Differences over 12 Years in Food Portion Size and Association with Excess Body Weight in the City of São Paulo, Brazil



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Food Grouping
2.4. Portion Size, Energy Density, and Energy Intake/Estimated Energy Requirement Ratio
2.5. Statistical Analysis
3. Results
3.1. Survey Participant Characteristics
3.2. Food Groupings Portion Sizes and Frequency of Intake
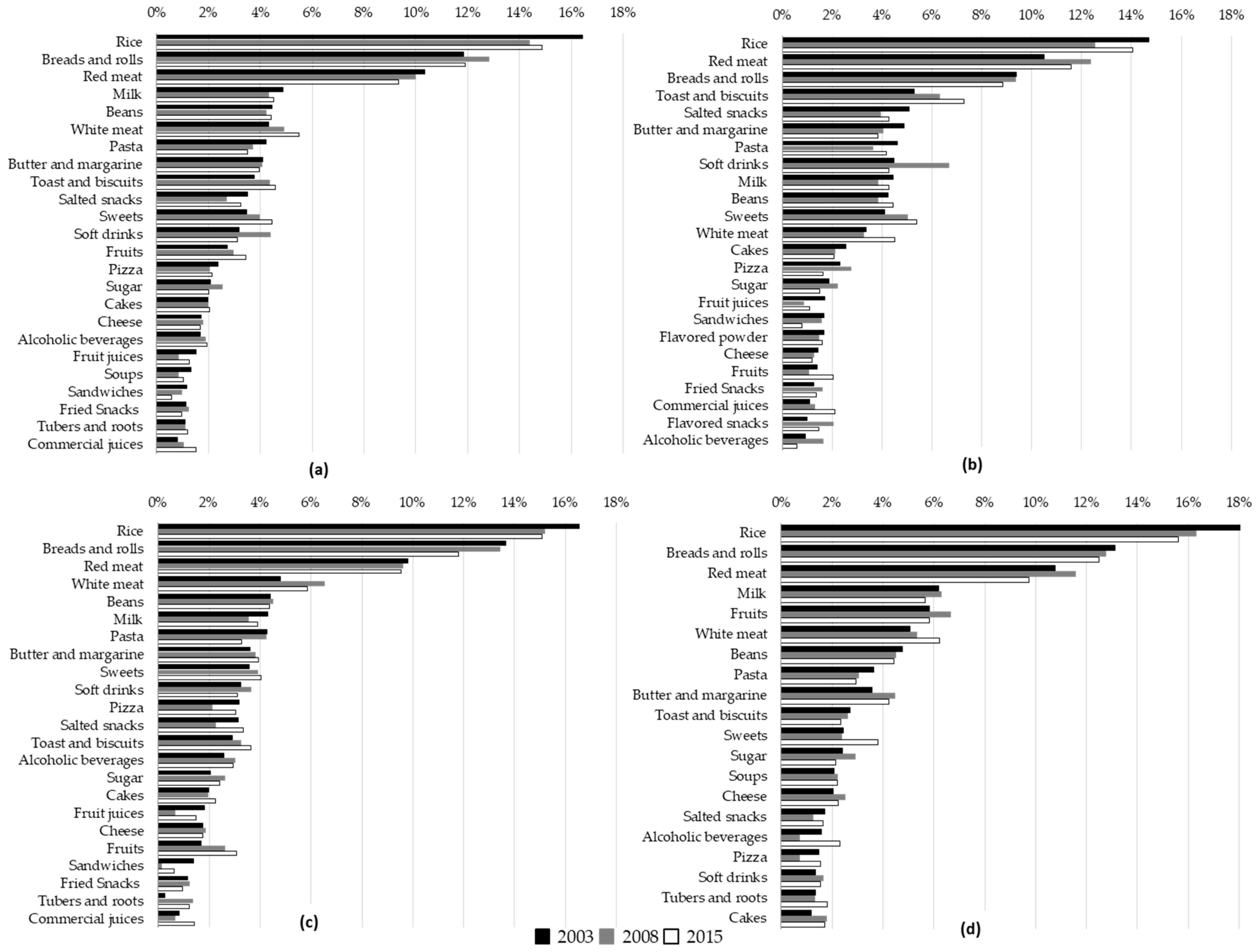
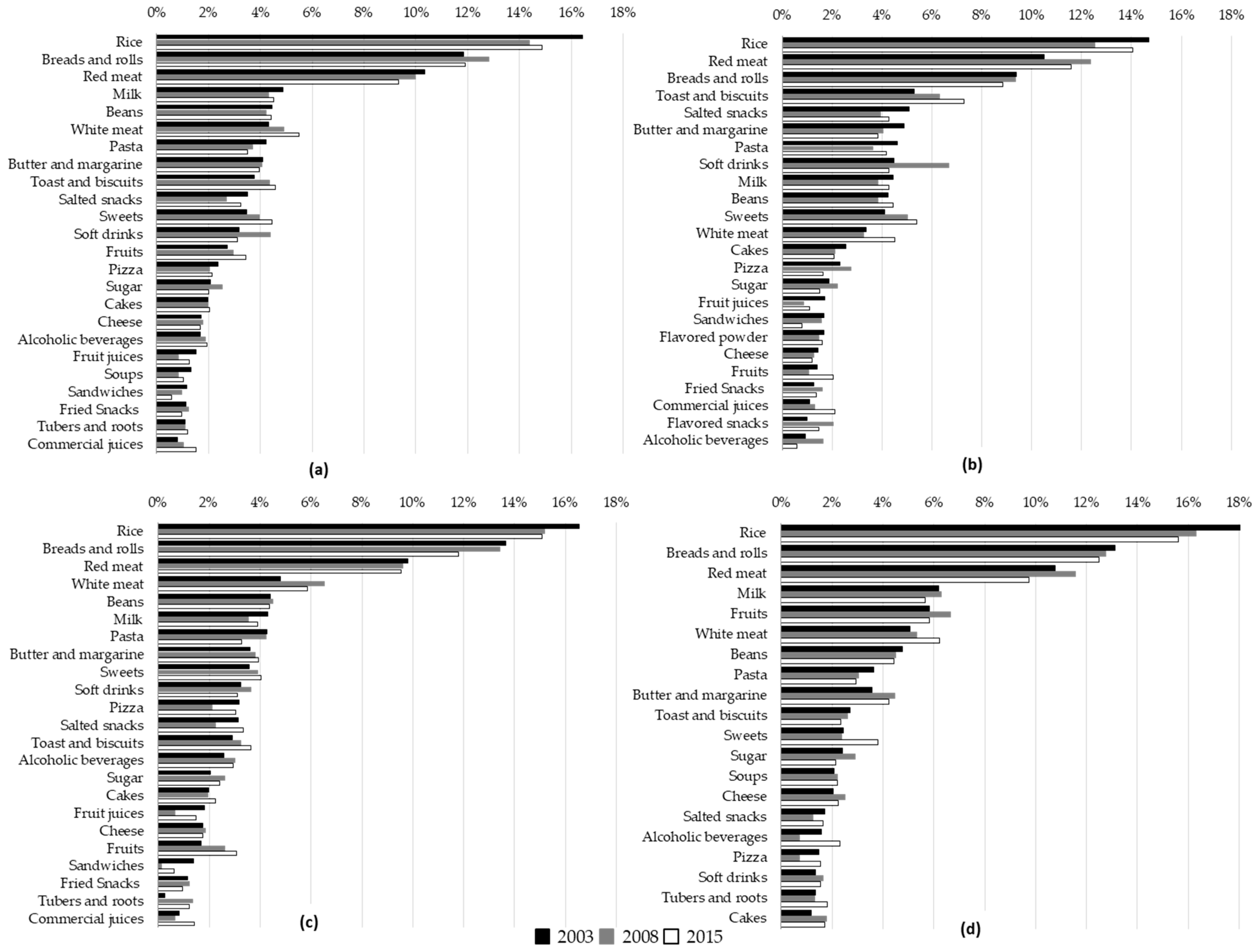
3.3. Food Groupings Contribution to Total Energy Intake
3.4. Association with Excess Body Weight
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Livingstone, M.B.E.; Pourshahidi, L.K. Portion Size and Obesity. Adv. Nutr. 2014, 5, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Ledikwe, J.H.; Ello-Martin, J.A.; Rolls, B.J. Portion sizes and the obesity epidemic. J. Nutr. 2005, 135, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Young, L.R.; Nestle, M. The contribution of expanding portion sizes to the US obesity epidemic. Am. J. Public Health 2002, 246–249. [Google Scholar] [CrossRef]
- Matthiessen, J.; Fagt, S.; Biltoft-Jensen, A.; Beck, A.M.; Ovesen, L. Size makes a difference. Public Health Nutr. 2003, 6, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Steenhuis, I.H.M.; Leeuwis, F.H.; Vermeer, W.M. Small, medium, large or supersize: Trends in food portion sizes in The Netherlands. Public Health Nutr. 2009, 13, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.J.; Popkin, B.M. Patterns and trends in food portion sizes, 1977–1998. JAMA 2003, 289, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Rolls, B.J.; Roe, L.S.; Meengs, J.S. Larger portion sizes lead to sustained increases in energy intake over 2 days. J. Am. Diet. Assoc. 2006, 106, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Rolls, B.J.; Roe, L.S.; Meengs, J.S. The effect of large portion sizes on energy intake is sustained for 11 days. Obesity 2007, 15, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, R.; Rydell, S.; Dunn, C.; Harnack, L.; Levine, A.; Pentel, P.; Baxter, J.; Walsh, E. Effects of portion size on chronic energy intake. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 27. [Google Scholar] [CrossRef] [PubMed]
- Raynor, H.A.; Wing, R.R. Package unit size and amount of food: Do both influence intake? Obesity (Silver Spring) 2007, 15, 2311–2319. [Google Scholar] [CrossRef] [PubMed]
- Smiciklas-Wright, H.; Mitchrll, D.C.; Mickle, S.J.; Goldman, J.D.; Cook, A. Foods commonly eaten in the United States, 1989–1991 and 1994–1996: Are portion sizes changing? J. Am. Diet Assoc. 2003, 103, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Wrieden, W.; Gregor, A.; Barton, K. Have food portion sizes increased in the UK over the last 20 years? Proc. Nutr. Soc. 2008, 67, 211. [Google Scholar] [CrossRef]
- Church, S. Trends in Portion Size in the UK—A Preliminary Review of Published Information; Food Standards Agency: London, UK, 2008.
