Comparison of 24-h Diet Records, 24-h Urine, and Duplicate Diets for Estimating Dietary Intakes of Potassium, Sodium, and Iodine in Children



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Recruitment
2.2. Demographic Data
2.3. 24-h Diet Records and Duplicate Diets
2.4. Urine Sample and Urinary Sodium, Potassium, and Iodine Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nguyen, T.T.M.; Miura, K.; Tanaka-Mizuno, S.; Tanaka, T.; Nakamura, Y.; Fujiyoshi, A.; Kadota, A.; Tamaki, J.; Takebayashi, T.; Okamura, T.; et al. Association of blood pressure with estimates of 24-h urinary sodium and potassium excretion from repeated single-spot urine samples. Hypertens. Res. 2019, 42, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Brion, M.J.; Ness, A.R.; Davey Smith, G.; Emmett, P.; Rogers, I.; Whincup, P.; Lawlor, D.A. Sodium intake in infancy and blood pressure at 7 years: Findings from the avon longitudinal study of parents and children. Eur. J. Clin. Nutr. 2008, 62, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Yusuf, S.; Mente, A.; Gao, P.; Mann, J.F.; Teo, K.; McQueen, M.; Sleight, P.; Sharma, A.M.; Dans, A.; et al. Urinary sodium and potassium excretion and risk of cardiovascular events. JAMA 2011, 306, 2229–2238. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.J.; Bibbins-Domingo, K.; Jin, Z.; Daviglus, M.L.; Goff, D.C., Jr.; Jacobs, D.R., Jr. Association of sodium and potassium intake with left ventricular mass: Coronary artery risk development in young adults. Hypertension 2011, 58, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Umesawa, M.; Iso, H.; Date, C.; Yamamoto, A.; Toyoshima, H.; Watanabe, Y.; Kikuchi, S.; Koizumi, A.; Kondo, T.; Inaba, Y.; et al. Relations between dietary sodium and potassium intakes and mortality from cardiovascular disease: The japan collaborative cohort study for evaluation of cancer risks. Am. J. Clin. Nutr. 2008, 88, 195–202. [Google Scholar] [CrossRef]
- Cook, N.R.; Appel, L.J.; Whelton, P.K. Lower levels of sodium intake and reduced cardiovascular risk. Circulation 2014, 129, 981–989. [Google Scholar] [CrossRef]
- D’Elia, L.; Galletti, F.; Strazzullo, P. Dietary salt intake and risk of gastric cancer. Cancer Treat. Res. 2014, 159, 83–95. [Google Scholar]
- D’Elia, L.; Rossi, G.; Ippolito, R.; Cappuccio, F.P.; Strazzullo, P. Habitual salt intake and risk of gastric cancer: A meta-analysis of prospective studies. Clin. Nutr. 2012, 31, 489–498. [Google Scholar] [CrossRef]
- Ge, S.; Feng, X.; Shen, L.; Wei, Z.; Zhu, Q.; Sun, J. Association between habitual dietary salt intake and risk of gastric cancer: A systematic review of observational studies. Gastroenterol. Res. Pract. 2012, 2012, 808120. [Google Scholar] [CrossRef]
