Sodium and Potassium Intake, Knowledge Attitudes and Behaviour Towards Salt Consumption Amongst Adults in Podgorica, Montenegro

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
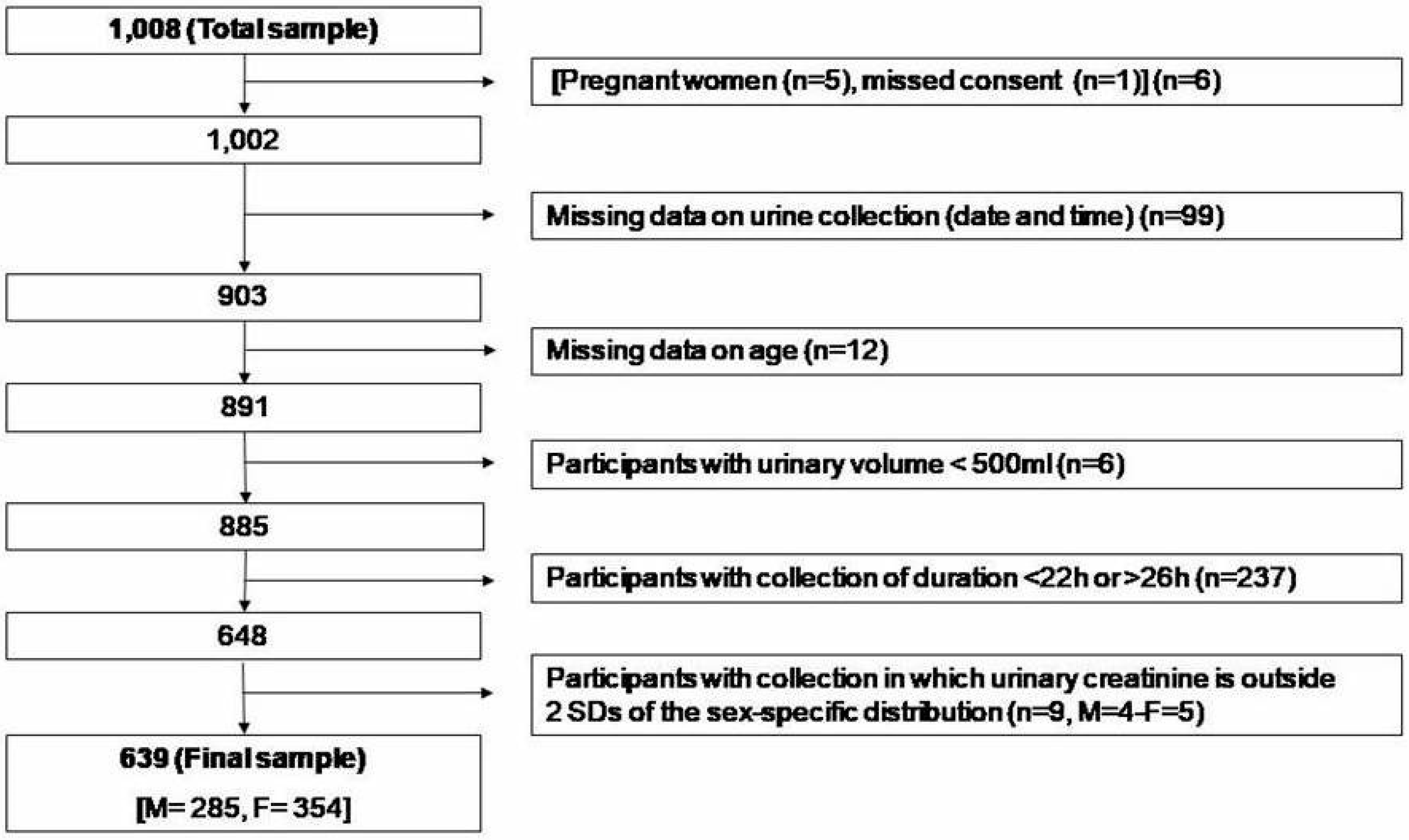
2.1. Participants and Recruitment
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
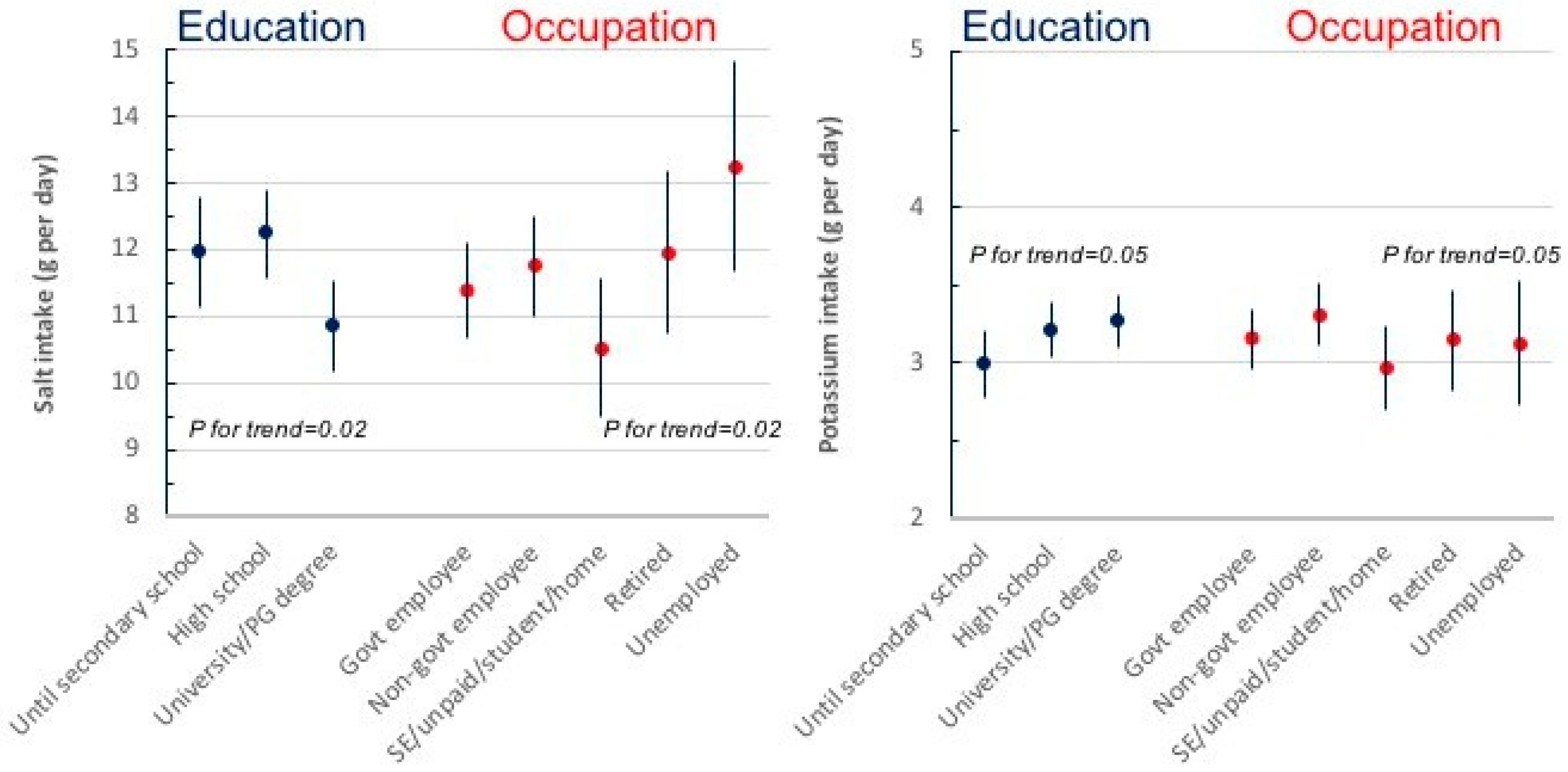
3.2. Daily Urinary Excretions of Volume, Sodium, Potassium and Creatinine and Salt and Potassium Intake
3.3. Knowledge, Attitude and Behaviours Towards Salt Intake
4. Discussion
4.1. Strengths and Limitations
4.2. Conclusions
Supplementary Materials
Author Contributions
Funding
#Salt Consumption Survey in Montenegro Study Group (in alphabetical order)
Acknowledgments
Conflicts of Interest
References
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef]
- World Health Organization. Non-Communicable Diseases; Country Profile: Geneva, Switzerland, 2014. [Google Scholar]
- National Registry for Acute Coronary Diseases and Cerebrovascular Diseases; Institute of Public Health: Podgorica, Montenegro, 2013.
