Breakfast Consumption in the UK: Patterns, Nutrient Intake and Diet Quality. A Study from the International Breakfast Research Initiative Group


Abstract
1. Introduction
2. Methods
2.1. Survey Sample
2.2. Dietary Assessment in NDNS
2.3. Dietary Intake at Breakfast
2.4. Diet Quality Assessment
2.5. Other Variables
2.6. Statistical Analysis
3. Results
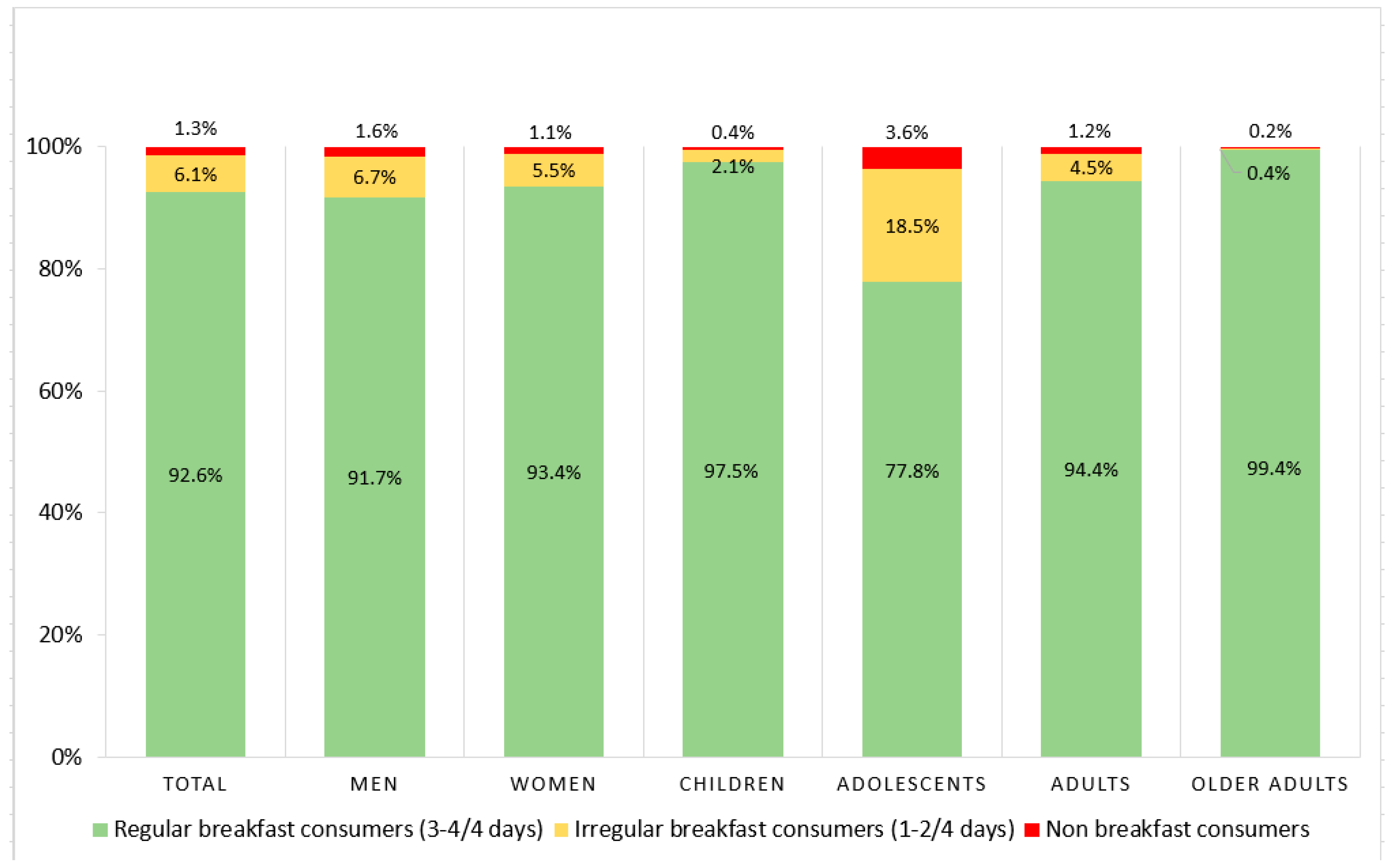
3.1. Regularity of Breakfast Consumption
3.2. Mean Energy, Macronutrient and Micronutrient Intakes Expressed as % Contribution to Breakfast and Daily Energy Intake
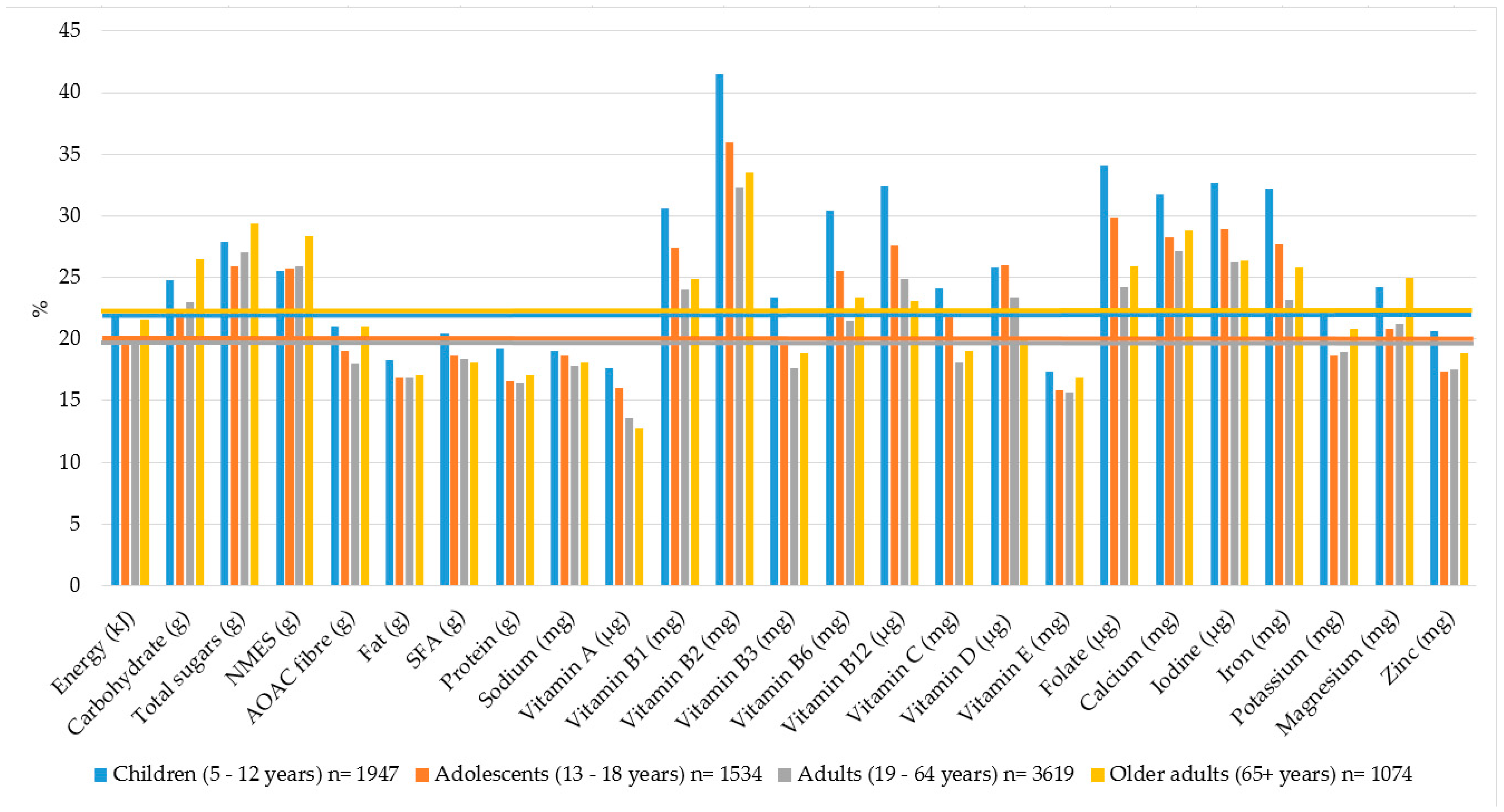
3.3. Percentage Contribution of Breakfast to Daily Energy and Nutrient Intakes
3.4. Percentage Contribution of Food Groups to Energy and Nutrient Intakes at Breakfast
3.5. Nutrient Intakes at Breakfast across Tertiles of NRF9.3 Diet Quality Score
3.6. Food Intakes at Breakfast by Tertiles of NRF 9.3 Diet Quality Score
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- De la Hunty, A.; Gibson, S.; Ashwell, M. Does regular breakfast cereal consumption help children and adolescents stay slimmer? A systematic review and meta-analysis. Obes. Facts 2013, 6, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.G. The benefits of breakfast cereal consumption: A systematic review of the evidence base. Adv. Nutr. 2014, 5, 636S–673S. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Dietrich, M.; Brown, C.J.P.; Clark, C.A.; Block, G. The effect of breakfast type on total daily energy intake and body mass index: Results from the third National Health and Nutrition Examination Survey (NHANES III). J. Am. Coll. Nutr. 2003, 22, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Ruszczynski, M. Systematic review demonstrating that breakfast consumption influences body weight outcomes in children and adolescents in Europe. Crit. Rev. Food Sci. Nutr. 2010, 50, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Cahill, L.E.; Chiuve, S.E.; Mekary, R.A.; Jensen, M.K.; Flint, A.J.; Hu, F.B.; Rimm, E.B. Prospective study of breakfast eating and incident coronary heart disease in a cohort of male US health