- Collins, K.; Watson, J.F.; Collins, C.E. Food and beverage portion sizes in Australian children: A secondary analysis of 1995 and 2007 national data. BMC Public Health 2014, 14, 517. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.A.; Livingstone, M.B.E.; McNulty, B.A.; Lyons, J.; Walton, J.; Flynn, A.; Segurado, R.; Dean, M.; Spence, M.; McCaffrey, T.A.; et al. Secular trends in reported portion size of food and beverages consumed by Irish adults. Br. J. Nutr. 2015, 113, 1148–1157. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, S.N.; Robson, P.J.; Livingstone, M.B.; Kiely, M.; Flynn, A.; Cran, G.W.; Gibney, M.J. Associations between daily food intake and excess adiposity in Irish adults: Towards the development of food-based dietary guidelines for reducing the prevalence of overweight and obesity. Int. J. Obes. 2006, 30, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.T.; Rennie, K.L.; Wallace, J.M.W.; Robson, P.J.; Welch, R.W.; Hannon-Fletcher, M.P.; Livingstone, M.B. Associations between the portion sizes of food groups consumed and measures of adiposity in the British National Diet and Nutrition Survey. Br. J. Nutr. 2009, 101, 1413–1420. [Google Scholar] [CrossRef] [PubMed]
- Albar, S.A.; Alwan, N.A.; Evans, C.E.L.; Cade, J.E. Is there an association between food portion size and BMI among British adolescents? Br. J. Nutr. 2014, 112, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Secretaria de Vigilância em Saúde, Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção de Saúde. Vigitel Brasil 2016: Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas por Inquérito Telefônico: Estimativas Sobre Frequência e Distribuição Sociodemográfica de Fatores de Risco e Proteção Para Doenças Crônicas nas Capitais dos 26 Estados Brasileiros e no Distrito Federal em 2016; Ministério da Saúde: Brasília, Brazil, 2017. (In Portuguese)
- Pereira, J.L.; Mendes, A.; Crispim, S.P.; Marchioni, D.M.; Fisberg, R.M. Association of Overweight with Food Portion Size among Adults of São Paulo-Brazil. PLoS ONE 2016, 11, e0164127. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, I.N.; Alencar, E.S.D. Association between excess weight and beverage portion size consumed in Brazil. Rev. Saúde Pública 2018, 52, 21. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. The nutrition transition and obesity in the developing world. J. Nutr. 2001, 131, 871S–873S. [Google Scholar] [CrossRef] [PubMed]
- Levy-Costa, R.B.; Sichieri, R.; Pontes, N.D.S.; Monteiro, C.A. Household food availability in Brazil: Distribution and trends (1974–2003). Rev. Saúde Pública 2005, 39, 530–540. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.C.G.P. ISA-CAPITAL Plano de Amostragem. Faculdade de Saúde Pública, Faculdade de Medicina, Universidade Estadual Paulista e Universidade Estadual de Campinas e Secretaria de Estado da Saúde. 2003. Available online: http://www.fsp.usp.br/isa-sp/pdf/planoamostralisacapital.pdf (accessed on 23 March 2018). (In Portuguese).
