Evaluation of Dietary Approaches for the Treatment of Non-Alcoholic Fatty Liver Disease: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Eligibility and Selection Criteria
2.3. Data Abstraction and Validity Assessment
2.4. Assessment of Risk of Bias and Study Quality
2.5. Data Synthesis and Analysis
3. Results
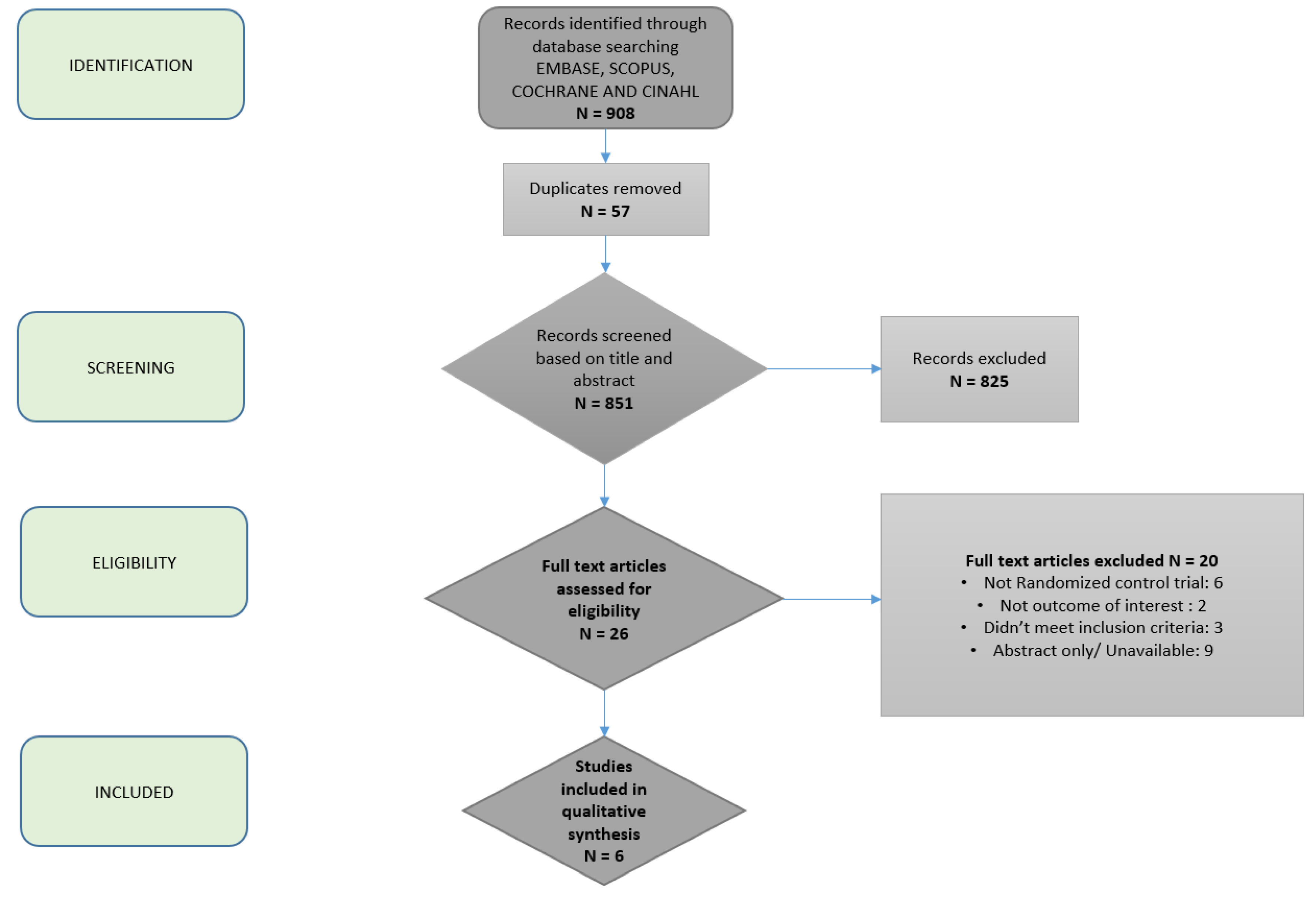
3.1. Studies Included in the Systematic Review
3.2. Characteristics of Studies
3.3. Impact of Diets on Hepatic Outcomes
3.4. Impact of Diets on Insulin Sensitivity and Lipid Profiles
3.5. Impact of Diets on Weight Loss
3.6. Quality Assessment and Risk of Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Farrell, G.C.; Larter, C.Z. Nonalcoholic fatty liver disease: From steatosis to cirrhosis. Hepatology 2006, 43 (Suppl. S1), S99–S112. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Konerman, M.A.; Jones, J.C.; Harrison, S.A. Pharmacotherapy for NASH: Current and emerging. J. Hepatol. 2018, 68, 362–375. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Gomez, E.; Martinez-Perez, Y.; Calzadilla-Bertot, L.; Torres-Gonzalez, A.; Gra-Oramas, B.; Gonzalez-Fabian, L.; Romero-Gomez, M. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology 2015, 149, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Romero-Gomez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with diet, physical activity and exercise. J. Hepatol. 2017, 67, 829–846. [Google Scholar] [CrossRef]
- Ross, R.; Dagnone, D.; Jones, P.J.; Smith, H.; Paddags, A.; Hudson, R.; Janssen, I. Reduction in obesity and related comorbid conditions after diet-induced weight loss or exercise-induced weight loss in men. A randomized, controlled trial. Ann. Intern. Med. 2000, 133, 92–103. [Google Scholar] [CrossRef]
- Noureddin, M.; Zelber-Sagi, S.; Wilkens, L.R.; Porcel, J.; Boushey, C.J.; Le Marchand, L.; Rosen, H.R.; Setiawan, V.W. Diet associations with nonalcoholic fatty liver disease in an ethnically diverse population: the Multiethnic Cohort. Hepatology 2019. Accepted Author Manuscript. [Google Scholar] [CrossRef] [PubMed]
- Zelber-Sagi, S.; Ivancovsky-Wajcman, D.; Fliss Isakov, N.; Webb, M.; Orenstein, D.; Shibolet, O.; Kariv, R. High red and processed meat consumption is associated with non-alcoholic fatty liver disease and insulin resistance. J. Hepatol. 2018, 68, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Fox, C.S.; Jacques, P.F.; Speliotes, E.K.; Hoffmann, U.; Smith, C.E.; McKeown, N.M. Sugar-sweetened beverage, diet soda, and fatty liver disease in the Framingham Heart Study cohorts. J. Hepatol. 2015, 63, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Haufe, S.; Engeli, S.; Kast, P.; Bohnke, J.; Utz, W.; Haas, V.; Sell, H. Randomized comparison of reduced fat and reduced carbohydrate hypocaloric diets on intrahepatic fat in overweight and obese human subjects. Hepatology 2011, 53, 1504–1514. [Google Scholar] [CrossRef]
