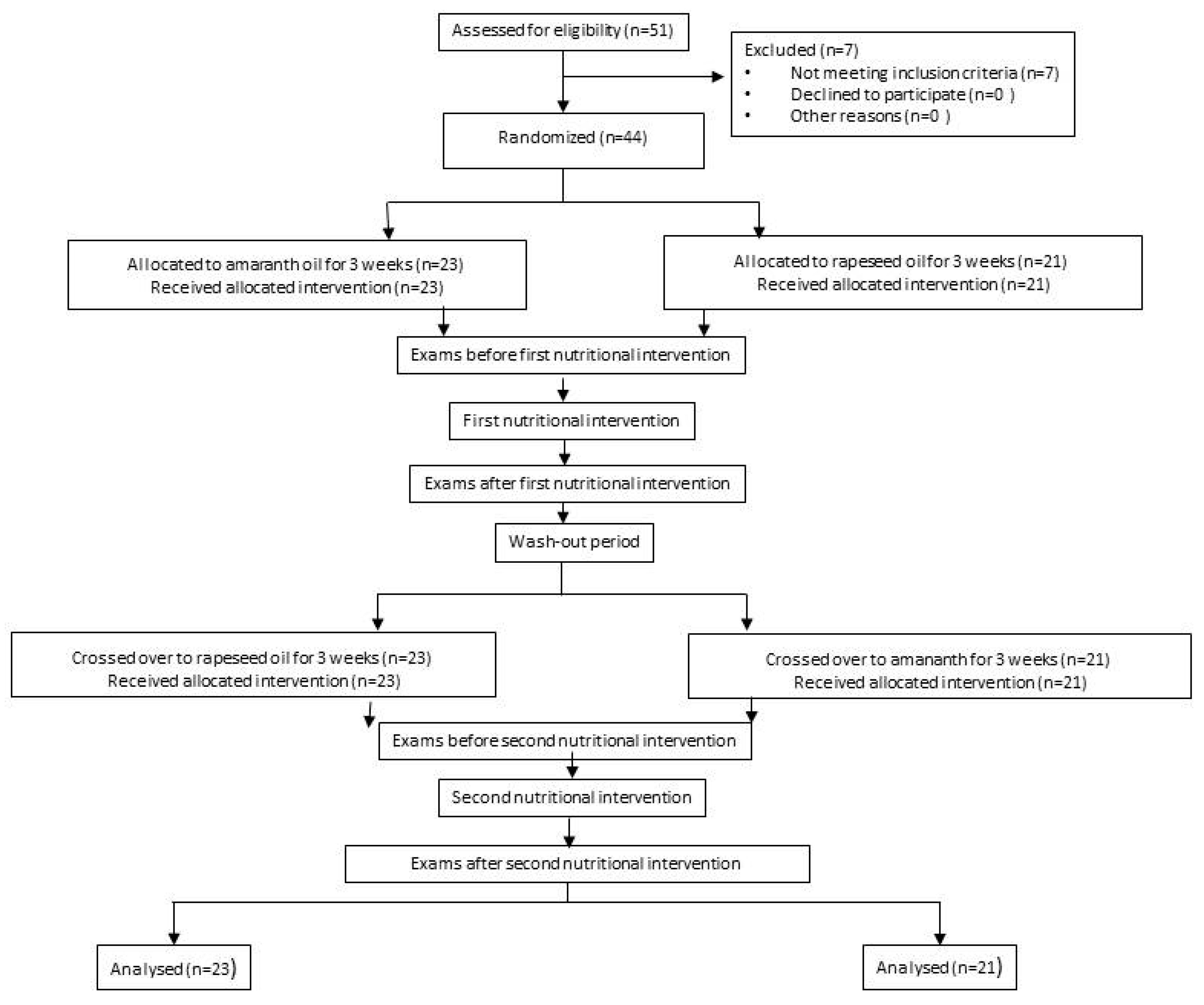
2.2. Study Design
2.3. Biochemical Analysis
2.4. Statistics
3. Results
3.1. Anthropometric Parameters
3.2. Biochemical Parameters
3.2.1. hsCRP
3.2.2. Novel Markers of AT
3.2.3. Lipid Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. Pharmacoeconomics 2015, 33, 673–689. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.A.; Singh, G.M.; Lu, Y.; Danaei, G.; Lin, J.K.; Finucane, M.M.; Bahalim, A.N.; McIntire, R.K.; Gutierrez, H.R.; Cowan, M.; et al. National, regional, and global trends in adult overweight and obesity prevalences. Popul. Health Metr. 2012, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Watanabe, T. Inflammatory reactions in the pathogenesis of atherosclerosis. J. Atheroscler. Thromb. 2003, 10, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Cybulsky, M.I.; Gimbrone, M.A. Endothelial expression of a mononuclear leukocyte adhesion molecule during atherogenesis. Science 1991, 251, 788–791. [Google Scholar] [CrossRef] [PubMed]
- Nie, Q.; Fan, J.; Haraoka, S.; Shimokama, T.; Watanabe, T. Inhibition of mononuclear cell recruitment in aortic intima by treatment with anti-ICAM-1 and anti-LFA-1 monoclonal antibodies in hypercholesterolemic rats: Implications of the ICAM-1 and LFA-1 pathway in atherogenesis. Lab. Investig. 1997, 77, 469–482. [Google Scholar] [PubMed]
- Dong, Z.M.; Chapman, S.M.; Brown, A.A.; Frenette, P.S.; Hynes, R.O.; Wagner, D.D. The combined role of P- and E-selectins in atherosclerosis. J. Clin. Investig. 1998, 102, 145–152. [Google Scholar] [CrossRef]
- Nakashima, Y.; Raines, E.W.; Plump, A.S.; Breslow, J.L.; Ross, R. Upregulation of VCAM-1 and ICAM-1 at atherosclerosis-prone sites on the endothelium in the ApoE-deficient mouse. Arter. Thromb. Vasc. Biol. 1998, 18, 842–851. [Google Scholar] [CrossRef]
- Johnson, J.L.; Newby, A.C. Macrophage heterogeneity in atherosclerotic plaques. Curr. Opin. Lipidol. 2009, 20, 370–378. [Google Scholar] [CrossRef]
- Fruchart, J.-C.; Nierman, M.C.; Stroes, E.S.G.; Kastelein, J.J.P.; Duriez, P. New risk factors for atherosclerosis and patient risk assessment. Circulation 2004, 109, III15–III19. [Google Scholar] [CrossRef]
- Mao, Y.; Qi, X.; Xu, W.; Song, H.; Xu, M.; Ma, W.; Zhou, L. Serum gamma-glutamyl transferase: A novel biomarker for coronary artery disease. Med. Sci. Monit. 2014, 20, 706–710. [Google Scholar]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef] [PubMed]
- De Gennaro Colonna, V.; Bianchi, M.; Pascale, V.; Ferrario, P.; Morelli, F.; Pascale, W.; Tomasoni, L.; Turiel, M. Asymmetric dimethylarginine (ADMA): An endogenous inhibitor of nitric oxide synthase and a novel cardiovascular risk molecule. Med. Sci. Monit. 2009, 15, RA91–RA101. [Google Scholar] [PubMed]
