1. Introduction
The World Health Organization reports that cardiovascular disease (CVD) is the number one cause of death globally and largely caused by risk factors that can be controlled, treated, or modified, such as high blood pressure, cholesterol, obesity, tobacco use, physical inactivity, an unhealthy diet, and diabetes [
1]. The inverse relationship between the consumption of a plant-based diet and CVD prevalence has previously been established from cross-sectional, prospective, case-control [
2,
3], and clinical studies, an effect attributed to dietary fiber decreasing serum cholesterol levels [
4,
5] and the antioxidant compounds that predispose to lipoprotein oxidation [
5,
6]. On the other hand, compounds usually encountered in meat-based diets, such as saturated and trans fatty acids, are associated with increased risk of developing atherosclerosis [
7].
Diet is generally regarded as a major contributing factor to CVD prevention and treatment, and is considered to be the most important environmental component affecting hypertension [
8]. In this context, the DASH (Dietary Approaches to Stop Hypertension) diet, characterized by higher intake of fruits, vegetables, low-fat dairy, grains, fish, and poultry, has been shown to be effective in reducing both systolic and diastolic blood pressure levels [
9,
10]. The study of dietary patterns represents a more holistic approach to the investigation of exposure–disease associations, as nutrients are not consumed in isolation, but rather as part of many different meals consisting of foods with a variety of both micro- and macronutrients. Principal component analysis (PCA) is a data-driven approach that reduces the large number of food variables into a smaller set that captures the major dietary traits of a population [
11].
The Pomaks have, for centuries, inhabited the mountains of Thrace, an area in the northeast of modern Greece. The Pomaks live across the Rhodope mountain range and, following World War II, their populations were split between Greece and Bulgaria. In Greece, Pomaks dwell in three main areas: villages to the north of Xanthi, Komotini, and Evros [
12]. They represent a Muslim minority in Greece with uncertain origins [