- Alves, M.C.G.P.; Escuder, M.M.L. Plano de amostragem do ISA-Capital 2008. Faculdade de Saúde Pública, Faculdade de Medicina, Universidade Estadual Paulista e Universidade Estadual de Campinas e Secretaria de Estado da Saúde. 2009. Available online: http://www.fsp.usp.br/isa-sp/pdf/planoamostral2008.pdf (accessed on 24 mar 2018). (In Portuguese).
- Fisberg, R.M.; Sales, C.H.; Fontanelli, M.M.; Pereira, J.L.; Alves, M.C.G.P.; Escuder, M.M.L.; Cesar, C.L.G.; Goldbaum, M. 2015 Health Survey of São Paulo with Focus in Nutrition: Rationale, Design, and Procedures. Nutrients 2018, 10, 169. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Matsudo, S.; Araujo, T.; Marsudo, V.; Andrade, D.; Andrade, E.; Braggion, G. Questionário Internacional de atividade física (IPAQ) estudo de validade e reprodutibilidade no Brasil. Rev. Bras. Atividade Fis. Saude 2001, 6, 5–18. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010; Available online: http://www.who.int/dietphysicalactivity/factsheet_recommendations/en/ (accessed on 22 March 2018).
- World Health Organization. WHO Child and Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; WHO: Geneva, Switzerland, 2006; Available online: http://www.who.int/childgrowth/standards/technical_report/en/ (accessed on 15 January 2018).
- World Health Organization. Consultation on Obesity: Preventing and Managing the Global Epidemic; WHO-Technical Report Series 894; WHO: Geneva, Switzerland, 1998. [Google Scholar]
- Lebrão, M.L.; Duarte, Y.A.O. SABE—Saúde, Bem-Estar e Envelhecimento—O Projeto Sabe no Município de São Paulo: Uma Abordagem Inicial, 1st ed.; Organização Pan-Americana da Saúde: Brasília, Brazil, 2003. (In Portuguese) [Google Scholar]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, A.B.V.; Lacerda, E.M.A.; Benzecry, E.H.; Gomes, M.C.S.; Costa, V.M. Tabela Para Avaliação de Consumo Alimentar em Medidas Caseiras, 5th ed.; Atheneu: São Paulo, Brazil, 2008. (In Portuguese) [Google Scholar]
- Fisberg, R.M.; Villar, B.S. Manual de Receitas e Medidas Caseiras Para Cálculo de Inquéritos Alimentares: Manual Elaborado Para Auxiliar o Processamento de Inquéritos Alimentares; Signus: São Paulo, Brazil, 2002. (In Portuguese) [Google Scholar]
- Núcleo de Estudos e Pesquisas em Alimentação (NEPA), Universidade Estadual de Campinas. Tabela Brasileira de Composição de Alimentos, 4th ed.; NEPA-UNICAMP: Campinas, Brazil, 2011. (In Portuguese) [Google Scholar]
- Block, G.; Hartman, A.M.; Dresser, C.M.; Carroll, M.D.; Gannon, J.; Gardner, L. A data-based approach to diet questionnaire design and testing. Am. J. Epidemiol. 1986, 124, 453–469. [Google Scholar]
- Fisher, J.O.; Goran, M.I.; Hetherington, M.M.; Rowe, S. Forefronts in portion size—An overview and synthesis of a roundtable discussion. Appetite 2015, 88, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization. Food Energy Methods of Analysis and Conversion Factors; Report of a Technical Workshop; FAO: Rome, Italy, 2003; Available online: http://www.fao.org/uploads/media/FAO_2003_Food_Energy_02.pdf (accessed on 25 March 2018).
- Banna, J.C.; McCrory, M.A.; Fialkowski, M.K.; Boushey, C. Examining Plausibility of self-reported energy intake Data: Considerations for Method selection. Front. Nutr. 2017, 4, 45. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Mattei, J.; Hu, F.B.; Campos, H. A higher ratio of beans to white rice is associated with lower cardiometabolic risk factors in Costa Rican adults. Am. J. Clin. Nutr. 2011, 94, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Basil, M.; Maibach, E.; Goldberg, J.; Snyder, D.A.N. Why Americans eat what they do: Taste, nutrition, cost, convenience, and weight control concerns as influences on food consumption. JADA 1998, 98, 1118–1126. [Google Scholar] [CrossRef]
- Cruwys, T.; Bevelander, K.E.; Hermans, R.C. Social modeling of eating: A review of when and why social influence affects food intake and choice. Appetite 2015, 86, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Munt, A.E.; Partridge, S.R.; Allman-Farinelli, M. The barriers and enablers of healthy eating among young adults: A missing piece of the obesity puzzle: A. scoping review. Obes. Rev. 2017, 18, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Mattes, R. Energy intake and obesity: Ingestive frequency outweighs portion size. Physiol. Behav. 2014, 134, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Duffey, K.J.; Popkin, B.M. Energy density, portion size, and eating occasions: Contributions to increased energy intake in the United States, 1977–2006. PLoS Med. 2011, 8, e1001050. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A.M.; Jebb, S.A. Fast foods, energy density and obesity: A possible mechanistic link. Obes. Rev. 2003, 4, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Sichieri, R. Dietary patterns and their associations with obesity in the Brazilian city of Rio de Janeiro. Obes. Res. 2002, 10, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.A.; Baltar, V.T.; Marchioni, D.M.L.; Fisberg, R.M. Examining associations between dietary patterns and metabolic CVD risk factors: A novel use of structural equation modelling. Br. J. Nutr. 2016, 115, 1586–1597. [Google Scholar] [CrossRef] [PubMed]