- Lau, D.C.W.; Dhillon, B.; Yan, H.; Szmitko, P.E.; Verma, S. Adipokines: Molecular links between obesity and atheroslcerosis. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, H2031–H2041. [Google Scholar] [CrossRef] [PubMed]
- Boden, W.E. High-density lipoprotein cholesterol as an independent risk factor in cardiovascular disease: Assessing the data from Framingham to the Veterans Affairs High-Density Lipoprotein Intervention Trial. Am. J. Cardiol. 2000, 86, 19L–22L. [Google Scholar] [CrossRef]
- Kaźmierczak, A.; Bolesławska, I.; Przysławski, J. Amaranth—Its use in the prevention and treatment of certain civilization-related diseases. Now. Lek. 2011, 80, 192–198. [Google Scholar]
- Bălăşoiu, M.; Bălăşoiu, A.T.; Stepan, A.E.; Dinescu, S.N.; Avrămescu, C.S.; Dumitrescu, D.; Cernea, D.; Alexandru, D. Proatherogenic adipocytokines levels in metabolic syndrome. Rom. J. Morphol. Embryol. 2014, 55, 29–33. [Google Scholar]
- Spilioti, E.; Holmbom, B.; Papavassiliou, A.G.; Moutsatsou, P. Lignans 7-hydroxymatairesinol and 7-hydroxymatairesinol 2 exhibit anti-inflammatory activity in human aortic endothelial cells. Mol. Nutr. Food Res. 2014, 58, 749–759. [Google Scholar] [CrossRef]
- Kabiri, N.; Asgary, S.; Setorki, M. Lipid lowering by hydroalcoholic extracts of Amaranthus caudatus L. induces regression of rabbits atherosclerotic lesions. Lipids Health Dis. 2011, 10, 89. [Google Scholar] [CrossRef]
- Antoniades, C.; Shirodaria, C.; Leeson, P.; Antonopoulos, A.; Warrick, N.; Van-Assche, T.; Cunnington, C.; Tousoulis, D.; Pillai, R.; Ratnatunga, C.; et al. Association of plasma asymmetrical dimethylarginine (ADMA) with elevated vascular superoxide production and endothelial nitric oxide synthase uncoupling: Implications for endothelial function in human atherosclerosis. Eur. Heart J. 2009, 30, 1142–1150. [Google Scholar] [CrossRef]
- Mels, C.M.C.; Schutte, A.E.; Huisman, H.W.; Smith, W.; Kruger, R.; van Rooyen, J.M.; Schwedhelm, E.; Atzler, D.; Böger, R.H.; Malan, N.T.; et al. Asymmetric dimethylarginine and symmetric dimethylarginine prospectively relates to carotid wall thickening in black men: The SABPA study. Amino Acids 2017, 49, 1843–1853. [Google Scholar] [CrossRef]
- Böger, R.H. Asymmetric dimethylarginine (ADMA): A novel risk marker in cardiovascular medicine and beyond. Ann. Med. 2006, 38, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, A.; Sarojini, G.; Devi, N.L. Hypocholesterolemic effect of amaranth seeds (Amaranthus esculantus). Plant. Foods Hum. Nutr. 1993, 44, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.A.; Lehmann, J.W.; Peterson, D.M. Amaranth and its oil inhibit cholesterol biosynthesis in 6-week-old female chickens. J. Nutr. 1996, 126, 1972–1978. [Google Scholar] [PubMed]