- European Heart Network. Transforming European Food and Drink Policies for Cardiovascular Health; European Heart Network: Brussels, Belgium, 2017; pp. 1–137. [Google Scholar]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J. Effect of lower sodium intake on health: Systematic review and meta-analysis. Br. Med. J. 2013, 346, f1326. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Li, J.; MacGregor, G.A. Effect of longer-term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. Br. Med. J. 2013, 346, f1325. [Google Scholar] [CrossRef] [PubMed]
- Strazzullo, P.; D’Elia, L.; Kandala, N.-B.; Cappuccio, F.P. Salt intake, stroke, and cardiovascular disease: Meta-analysis of prospective studies. Br. Med. J. 2009, 339, b4567. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R.; Cutler, J.A.; Obarzanek, E.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: Observational follow-up of the Trials of Hypertension Prevention (TOHP). Br. Med. J. 2007, 334, 885–888. [Google Scholar] [CrossRef]
- Cappuccio, F.P. Cardiovascular and other effects of salt consumption. Kidney Int. 2013, 3, 312–315. [Google Scholar] [CrossRef]
- D’Elia, L.; Rossi, G.; Schiano di Cola, M.; Savino, I.; Galletti, F.; Strazzullo, P. Meta-analysis of the effect of dietary sodium restriction with or without concomitant renin–angiotensin–aldosterone system-inhibiting treatment on albuminuria. Clin. J. Am. Soc. Nephrol. 2015, 10, 1542–1552. [Google Scholar] [CrossRef]
- D’Elia, L.; Galletti, F.; La Fata, E.; Sabino, P.; Strazzullo, P. Effect of dietary sodium restriction on arterial stiffness: Systematic review and meta-analysis of the randomized controlled trials. J. Hypertens. 2018, 36, 734–743. [Google Scholar] [CrossRef]
- World Health Organization. Guideline. Sodium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; Capewell, S. Facts, issues, and controversies in salt reduction for the prevention of cardiovascular disease. Funct. Food Rev. 2015, 7, 41–61. [Google Scholar]
- WHO Regional Office for Europe. Mapping Salt Reduction Initiatives in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Mattes, R.D.; Donnelly, D. Relative contributions of dietary sources. J. Am. Coll. Nutr. 1991, 10, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Castillo, C.P.; Warrender, S.; Whitehead, T.P.; James, W.P. An assessment of the sources of dietary salt in a British population. Clin. Sci. 1987, 72, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Jovicic-Bata, J.; Grujicic, M.; Raden, S.; Novakovic, B. Sodium intake and dietary sources of sodium in a sample of undergraduate students from NoviSad, Serbia. Vojnosanitetski Pregled 2016, 73, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Ribič, C.H.; Zakotnik, J.M.; Vertnik, L.; Vegnuti, M.; Cappuccio, F.P. Salt intake of the Slovene population assessed by 24-hour urinary sodium excretion. Public Health Nutr. 2010, 13, 1803–1809. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013; pp. 1–103. [Google Scholar]
- Cappuccio, F.P.; Capewell, S.; Lincoln, P.; McPherson, K. Policy options to reduce population salt intake. Br. Med. J. 2011, 343, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.R.C.; Appel, L.J.; Cappuccio, F.P.; Correa-Rotter, R.; Hankey, G.J.; Lackland, D.T.; MacGregor, G.; Neal, B.; Niebylski, M.L.; Webster, J.; et al. A call for quality research on salt intake and health: From the World Hypertension League and Supporting Organizations. J. Clin. Hypertens. 2014, 16, 469–471. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. Br. Med. J. 2013, 346, f1378. [Google Scholar] [CrossRef]
- D’Elia, L.; Barba, G.; Cappuccio, F.P.; Strazzullo, P. Potassium Intake, Stroke, and Cardiovascular Disease. A meta-analysis of Prospective Studies. J. Am. Coll. Cardiol. 2011, 57, 1210–1219. [Google Scholar] [CrossRef]
- D’Elia, L.; Iannotta, C.; Sabino, P.; Ippolito, R. Potassium rich-diet and risk of stroke: Updated meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 585–587. [Google Scholar] [CrossRef]
- World Health Organization. Guideline: Potassium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012; pp. 1–52. [Google Scholar]
- Pan American Health Organization/World Health Organization. Salt-Smart Americas: A Guide for Country-Level Action; PAHO: Washington, DC, USA, 2013; pp. 1–159. [Google Scholar]
- World Health Organization. How to Obtain Measures of Population-Level Sodium Intake in 24-Hour Urine Samples; WHO-EM/NUT/279/E; World Health Organization/Regional Office of the Eastern Mediterranean: Cairo, Egypt, 2018; pp. 1–51. [Google Scholar]
- World Medical Association. Declaration of Helsinki. Recommendations guiding doctors in clinical research. Bull. World Health Org. 2008, 86, 650–651. [Google Scholar]
- World Health Organization. The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance (STEPS); WHO: Geneva, Switzerland; Available online: http://www.who.int/ncds/surveillance/steps/STEPS_Instrument_v2.1.pdf (accessed on 11 January 2019).