- Sichieri, R.; Moura, A.S.; Genelhu, V.; HU, F.; Willett, W.C. An 18-mo randomized trial of a low-glycemic-index diet and weight change in Brazilian women. Am. J. Clin. Nutr. 2007, 86, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Cunha, D.B.; de Almeida, R.M.; Sichieri, R.; Pereira, R.A. Association of dietary patterns with BMI and waist circumference in a low-income neighbourhood in Brazil. Br. J. Nutr. 2010, 104, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, Y.; Fulgoni, V.L., III. Bean consumption is associated with greater nutrient intake, reduced systolic blood pressure, lower body weight, and a smaller waist circumference in adults: Results from the National Health and Nutrition Examination Survey 1999–2002. J. Am. Coll. Nutr. 2008, 27, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Azadbakht, L.; Haghighatdoost, F.; Esmaillzadeh, A. White rice consumption, body mass index, and waist circumference among Iranian female adolescents. J. Am. Coll. Nutr. 2016, 35, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.G.M.; da Costa Proença, R.P.; Calvo, M.C.M.; Fiates, G.M.R. Overweight/obesity is associated with food choices related to rice and beans, colors of salads, and portion size among consumers at a restaurant serving buffet-by-weight in Brazil. Appetite 2012, 59, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Rhee, J.J.; Mattei, J.; Campos, H. Association between commercial and traditional sugar-sweetened beverages and measures of adiposity in Costa Rica. Public Health Nutr. 2012, 15, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; O’Connor, L.; Ye, Z.; Mursu, J.; Hayashino, Y.; Bhupathiraju, S.N.; Forouhi, N.G. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. BMJ 2015, 351, h3576. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Malik, V.; Rexrode, K.M.; Manson, J.E.; Willett, W.C.; Hu, F.B. Sweetened beverage consumption and risk of coronary heart disease in women. Am. J. Clin. Nutr. 2009, 89, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.M.; Micha, R.; Khatibzadeh, S.; Shi, P.; Lim, S.; Andrews, K.G.; Engell, R.E.; Ezzati, M.; Mozaffarian, D.; Global Burden of Diseases Nutrition and Chronic Diseases Expert Group (NutriCoDE). Global, Regional, and National Consumption of Sugar-Sweetened Beverages, Fruit Juices, and Milk: A Systematic Assessment of Beverage Intake in 187 Countries. PLoS ONE 2015, 10, e0124845. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Shaper, A.G. Alcohol, body weight, and weight gain in middle-aged men. Am. J. Clin. Nutr. 2003, 77, 1312–1317. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Field, A.E.; Colditz, G.A.; Rimm, E.B. Alcohol intake and 8-year weight gain in women: A prospective study. Obes. Res. 2004, 12, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Lee, I.M.; Manson, J.E.; Buring, J.E.; Sesso, H.D. Alcohol consumption, weight gain, and risk of becoming overweight in middle-aged and older women. Arch. Int. Med. 2010, 170, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Vergnaud, A.C.; Norat, T.; Romaguera, D.; Mouw, T.; May, A.M.; Travier, N.; Luan, J.; Wareham, N.; Slimani, N.; Rinaldi, S.; et al. Meat consumption and prospective weight change in participants of the EPIC-PANACEA study. Am. J. Clin. Nutr. 2010, 92, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Bouvard, V.; Loomis, D.; Guyton, K.Z.; Grosse, Y.; Ghissassi, E.F.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K.; International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015, 16, 1599–1600. [Google Scholar] [CrossRef]
- Pereira, R.; Duffey, K.; Sichieri, R.; Popkin, B. Sources of excessive saturated fat, trans fat and sugar consumption in Brazil: An analysis of the first Brazilian nationwide individual dietary survey. Public Health Nutr. 2014, 17, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.M.; Piovezan, L.G.; Selem, S.S.C.; de Castro, A.; Fisberg, R.M.; Marchioni, D.M.L. Validação e calibração de medidas de peso e altura autorreferidas por indivíduos da cidade de São Paulo. Rev. Bras. Epidemiol. 2014, 7, 735–746. [Google Scholar] [CrossRef]