- Berger, A.; Gremaud, G.; Baumgartner, M.; Rein, D.; Monnard, I.; Kratky, E.; Geiger, W.; Burri, J.; Dionisi, F.; Allan, M.; et al. Cholesterol-lowering properties of amaranth grain and oil in hamsters. Int. J. Vitam. Nutr. Res. 2003, 73, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Martirosyan, D.M.; Miroshnichenko, L.A.; Kulakova, S.N.; Pogojeva, A.V.; Zoloedov, V.I. Amaranth oil application for coronary heart disease and hypertension. Lipids Health Dis. 2007, 6, 1. [Google Scholar] [CrossRef][Green Version]
- De Castro, L.I.A.; Soares, R.A.M.; Saldiva, P.H.N.; Ferrari, R.A.; Miguel, A.M.R.O.; Almeida, C.A.S.; Arêas, J.A.G. Amaranth oil increased fecal excretion of bile Acid but had no effect in reducing plasma cholesterol in hamsters. Lipids 2013, 48, 609–618. [Google Scholar] [CrossRef]
- Miettinen, T.A.; Vanhanen, H. Serum concentration and metabolism of cholesterol during rapeseed oil and squalene feeding. Am. J. Clin. Nutr. 1994, 59, 356–363. [Google Scholar] [CrossRef]
- Fattore, E.; Fanelli, R. Palm oil and palmitic acid: A review on cardiovascular effects and carcinogenicity. Int. J. Food Sci. Nutr. 2013, 64, 648–659. [Google Scholar] [CrossRef]
- Clandinin, M.T.; Cook, S.L.; Konard, S.D.; French, M.A. The effect of palmitic acid on lipoprotein cholesterol levels. Int. J. Food Sci. Nutr. 2000, 51, S61–S71. [Google Scholar] [CrossRef]
- Fernández-Macías, J.C.; Ochoa-Martínez, A.C.; Varela-Silva, J.A.; Pérez-Maldonado, I.N. Atherogenic Index of Plasma: Novel Predictive Biomarker for Cardiovascular Illnesses. Arch. Med. Res. 2019, 50, 285–294. [Google Scholar] [CrossRef]
- Dobiásová, M. AIP–atherogenic index of plasma as a significant predictor of cardiovascular risk: From research to practice. Vnitr. Lek. 2006, 52, 64–71. [Google Scholar] [PubMed]
- Edwards, M.K.; Blaha, M.J.; Loprinzi, P.D. Atherogenic Index of Plasma and Triglyceride/High-Density Lipoprotein Cholesterol Ratio Predict Mortality Risk Better Than Individual Cholesterol Risk Factors, Among an Older Adult Population. Mayo Clin. Proc. 2017, 92, 680–681. [Google Scholar] [CrossRef] [PubMed]
- Lankinen, M.A.; Fauland, A.; Shimizu, B.-I.; Ågren, J.; Wheelock, C.E.; Laakso, M.; Schwab, U.; Pihlajamäki, J. Inflammatory response to dietary linoleic acid depends on FADS1 genotype. Am. J. Clin. Nutr. 2019, 109, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Duś-Żuchowska, M.; Bajerska, J.; Krzyżanowska, P.; Chmurzyńska, A.; Miśkiewicz-Chotnicka, A.; Muzsik, A.; Walkowiak, J. The Central European diet as an alternative to the Mediterranean diet in atherosclerosis prevention in postmenopausal obese women with a high risk of metabolic syndrome-a randomized nutrition-al trial. Acta Sci. Pol. Technol. Aliment. 2018, 17, 399–407. [Google Scholar] [PubMed]