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redón, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2013, 31, 1281–1357. [Google Scholar] [CrossRef] [PubMed]
- Oesch, U.; Ammann, D.; Simon, W. Ion-selective membrane electrodes for clinical use. Clin. Chem. 1986, 32, 1448–1459. [Google Scholar] [PubMed]
- Junge, W.; Wilke, B.; Halabi, A.; Klein, G. Determination of reference intervals for serum creatinine, creatinine excretion and creatinine clearance with an enzymatic and a modified Jaffé method. Clin. Chim. Acta 2004, 344, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Ji, C.; Donfrancesco, C.; Palmieri, L.; Ippolito, R.; Vanuzzo, D.; Giampaoli, S.; Strazzullo, P. Geographic and socio-economic variation of sodium and potassium intake in Italy. Results from the MINISAL-GIRCSI programme. BMJ Open 2015, 5, e007467. [Google Scholar] [CrossRef] [PubMed]
- Donfrancesco, C.; Ippolito, R.; Lo Noce, C.; Palmieri, L.; Iacone, R.; Russo, O.; Vanuzzo, D.; Galletti, F.; Galeone, D.; Giampaoli, S.; et al. Excess dietary sodium and inadequate potassium intake in Italy: Results of the MINISAL study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Vasara, E.; Marakis, G.; Breda, J.; Skepastianos, P.; Hassapidou, M.; Kafatos, A.; Rodopaios, N.; Koulouri, A.; Cappuccio, F.P. Sodium and Potassium Intake in Healthy Adults in Thessaloniki Greater Metropolitan Area-The Salt Intake in Northern Greece (SING) Study. Nutrients 2017, 22, 417. [Google Scholar] [CrossRef] [PubMed]
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.E.; Lim, S.S.; Danaei, G.; Mozaffarian, D.; on behalf of the Global Burden of Diseases Nutrition and Chronic Diseases Expert Group (NutriCoDE). Global, regional and national sodium intakes in 1990 and 2010: A systematic analysis of 24 h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3, e003733. [Google Scholar] [CrossRef] [PubMed]
- Commission of Social Determinants of Health. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; Final Report of the Commission on Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008; pp. 1–246. ISBN 978 92 4 156370 3. [Google Scholar]
- The Marmot Review Group. Fair Society, Healthy Lives. Strategic Review of Health Inequalities in England Post-2010; The Marmot Review Group: London, UK, 2010; pp. 1–238. [Google Scholar]
- Millett, C.; Laverty, A.A.; Stylianou, N.; Kirsten Bibbins-Domingo, K.; Pape, U.J. Impacts of a national strategy to reduce population salt intake in England: Serial cross-sectional study. PLoS ONE 2012, 7, e29836. [Google Scholar] [CrossRef]
- Ji, C.; Kandala, N.-B.; Cappuccio, F.P. Spatial variation of salt intake in Britain and association with socioeconomic status. BMJ Open 2013, 3, e002246. [Google Scholar] [CrossRef]
- Ji, C.; Cappuccio, F.P. Socioeconomic inequality in salt intake in Britain 10 years after a national salt reduction program. BMJ Open 2014, 4, e005683. [Google Scholar] [CrossRef]
- Capewell, S.; Graham, H. Will cardiovascular disease prevention widen health inequalities? PLoS Med. 2010, 7, e1000320. [Google Scholar] [CrossRef]