- Browning, J.D.; Baker, J.A.; Rogers, T.; Davis, J.; Satapati, S.; Burgess, S.C. Short-term weight loss and hepatic triglyceride reduction: Evidence of a metabolic advantage with dietary carbohydrate restriction. Am. J. Clin. Nutr. 2011, 93, 1048–1052. [Google Scholar] [CrossRef]
- Rodriguez-Hernandez, H.; Cervantes-Huerta, M.; Rodriguez-Moran, M.; Guerrero-Romero, F. Decrease of aminotransferase levels in obese women is related to body weight reduction, irrespective of type of diet. Ann. Hepatol. 2011, 10, 486–492. [Google Scholar] [CrossRef]
- De Luis, D.A.; Aller, R.; Izaola, O.; Gonzalez Sagrado, M.; Conde, R. Effect of two different hypocaloric diets in transaminases and insulin resistance in nonalcoholic fatty liver disease and obese patients. Nutr. Hosp. 2010, 25, 730–735. [Google Scholar] [PubMed]
- Schugar, R.C.; Crawford, P.A. Low-carbohydrate ketogenic diets, glucose homeostasis, and nonalcoholic fatty liver disease. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Markova, M.; Pivovarova, O.; Hornemann, S.; Sucher, S.; Frahnow, T.; Wegner, K.; Herder, C. Isocaloric Diets High in Animal or Plant Protein Reduce Liver Fat and Inflammation in Individuals with Type 2 Diabetes. Gastroenterology 2017, 152, 571–585. [Google Scholar] [CrossRef] [PubMed]
- Arslanow, A.; Teutsch, M.; Walle, H.; Grünhage, F.; Lammert, F.; Stokes, C.S. Short-Term Hypocaloric High-Fiber and High-Protein Diet Improves Hepatic Steatosis Assessed by Controlled Attenuation Parameter. Clin. Transl. Gastroenterol. 2016, 7, e176. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; Wilson, A.M. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef]
- Nordmann, A.J.; Suter-Zimmermann, K.; Bucher, H.C.; Shai, I.; Tuttle, K.R.; Estruch, R. Meta-analysis comparing Mediterranean to low-fat diets for modification of cardiovascular risk factors. Am. J. Med. 2011, 124, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Aller, R.; Izaola, O.; de la Fuente, B.; De Luis Roman, D.A. Mediterranean Diet is Associated with Liver Histology in Patients with Non Alcoholic Fatty Liver Disease. Nutr. Hosp. 2015, 32, 2518–2524. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2016, 354, i4086. [Google Scholar]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Misciagna, G.; Del Pilar Diaz, M.; Caramia, D.V.; Bonfiglio, C.; Franco, I.; Noviello, M.R.; Caruso, M.G. Effect of a Low Glycemic Index Mediterranean Diet on Non-Alcoholic Fatty Liver Disease. A Randomized Controlled Clinici Trial. J. Nutr. Health Aging 2017, 21, 404–412. [Google Scholar] [CrossRef]