professionals. Circulation 2013, 128, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, R.; Di Castelnuovo, A.; Melegari, C.; De Lucia, F.; Santimone, I.; Sciarretta, A.; Barisciano, P.; Persichillo, M.; De Curtis, A.; Zito, F.; et al. Typical breakfast food consumption and risk factors for cardiovascular disease in a large sample of Italian adults. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, K.; Schwingshackl, L.; Gottschald, M.; Knuppel, S.; Stelmach-Mardas, M.; Aleksandrova, K.; Boeing, H. Breakfast quality and cardiometabolic risk profiles in an upper middle-aged German population. Eur. J. Clin. Nutr. 2017, 71, 1312–1320. [Google Scholar] [CrossRef] [PubMed]
- Kubota, Y.; Iso, H.; Sawada, N.; Tsugane, S.; Group, J.S. Association of breakfast intake with incident stroke and coronary heart disease: The Japan public health center-based study. Stroke 2016, 47, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Hallstrom, L.; Labayen, I.; Ruiz, J.R.; Patterson, E.; Vereecken, C.A.; Breidenassel, C.; Gottrand, F.; Huybrechts, I.; Manios, Y.; Mistura, L.; et al. Breakfast consumption and CVD risk factors in European adolescents: The Helena (Healthy Lifestyle in Europe by Nutrition in Adolescence) study. Public Health Nutr. 2013, 16, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Hoyland, A.; Dye, L.; Lawton, C.L. A systematic review of the effect of breakfast on the cognitive performance of children and adolescents. Nutr. Res. Rev. 2009, 22, 220–243. [Google Scholar] [CrossRef] [PubMed]
- Dye, L. European Breakfast Cereal Association: The Importance of Breakfast in Europe. A Review of National Policies and Health Campaigns. Available online: http://ceereal.eu/images/publications/BIB_Report_FINAL.pdf (accessed on 10 March 2018).
- Porter, S. British Dietetic Association Healthy Breakfast Food Fact Sheet. Available online: https://www.bda.uk.com/foodfacts/healthy_breakfast (accessed on 8 March 2018).
- Crawley, H. The Caroline Walker Trust Eating Well at School. Nutritional and Practical Guidelines. Available online: http://www.cwt.org.uk/publications/ (accessed on 5 February 2018).