13]. According to the most dominant theory, the Pomaks are descendants of the natives of the Rhodope Mountains [
14].
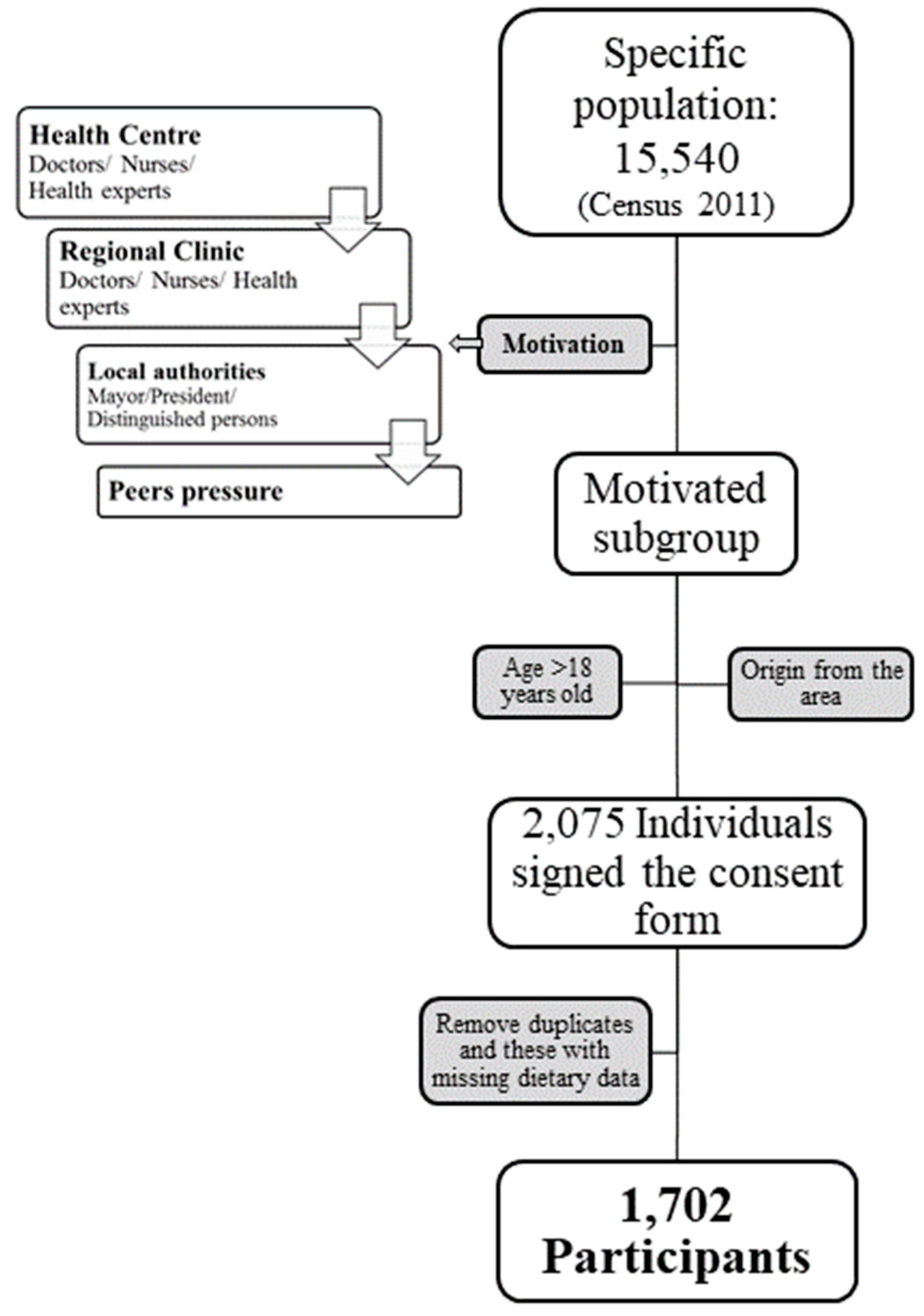
Although the population has been the object of extensive research, in terms of politics and folklore culture, to date there have not been any studies on their health and lifestyle. The main objective of this work was to conduct a well-phenotyped, population-based study in order to facilitate epidemiological analyses with respect to cardiovascular disease. The present study investigates the potential associations between dietary patterns derived from analyzing the eating habits of the local Pomak populations and cardiometabolic risk factors, as well as diabetes prevalence.
3. Results
The anthropometric and clinical characteristics of the population are presented in
Table 1. Of the 1702 participants, 30.7% were male and 69.3% female. The mean age of the population was 44.9 years and male volunteers were on average 5.5 years older than women (
p < 0.001). In addition, men were found to have greater WC (96.1 vs. 90.4 cm,
p < 0.001) and WHR (0.94 vs. 0.84,
p = 3.0E-80) than women. However, women showed a higher BMI compared to men (28 vs. 26.4 kg/m
2,
p < 0.001). A larger proportion of men were categorized as overweight (44.7% vs. 31.7%), while the proportion of obese women in the population was much greater than for men (25.9% vs. 5.5%,
p < 0.001). The mean value for systolic blood pressure was 131.2 mmHg, with men presenting significantly higher levels than women (133.3 vs. 130.1 mmHg,
p = 0.001). Refined cereals, dairy, vegetables, and sweets showed the greatest weekly consumption of all the food groups.
Hypertension and hyperlipidemia were the most prevalent disorders in the population (
Table 2). A higher percentage of men had hyperlipidemia (19.5% vs. 15.4%,
p = 0.036), presbyopia (11.1% vs. 6.2%,
p < 0.001), type 2 diabetes (10.2% vs. 6.1%,
p = 0.003), and coronary heart disease (11.7% vs. 4.6%,
p < 0.001) compared to women, while depression (11.7% vs. 7.5%,
p = 0.008), hypothyroidism (11.5% vs. 2.1%,
p < 0.001), and migraine (8.8% vs. 4.8%,
p = 0.004) were more prevalent in women.