- Katsagoni, C.N.; Papatheodoridis, G.V.; Ioannidou, P.; Deutsch, M.; Alexopoulou, A.; Papadopoulos, N.; Kontogianni, M.D. Improvements in clinical characteristics of patients with non-alcoholic fatty liver disease, after an intervention based on the Mediterranean lifestyle: A randomised controlled clinical trial. Br. J. Nutr. 2018, 120, 164–175. [Google Scholar] [CrossRef]
- Abenavoli, L.; Greco, M.; Milic, N.; Accattato, F.; Foti, D.; Gulletta, E.; Luzza, F. Effect of Mediterranean Diet and Antioxidant Formulation in Non-Alcoholic Fatty Liver Disease: A Randomized Study. Nutrients 2017, 9, 870. [Google Scholar] [CrossRef]
- Properzi, C.; O’Sullivan, T.A.; Sherriff, J.L.; Ching, H.L.; Jeffrey, G.P.; Buckley, R.F.; Adams, L.A. Ad Libitum Mediterranean and Low-Fat Diets Both Significantly Reduce Hepatic Steatosis: A Randomized Controlled Trial. Hepatology 2018, 68, 1741–1754. [Google Scholar] [CrossRef]
- Johari, M.I.; Yusoff, K.; Haron, J.; Nadarajan, C.; Ibrahim, K.N.; Wong, M.S.; Ma, Z.F. A Randomised Controlled Trial on the Effectiveness and Adherence of Modified Alternate-day Calorie Restriction in Improving Activity of Non-Alcoholic Fatty Liver Disease. Sci. Rep. 2019, 9, 11232. [Google Scholar] [CrossRef]
- Dietz, W.H. The response of the US Centers for Disease Control and Prevention to the obesity epidemic. Annu. Rev. Public Health 2015, 36, 575–596. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year Country | Study Design Duration | N | Demographics Mean Age (Years), Sex | Baseline Mean BMI (kg/m2) Comorbidities | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|---|---|---|
| Ryan, 2013 Australia | Randomized, crossover 6 weeks | 12 (each was their own control) | Age: 55 ± 14 Sex: 50% female | 32.0 ± 4 | Biopsy-proven NAFLD MetSyn <7 alcoholic drinks/week for women and <10/week for men | Diabetes |
| Misciagna, 2017 Italy | Double-blind, randomized controlled trial 6 months | 98 LGMID: 50 Control: 48 | Age: 18–79 Sex: 26.5% female | Normal (n = 3 in LGMID) Overweight (n = 13 in both groups) Obese (n = 35 INRAN group, n = 34 LGIMD group) | Moderate to severe NAFLD based on US | Overt CVD or revascularization Stroke Clinical PAD Diabetes Severe medical condition that may impair participation Recent weight loss On special diet or weight-loss program Inability to follow MD |