- Gibney, M.J.; Barr, S.I.; Bellisle, F.; Drewnowski, A.; Fagt, S.; Livingstone, B.; Masset, G.; Varela Moreiras, G.; Moreno, L.; Smith, J.; et al. Breakfast in human nutrition: The International Breakfast Research Initiative. Nutrients 2018, 10, 559. [Google Scholar] [CrossRef] [PubMed]
- Priebe, M.G.; McMonagle, J.R. Effects of ready-to-eat-cereals on key nutritional and health outcomes: A systematic review. PLoS ONE 2016, 11, e0164931. [Google Scholar] [CrossRef] [PubMed]
- Van den Boom, A.; Serra-Majem, L.; Ribas, L.; Ngo, J.; Pérez-Rodrigo, C.; Aranceta, J.; Fletcher, R. The contribution of ready-to-eat cereals to daily nutrient intake and breakfast quality in a Mediterranean setting. J. Am. Coll. Nutr. 2006, 25, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Albertson, A.M.; Wold, A.C.; Joshi, N. Ready-to-eat cereal consumption patterns: The relationship to nutrient intake, whole grain intake, and body mass index in an older American population. J. Aging Res. 2012, 2012, 631310. [Google Scholar] [CrossRef] [PubMed]
- Barr, S.I.; DiFrancesco, L.; Fulgoni, V.L., III. Consumption of breakfast and the type of breakfast consumed are positively associated with nutrient intakes and adequacy of Canadian adults. J. Nutr. 2013, 143, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Azadbakht, L.; Haghighatdoost, F.; Feizi, A.; Esmaillzadeh, A. Breakfast eating pattern and its association with dietary quality indices and anthropometric measurements in young women in Isfahan. Nutrition 2013, 29, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Min, C.; Noh, H.; Kang, Y.S.; Sim, H.J.; Baik, H.W.; Song, W.O.; Yoon, J.; Park, Y.H.; Joung, H. Skipping breakfast is associated with diet quality and metabolic syndrome risk factors of adults. Nutr. Res. Pract. 2011, 5, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Gibson, S.A.; Gunn, P. What’s for breakfast? Nutritional implications of breakfast habits: Insights from the NDNS dietary records. Nutr. Bull. 2011, 36, 78–86. [Google Scholar] [CrossRef]
- Coulthard, J.D.; Palla, L.; Pot, G.K. Breakfast consumption and nutrient intakes in 4–18-year-olds: UK national diet and nutrition survey rolling programme (2008–2012). Br. J. Nutr. 2017, 118, 280–290. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Byrd-Bredbenner, C.; Hayes, D.; Jana, L.; Klinger, S.E.; Stephenson-Martin, S. The role of breakfast in health: Definition and criteria for a quality breakfast. J. Acad. Nutr. Diet 2014, 114, S8–S26. [Google Scholar] [CrossRef] [PubMed]
- Bates, B.; Lennox, A.; Prentice, A.; Bates, C. National Diet and Nutrition Survey Results from Years 1, 2, 3 and 4 (Combined) of the Rolling Programme (2008/2009–2011/2012); Public Health England: London, UK, 2014.
- Bates, B.; Cox, L.; Page, S.N.P.; Prentice, A.; Steer, T.; Swan, G. National Diet and Nutrition Survey Results from Years 5 and 6 (Combined) of the Rolling Programme (2012/2013–2013/2014); Public Health England: London, UK, 2016.
- UK Data Archive National Diet and Nutrition Survey Years 1–6. Available online: http://www.data-archive.ac.uk/ (accessed on 4 April 2017).
- Englyst, H.N.; Quigley, M.E.; Hudson, G.J. Determination of dietary fibre as non-starch polysaccharides with gas-liquid chromatographic, high-performance liquid chromatographic or spectrophotometric measurement of constituent sugars. Analyst 1994, 119, 1497–1509. [Google Scholar] [CrossRef] [PubMed]
- Scientific Advisory Committee on Nutrition Carbohydrates and Health. Available online: https://www.gov.uk/government/publications/sacn-carbohydrates-and-health-report (accessed on 10 June 2017).
- Drewnowski, A.; Fulgoni, V.L. Nutrient profiling of foods: Creating a nutrient-rich food index. Nutr. Rev. 2008, 66, 23–39. [Google Scholar] [CrossRef] [PubMed]
- EUR-Lex Access to European Union Law: Regulation (EU) no 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the Provision of Food Information to Consumers, Amending Regulations (EC) No. 1924/2006 and (EC) No. 1925/2006 of the European Parliament and of the Council, and Repealing Commission Directive 87/250/eec, Council Directive 90/496/eec, Commission Directive 1999/10/EC, Directive 2000/13/ec of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/ec and Commission Regulation (EC) No. 608/2004 text with eea Relevance. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?qid=1527757791212&uri=CELEX:32011R1169 (accessed on 13 November 2017).
- World Health Organisation Guideline: Sugar Intake for Adults and Children. Available online: http://www.who.int/nutrition/publications/guidelines/sugars_intake/en/ (accessed on 15 November 2017).
- European Food Safety Authority Scientific Opinion on Dietary Reference Values for Carbohydrates and Dietary Fibre. Available online: https://www.efsa.europa.eu/en/efsajournal/pub/1462 (accessed on 18 November 2017).
- Office for National Statistics. The National Statistics Socio-Economic Classification (NS-SEC). Available online: https://www.ons.gov.uk/methodology/classificationsandstandards/otherclassifications/thenationalstatisticssocioeconomicclassificationnssecrebasedonsoc2010 (accessed on 14 September 2017).
- Aranceta, J.; Serra-Majem, L.; Ribas, L.; Pérez-Rodrigo, C. Breakfast consumption in Spanish children and young people. Public Health Nutr. 2001, 4, 1439–1444. [Google Scholar] [CrossRef] [PubMed]
- Barr, S.I.; DiFrancesco, L.; Fulgoni, V.L., III. Breakfast consumption is positively associated with nutrient adequacy in Canadian children and adolescents. Br. J. Nutr. 2014, 112, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- Levin, K.A.; Kirby, J. Irregular breakfast consumption in adolescence and the family environment: Underlying causes by family structure. Appetite 2012, 59, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Hallstrom, L.; Vereecken, C.A.; Ruiz, J.R.; Patterson, E.; Gilbert, C.C.; Catasta, G.; Diaz, L.E.; Gomez-Martinez, S.; Gonzalez Gross, M.; Gottrand, F.; et al. Breakfast habits and factors influencing food choices at breakfast in relation to socio-demographic and family factors among European adolescents. The Helena study. Appetite 2011, 56, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.; Dupuy, M.; Rasmussen, M.; Kelly, C.; Nansel, T.R.; Al Sabbah, H.; Baldassari, D.; Jordan, M.D.; Maes, L.; Niclasen, B.V.; et al. Breakfast consumption and its socio-demographic and lifestyle correlates in schoolchildren in 41 countries participating in the HBSC study. Int. J. Public Health 2009, 54 (Suppl. 2), 180–190. [Google Scholar] [CrossRef] [PubMed]
- Wijtzes, A.I.; Jansen, W.; Jaddoe, V.W.; Franco, O.H.; Hofman, A.; van Lenthe, F.J.; Raat, H. Social inequalities in young children’s meal skipping behaviors: The generation r study. PLoS ONE 2015, 10, e0134487. [Google Scholar] [CrossRef] [PubMed]
- Bruening, M.; Larson, N.; Story, M.; Neumark-Sztainer, D.; Hannan, P. Predictors of adolescent breakfast consumption: Longitudinal findings from project EAT. J. Nutr. Educ. Behav. 2011, 43, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, G.R.; Voss, C.; Dye, L. Associations between habitual school-day breakfast consumption, body mass index, physical activity and cardiorespiratory fitness in English schoolchildren. Eur. J. Clin. Nutr. 2010, 64, 1086–1092. [Google Scholar] [CrossRef] [PubMed]
- Tedstone, A.; Coulton, V.; Targett, V.; Bennett, A.; Sweeney, K.; Morgan, K.; Clegg, E.; Robinson, M.; Dowd, L.; Knowles, B.; et al. Sugar Reduction and Wider Reformulation Programme: Report on Progress Towards the First 5% Reduction and Next Steps; Public Health England: London, UK, 2018.