- Deriaz, D.; Guessous, I.; Vollenweider, P.; Devuyst, O.; Burnier, M.; Bochud, M.; Ponte, B. Estimated 24-h urinary sodium and sodium-to-potassium ratio are predictors of kidney function decline in a population-based study. J. Hypertens. 2019, 37, 1853–1860. [Google Scholar] [CrossRef]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Riley, M.D.; Whiting, S. Association between urinary potassium, urinary sodium, current diet, and bone density in prepubertal children. Am. J. Clin. Nutr. 2001, 73, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Rafie, N.; Hamedani, S.G.; Mohammadifard, N.; Feizi, A.; Safavi, S.M. 24-h urinary sodium to potassium ratio and its association with obesity in children and adolescents. Eur. J. Nutr. 2019, 58, 947–953. [Google Scholar] [CrossRef]
- Jain, N.; Minhajuddin, A.T.; Neeland, I.J.; Elsayed, E.F.; Vega, G.L.; Hedayati, S.S. Association of urinary sodium-to-potassium ratio with obesity in a multiethnic cohort. Am. J. Clin. Nutr. 2014, 99, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Nazeri, P.; Bahadoran, Z.; Khalili-Moghadam, S.; Azizi, F. Dietary sodium to potassium ratio and the incidence of chronic kidney disease in adults: A longitudinal follow-up study. Prev. Nutr. Food Sci. 2018, 23, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R.; Obarzanek, E.; Cutler, J.A.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K.; Trials of Hypertension Prevention Collaborative Research Group. Joint effects of sodium and potassium intake on subsequent cardiovascular disease: The trials of hypertension prevention follow-up study. Arch. Intern. Med. 2009, 169, 32–40. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Potassium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]
- Lucko, A.M.; Doktorchik, C.; Woodward, M.; Cogswell, M.; Neal, B.; Rabi, D.; Anderson, C.; He, F.J.; MacGregor, G.A.; L’Abbe, M.L.; et al. Percentage of ingested sodium excreted in 24-h urine collections: A systematic review and meta-analysis. J. Clin. Hypertens. 2018, 20, 1220–1229. [Google Scholar] [CrossRef]
- Australian Department of Health and Ageing; National Health and Medical Research Council; New Zealand Ministry of Health. Nutrient Reference Values for Australia and New Zealand; Australian Department of Health and Ageing & New Zealand Ministry of Health: Canberra, Australia, 2006.
- Perkin-Elmer Corporation. Analytical Methods for Atomic Absorption Spectrophotometry; Perkin-Elmer Co.: Shelton, CT, USA, 1996. [Google Scholar]
- Fecher, P.A.; Goldmann, I.; Nagengast, A. Determination of iodine in food samples by inductively coupled plasma mass spectrometry after alkaline extraction. J. Anal. At. Spectrom. 1998, 13, 977–982. [Google Scholar] [CrossRef]