- Hogberg, L.; Cnattingius, S.; Lundholm, C.; Sparen, P.; Iliadou, A.N. Intergenerational social mobility and the risk of hypertension. J. Epidemiol. Community Health 2012, 66, e9. [Google Scholar] [CrossRef] [PubMed]
- Lopez, C.N.; Martinez-Gonzalez, M.A.; Sanchez-Villegas, A.; Alonso, A.; Pimenta, A.M.; Bes-Rastrollo, M. Costs of Mediterranean and western dietary patterns in a Spanish cohort and their relationship with prospective weight change. J. Epidemiol. Community Health 2009, 63, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Monsivais, P.; Cook, A.J.; Drewnowski, A. Does diet cost mediate the relation between socioeconomic position and diet quality? Eur. J. Clin. Nutr. 2011, 65, 1059–1066. [Google Scholar] [CrossRef]
- Bonaccio, M.; Di Castelnuovo, A.; Pounis, G.; Costanzo, S.; Persichillo, M.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; for the Moli-sani Study Investigators. High adherence to the Mediterranean diet is associated with cardiovascular protection in higher but not in lower socioeconomic groups: Prospective findings from the Moli-sani study. Int. J. Epidemiol. 2017, 46, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Fernandez, R.; Siopa, M.; Simpson, S.J.; Amiya, R.M.; Breda, J.; Cappuccio, F.P. Current salt reduction policies across gradients of inequality-adjusted human development in the WHO European region: Minding the gaps. Public Health Nutr. 2014, 17, 1894–1904. [Google Scholar] [CrossRef]
- Lerchl, K.; Rakova, N.; Dahlmann, A.; Rauh, M.; Goller, U.; Basner, M.; Dinges, D.F.; Beck, L.; Agureev, A.; Larina, I.; et al. Agreement between 24-hour salt ingestion and sodium excretion in a controlled environment. Hypertension 2015, 66, 850–857. [Google Scholar] [CrossRef]
- Census of Population, Households and Dwellings in Montenegro 2011. Monstat, 2011. Available online: http://www.monstat.org/userfiles/file/popis2011/saopstenje/saopstenje(1).pdf (accessed on 16 October 2018).




{kind=link}
{kind=link}
{kind=link}
| All (n = 639) | Men (n = 285) | Women (n = 354) | |
|---|---|---|---|
| Age (yrs) | 46.8 (11.3) | 46.7 (11.3) | 46.9 (11.3) |
| Height (cm) | 175.4 (9.2) | 182.5 (7.0) | 169.6 (6.1) † |
| Weight (kg) | 79.8 (16.8) | 90.9 (15.2) | 70.7 (12.0) † |
| BMI (kg/m2) | 25.8 (4.2) | 27.1 (3.8) | 24.6 (4.3) † |
| Systolic blood pressure (mmHg) | 125.1 (16.2) | 129.2 (14.4) | 121.8 (16.7) † |
| Diastolic blood pressure (mmHg) | 79.1 (9.2) | 80.7 (7.6) | 77.9 (10.1) † |
| Pulse Rate (b/min) | 72.4 (8.7) | 73.3 (8.5) | 71.6 (8.9) † |
| Current smokers n (%) | 166 (26.2) | 68 (23.9) | 98 (28.1) |
| Occupation* (in the last 12 months) n (%) | |||
| Government employee | 195 (30.6) | 74 (26.0) | 121 (34.5) † |
| Non-government employee | 188 (29.5) | 99 (34.7) | 89 (25.4) |
| Self-employed | 47 (7.4) | 32 (11.2) | 15 (4.3) |
| Unpaid | 6 (0.9) | 4 (1.4) | 2 (0.6) |
| Student | 3 (0.5) | 2 (0.7) | 1 (0.3) |
| Housewife | 39 (6.1) | - | 39 (11.1) |
| Retired | 80 (12.6) | 35 (12.3) | 45 (12.8) |