| Katsagoni, 2018 Greece | Single-blind, randomized, controlled 6 months | 63 CG: 21 recruited, 7 dropped out MDG: 21 MLG: 21 | Age: 18–65 Sex: 31.7 % female | 25–40 | US and/or biopsy-proven NAFLD and elevated ALT and/or У-GGT | Other causes of liver disease or steatosis Weekly alcohol consumption of >210 g for men or >140 g for women -Diabetes Currently on weight-loss diet |
| Abenavoli, 2017 Italy | Randomized controlled 6 months | 50 MD: 20 MD + AO: 20 CG: 10 | Age: MD: 52 (40–60) MD+AO: 46 (40–57) Control:33 (28–40) Sex (% female): MD: 40% MD+AO: 20% Control: 40% | MD: 31 (29–33) MD+AO: 29 (28–32) Control: 29 (27–31) | Adults with NAFLD BMI > 25 kg/m2 | Hepatitis B/C Other systemic diseases (cardiac, renal, autoimmune, metabolic) Treatment with insulin Smoking Significant alcohol use Recreational drug use Exposure to liver toxins |
| Properzi, 2018 Australia | Single-blinded, randomized controlled 12 weeks | 51 MD: 26 LF: 25 | Age: MD: 51 + 13.36 LF: 53 + 9.06 Race: MD: 80.8% white LD: 84% white Sex: MD: 42% female LF: 56% female | MD: 31.5 ± 4.1 LF: 30.2 ± 5.6 For MD, LF respectively: DM (30%, 28%) HTN (34.6%, 40%) HLD (57.7%, 44%) CVD (19.2%, 12%) | NAFLD diagnosis with HS > 5.5% on MRS | Unstable body weight variation (>5% change in prior 3 months) Use of weight loss medications HbA1c > 8.5% Pioglitazone use Decompensated cirrhosis Renal failure Malignancy Atrial fibrillation Pregnancy or lactation Current smoking Significant alcohol use |
| Johari, 2019 Malaysia | Randomized, controlled 8 weeks | 43 MACR: 33 Control: 10 | Age: 45.33 ± 10.77 Sex: 23.2% female | 31.60 ± 5.19 17/33 with diabetes (equal proportions in intervention and control arms) | Ages 18–70 years BMI 17.5–40 kg/m2 Elevated ALT and AST | Other cause of liver disease Significant alcohol intake Pregnancy Active weight loss program/weight loss Medication use Substance abuse Psychiatric disease Unable to tolerate fasting |
| Author | Dietary Intervention | Adherence Assessment | Baseline Steatosis/Fibrosis | Change in Hepatic Steatosis/Fibro-sis | Changes in Body Weight (kg) or BMI (kg/m2) (Means) | Change in AST and/or ALT (IU/L) | Change in Total Cholesterol and Triglycerides (md/dl) | Change in Insulin Sensitivity (HOMA-IR) (Normal < 2) |
|---|---|---|---|---|---|---|---|---|
| Ryan | 6 weeks MD (40% mon-and omega-3 polyunsaturated fat, 40% carbohydrate, 20% protein) with 6-week washout period during crossover, followed by 6 weeks LF/HCD (30% fat, 50% carbohydrate, 20% protein); food was supplied; up to 2 alcoholic drinks 5 days per week | 7-day food diary at the beginning and end of dietary intervention | IHL% Based on H-MRS: MD: 14.2 ± 11.7 LF/HCD: 11.2 ± 4.4 | IHL% Based on H-MRS: MD: 8.6 ± 7.0 (p < 0.05) LF/HCD: 10.0 ± 3.6 (p > 0.05) | MD: Wt: 88.3 → 87.3 (p > 0.05) BMI: 31.5 → 31.2 (p > 0.05) LF/HCD: Wt: 90.7 → 80.3 (p > 0.05) BMI: 31.5 → 30.8 (p > 0.05) | No significant change in ALT with either diet | MD: TG: 224 → 201 (p > 0.05) LF/HCD: TG: 222 → 221 (p > 0.05) | MD: 4.7 → 3.0 (p < 0.01) LF/HCD: 4.1 → 3.9 (p > 0.05) |