Table 3 shows the sociodemographic and lifestyle characteristics of the Pomak population. The vast majority of the participants was married (86.7%) and reported primary education (72.2%). The proportion of illiteracy was higher in women than in men (13.2% vs. 5.8%,
p < 0.001). The proportion of both current and former smokers was 20 and 40 times higher in men compared to women, respectively, while the vast majority of women (97.3%) and one third of men (35%) had never smoked (
p < 0.001).
PCA highlighted four different dietary patterns (components), the factor loadings of which are presented in
Table 4. Alcohol and pork consumption were excluded as their consumption in the Pomak population was insignificant due to religious reasons. Fifteen out of the 48 remaining foods or food groups were included in the PCA as highly intercorrelated. The KMO criterion was 0.72, and 52% of the total variance was explained by the four dietary components. The components were defined according to the higher absolute scores that indicate greater contribution to each component. Thus, there are: the “high in sugars” dietary pattern (component 1), which includes fresh fruits, milky sweets, chocolate, beverages, juices, and starchy sweets; the “quick choices” dietary pattern (component 2), which is composed of processed red meat, ready-made pies, refined breads, and fries; the “balanced” dietary pattern (component 3), that consists of refined pasta, white rice, vegetables, legumes, and red meat; and the “homemade” dietary pattern (component 4), that is characterized by homemade pies, full-fat cheese, and potato consumption. The median of the scores for each component was used to divide the population into two groups: low and high adherence to the particular pattern.
As presented in
Table 5, women had significantly higher HDL cholesterol (
p < 0.001) and lower triglyceride levels (
p < 0.001) than men. The group with the higher scores in the “high in sugar” pattern and the balanced diet had elevated mean glucose levels. Mean HDL cholesterol was lower in the group with higher adherence scores to the “high in sugar” pattern, while LDL and total cholesterol levels were found to be higher in the group with lower adherence scores to the “quick choices” dietary pattern. The group with higher scores in the “high in sugar” pattern presented lower triglycerides levels compared to the group with lower scores in the same pattern.
The multiadjusted linear regression results are shown in
Table 6. In particular, component 1 with the high sugar content was associated with higher SBP (
β = 2.47,
p < 0.001), DBP (
β = 1.46,
p < 0.001), and glucose levels (
β = 3.44,
p < 0.001). Additionally, the high in sugars diet was found to be significantly associated with increased LDL cholesterol but the association was found not significant after adjustment for the remaining components of the diet. Component 2, representing the quick choices/junk food pattern, was found to be associated with increased insulin levels, albeit without high statistical significance (
β = 0.73,
p = 0.025). Component 3, representing the balanced diet, was significantly associated with reduced SBP (
β = −1.59,
p = 0.001). Component 4, the homemade dietary pattern, was found to be significantly associated with higher HDL levels, after adjusting for confounders, but the effect was nonsignificant when the remaining dietary patterns were taken into account.
Logistic regression analyses, summarized in
Table 7, showed that higher adherence to the high in sugars dietary pattern was nominally associated with increased risk of low HDL (OR [95%CI] 1.84 [1.24,2.75],
p = 0.003) and systolic hypertension (OR [95%CI] 2.40 [1.38,4.17],
p = 0.002) and statistically significantly associated with increased risk for diastolic hypertension (OR [95%CI] 2.61 [1.55,4.39],
p < 0.001), compared to lower adherence (
p-values are here compared to the adjusted cut-off of
p = 0.0125.)
4. Discussion
This is the first report of a cross-sectional cohort that describes the geographically and religiously isolated, genetically homogeneous [
33] population from the Pomak villages in Xanthi, as part of the HELIC-Pomak study (
www.helic.org). One advantage of isolated populations is that they are characterized by environmental homogeneity [
34] and thus a smaller sample size is required to detect an association with sufficient statistical power.