- Maki, K.C.; Phillips-Eakley, A.K.; Smith, K.N. The effects of breakfast consumption and composition on metabolic wellness with a focus on carbohydrate metabolism. Adv. Nutr. 2016, 7, 613S–621S. [Google Scholar] [CrossRef] [PubMed]
- Galioto, R.; Spitznagel, M.B. The effects of breakfast and breakfast composition on cognition in adults. Adv. Nutr. 2016, 7, 576S–589S. [Google Scholar] [CrossRef] [PubMed]
- Blom, W.A.M.; Lluch, A.; Stafleu, A.; Vinoy, S.; Holst, J.J.; Schaafsma, G.; Hendriks, H.F.J. Effect of a high-protein breakfast on the postprandial ghrelin response. Am. J. Clin. Nutr. 2006, 83, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Bush, N.C.; Resuehr, H.E.S.; Goree, L.L.; Locher, J.L.; Bray, M.S.; Soleymani, T.; Gower, B.A. A high-fat compared with a high-carbohydrate breakfast enhances 24-hour fat oxidation in older adults. J. Nutr. 2018, 148, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Ashcroft, J.; Semmler, C.; Carnell, S.; van Jaarsveld, C.H.; Wardle, J. Continuity and stability of eating behaviour traits in children. Eur. J. Clin. Nutr. 2008, 62, 985–990. [Google Scholar] [CrossRef] [PubMed]
- British Nutrition Foundation Fortification. Available online: https://www.nutrition.org.uk/nutritionscience/foodfacts/fortification.html (accessed on 15 January 2018).
- Fayet-Moore, F.; McConnell, A.; Tuck, K.; Petocz, P. Breakfast and breakfast cereal choice and its impact on nutrient and sugar intakes and anthropometric measures among a nationally representative sample of Australian children and adolescents. Nutrients 2017, 9, 1045. [Google Scholar] [CrossRef] [PubMed]
- Holmes, B.A.; Kaffa, N.; Campbell, K.; Sanders, T.A. The contribution of breakfast cereals to the nutritional intake of the materially deprived UK population. Eur. J. Clin. Nutr. 2012, 66, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.M.; O’Neil, C.E.; Keast, D.R.; Cho, S.; Nicklas, T.A. Ready-to-eat cereal breakfasts are associated with improved nutrient intake and dietary adequacy but not body mass index in black adolescents. Am. J. Lifestyle Med. 2009, 3, 500–508. [Google Scholar] [CrossRef]
- Galvin, M.A.; Kiely, M.; Flynn, A. Impact of ready-to-eat breakfast cereal (RTEBC) consumption on adequacy of micronutrient intakes and compliance with dietary recommendations in Irish adults. Public Health Nutr. 2002, 6, 351–363. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Nicklas, T.A.; Fulgoni, V.L., III. Nutrient intake, diet quality, and weight/adiposity parameters in breakfast patterns compared with no breakfast in adults: National Health and Nutrition Examination Survey 2001–2008. J. Acad. Nutr. Diet 2014, 114, S27–S43. [Google Scholar] [CrossRef] [PubMed]
- Widaman, A.M.; Witbracht, M.G.; Forester, S.M.; Laugero, K.D.; Keim, N.L. Chronic stress is associated with indicators of diet quality in habitual breakfast skippers. J. Acad. Nutr. Diet. 2016, 116, 1776–1784. [Google Scholar] [CrossRef] [PubMed]
- Hearty, A.P.; Gibney, M.J. Analysis of meal patterns with the use of supervised data mining techniques--artificial neural networks and decision trees. Am. J. Clin. Nutr. 2008, 88, 1632–1642. [Google Scholar] [CrossRef] [PubMed]
- Woolhead, C.; Gibney, M.J.; Walsh, M.C.; Brennan, L.; Gibney, E.R. A generic coding approach for the examination of meal patterns. Am. J. Clin. Nutr. 2015, 102, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 hour recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101 (Suppl. 2), S73–S85. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Population (n = 8174) | Children 5–12 years (n = 1947) | Adolescents 13–18 years (n = 1534) | Adults 19–64 years (n = 3619) | Older Adults 65+ Years (n = 1074) | p Value * | p Value ** | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | |||||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Energy (kJ) | 1442 | 721 | 7062 | 2049 | 1450 | 541 | 6664 | 1489 | 1471 | 773 | 7518 | 2202 | 1425 | 795 | 7193 | 2223 | 1444 | 668 | 6690 | 1895 | ˂0.001 | ˂0.001 |