- Sarker, U.; Oba, S. Drought stress enhances nutritional and bioactive compounds, phenolic acids and antioxidant capacity of Amaranthus leafy vegetable. BMC Plant. Biol. 2018, 18, 258. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Mean ± SD | Median (1st–3rd Quartile) | |
|---|---|---|
| Age (years) | 48.77 ± 10.21 | 49.00 (42.00; 56.25) |
| Height (cm) | 168.0 ± 8.6 | 168.3 (160.0; 174.0) |
| BW (kg) | 87.7 ± 15.1 | 89.8 (73.4; 100.3) |
| WC (cm) | 99.2 ± 13.3 | 99.0 (90.8;108.0) |
| WHR | 0.89 ± 0.08 | 0.91 (0.83; 0.95) |
| BMI (kg/m2) | 31.00 ± 4.61 | 30.60 (27.44; 33.16) |
| hsCRP (mg/dL) | 4.59 ± 5.64 | 2.20 (0.98; 4.90) |
| ADMA (nmol/L) | 1.36 ± 1.15 | 0.84 (0.64; 1.69) |
| sVCAM (ng/mL) | 851.49 ± 199.47 | 776.80 (724.43; 974.53) |
| sP-selectin (ng/mL) | 127.66 ± 29.17 | 125.00 (11.53; 145.42) |
| TC (mg/dL) | 223.02 ± 37.17 | 219.00 (196.00; 234.50) |
| LDL (mg/dL) | 135.62 ± 37.99 | 125.65 (113.28; 153.00) |
| HDL (mg/dL) | 56.43 ± 15.87 | 53.00 (43.00; 66.25) |
| TG (mg/dL) | 150.16 ± 70.08 | 129.50 (113.25; 189.25) |
| AIP | 0.04 ± 0.28 | 0.07 (−0.17; 0.22) |
| Analyzed Basic Nutrients | Patients (n = 44) | |
|---|---|---|
| Mean ± SD | Median (1st–3rd Quartile) | |
| Energy [kcal] | 2153 ± 656 | 2072 (1642; 6870) |
| Energy from fats (%) | 37.6 ± 6.7 | 35.7 (32.9; 42.2) |
| Energy from protein (%) | 15.3 ± 2.4 | 15.4 (13.9; 16.7) |
| Energy from carbohydrates (%) | 47.1 ± 7.2 | 47.5 (42.2; 52.9) |
| Protein (g) | 80.2 ± 21.3 | 78.8 (64.6; 93.4) |
| Fat (g) | 89.8 ± 21.3 | 85.9 (72.5; 102.5) |
| Cholesterol (mg) | 331 ± 128 | 316 (235; 391) |
| SFA (g) | 28.8 ± 11.9 | 27.1 (20.6; 35.1) |
| MUFA (g) | 38.7 ± 13.5 | 37.1 (31.2; 43.3) |
| PUFA (g) | 15.9 ± 4.6 | 15.1 (12.9; 19.0) |
| Carbohydrates (g) | 262.6 ± 81.6 | 259.1 (197.3; 312.9) |
| Δ | AmO | RaO | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (1st–3rd Quartile) | Mean ± SD | Median (1st–3rd Quartile) | ||
| BW (kg) | −0.2 ± 1.3 | −0.1 (−0.7; 0.5) | 0.0 ± 1.6 | 0.1 (−0.5; 0.8) | 0.274 |
| WC (cm) | −0.9 ± 3.7 | −1.0 (−4.0; 1.3) | −0.4 ± 3.1 | 0.0 (−2.0; 2.0) | 0.484 |
| WHR | 0.00 ± 0.03 | 0.00 (−0.02; 0.03) | 0.00 ± 0.03 | 0.00 (−0.03; 0.02) | 0.882 |
| BMI (kg/m2) | 0.07 ± 0.47 | −0.04 (−0.24; 0.17) | 0.01 ± 0.56 | 0.04 (−0.19; 0.27) | 0.232 |
| Δ | AmO | RaO | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (1st–3rd Quartile) | Mean ± SD | Median (1st–3rd Quartile) | ||
| hsCRP (mg/dL) | 0.18 ± 3.03 | 0.15 (−0.43; 0.75) | −0.32 ± 4.99 | 0.00 (−0.73; 1.30) | 0.554 |
| ADMA (nmol/L) | −0.01 ± 0.34 | 0.00 (−0.17; 0.10) | 0.08 ± 0.41 | 0.06 (−0.02; 0.25) | 0.135 |