The Pomak population was found to be overweight, in keeping with observations from the general Greek population in the ATTICA study [
35]. The ATTICA study is a population-based health and nutrition survey, which attempts to evaluate several cardiovascular risk factors in the greater urban area of Athens, Greece [
36]. One third (31.3%) of the Pomak population was obese, while the corresponding percentage from the Greek Muslim community in the MetS-Greece study from the same area was 63.6% [
37]. The discrepancy might be due to the sample size and the population origin, as the MetS study only included 300 individuals from inside and around the city of Xanthi, while in our study we included 1702 individuals from many different villages including Kentavros, Glafki, Echinos, Pachni, Dimario, Melivia, Sminthy, Thermes, Miki, Oreo, and other Pomak villages. Inhabitants of more distant villages have preserved traditional characteristics in many aspects of their lives, while the residents of more urbanized areas and cities conform more closely to the mainstream Greek lifestyle. Consumption of red meat, dairy, and sweets was 2–3 times higher in the Pomak population compared to that of the Attica general population [
38], while vegetables, fruits, legumes, and potatoes intake was 2–4 times lower.
The proportion of individuals with hypertension (26.1%) found in the present study was comparable with that of other Greek studies [
36,
37,
38], but much lower than the ones reported (80%) by other isolated, but older, populations, such as the one on the island of Vis in Croatia [
39]. Occurrence of hyperlipidemia (16.7%) was in the same direction and magnitude compared to the ATTICA study [
38] which found a higher prevalence of the disease (43%). The prevalence of type 2 diabetes (7.3%) was comparable to that of the general Greek population [
36] and also to the one of the aforementioned isolated population from the island of Vis, Croatia [
39], but half of that reported (14.6%) in the chronic disease records of the local medical center [
40]. However, this apparent discrepancy may be due to the fact that these records only included three areas/villages.
The overwhelming majority of the population was married (86%), indicating the traditional position of the family within the society, a trend which is attenuated in more urban areas [
36]. Most of the participants had attained primary education, with more men being educated than women, a characteristic unlike that of the urban Greek population [
41] which reports almost double the number of total years in education. The smoking habits of men were similar to those of the general population of Attica [
42], while almost all women (97%) had never smoked, hinting at the preservation of a past etiquette that indicates the traditional character of this tobacco farming population.
It is noteworthy that the traditional lifestyle of the populations inhabiting the Pomak villages has been extensively studied in various locations, usually referring to factors such as eating habits, which may differ slightly or considerably among the different villages.
In this study, the characterization of the unique diet of the Pomak population was achieved through a posteriori technique, PCA analysis, generating patterns using empirically obtained data [
43]. Thus, the derived patterns reflect the most representative eating habits of the population.
The predominant dietary pattern is the “high in sugars” pattern (16.3% of the variance explained), and is very typical and closely connected with the sociocultural aspect of food in the Pomak population. Sweets, which are the main compound of the pattern, are offered after funerals in the form of chocolate or Turkish delight. In addition, increased sweets consumption is highlighted by the existence of a festival dedicated to the offering and the consumption of sweets, the “Seker Bayrami” or “Bayram of Sweets” [
12]. Bayram is the word used for festivals or holidays and is applicable to secular and mainly religious celebrations in Islam. In the present study, this particular pattern, which was rich in sugars, was negatively associated with HDL cholesterol levels. A cross-sectional study evaluating data from the National Health and Nutrition Examination Survey 1999–2006 also reported similar findings [
44]. The resulting low HDL cholesterol concentrations could be driven by the role of refined carbohydrates on the pathway that decreases insulin sensitivity, increases visceral adiposity, and stimulates hepatic de novo lipogenesis [
45].