| Carbohydrates (g) | 52 | 25 | 220 | 68 | 54 | 19 | 218 | 51 | 54 | 27 | 242 | 74 | 50 | 26 | 218 | 72 | 53 | 25 | 201 | 62 | ˂0.001 | ˂0.001 |
| Carbohydrates (% E) | 59 | 13 | 49 | 6 | 60 | 10 | 52 | 5 | 60 | 13 | 51 | 6 | 58 | 14 | 48 | 7 | 59 | 12 | 47 | 6 | ˂0.001 | ˂0.001 |
| Total sugars (g) | 26 | 16 | 96 | 42 | 27 | 13 | 99 | 35 | 26 | 17 | 105 | 47 | 24 | 16 | 93 | 44 | 26 | 16 | 89 | 38 | ˂0.001 | ˂0.001 |
| Total sugars (% E) | 30 | 15 | 21 | 7 | 30 | 11 | 23 | 6 | 30 | 16 | 22 | 7 | 30 | 16 | 20 | 7 | 30 | 14 | 21 | 6 | 0.009 | ˂0.001 |
| NMES (g) | 15 | 13 | 60 | 38 | 16 | 11 | 63 | 30 | 18 | 15 | 76 | 42 | 14 | 12 | 56 | 39 | 14 | 12 | 48 | 30 | ˂0.001 | ˂0.001 |
| NMES (% E) | 17 | 14 | 13 | 6 | 17 | 10 | 15 | 6 | 21 | 15 | 16 | 7 | 17 | 15 | 12 | 7 | 15 | 12 | 11 | 5 | ˂0.001 | ˂0.001 |
| AOAC fibre (g) | 3 | 2 | 17 | 6 | 3 | 2 | 15 | 4 | 3 | 2 | 16 | 5 | 3 | 3 | 18 | 7 | 4 | 3 | 18 | 6 | ˂0.001 | ˂0.001 |
| Fat (g) | 11 | 9 | 65 | 24 | 11 | 6 | 59 | 17 | 11 | 9 | 68 | 24 | 11 | 9 | 67 | 26 | 11 | 8 | 63 | 23 | 0.007 | ˂0.001 |
| Fat (% E) | 28 | 11 | 34 | 6 | 27 | 9 | 34 | 5 | 28 | 12 | 34 | 5 | 28 | 12 | 35 | 6 | 27 | 12 | 35 | 6 | 0.104 | ˂0.001 |
| SFA (g) | 5 | 4 | 24 | 10 | 5 | 3 | 23 | 8 | 5 | 4 | 25 | 10 | 5 | 4 | 25 | 11 | 4 | 4 | 25 | 10 | ˂0.001 | ˂0.001 |
| SFA (% E) | 12 | 6 | 13 | 3 | 12 | 5 | 13 | 3 | 11 | 5 | 13 | 3 | 11 | 6 | 13 | 3 | 11 | 6 | 14 | 4 | ˂0.001 | ˂0.001 |
| Protein (g) | 12 | 7 | 67 | 22 | 11 | 5 | 58 | 14 | 11 | 8 | 67 | 23 | 12 | 8 | 72 | 23 | 12 | 6 | 68 | 19 | ˂0.001 | ˂0.001 |
| Protein (% E) | 14 | 5 | 16 | 4 | 13 | 3 | 15 | 2 | 13 | 5 | 15 | 3 | 14 | 6 | 17 | 4 | 14 | 5 | 17 | 3 | ˂0.001 | ˂0.001 |
| Total Population (n = 8174) | Children 5–12 years (n = 1947) | Adolescents 13–18 years (n = 1534) | Adults 19–64 years (n = 3619) | Older Adults 65+ Years (n = 1074) | p Value * | p Value ** | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | |||||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Vitamin A (µg) | 100 | 201 | 826 | 844 | 99 | 126 | 627 | 445 | 92 | 212 | 650 | 502 | 102 | 228 | 907 | 872 | 107 | 194 | 1166 | 1374 | ˂0.001 | ˂0.001 |
| Vitamin B1 (mg) | 0.4 | 0.2 | 1.4 | 0.5 | 0.4 | 0.2 | 1.3 | 0.4 | 0.4 | 0.3 | 1.4 | 0.5 | 0.4 | 0.3 | 1.4 | 0.5 | 0.4 | 0.2 | 1.4 | 0.5 | ˂0.001 | ˂0.001 |
| Vitamin B2 (mg) | 0.6 | 0.4 | 1.5 | 0.6 | 0.6 | 0.3 | 1.5 | 0.6 | 0.5 | 0.4 | 1.5 | 0.7 | 0.5 | 0.4 | 1.6 | 0.7 | 0.6 | 0.3 | 1.6 | 0.6 | ˂0.001 | ˂0.001 |
| Vitamin B3 (mg) | 6 | 4 | 32 | 12 | 6 | 3 | 28 | 8 | 7 | 5 | 33 | 13 | 6 | 5 | 35 | 13 | 6 | 3 | 31 | 10 | ˂0.001 | ˂0.001 |
| Vitamin B6 (mg) | 0.5 | 0.4 | 2.0 | 1.0 | 0.5 | 0.3 | 1.8 | 0.7 | 0.5 | 0.5 | 2.1 | 1.2 | 0.5 | 0.4 | 2.1 | 1.1 | 0.5 | 0.4 | 2.0 | 0.8 | ˂0.001 | ˂0.001 |
| Vitamin B12 (µg) | 1.2 | 1.1 | 4.8 | 3.2 | 1.3 | 0.8 | 4.1 | 1.8 | 1.1 | 1.0 | 4.2 | 2.5 | 1.2 | 1.3 | 5.0 | 3.4 | 1.2 | 1.0 | 6.0 | 4.5 | ˂0.001 | ˂0.001 |
| Vitamin C (mg) | 18 | 24 | 80 | 54 | 22 | 22 | 84 | 49 | 19 | 26 | 78 | 55 | 17 | 25 | 79 | 58 | 17 | 22 | 77 | 48 | ˂0.001 | ˂0.001 |
| Vitamin D (µg) | 0.6 | 0.8 | 2.6 | 1.8 | 0.6 | 0.6 | 2.0 | 1.2 | 0.6 | 0.8 | 2.2 | 1.4 | 0.7 | 0.9 | 2.8 | 2.0 | 0.7 | 0.9 | 3.3 | 2.3 | 0.003 | ˂0.001 |
| Vitamin E (mg) | 1.4 | 1.9 | 8.6 | 3.8 | 1.3 | 0.9 | 7.4 | 2.6 | 1.4 | 1.7 | 8.9 | 3.8 | 1.5 | 2.4 | 9.1 | 4.2 | 1.4 | 1.2 | 8.3 | 3.5 | 0.005 | ˂0.001 |