- Mendez, M.A.; Popkin, B.M.; Buckland, G.; Schroder, H.; Amiano, P.; Barricarte, A.; Huerta, J.M.; Quirós, J.R.; Sánchez, M.J.; González, C.A. Alternative methods of accounting for under-reporting and overreporting when measuring dietary intake-obesity relations. Am. J. Epidemiol. 2011, 173, 448–458. [Google Scholar] [CrossRef] [PubMed]
- Lafay, L.; Mennen, L.; Basdevant, A.; Charles, M.A.; Borys, J.M.; Eschwege, E.; Romon, M. Does energy intake underreporting involve all kinds of food or only specific food items? Results from the Fleurbaix Laventie Ville Santé (FLVS) study. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1500–1506. [Google Scholar] [CrossRef] [PubMed]
- Lissner, L. Measuring food intake in studies of obesity. Public Health Nutr. 2002, 5, 889–892. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística. Estatística I-IBdGe–Cidades. Available online: https://cidades.ibge.gov.br/brasil/sp/sao-paulo/panorama (accessed on 29 March 2017). (In Portuguese)

{kind=link}
| ISA-Nutrition 2003 | ISA-Nutrition 2008 | |||||||||||||
| Total Population (n = 2060) | Without EBW (n = 1427) b | With EBW (n = 633) b | Total Population (n = 1556) | Without EBW (n = 997) b | With EBW (n = 559) b | |||||||||
| % | 95% CL | % | 95% CL | % | 95% CL | pc | % | 95% CL | % | 95% CL | % | 95% CL | pc | |
| Age group | ||||||||||||||
| Adolescents (12–19 years) | 17.5 | (15.6, 19.6) | 82.2 | (82.8, 89.1) | 13.8 | (10.9, 17.2) | 24.3 | (21.2, 27.6) | 75.2 | (70.7, 79.3) | 24.8 | (20.7, 29.3) | ||
| Adults (20–59 years) | 70.1 | (68.0, 72.1) | 59.0 | (55.5, 62.6) | 41.0 | (37.4, 44.6) | 62.6 | (58.9, 66.1) | 53.1 | (48.7, 57.4) | 46.9 | (42.6, 51.3) | ||
| Older adults (60 years or more) | 12.4 | (10.8, 14.2) | 64.1 | (59.2, 68.6) | 36.0 | (31.4, 40.8) | 0.000 | 13.2 | (11.0, 15.7) | 66.0 | (61.9, 69.8) | 34.0 | (30.2, 38.1) | 0.000 |
| Gender | ||||||||||||||
| Female | 52.4 | (49.5, 55.2) | 66.5 | (62.8, 69.9) | 33.6 | (30.1, 37.2) | 54.3 | (51.8,.56.8) | 61.8 | (57.8, 65.5) | 38.3 | (34.5, 42.2) | ||
| Male | 47.6 | (44.8, 50.4) | 62.1 | (57.7, 66.3) | 37.9 | (33.7, 42.3) | 0.145 | 45.7 | (43.1, 48.2) | 58.2 | (53.3, 63.0) | 41.8 | (37.0, 46.7) | 0.259 |
| Racial Self-identification | ||||||||||||||
| White | 67.2 | (63.2,71.0) | 61.9 | (58.7, 65.1) | 38.1 | (34.9, 41.3) | 60.5 | (54.7, 65.9) | 59.5 | (55.7, 63.2) | 40.5 | (36.8, 44.3) | ||
| Non white | 32.8 | (29.1, 36.8) | 69.6 | (65.4, 73.5) | 30.4 | (26.5, 34.6) | 0.004 | 39.5 | (34.0, 45.3) | 61.2 | (55.4, 66.7) | 38.8 | (33.3, 44.6) | 0.435 |
| Education of parent/householder | ||||||||||||||
| ≤9 years | 54.0 | (49.5, 58.4) | 65.3 | (61.8, 68.7) | 34.7 | (31.3, 38.2) | 46.8 | (40.4, 53.2) | 60.7 | (56.1, 65.1) | 39.3 | (34.9, 43.9) | ||
| >9 years | 46.0 | (41.6, 50.5) | 63.5 | (58.9, 67.8) | 36.5 | (32.2, 41.1) | 0.521 | 53.3 | (46.8, 59.6) | 59.5 | (55.5, 63.4) | 40.5 | (36.6, 44.5) | 0.675 |
| Household income d | ||||||||||||||
| ≤1 MW d | 38.5 | (34.0, 43.2) | 68.4 | (63.6, 72.9) | 31.6 | (27.1, 36.4) | 44.3 | (39.1, 49.5) | 65.6 | (61.3, 69.7) | 34.4 | (30.3, 38.7) | ||
| >1 MW d | 61.5 | (56.8, 66.0) | 61.9 | (58.4, 65.3) | 38.1 | (34.7, 41.6) | 0.041 | 55.7 | (50.4, 60.9) | 55.8 | (51.9, 59.6) | 44.2 | (40.4, 48.1) | 0.000 |
| Leisure-time Physical Activity Level | ||||||||||||||
| Meet the recommendation | 22.7 | (19.9, 25.8) | 62.2 | (56.8, 67.3) | 37.8 | (32.7, 43.2) | 22.2 | (20.3, 24.4) | 57.4 | (50.3, 64.2) | 42.6 | (35.8, 50.7) | ||
| Don’t meet the recommendation | 77.3 | (74.2, 80.1) | 65.0 | (62.0, 67.9) | 35.0 | (32.1, 38.0) | 0.339 | 77.8 | (75.6, 79.7) | 61.1 | (57.5, 64.5) | 38.9 | (35.5, 42.5) | 0.362 |
| Global Physical Activity Level | ||||||||||||||
| Meet the recommendation | 77.2 | (74.0, 80.1) | 65.8 | (61.1, 70.3) | 34.2 | (29.7, 38.9) | 79.8 | (77.0, 82.4) | 58.4 | (55.1, 61.7) | 41.6 | (38.3, 44.9) | ||
| Don’t meet the recommendation | 22.8 | (19.9, 26.0) | 64.1 | (61.0, 67.1) | 35.9 | (32.9, 39.0) | 0.517 | 20.2 | (17.6, 23.0) | 67.0 | (61.0, 72.4) | 33.0 | (27.6, 39.0) | 0.008 |
| Smoking status | ||||||||||||||
| Never | 65.9 | (62.9, 68.8) | 65.8 | (62.4, 69.0) | 34.2 | (31.0, 37.6) | 66.4 | (63.1, 69.5) | 63.2 | (59.7, 66.5) | 36.8 | (33.5, 40.3) | ||
| Former | 19.2 | (16.6, 22.0) | 70.4 | (63.1, 76.8) | 29.6 | (23.2, 36.9) | 15.4 | (12.9, 18.3) | 46.7 | (39.0, 54.5) | 53.3 | (45.5, 61.0) | ||
| Current | 15.0 | (12.4, 17.9) | 50.1 | (52.4, 57.3) | 49.9 | (42.6, 57.2) | 0.000 | 18.2 | (15.4, 21.4) | 60.5 | (53.4, 67.1) | 39.5 | (32.9, 46.6) | 0.000 |