- Marthaler, T. Monitoring of Renal Fluoride Excretion in Community Preventive Programmes on Oral Health; World Health Organization (WHO): Geneva, Switzerland, 1999. [Google Scholar]
- Harttig, U.; Haubrock, J.; Knuppel, S.; Boeing, H.; Consortium, E. The msm program: Web-based statistics package for estimating usual dietary intake using the multiple source method. Eur. J. Clin. Nutr. 2011, 65 (Suppl. 1), S87–S91. [Google Scholar] [CrossRef]
- Nam, G.E.; Kim, S.M.; Choi, M.-K.; Heo, Y.R.; Hyun, T.S.; Lyu, E.S.; Oh, S.Y.; Park, H.R.; Ro, H.K.; Han, K. Association between 24-h urinary sodium excretion and obesity in korean adults: A multicenter study. Nutrition 2017, 41, 113–119. [Google Scholar] [CrossRef]
- Park, Y.; Dodd, K.W.; Kipnis, V.; Thompson, F.E.; Potischman, N.; Schoeller, D.A.; Baer, D.J.; Midthune, D.; Troiano, R.P.; Bowles, H. Comparison of self-reported dietary intakes from the automated self-administered 24-h recall, 4-d food records, and food-frequency questionnaires against recovery biomarkers. Am. J. Clin. Nutr. 2018, 107, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Trijsburg, L.; De Vries, J.; Boshuizen, H.; Hulshof, P.; Hollman, P.; Van‘t Veer, P.; Geelen, A. Comparison of duplicate portion and 24 h recall as reference methods for validating a ffq using urinary markers as the estimate of true intake. Br. J. Nutr. 2015, 114, 1304–1312. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.W.; Mertz, W.; Judd, J.T.; Marshall, M.W.; Kelsay, J.L.; Prather, E.S. Effect of making duplicate food collections on nutrient intakes calculated from diet records. Am. J. Clin. Nutr. 1984, 40, 1333–1337. [Google Scholar] [CrossRef] [PubMed]
- Johansson, G.; Åkesson, A.; Berglund, M.; Nermell, B.; Vahter, M. Validation with biological markers for food intake of a dietary assessment method used by swedish women with three different with dietary preferences. Public Health Nutr. 1998, 1, 199–206. [Google Scholar] [CrossRef]
- Lerchl, K.; Rakova, N.; Dahlmann, A.; Rauh, M.; Goller, U.; Basner, M.; Dinges, D.F.; Beck, L.; Agureev, A.; Larina, I. Agreement between 24-h salt ingestion and sodium excretion in a controlled environment. Hypertension 2015, 66, 850–857. [Google Scholar] [CrossRef]
- Turban, S.; Miller, E.R.; Ange, B.; Appel, L.J. Racial differences in urinary potassium excretion. J. Am. Soc. Nephrol. 2008, 19, 1396–1402. [Google Scholar] [CrossRef]
- Birukov, A.; Rakova, N.; Lerchl, K.; Olde Engberink, R.H.; Johannes, B.; Wabel, P.; Moissl, U.; Rauh, M.; Luft, F.C.; Titze, J. Ultra-long–term human salt balance studies reveal interrelations between sodium, potassium, and chloride intake and excretion. Am. J. Clin. Nutr. 2016, 104, 49–57. [Google Scholar] [CrossRef]