The former pattern was also found to be associated with increased systolic and diastolic blood pressure. According to a systematic review and meta-analysis of six prospective cohorts, sugar-sweetened beverage consumption was indeed found to be associated with a modest risk of developing hypertension [
46]. A different systematic review and meta-analysis of eight studies further demonstrated statistically significant associations between sugary beverage consumption and hypertension [
47]. Moreover, habitual consumption of fruit juice was found to be associated with higher central blood pressure and central pulse pressure [
48], suggesting the overconsumption of added fructose as the main cause [
49,
50]. As expected, the “high in sugars” pattern was also associated with increased glucose levels. This is consistent with the results from the EPIC-InterAct study where sugar-sweetened soft drinks were associated with an increased prevalence of type 2 diabetes [
51]. The European Prospective Investigation into Cancer and Nutrition (EPIC) study is one of the largest cohort studies in the world, with participants from 10 European countries, and is designed to investigate the relationships between dietary, environmental, and lifestyle factors, and the incidence of chronic diseases. The EPIC-Netherlands follow-up study stated that carbohydrate (hazard ratio 1.15) and starch (hazard ratio 1.25) intake was related to increased diabetes risk [
52]. Bringing these together, it is apparent that dietary sugars have many unfavorable effects on a whole spectrum of metabolic disorders that take place in CVD and metabolic syndrome [
53].
The “high in sugars” pattern observed in the Pomak population is associated with most of the components of metabolic syndrome, while in the ATTICA study, the “sweets” pattern was not associated with any aspect of metabolic syndrome [
54]. One possible reason for this discrepancy could be the differencing tools used for dietary assessment (72 vs. 156 items FFQ) and the diversity of the compounds composing each particular pattern/component. The fat content of the milky sweets and chocolates in the “high in sugars” pattern of the Pomak population may intensify the negative effects on cardiovascular risk, while the specific food compounds of the “sweets” pattern of the ATTICA study are not known.
High fat consumption is mainly represented by the “quick choices pattern”, which includes processed meat, fries, and ready-made pies, as well as refined breads, comprising a fast/junk food pattern. This particular pattern was nominally associated with increased levels of insulin, a finding consistent with current literature, suggesting meat consumption to be associated with hyperinsulinaemia and type 2 diabetes [
38,
55]. The total fat, mainly consisting of the saturated fat of the meat and the trans fatty acids of the fried potatoes, is believed to contribute to the increased prevalence of insulin resistance and type 2 diabetes [
56,
57,
58].
The “balanced pattern” represents the consumption of rice, pasta, red meat, vegetables, and legumes. Rice is a traditional food of the Pomak population which, in the form of pilaf, is the main dish at ceremonies and celebrations like funerals and weddings. Red meat, such as lamb and beef, has had a central role in the social life of the Pomaks throughout their history, with the dedication of an entire religious festival to its consumption, called “Kurban Bayramı” or “Sacrifice Bayram” [
12]. The former represents a prudent dietary pattern that incorporates customs and traditions of Pomaks and is found to be associated with reduced systolic and diastolic blood pressure. Similar results have been reported by the ATTICA study [
42], where the Mediterranean diet was associated with a lower risk of hypertension (OR = 0.74,
p = 0.021). Pala et al. found that hypertension was associated with adherence to the pasta and meat pattern [
59]. The opposite findings demonstrated in the present study could be attributed to the additional constituents of the pasta and meat pattern such as other animal fats, wine, bread, processed meat, and pork. Moreover, the presence of vegetables and legumes in the Pomak “balanced pattern” may play a protective role against CVD. The “balanced pattern” was also associated with lower LDL cholesterol levels, a finding consistent with current literature [
60].
The cross-sectional nature of this study does not allow for cause/effect implications to be drawn or generalization of the results from this particular Pomak population. Selection bias should also be considered as a limitation of our study without any data for comparison between responders and nonresponders. Another limitation is that the medical history and medication information come from self-reported data, subjected to possible under-reporting or memory bias. In addition, the FFQ used has not been validated in this specific population, although it has been validated in the general Greek population [
21]. Moreover, the principal component analysis is partly underpinned by subjective decisions like how many foods and/or food groups have been included, how many components have been retained, and/or the nomenclature of the patterns, which is also a potential limitation. Seven outcomes of interest have been tested, using the stringent Bonferroni corrected
p-value of 0.0125. Using this significance threshold, the associations of the “high in sugar” dietary pattern with SBP, DBP, and glucose levels and the association of the “balanced” dietary pattern with SBP levels, are the only ones to remain significant. The association between the “quick choices” dietary pattern and insulin becomes suggestive as it no longer reaches nominal significance.

 ,
, 

{kind=link}