| Alcohol intake | ||||||||||||||
| Never | 46.1 | (42.5, 49.7) | 67.4 | (63.4, 71.2) | 32.6 | (28.8, 36.6) | 50.0 | (46.7, 53.2) | 63.4 | (59.3, 67.3) | 36.6 | (32.7, 40.7) | ||
| ≤3 times per week | 48.6 | (45.0, 52.2) | 62.0 | (57.9, 65.9) | 38.0 | (34.1, 42.1) | 44.8 | (41.6, 48.1) | 57.3 | (52.2, 62.2) | 42.7 | (37.8, 47.8) | ||
| >3 times per week | 5.32 | (4.10, 6.88) | 57.6 | (44.1, 70.1) | 42.4 | (29.9, 55.9) | 0.110 | 5.23 | (4.0, 6.8) | 54.7 | (42.5, 66.4) | 45.3 | (33.6, 57.5) | 0.094 |
| mean | IQR | mean | IQR | mean | IQR | pc | mean | IQR | mean | IQR | mean | IQR | pc | |
| Dietary intake | ||||||||||||||
| Total energy (kcal/day) | 1826 | (1235, 2304) | 1849 | (1269, 2290) | 1786 | (1204, 2310) | 0.214 | 1932 | (1256, 2430) | 1994 | (1318, 2488) | 1838 | (1177, 2321) | 0.002 |
| EI/EER | 0.71 | (0.49, 0.87) | 0.74 | (0.50, 0.92) | 0.65 | (0.46, 0.81) | 0.000 | 0.77 | (0.50, 0.96) | 0.82 | (0.55, 1.02) | 0.69 | (0.44, 0.84) | 0.000 |
| Total grams (g/day) | 1547 | (1041, 1847) | 1517 | (1065, 1833) | 1602 | (998, 1900) | 0.461 | 1666 | (1130, 2047) | 1699 | (1161, 2067) | 1616 | (1075, 1999) | 0.037 |
| Total energy density (kcal/g) | 1.26 | (1.00, 1.47) | 1.26 | (1.00, 1.47) | 1.25 | (0.98, 1.47) | 0.479 | 1.19 | (0.97, 1.36) | 1.21 | (1.00, 1.38) | 1.17 | (0.95, 1.35) | 0.026 |
| Protein (%kcal) | 17.1 | (13.3, 19.9) | 16.9 | (13.1, 19.8) | 17.5 | (13.6, 20.4) | 0.102 | 17.4 | (13.2, 10.4) | 17.1 | (13.2, 19.8) | 17.7 | (13.2, 21.0) | 0.074 |
| Carbohydrates (%kcal) | 47.7 | (41.48, 53.7) | 48.4 | (42.5, 53.9) | 46.3 | (40.2, 52.9) | 0.002 | 47.5 | (41.5, 54.3) | 47.8 | (41.6, 54.5) | 47.0 | (40.6, 54.2) | 0.425 |
| Total Fat (%kcal) | 32.7 | (27.3, 38.3) | 32.4 | (26.9, 37.8) | 33.2 | (28.0, 38.9) | 0.097 | 32.4 | (26.5, 38.0) | 32.4 | (26.7, 38.0) | 32.3 | (26.3, 38.2) | 0.910 |
| ISA-Nutrition 2015 | p-Values for the Difference Across Surveys c | |||||||||||||
| Total Population (n = 1654) | Without EBW (n = 969) b | With EBW (n = 685) b | ||||||||||||
| % | 95% CL | % | 95% CL | % | 95% CL | pc | Total Population | Without EBW | With EBW | |||||
| Age group | ||||||||||||||
| Adolescents (12–19 years) | 22.8 | (20.5, 25.3) | 70.6 | (65.9, 74.9) | 29.4 | (25.2, 34.1) | ||||||||
| Adults (20–59 years) | 54.3 | (51.5, 57.0) | 45.8 | (41.5, 50.2) | 54.2 | (49.8, 58.5) | ||||||||
| Older adults (60 years or more) | 22.9 | (20.1, 26.0) | 63.1 | (58.3, 67.6) | 36.9 | (32.4, 41.7) | 0.000 | 0.000 | 0.000 | 0.000 | ||||
| Gender | ||||||||||||||
| Female | 49.7 | (46.8, 52.7) | 54.5 | (50.9, 58.1) | 45.5 | (41.9, 49.1) | ||||||||
| Male | 50.3 | (47.3, 53.2) | 56.3 | (52.1, 60.4) | 43.7 | (39.6, 47.9) | 0.482 | 0.112 | 0.054 | 0.673 | ||||
| Racial Self-identification | ||||||||||||||
| White | 50.4 | (46.5, 54.2) | 53.5 | (49.1, 57.9) | 46.5 | (42.1, 50.9) | ||||||||
| Non white | 49.7 | (45.8, 53.5) | 57.2 | (53.1, 61.1) | 42.8 | (38.9, 46.9) | 0.233 | 0.000 | 0.000 | 0.000 | ||||
| Education of parent/householder | ||||||||||||||
| ≤9 years | 45.0 | (40.8, 49.3) | 56.2 | (52.4, 59.9) | 43.8 | (40.1, 47.6) | ||||||||
| >9 years | 55.0 | (50.7, 59.2) | 54.4 | (49.6, 59.2) | 45.6 | (40.8, 50.4) | 0.586 | 0.028 | 0.056 | 0.099 | ||||
| Household income d | ||||||||||||||
| ≤1 MW d | 49.9 | (44.8, 54.9) | 54.3 | (50.2, 58.2) | 45.8 | (41.8, 49.8) | ||||||||
| >1 MW d | 50.1 | (45.1, 55.2) | 53.8 | (48.7, 58.7) | 46.3 | (41.3, 51.3) | 0.881 | 0.007 | 0.031 | 0.003 | ||||
| Leisure-time Physical Activity Level | ||||||||||||||
| Meet the recommendation | 21.9 | (19.5, 24.6) | 58.2 | (51.7, 64.5) | 41.8 | (35.5, 48.3) | ||||||||
| Don’t meet the recommendation | 78.1 | (75.4, 80.5) | 54.6 | (51.7, 57.6) | 45.4 | (42.4, 48.3) | 0.286 | 0.883 | 0.755 | 0.407 | ||||
| Global Physical Activity Level | ||||||||||||||
| Meet the recommendation | 74.6 | (71.6, 77.4) | 59.4 | (53.8, 64.7) | 40.6 | (35.3, 46.2) | ||||||||
| Don’t meet the recommendation | 25.4 | (22.6, 28.4) | 54.3 | (50.9, 57.6) | 45.7 | (42.4, 49.1) | 0.130 | 0.076 | 0.209 | 0.050 | ||||
| Smoking status | ||||||||||||||
| Never | 71.0 | (68.1, 73.7) | 56.4 | (53.0, 59.8) | 43.6 | (40.2, 47.0) | ||||||||
| Former | 15.0 | (12.8, 17.6) | 44.3 | (37.8, 50.9) | 55.7 | (49.1, 62.2) | ||||||||
| Current | 14.0 | (12.1, 16.1) | 62.0 | (54.1, 69.4) | 38.0 | (30.6, 45.9) | 0.002 | 0.023 | 0.000 | 0.013 | ||||
| Alcohol intake | ||||||||||||||
| Never | 58.6 | (54.5, 62.6) | 58.8 | (55.2, 62.3) | 41.2 | (37.7, 44.8) | ||||||||
| ≤3 times per week | 38.9 | (35.0, 42.8) | 50.1 | (44.8, 55.3) | 49.9 | (44.7, 55.2) | ||||||||