| Misciagna * | LGIMD (n = 50) or INRAN (n = 48) | MAI based on weekly for the first month then monthly diet journal entries | Moderate to severe NAFLD based on US Moderate NAFLD: n = 34 in INRAN, n = 35 in LGIMD Severe NAFLD: n = 14 in INRAN, n = 15 in LGIMD | Significant reduction in NAFLD score based on US in both men and women in the LGIMD group until 55 years of age | Reduction in the number of obese patients in both diet groups at 6 months, but increase in number of overweight patients in both groups | Significant reduction in ALT in both groups AST normal at baseline and end of study in all patients in both groups | LGIMD: Reported as number of people with improvement TG: 11% patients levels normalized | |
| Katsa-goni | CG or MDG, or MLG; All 3 groups given energy-restriction regimen, with 45% carbohydrates, 20% protein, and 35% lipids CG: given general written dietary guidelines for healthy lifestyle MDG and MLG: 7 60-min small group dietary counseling sessions to enhance MD adherence (every 2 weeks, for first 2 months, then monthly for next 4 months) MLG: given goal of moderate-to-vigorous physical activity ≥30 min/day and 7–9 h of sleep per day | -Self-monitoring: Special forms for intervention goals or 3-day dietary records, Med. Diet Score, 69-itm FFQ and 24 h food recall at baseline and end of study MLG group given a pedometer with goal of 10,000 steps/day | MDG: TE: 6.6 kPa NFS: −2.36 MLG: TE: 7.1 kPa NFS: −2.11 | MDG: TE: 6.1 kPa (p = 0.002) NFS: -2.38 (p = 0.65) MLG: TE: 6.1 kPa (p = 0.002) NFS: −2.09 (p = 0.65) | MDG Wt loss: −5.4% loss (p = 0.01) BMI: 31.6 → 28.2 (p = 0.008) MLG: Wt loss: −6.3% (p= 0.01) BMI: 32.44 → 30.55 (p = 0.008) | MDG: ALT 51 → 34 (p = 0.09) MLG: ALT 54 → 32(p = 0.09) Per protocol: Non-significant reduction in ALT in MDG | MDG: TC: 197.2 → 185.6 (p = 0.08) TG: 132.86 → 106.29 (p = 0.28) | MDG: 3.4 → 2.6 (p = 0.60) |
| Abena-voli | MD vs. MD + Antioxidant (AO) vs. control (regular diet) | Monthly phone calls | MD: FL index: 71 (56–85) TE: 8.1 (6.7–9.2) kPa MD + AO: FL Index: 58 (42–69) TE: 6.9 (6.7–7.2) kPa | MD: FL index: 45 (39–69), (p = 0.002) TE: 6.0 (5.1–7.0) kPa (p = 0.0001) MD + AO: FL Index: 38 (29–45) (p = 0.003) TE: 5.0 (4.7–5.2) kPa (p = 0.0001) | MD: Wt: 83 → 78 (p = 0.0001) BMI: 31 → 29 (p = 0.0001) MD + AO Wt: 90 → 81 (p = 0.002) BMI: 29 → 27 (p = 0.0001) | No significant change in either group | MD: TC: 189 → 156 (p = 0.0001) TG: 140 → 85 (p = 0.0001) MD+AO: TC: 198 → 152 (p = 0.0001) TG: 106 → 75 (p = 0.011) | MD: 1.9 (0.9–2.4) → 1.8 (0.6–3.4) (p = 0.985) MD + AO: 4 (3–6) → 2 (1–2) (p = 0.001) |