| Folate (µg) | 64 | 46 | 227 | 94 | 69 | 39 | 196 | 68 | 65 | 49 | 210 | 86 | 62 | 48 | 246 | 102 | 66 | 47 | 245 | 94 | ˂0.001 | ˂0.001 |
| Calcium (mg) | 229 | 138 | 801 | 307 | 258 | 139 | 808 | 283 | 218 | 145 | 784 | 337 | 217 | 135 | 802 | 310 | 232 | 129 | 811 | 292 | ˂0.001 | ˂0.001 |
| Iodine (µg) | 41 | 30 | 151 | 78 | 45 | 30 | 136 | 64 | 36 | 31 | 127 | 76 | 41 | 28 | 160 | 79 | 46 | 29 | 180 | 86 | ˂0.001 | ˂0.001 |
| Iron (mg) | 2.7 | 1.8 | 9.8 | 3.4 | 2.9 | 1.6 | 8.8 | 2.5 | 2.8 | 2.0 | 9.6 | 3.4 | 2.5 | 1.8 | 10.3 | 3.6 | 2.6 | 1.7 | 9.9 | 3.3 | ˂0.001 | ˂0.001 |
| Potassium (mg) | 506 | 283 | 2534 | 808 | 491 | 223 | 2194 | 546 | 435 | 257 | 2345 | 755 | 525 | 310 | 2742 | 867 | 573 | 301 | 2719 | 801 | ˂0.001 | ˂0.001 |
| Magnesium (mg) | 51 | 31 | 227 | 79 | 48 | 22 | 195 | 50 | 44 | 26 | 211 | 69 | 54 | 34 | 250 | 88 | 60 | 32 | 236 | 77 | ˂0.001 | ˂0.001 |
| Sodium (mg) | 388 | 316 | 2107 | 756 | 357 | 219 | 1895 | 551 | 420 | 343 | 2232 | 778 | 396 | 350 | 2199 | 822 | 368 | 294 | 2002 | 719 | ˂0.001 | ˂0.001 |
| Zinc (mg) | 1.4 | 0.9 | 7.7 | 2.8 | 1.3 | 0.7 | 6.6 | 2.0 | 1.3 | 0.9 | 7.5 | 2.7 | 1.5 | 1.0 | 8.3 | 3.0 | 1.5 | 0.8 | 8.1 | 2.6 | ˂0.001 | ˂0.001 |
| Children (5–17 years) (n = 3283) | Adults (18+ Years) (n = 4891) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 (n = 1094) | T2 (n = 1095) | T3 (n = 1094) | T1 (n = 1630) | T2 (n = 1631) | T3 (n = 1630) | |||||||||||
| Mean | SD | Mean | SD | Mean | SD | p Value * | p Value ** | Mean | SD | Mean | SD | Mean | SD | p Value * | p Value ** | |
| NRF 9.3 score | 483 | 68 | 608 | 26 | 717 | 49 | ˂0.001 | ˂0.001 | 523 | 86 | 672 | 30 | 788 | 44 | ˂0.001 | ˂0.001 |
| Energy (kJ) ‡ | 1518 | 738 | 1452 | 615 | 1439 | 575 | 0.156 | 0.113 | 1452 | 858 | 1443 | 756 | 1375 | 673 | 0.204 | 0.057 |
| Carbohydrates (g) ‡ | 55 | 26 | 53 | 22 | 54 | 21 | 0.491 | 0.399 | 49 | 27 | 50 | 26 | 52 | 25 | 0.001 | 0.076 |
| Carbohydrates (% E) ‡ | 59 | 12 | 60 | 11 | 61 | 10 | 0.002 | 0.003 | 57 | 15 | 57 | 13 | 61 | 12 | ˂0.001 | ˂0.001 |
| Total sugars (g) ‡ | 29 | 18 | 26 | 15 | 25 | 13 | ˂0.001 | ˂0.001 | 26 | 17 | 23 | 16 | 25 | 15 | ˂0.001 | ˂0.001 |
| Total sugars (% E) ‡ | 32 | 15 | 30 | 13 | 29 | 12 | ˂0.001 | ˂0.001 | 33 | 20 | 27 | 14 | 30 | 14 | ˂0.001 | ˂0.001 |
| NMES (g) ‡ | 21 | 16 | 16 | 12 | 13 | 9 | ˂0.001 | ˂0.001 | 18 | 15 | 13 | 11 | 11 | 9 | ˂0.001 | ˂0.001 |
| NMES (% E) ‡ | 23 | 15 | 18 | 12 | 14 | 9 | ˂0.001 | ˂0.001 | 23 | 19 | 14 | 12 | 12 | 10 | ˂0.001 | ˂0.001 |
| AOAC fibre (g) ‡ | 2.5 | 1.9 | 3.0 | 1.8 | 3.7 | 2.2 | ˂0.001 | ˂0.001 | 2.4 | 2.0 | 3.5 | 2.5 | 4.6 | 3.0 | ˂0.001 | ˂0.001 |
| Fat (g) ‡ | 12 | 9 | 11 | 7 | 10 | 6 | ˂0.001 | ˂0.001 | 13 | 11 | 12 | 9 | 9 | 7 | ˂0.001 | ˂0.001 |
| Fat (% E) ‡ | 29 | 11 | 28 | 10 | 25 | 10 | ˂0.001 | ˂0.001 | 30 | 13 | 29 | 12 | 24 | 10 | ˂0.001 | ˂0.001 |
| SFA (g) ‡ | 5 | 4 | 5 | 3 | 4 | 3 | ˂0.001 | ˂0.001 | 6 | 5 | 5 | 4 | 3 | 3 | ˂0.001 | ˂0.001 |
| SFA (% E) ‡ | 13 | 6 | 12 | 5 | 11 | 4 | ˂0.001 | ˂0.001 | 13 | 7 | 12 | 6 | 9 | 4 | ˂0.001 | ˂0.001 |
| Protein (g) ‡ | 11 | 7 | 11 | 6 | 12 | 6 | ˂0.001 | ˂0.001 | 11 | 8 | 12 | 8 | 12 | 7 | ˂0.001 | ˂0.001 |
| Protein (% E) ‡ | 12 | 4 | 13 | 4 | 14 | 4 | ˂0.001 | ˂0.001 | 12 | 6 | 14 | 5 | 16 | 5 | ˂0.001 | ˂0.001 |
| Children (5–17 years) (n = 3283) | Adults (18+ Years) (n = 4891) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 (n = 1094) | T2 (n = 1095) | T3 (n = 1094) | T1 (n = 1630) | T2 (n = 1631) | T3 (n = 1630) | |||||||||||
| Mean | SD | Mean | SD | Mean | SD | p Value * | p Value ** | Mean | SD | Mean | SD | Mean | SD | p Value * | p Value ** | |
| Vitamin A (µg) | 90 | 143 | 96 | 136 | 107 | 227 | 0.001 | 0.001 | 98 | 135 | 109 | 192 | 97 | 293 | ˂0.001 | 0.001 |