| >3 times per week | 2.55 | (1.70, 3.79) | 61.1 | (45.3, 74.9) | 38.9 | (25.1, 54.7) | 0.010 | 0.000 | 0.000 | 0.003 | ||||
| mean | IQR | mean | IQR | mean | IQR | pc | Total Population | Without EBW | With EBW | |||||
| Dietary intake | ||||||||||||||
| Total energy (kcal/day) | 1877 | (1262, 2344) | 1952 | (1285, 2472) | 1783 | (1226, 2208) | 0.002 | 0.00 | 0.01 | 0.84 | ||||
| EI/EER | 0.72 | (0.49, 0.89) | 0.78 | (0.54, 0.96) | 0.65 | (0.45, 0.78) | 0.000 | 0.00 | 0.00 | 0.97 | ||||
| Total grams (g/day) | 1615 | (1110, 1967) | 1640 | (1139, 2018) | 1585 | (1082, 1913) | 0.021 | 0.02 | 0.00 | 0.15 | ||||
| Total energy density (kcal/g) | 1.22 | (0.98, 1.40) | 1.24 | (1.00, 1.43) | 1.19 | (0.97, 1.36) | 0.040 | 0.01 | 0.08 | 0.03 | ||||
| Protein (%kcal) | 17.2 | (13.2, 20.0) | 17.2 | (13.1, 20.0) | 17.1 | (13.2, 20.0) | 0.767 | 0.04 | 0.51 | 0.34 | ||||
| Carbohydrates (%kcal) | 48.1 | (42.3, 54.1) | 48.5 | (42.4, 55.2) | 47.6 | (42.2, 52.8) | 0.033 | 0.00 | 0.68 | 0.08 | ||||
| Total Fat (%kcal) | 31.8 | (26.7, 37.1) | 31.5 | (26.3, 36.7) | 32.2 | (27.3, 37.5) | 0.115 | 0.11 | 0.05 | 0.03 | ||||
| Total Population (n = 5270) | ||||||||||
| ISA-Nutrition 2003 (n = 2060) | ISA-Nutrition 2008 (n = 1556) | |||||||||
| Food Grouping a | Consumption | Portion Size (g) | Consumption | Portion Size (g) | ||||||
| % | SE | Mean | Median | IQR | % | SE | Mean | Median | IQR | |
| Alcoholic beverages | 9.3 | 0.01 | 732.8 | 542.4 | (602.6, 862.9) | 10.2 | 0.01 | 726.1 | 477.2 | (590.0, 862.1) |
| Beans | 63.3 | 0.02 | 104.3 | 86.0 | (98.6, 110.1) | 65.8 | 0.02 | 108.6 | 86.0 | (103.2, 114.0) |
| Breads and rolls | 71.4 | 0.01 | 62.0 | 50.0 | (59.6, 64.4) | 70.9 | 0.01 | 63.8 | 50.0 | (61.1, 66.6) |
| Butter and margarine | 47.1 | 0.02 | 16.2 | 15.0 | (14.4, 18.0) | 41.5 | 0.02 | 18.4 | 15.0 | (16.7,20.0) |
| Cakes | 10.4 | 0.01 | 91.5 | 60.2 | (76.7, 106.2) | 11.0 | 0.01 | 90.0 | 70.0 | (79.5, 100.4) |
| Cheese | 25.6 | 0.02 | 37.8 | 30.0 | (34.3, 41.4) | 25.6 | 0.02 | 37.8 | 30.0 | (34.4, 41.2) |
| Coffee and tea | 75.5 | 0.01 | 117.6 | 96.1 | (112.5, 122.7) | 69.3 | 0.02 | 116.8 | 97.6 | (109.9, 123.8) |
| Cold Cuts | 11.6 | 0.01 | 40.1 | 30.0 | (34.2, 46.0) | 16.2 | 0.02 | 33.9 | 30.0 | (29.5, 38.4) |
| Commercial juices | 17.0 | 0.01 | 312.3 | 257.1 | (289.3, 335.2) | 25.3 | 0.02 | 290.9 | 240.0 | (274.9, 306.9) |
| Eggs | 9.3 | 0.01 | 56.5 | 50.0 | (52.8, 60.2) | 10.5 | 0.01 | 49.4 | 50.0 | (42.6, 56.2) |
| Flavored powder | 12.1 | 0.01 | 30.3 | 25.0 | (27.1, 33.6) | 12.4 | 0.01 | 27.3 | 24.0 | (23.6, 30.9) |
| Flavored snacks | 2.5 | 0.00 | 75.4 | 50.0 | (35.2, 115.5) | 3.4 | 0.01 | 74.9 | 60.0 | (56.0, 93.8) |
| Fried snacks | 5.7 | 0.01 | 117.6 | 100.0 | (101.3, 133.9) | 6.0 | 0.01 | 145.8 | 100.0 | (118.4, 173.3) |
| Fruit juices | 20.8 | 0.01 | 446.9 | 251.6 | (155.4, 738.5) | 20.1 | 0.01 | 268.5 | 240.4 | (248.9, 288.0) |
| Fruits | 28.8 | 0.02 | 163.4 | 135.0 | (152.6, 174.1) | 34.1 | 0.02 | 172.4 | 142.0 | (157.6, 187.3) |
| Leafy Vegetables | 40.2 | 0.02 | 40.5 | 30.0 | (36.4, 44.6) | 40.3 | 0.01 | 41.6 | 30.0 | (37.6, 45.7) |
| Milk | 62.7 | 0.01 | 170.4 | 148.5 | (161.8, 178.9) | 58.5 | 0.02 | 162.8 | 128.9 | (154.3, 171.3) |
| Pasta | 19.9 | 0.01 | 238.5 | 238.8 | (219.7, 257.2) | 19.3 | 0.01 | 214.8 | 208.8 | (198.0, 231.6) |
| Pizza | 7.2 | 0.01 | 299.7 | 286.5 | (253.1, 346.2) | 7.7 | 0.01 | 229.3 | 190.3 | (196.3, 262.3) |
| Red meat | 57.1 | 0.01 | 112.5 | 100.0 | (107.3, 117.6) | 59.9 | 0.02 | 116.2 | 100.0 | (107.3, 125.0) |
| Rice | 78.3 | 0.02 | 160.8 | 132.5 | (152.5,169.2) | 80.8 | 0.02 | 145.0 | 124.0 | (137.3, 152.6) |
| Salted snacks | 17.7 | 0.01 | 97.5 | 71.3 | (84.9, 110.1) | 16.4 | 0.01 | 102.3 | 73.2 | (86.6, 117.9) |
| Sandwiches | 4.3 | 0.01 | 223.5 | 200.0 | (196.0, 250.9) | 4.9 | 0.01 | 169.5 | 158.9 | (142.6, 196.4) |
| Soft drinks | 32.6 | 0.01 | 340.4 | 302.8 | (319.4, 361.3) | 38.8 | 0.02 | 327.2 | 250.0 | (308.8, 345.6) |
| Soups | 9.9 | 0.02 | 414.6 | 329.4 | (344.3, 484.9) | 4.8 | 0.01 | 402.9 | 325.0 | (331.1, 474.8) |
| Sugar | 57.2 | 0.02 | 10.1 | 7.7 | (9.28, 11.0) | 63.9 | 0.02 | 10.2 | 8.0 | (9.49, 10.8) |
| Sweets | 20.7 | 0.01 | 87.7 | 66.7 | (80.3, 95.1) | 29.2 | 0.02 | 84.1 | 56.0 | (75.0, 93.2) |
| Toast and Biscuits | 24.1 | 0.01 | 47.1 | 32.0 | (42.1, 52.0) | 26.9 | 0.01 | 49.6 | 30.0 | (43.8, 55.4) |
| Tubers and roots | 13.9 | 0.01 | 118.7 | 90.0 | (101.2, 136.2) | 15.6 | 0.01 | 132.7 | 85.0 | (92.5, 172.8) |
| Vegetables | 43.1 | 0.02 | 75.7 | 60.0 | (68.7, 82.8) | 42.6 | 0.02 | 79.2 | 52.5 | (67.4, 90.8) |
| White meat | 33.0 | 0.02 | 99.3 | 80.0 | (91.3, 107.3) | 37.1 | 0.01 | 116.5 | 100.0 | (104.1, 128.8) |