| Unemployed (able to work) | 36 (5.7) | 18 (6.3) | 18 (5.1) |
| Unemployed (unable to work) | 5 (0.8) | 3 (1.1) | 2 (0.6) |
| Other | 11 (1.7) | 6 (2.1) | 5 (1.4) |
| Refused | 26 (4.1) | 12 (4.2) | 14 (4.0) |
| Education attainment * n (%) | |||
| Less than primary school | 6 (0.9) | 2 (0.7) | 4 (1.1) |
| Primary school | 24 (3.8) | 9 (3.2) | 15 (4.3) |
| Secondary school | 128 (20.1) | 57 (20.0) | 71 (20.2) |
| High school | 237 (37.3) | 119 (41.8) | 118 (33.6) |
| College/University | 201 (31.6) | 81 (28.4) | 120 (34.2) |
| Postgraduate degree | 26 (4.1) | 12 (4.2) | 14 (4.0) |
| Refused | 14 (2.2) | 5 (1.8) | 9 (2.6) |
| All (n = 639) | Men (n = 285) | Women (n = 354) | |
|---|---|---|---|
| Volume (mL/24 h) | 1629 (608) | 1694 (569) | 1576 (633) * |
| Sodium (mmoL/24 h) | 186.5 (90.3) | 221.9 (101.3) | 158.0 (68.2) † |
| Potassium (mmoL/24 h) | 62.5 (26.2) | 68.5 (27.6) | 57.6 (23.9) † |
| Creatinine (g/24 h) | 1.41 (0.55) | 1.73 (0.60) | 1.15 (0.35) † |
| Salt intake (g/day) | 11.6 (5.6) | 13.9 (6.3) | 9.9 (4.3) † |
| Potassium intake (g/day) | 3.2 (1.3) | 3.5 (1.4) | 2.9 (1.2) † |
| Question | Total (n = 639) | Men (n = 285) | Women (n = 354) |
|---|---|---|---|
| Do you add salt to food at the table? (Often/Always) | 73.8% | 79.1% | 67.2% * |
| In the food you eat at home salt is added in cooking (Often/Always) | 21.4% | 25.2% | 18.3% ** |
| How much salt do you think you consume? (Far too much/Too much) | 35.6% | 37.5% | 34.0% |
| Do you think that a high salt diet could cause a serious health problem? (Yes) | 85.8% | 82.8% | 88.3% |
| How important is lowering salt/sodium in your diet? (Very important) | 44.2% | 40.5% | 47.1% |
| Do you do anything on a regular basis to control your salt/sodium intake? (Yes) | 34.3% | 27.6% | 39.8% * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Elia, L.; Brajović, M.; Klisic, A.; Breda, J.; Jewell, J.; Cadjenović, V.; Cappuccio, F.P. Sodium and Potassium Intake, Knowledge Attitudes and Behaviour Towards Salt Consumption Amongst Adults in Podgorica, Montenegro. Nutrients 2019, 11, 160. https://doi.org/10.3390/nu11010160
D’Elia L, Brajović M, Klisic A, Breda J, Jewell J, Cadjenović V, Cappuccio FP. Sodium and Potassium Intake, Knowledge Attitudes and Behaviour Towards Salt Consumption Amongst Adults in Podgorica, Montenegro. Nutrients. 2019; 11(1):160. https://doi.org/10.3390/nu11010160
Chicago/Turabian StyleD’Elia, Lanfranco, Mina Brajović, Aleksandra Klisic, Joao Breda, Jo Jewell, Vuk Cadjenović, and Francesco P Cappuccio. 2019. "Sodium and Potassium Intake, Knowledge Attitudes and Behaviour Towards Salt Consumption Amongst Adults in Podgorica, Montenegro" Nutrients 11, no. 1: 160. https://doi.org/10.3390/nu11010160
APA StyleD’Elia, L., Brajović, M., Klisic, A., Breda, J., Jewell, J., Cadjenović, V., & Cappuccio, F. P. (2019). Sodium and Potassium Intake, Knowledge Attitudes and Behaviour Towards Salt Consumption Amongst Adults in Podgorica, Montenegro. Nutrients, 11(1), 160. https://doi.org/10.3390/nu11010160