| Vitamin B1 (mg) | 0.4 | 0.2 | 0.4 | 0.2 | 0.4 | 0.2 | ˂0.001 | ˂0.001 | 0.3 | 0.2 | 0.4 | 0.2 | 0.4 | 0.3 | ˂0.001 | ˂0.001 |
| Vitamin B2 (mg) | 0.5 | 0.4 | 0.6 | 0.3 | 0.7 | 0.4 | ˂0.001 | ˂0.001 | 0.4 | 0.4 | 0.5 | 0.4 | 0.6 | 0.4 | ˂0.001 | ˂0.001 |
| Vitamin B3 (mg) | 6 | 4 | 6 | 3 | 7 | 4 | ˂0.001 | ˂0.001 | 5 | 5 | 6 | 4 | 7 | 4 | ˂0.001 | ˂0.001 |
| Vitamin B6 (mg) | 0.5 | 0.5 | 0.5 | 0.3 | 0.6 | 0.4 | ˂0.001 | ˂0.001 | 0.4 | 0.5 | 0.5 | 0.4 | 0.5 | 0.4 | ˂0.001 | ˂0.001 |
| Vitamin B12 (µg) | 1.1 | 0.9 | 1.2 | 0.9 | 1.4 | 1.0 | ˂0.001 | ˂0.001 | 1.1 | 1.1 | 1.2 | 1.0 | 1.3 | 1.4 | ˂0.001 | ˂0.001 |
| Vitamin C (mg) | 18 | 23 | 22 | 24 | 22 | 24 | ˂0.001 | ˂0.001 | 11 | 18 | 16 | 24 | 23 | 27 | ˂0.001 | ˂0.001 |
| Vitamin D (µg) | 0.5 | 0.6 | 0.6 | 0.7 | 0.7 | 0.8 | ˂0.001 | ˂0.001 | 0.5 | 0.7 | 0.7 | 0.9 | 0.8 | 0.9 | ˂0.001 | ˂0.001 |
| Vitamin E (mg) | 1.3 | 1.7 | 1.3 | 1.0 | 1.4 | 1.2 | ˂0.001 | ˂0.001 | 1.2 | 1.2 | 1.5 | 1.4 | 1.7 | 3.2 | ˂0.001 | ˂0.001 |
| Folate (µg) | 56 | 39 | 67 | 40 | 79 | 44 | ˂0.001 | ˂0.001 | 47 | 41 | 64 | 52 | 76 | 48 | ˂0.001 | ˂0.001 |
| Calcium (mg) | 226 | 140 | 244 | 145 | 260 | 142 | ˂0.001 | ˂0.001 | 201 | 135 | 224 | 137 | 232 | 128 | ˂0.001 | ˂0.001 |
| Iodine (µg) | 35 | 28 | 41 | 29 | 48 | 34 | ˂0.001 | ˂0.001 | 36 | 27 | 42 | 29 | 46 | 29 | ˂0.001 | ˂0.001 |
| Iron (mg) | 2.5 | 1.6 | 2.9 | 1.7 | 3.3 | 1.8 | ˂0.001 | ˂0.001 | 2.0 | 1.6 | 2.5 | 1.8 | 3.0 | 1.8 | ˂0.001 | ˂0.001 |
| Potassium (mg) | 419 | 231 | 470 | 230 | 523 | 243 | ˂0.001 | ˂0.001 | 420 | 249 | 535 | 308 | 637 | 322 | ˂0.001 | ˂0.001 |
| Magnesium (mg) | 41 | 22 | 46 | 23 | 53 | 26 | ˂0.001 | ˂0.001 | 41 | 25 | 54 | 32 | 68 | 38 | ˂0.001 | ˂0.001 |
| Sodium (mg) | 420 | 338 | 378 | 263 | 356 | 219 | ˂0.001 | 0.001 | 424 | 398 | 409 | 334 | 337 | 262 | ˂0.001 | ˂0.001 |
| Zinc (mg) | 1.2 | 0.8 | 1.3 | 0.7 | 1.5 | 0.8 | ˂0.001 | ˂0.001 | 1.3 | 0.9 | 1.5 | 0.9 | 1.6 | 1.1 | ˂0.001 | ˂0.001 |
| Children and Adolescents (5–17) years (n = 3283) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 (n = 1094) | T2 (n = 1095) | T3 (n = 1094) | |||||||||
| Mean | SD | % Consumers | Mean | SD | % Consumers | Mean | SD | % Consumers | p Value * | p Value ** | |
| Tea coffee and water (mL) | 146.9 | 165 | 57 | 152 | 168 | 61 | 163.5 | 174 | 66 | 0.323 | 0.541 |
| Semi skimmed milk (mL) | 74.4 | 95 | 54 | 90.2 | 96 | 64 | 104.2 | 102 | 66 | ˂0.001 | ˂0.001 |
| Sugar preserves and sweet spreads (g) | 6.6 | 10 | 46 | 6.4 | 11 | 46 | 5.4 | 10 | 43 | 0.001 | 0.001 |
| High-fibre breakfast cereals (g) | 13.7 | 30 | 31 | 22 | 36 | 46 | 28.2 | 38 | 57 | 0.001 | 0.001 |
| White bread (g) | 30.7 | 36 | 53 | 25.2 | 32 | 47 | 22.4 | 33 | 40 | 0.020 | 0.036 |
| Fruit (g) | 23.6 | 54 | 23 | 42 | 61 | 42 | 54.7 | 63 | 53 | 0.327 | 0.331 |
| Other breakfast cereals (g) | 15.9 | 21 | 45 | 16.5 | 20 | 49 | 17.3 | 21 | 51 | 0.225 | 0.385 |
| Reduced fat spread (g) | 3.5 | 6 | 28 | 4 | 7 | 34 | 4 | 7 | 34 | 0.207 | 0.531 |
| Fruit juice (mL) | 60.8 | 110 | 28 | 69.3 | 105 | 35 | 58.6 | 97 | 32 | 0.016 | 0.025 |
| Biscuits (g) | 9.2 | 19 | 27 | 8.1 | 16 | 27 | 6.4 | 14 | 23 | 0.006 | 0.008 |
| Whole milk (mL) | 40.3 | 83 | 26 | 40.3 | 83 | 25 | 41.5 | 83 | 25 | 0.237 | 0.279 |
| Eggs and egg dishes (g) | 8.5 | 27 | 12 | 12 | 32 | 16 | 13 | 33 | 17 | 0.561 | 0.513 |
| Miscellaneous (g) | 4.3 | 18 | 19 | 3.3 | 18 | 16 | 3.6 | 24 | 17 | 0.003 | 0.006 |
| Butter (g) | 2.7 | 7 | 18 | 2.1 | 6 | 16 | 1.5 | 5 | 12 | 0.002 | 0.003 |
| Bacon and ham (g) | 9.0 | 22 | 18 | 6.1 | 17 | 14 | 4.5 | 15 | 10 | 0.152 | 0.265 |
| Brown granary and wheatgerm bread (g) | 5.6 | 19 | 9 | 8 | 22 | 15 | 9.4 | 23 | 17 | 0.172 | 0.236 |