| Properzi | MD (40% carbs, 40% fats, and 20% protein) vs. LF diet (50% carbs, 30% fat, and 20% protein) | Weekly dietician follow-up x 4 weeks, then monthly dietician follow-up | MD: Hepatic fat on MRS 34.2 ± 16.3% TE: 12.4 ± 15.4 kPa LF: Hepatic fat on MRS 21.5 ± 10%, TE: 7.0 ± 3.8 kPa | MD: Hepatic fat on MRS 24.0 ± 14.7% (p < 0.001) Liver stiffness: 11.7 ± 15.3 kPa (p = 0.11) LF: Hepatic fat on MRS 15.3 ± 7.7% (p < 0.001), Liver stiffness: 7.0 ± 6.0 kPa (p = 0.20) | MD: Wt: 89.3 → 87.3 (p < 0.001) BMI: 31.8 (4.0) → 31.1 (4.0) (p < 0.001) LF: Wt: 81.3 → 79.6 (p = 0.001) BMI: 30.1(5.69) → 29.5 (5.8) (p = 0.001) | MD: ALT 77 → 69 (p = 0.049) LF: ALT 68 → 56 (p = 0.004) | MD: TC: 184.8 → 175.2 (p = 0.010) TG: 165.6 → 144.2 (p = 0.008) LF: TC: 202.2 → 199.2 (p = 0.27) TG:144.4 → 139.9 (p = 0.38) | MD: 3.91 → 3.63 (p = 0.263) LF: 2.76 → 2.95 (p = 0.040) |
| Johari | MACR (type of IF) 70% calorie restricted diet between 2:00 p.m. and 8:00 p.m. one day, alternating with regular diet next day | Intermittent phone calls to patients by investigator Biweekly follow-up with dietician | Steatosis on US: 1.93 TE 5.87 kPA | Steatosis on US: 1.43 (Δ = 0.50, p = 0.001) Elastography: 5.01 kPA (Δ = 0.86 kPA, p = 0.001) | Weight 80.8 → 78.9 (p = 0.003) BMI = 31.73 → 30.95 (p = 0.03) | ALT 84.3→ 59.17 iU/L (p = 0.001) AST 51.4 → 42.7 iU/L (p = 0.004) | MACR: TC: 205.72 → 204.18 (p = 0.78) TG: 174.5 →185.12 (p = 0.58) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeed, N.; Nadeau, B.; Shannon, C.; Tincopa, M. Evaluation of Dietary Approaches for the Treatment of Non-Alcoholic Fatty Liver Disease: A Systematic Review. Nutrients 2019, 11, 3064. https://doi.org/10.3390/nu11123064
Saeed N, Nadeau B, Shannon C, Tincopa M. Evaluation of Dietary Approaches for the Treatment of Non-Alcoholic Fatty Liver Disease: A Systematic Review. Nutrients. 2019; 11(12):3064. https://doi.org/10.3390/nu11123064
Chicago/Turabian StyleSaeed, Naba, Brian Nadeau, Carol Shannon, and Monica Tincopa. 2019. "Evaluation of Dietary Approaches for the Treatment of Non-Alcoholic Fatty Liver Disease: A Systematic Review" Nutrients 11, no. 12: 3064. https://doi.org/10.3390/nu11123064
APA StyleSaeed, N., Nadeau, B., Shannon, C., & Tincopa, M. (2019). Evaluation of Dietary Approaches for the Treatment of Non-Alcoholic Fatty Liver Disease: A Systematic Review. Nutrients, 11(12), 3064. https://doi.org/10.3390/nu11123064