| sVCAM (ng/mL) | −9.12 ± 127.94 | 4.45 (−103.78; 57.58) | −50.83 ± 128.03 | −62.95 (−112.73; 7.20) | 0.107 |
| sP-selectin (ng/mL) | −2.51 ± 19.05 | −3.2 (−17.29; 9.63) | −2.11 ± 19.78 | −5.36 (−15.30; 10.62) | 0.616 |
| Δ | AmO | RaO | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (1st–3rd Quartile) | Mean ± SD | Median (1st–3rd Quartile) | ||
| TC (mg/dL) | 5.52 ±35.61 | 11.00 (−8.25; 26.00) | −8.43 ± 17.65 | −5.00 (−20.25; 5.25) | 0.002 |
| LDL (mg/dL) | 4.43 ± 34.96 | 11.20 (−8.2; 20.7) | −7.55 ± 16.41 | −7.2 (−17.00; 4.03) | 0.002 |
| HDL (mg/dL) | 0.54 ± 6.26 | 0.50 (−3.25; 5.00) | −0.65 ± 6.81 | 0.00 (−5.00; 4.25) | 0.805 |
| TG (mg/dL) | 7.43 ± 62.96 | 0.50 (−21.25; 23.25) | 1.39 ± 51.66 | −1.00 (−28.75; 29.25) | 0.788 |
| AIP | 0.01 ± 0.15 | −0.02 (−0.09;0.08) | 0.00 ± 0.21 | −0.28 (−0.15; 0.10) | 0.427 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dus-Zuchowska, M.; Walkowiak, J.; Morawska, A.; Krzyzanowska-Jankowska, P.; Miskiewicz-Chotnicka, A.; Przyslawski, J.; Lisowska, A. Amaranth Oil Increases Total and LDL Cholesterol Levels without Influencing Early Markers of Atherosclerosis in an Overweight and Obese Population: A Randomized Double-Blind Cross-Over Study in Comparison with Rapeseed Oil Supplementation. Nutrients 2019, 11, 3069. https://doi.org/10.3390/nu11123069
Dus-Zuchowska M, Walkowiak J, Morawska A, Krzyzanowska-Jankowska P, Miskiewicz-Chotnicka A, Przyslawski J, Lisowska A. Amaranth Oil Increases Total and LDL Cholesterol Levels without Influencing Early Markers of Atherosclerosis in an Overweight and Obese Population: A Randomized Double-Blind Cross-Over Study in Comparison with Rapeseed Oil Supplementation. Nutrients. 2019; 11(12):3069. https://doi.org/10.3390/nu11123069
Chicago/Turabian StyleDus-Zuchowska, Monika, Jaroslaw Walkowiak, Anna Morawska, Patrycja Krzyzanowska-Jankowska, Anna Miskiewicz-Chotnicka, Juliusz Przyslawski, and Aleksandra Lisowska. 2019. "Amaranth Oil Increases Total and LDL Cholesterol Levels without Influencing Early Markers of Atherosclerosis in an Overweight and Obese Population: A Randomized Double-Blind Cross-Over Study in Comparison with Rapeseed Oil Supplementation" Nutrients 11, no. 12: 3069. https://doi.org/10.3390/nu11123069
APA StyleDus-Zuchowska, M., Walkowiak, J., Morawska, A., Krzyzanowska-Jankowska, P., Miskiewicz-Chotnicka, A., Przyslawski, J., & Lisowska, A. (2019). Amaranth Oil Increases Total and LDL Cholesterol Levels without Influencing Early Markers of Atherosclerosis in an Overweight and Obese Population: A Randomized Double-Blind Cross-Over Study in Comparison with Rapeseed Oil Supplementation. Nutrients, 11(12), 3069. https://doi.org/10.3390/nu11123069