| Buns, cakes, pastries & fruit pies (g) | 11.2 | 28 | 17 | 14 | 33 | 21 | 7.9 | 22 | 14 | 0.023 | 0.036 |
| Wholemeal bread (g) | 3.1 | 15 | 5 | 4.7 | 16 | 10 | 7.9 | 20 | 16 | 0.002 | 0.005 |
| Soft drinks not low calorie (mL) | 105.9 | 166 | 36 | 49.1 | 115 | 19 | 26.1 | 86 | 11 | ˂0.001 | 0.001 |
| Soft drinks low calorie (mL) | 53.4 | 114 | 21 | 59.4 | 122 | 23 | 61 | 123 | 24 | 0.923 | 0.602 |
| Adults (18+ Years) (n= 4891) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 (n = 1630) | T2 (n = 1631) | T3 (n = 1630) | |||||||||
| Mean | SD | % Consumers | Mean | SD | % Consumers | Mean | SD | % Consumers | p Value * | p Value ** | |
| Tea coffee and water (mL) | 366.5 | 226 | 92 | 402.1 | 217 | 97 | 466.5 | 242 | 98 | ˂0.001 | ˂0.001 |
| Semi skimmed milk (mL) | 56.6 | 73 | 62 | 72.1 | 83 | 69 | 76.3 | 81 | 69 | ˂0.001 | ˂0.001 |
| Sugar preserves and sweet spreads (g) | 10.9 | 12 | 67 | 8.1 | 10 | 56 | 6.7 | 10 | 47 | ˂0.001 | ˂0.001 |
| High-fibre breakfast cereals (g) | 15.9 | 38 | 26 | 27.6 | 49 | 44 | 34.9 | 47 | 58 | 0.923 | 0.818 |
| White bread (g) | 30.2 | 37 | 50 | 25.7 | 34 | 44 | 13.4 | 28 | 24 | 0.032 | 0.078 |
| Fruit (g) | 23.1 | 53 | 22 | 43.2 | 67 | 42 | 70 | 83 | 61 | ˂0.001 | ˂0.001 |
| Other breakfast cereals (g) | 9.4 | 18 | 26 | 9.9 | 18 | 29 | 9.4 | 17 | 28 | 0.003 | 0.002 |
| Reduced fat spread (g) | 4.7 | 8 | 32 | 4.6 | 8 | 33 | 3.4 | 6 | 28 | ˂0.001 | ˂0.001 |
| Fruit juice (mL) | 30.5 | 86 | 14 | 41.7 | 93 | 21 | 41.5 | 87 | 24 | ˂0.001 | ˂0.001 |
| Biscuits (g) | 7.2 | 17 | 22 | 7 | 16 | 23 | 5.6 | 12 | 22 | ˂0.001 | ˂0.001 |
| Whole milk (mL) | 28.7 | 69 | 27 | 20.4 | 61 | 18 | 8.2 | 36 | 8 | 0.766 | 0.853 |
| Eggs and egg dishes (g) | 14.4 | 36 | 17 | 16.9 | 37 | 21 | 20.2 | 41 | 23 | 0.525 | 0.306 |
| Miscellaneous (g) | 6.3 | 33 | 17 | 5.1 | 30 | 17 | 4.4 | 25 | 20 | ˂0.001 | ˂0.001 |
| Butter (g) | 4.0 | 8 | 24 | 3.4 | 7 | 22 | 1.4 | 4 | 12 | ˂0.001 | ˂0.001 |
| Bacon and ham (g) | 10.9 | 25 | 20 | 9.9 | 24 | 19 | 5.9 | 18 | 12 | 0.031 | 0.026 |
| Brown granary and wheatgerm bread (g) | 6.9 | 21 | 12 | 9.3 | 23 | 17 | 11 | 24 | 20 | 0.102 | 0.141 |
| Buns, cakes, pastries & fruit pies (g) | 11.5 | 30 | 16 | 8.9 | 25 | 14 | 5.8 | 19 | 10 | ˂0.001 | ˂0.001 |
| Wholemeal bread (g) | 5.7 | 19 | 10 | 9.9 | 24 | 18 | 13.6 | 27 | 26 | 0.157 | 0.272 |
| Soft drinks not low calorie (mL) | 59.1 | 153 | 16 | 20.7 | 86 | 7 | 13.6 | 65 | 6 | ˂0.001 | ˂0.001 |
| Soft drinks low calorie (mL) | 35.2 | 129 | 9 | 24.5 | 102 | 6 | 22.5 | 96 | 7 | 0.021 | 0.017 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaal, S.; Kerr, M.A.; Ward, M.; McNulty, H.; Livingstone, M.B.E. Breakfast Consumption in the UK: Patterns, Nutrient Intake and Diet Quality. A Study from the International Breakfast Research Initiative Group. Nutrients 2018, 10, 999. https://doi.org/10.3390/nu10080999
Gaal S, Kerr MA, Ward M, McNulty H, Livingstone MBE. Breakfast Consumption in the UK: Patterns, Nutrient Intake and Diet Quality. A Study from the International Breakfast Research Initiative Group. Nutrients. 2018; 10(8):999. https://doi.org/10.3390/nu10080999
Chicago/Turabian StyleGaal, Szilvia, Maeve A. Kerr, Mary Ward, Helene McNulty, and M. Barbara E. Livingstone. 2018. "Breakfast Consumption in the UK: Patterns, Nutrient Intake and Diet Quality. A Study from the International Breakfast Research Initiative Group" Nutrients 10, no. 8: 999. https://doi.org/10.3390/nu10080999
APA StyleGaal, S., Kerr, M. A., Ward, M., McNulty, H., & Livingstone, M. B. E. (2018). Breakfast Consumption in the UK: Patterns, Nutrient Intake and Diet Quality. A Study from the International Breakfast Research Initiative Group. Nutrients, 10(8), 999. https://doi.org/10.3390/nu10080999