- Zimmermann, M.B. Methods to assess iron and iodine status. Br. J. Nutr. 2008, 99, S2–S9. [Google Scholar] [CrossRef]
- World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers; World Health Organization (WHO): Geneva, Switzerland, 2007. [Google Scholar]
- World Health Organization. The Shake Technical Package for Salt Reduction; World Health Organization (WHO): Geneva, Switzerland, 2016. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N (%) a |
|---|---|
| Age, years | 9.6 (0.7) |
| Sex, female | 41 (48.8) |
| Ethnicity | |
| NZEO b | 73 (86.9) |
| Māori or Pacific | 11 (13.1) |
| School decile, median (25th, 75th percentile) | 8 (6, 9) |
| N b | Sodium (mg) | Potassium (mg) | Iodine (μg) | |
|---|---|---|---|---|
| 24-h urine a,b, mean (SD) | 82 | 2119 (439) | 1414 (345) | 74 (17) |
| 24-h record a, mean (SD) | 84 | 2223 (152) | 2108 (111) | 52 (6) |
| Duplicate diet a,b, mean (SD) | 37 | 1886 (405) b | 2172 (593) b | 95 (18) |
| Mean differences a (95% CI) | ||||
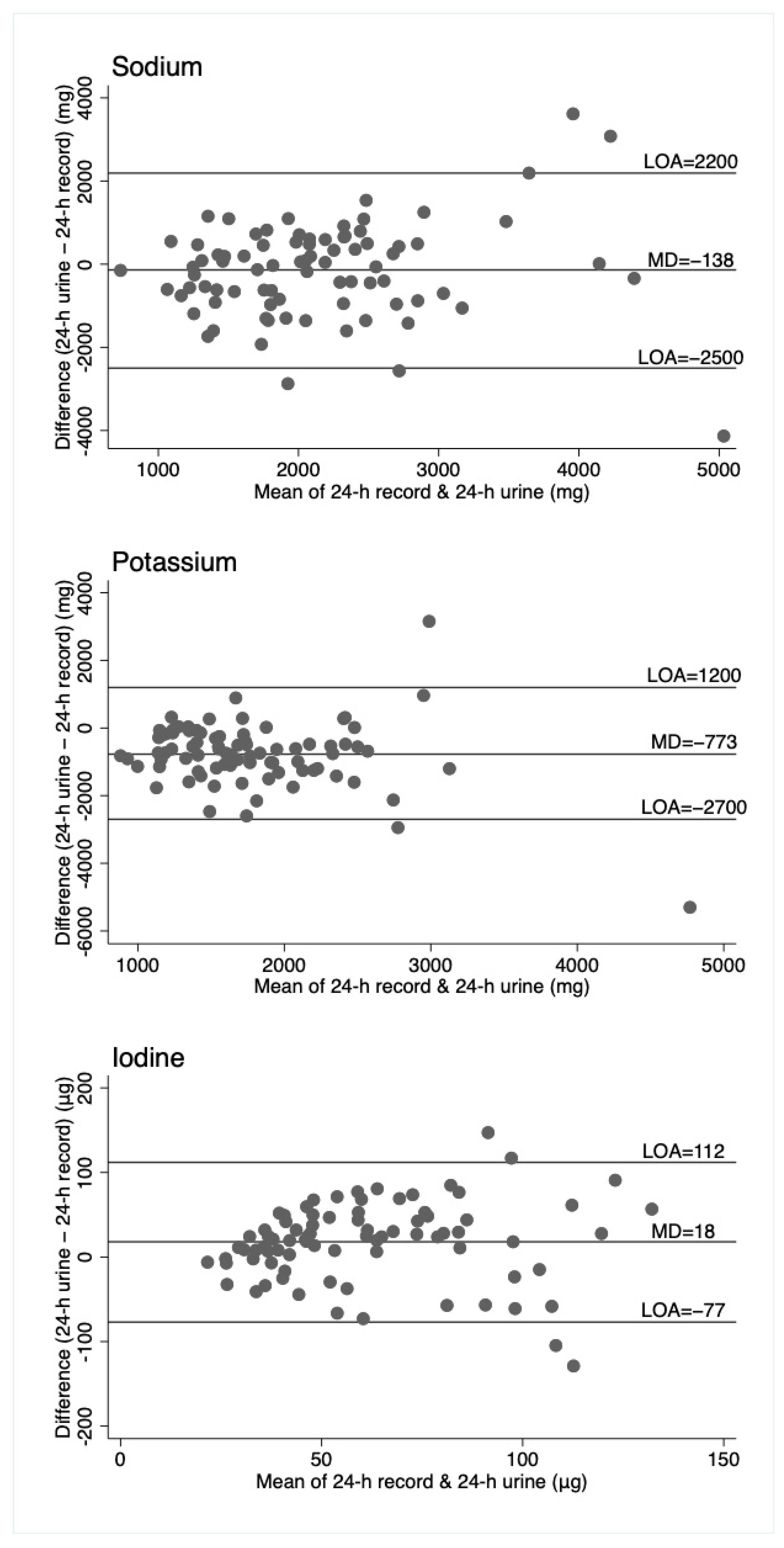
| 24-h record -24-h urine | 82 | 138 (−118, 394) | 773 (557, 990) | −18 (−28, −7) |
| duplicate diet -24-h urine | 36 | −237 (−542, 69) b | 863 (543, 1183) b | 24 (8, 40) |
| duplicate diet -24-h record | 37 | −250 (−471, −29) b | 254 (−10, 519) b | 43 (29, 57) |
| Mean differences (95%CI) for participants with all three measures a | ||||
| 24-h record -24-h urine | 34 | 22 (−363, 407) | 606 (320, 902) | −20 (−35, −5) |
| duplicate diet -24-h urine | 34 | −237 (−542, 69) | 863 (543, 1183) | 24 (8, 40) |
| duplicate diet -24-h record | 34 | −259 (−486, −32) | 257 (−16, 549) | 44 (29, 58) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peniamina, R.; Skeaff, S.; Haszard, J.J.; McLean, R. Comparison of 24-h Diet Records, 24-h Urine, and Duplicate Diets for Estimating Dietary Intakes of Potassium, Sodium, and Iodine in Children. Nutrients 2019, 11, 2927. https://doi.org/10.3390/nu11122927
Peniamina R, Skeaff S, Haszard JJ, McLean R. Comparison of 24-h Diet Records, 24-h Urine, and Duplicate Diets for Estimating Dietary Intakes of Potassium, Sodium, and Iodine in Children. Nutrients. 2019; 11(12):2927. https://doi.org/10.3390/nu11122927
Chicago/Turabian StylePeniamina, Rana, Sheila Skeaff, Jillian J. Haszard, and Rachael McLean. 2019. "Comparison of 24-h Diet Records, 24-h Urine, and Duplicate Diets for Estimating Dietary Intakes of Potassium, Sodium, and Iodine in Children" Nutrients 11, no. 12: 2927. https://doi.org/10.3390/nu11122927
APA StylePeniamina, R., Skeaff, S., Haszard, J. J., & McLean, R. (2019). Comparison of 24-h Diet Records, 24-h Urine, and Duplicate Diets for Estimating Dietary Intakes of Potassium, Sodium, and Iodine in Children. Nutrients, 11(12), 2927. https://doi.org/10.3390/nu11122927