| Total Population (n = 5270) | ||||||||||
| ISA-Nutrition 2015 (n = 1654) | p-Values for Difference Across the Surveys b | |||||||||
| Food Grouping a | Consumption | Portion Size (g) | ||||||||
| % | SE | Mean | Median | IQR | Frequency | Portion Size | ||||
| Alcoholic beverages | 10.9 | 0.01 | 681.8 | 351.5 | (514.9, 848.7) | 0.278 | 0.638 | |||
| Beans | 66.9 | 0.02 | 107.3 | 86.0 | (102.6, 112.1) | 0.173 | 0.409 | |||
| Breads and rolls | 75.2 | 0.01 | 58.9 | 50.0 | (56.7, 61.1) | 0.057 | 0.086 | |||
| Butter and margarine | 47.9 | 0.01 | 17.4 | 15.0 | (16.5, 18.3) | 0.913 | 0.229 | |||
| Cakes | 12.4 | 0.01 | 90.0 | 60.8 | (76.3, 103.7) | 0.175 | 0.881 | |||
| Cheese | 26.6 | 0.01 | 35.7 | 30.0 | (32.5, 38.8) | 0.673 | 0.390 | |||
| Coffee and tea | 71.8 | 0.01 | 143.8 | 125.1 | (135.1, 152.5) | 0.038 | 0.000 | |||
| Cold Cuts | 12.6 | 0.01 | 28.7 | 20.0 | (24.2, 33.2) | 0.369 | 0.003 | |||
| Commercial juices | 28.8 | 0.02 | 281.9 | 240.0 | (261.8, 302.0) | 0.000 | 0.054 | |||
| Eggs | 11.9 | 0.01 | 70.1 | 50.0 | (62.5, 77.7) | 0.075 | 0.002 | |||
| Flavored powder | 11.8 | 0.01 | 27.7 | 24.0 | (24.1, 31.4) | 0.854 | 0.262 | |||
| Flavored snacks | 3.7 | 0.01 | 58.9 | 48.5 | (47.6, 70.2) | 0.066 | 0.415 | |||
| Fried snacks | 5.0 | 0.01 | 106.7 | 100.0 | (92.8, 120.7) | 0.530 | 0.565 | |||
| Fruit juices | 21.1 | 0.01 | 287.0 | 251.6 | (266.8, 307.1) | 0.904 | 0.277 | |||
| Fruits | 45.5 | 0.02 | 156.0 | 131.0 | (147.0, 164.9) | 0.000 | 0.258 | |||
| Leafy Vegetables | 42.3 | 0.02 | 37.2 | 30.0 | (34.3, 40.1) | 0.445 | 0.224 | |||
| Milk | 59.2 | 0.02 | 164.9 | 148.5 | (157.9, 171.9) | 0.107 | 0.297 | |||
| Pasta | 19.2 | 0.01 | 192.1 | 168.2 | (168.5, 215.7) | 0.718 | 0.003 | |||
| Pizza | 6.7 | 0.01 | 285.9 | 302.1 | (249.4, 322.4) | 0.740 | 0.507 | |||
| Red meat | 58.7 | 0.02 | 103.2 | 92.5 | (97.3, 109.0) | 0.413 | 0.027 | |||
| Rice | 82.6 | 0.01 | 146.0 | 125.0 | (138.7, 153.3) | 0.052 | 0.007 | |||
| Salted snacks | 15.8 | 0.01 | 119.6 | 100.0 | (106.5, 132.6) | 0.264 | 0.022 | |||
| Sandwiches | 3.3 | 0.01 | 170.4 | 158.9 | (142.4, 198.3) | 0.300 | 0.007 | |||
| Soft drinks | 30.9 | 0.01 | 326.3 | 275.1 | (307.2, 345.3) | 0.594 | 0.312 | |||
| Soups | 7.4 | 0.01 | 388.4 | 392.1 | (338.2, 438.6) | 0.183 | 0.561 | |||
| Sugar | 55.1 | 0.02 | 10.9 | 8.1 | (9.93, 11.8) | 0.614 | 0.279 | |||
| Sweets | 34.2 | 0.02 | 70.5 | 45.0 | (62.6, 78.3) | 0.000 | 0.002 | |||
| Toast and Biscuits | 28.0 | 0.01 | 53.8 | 30.0 | (47.1, 60.5) | 0.040 | 0.112 | |||
| Tubers and roots | 16.2 | 0.01 | 131.1 | 80.0 | (107.4, 154.7) | 0.153 | 0.396 | |||
| Vegetables | 46.9 | 0.02 | 71.4 | 52.0 | (65.3, 77.6) | 0.11 | 0.399 | |||
| White meat | 37.7 | 0.01 | 111.8 | 100.0 | (104.5, 119.1) | 0.031 | 0.021 | |||
| Food Grouping b | Adjusted Model for Portion Size c | |||
|---|---|---|---|---|
| nd | OR | 95% CI | p | |
| Alcoholic beverages | 381 | 1.003 | (0.99, 1.01) | 0.276 |
| Beans e | 3236 | 1.014 | (1.00, 1.03) | 0.148 |
| Breads and rolls | 3514 | 1.024 | (0.99, 1.06) | 0.155 |
| Butter and margarine | 2215 | 1.058 | (0.96, 1.16) | 0.239 |
| Cakes | 510 | 1.005 | (0.97, 1.04) | 0.774 |
| Cheese | 1161 | 1.046 | (0.98, 1.11) | 0.154 |
| Coffee and tea | 3469 | 1.010 | (1.00, 1.02) | 0.059 |
| Cold cuts | 581 | 1.112 | (1.04, 1.19) | 0.004 |
| Commercial juices | 1066 | 1.020 | (1.01, 1.03) | 0.002 |
| Eggs | 504 | 1.096 | (1.00, 1.21) | 0.062 |
| Flavored powder | 635 | 1.017 | (0.94, 1.11) | 0.699 |
| Flavored Snacks | 171 | 1.037 | (1.00, 1.07) | 0.278 |
| Fried snacks | 252 | 1.056 | (1.00, 1.11) | 0.030 |
| Fruit juices | 919 | 1.014 | (1.00, 1.03) | 0.044 |
| Fruits | 1795 | 1.004 | (0.99, 1.02) | 0.440 |
| Leafy vegetables | 1927 | 1.018 | (0.98, 1.06) | 0.377 |
| Milk | 3012 | 1.001 | (0.99, 1.01) | 0.867 |
| Pasta | 887 | 1.013 | (1.00, 1.03) | 0.081 |
| Pizza | 290 | 1.028 | (1.01, 1.05) | 0.007 |
| Red meat | 2779 | 1.017 | (1.00, 1.03) | 0.027 |
| Rice | 3951 | 1.025 | (1.01, 1.04) | 0.000 |
| Salted snacks | 799 | 1.031 | (1.01, 1.06) | 0.010 |
| Sandwiches | 172 | 0.989 | (0.93, 1.05) | 0.711 |
| Soft drinks | 1589 | 1.011 | (1.00, 1.02) | 0.005 |
| Soups | 376 | 1.016 | (1.00, 1.03) | 0.010 |
| Sugar | 2793 | 1.148 | (1.02, 1.29) | 0.020 |
| Sweets | 1260 | 1.009 | (0.99, 1.03) | 0.407 |
| Toast and biscuits | 1286 | 1.009 | (0.98, 1.04) | 0.578 |
| Tubers and roots | 704 | 1.011 | (0.99, 1.03) | 0.187 |
| Vegetables | 1997 | 1.016 | (1.00, 1.03) | 0.089 |
| White meat | 1624 | 0.999 | (0.98, 1.02) | 0.882 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, J.L.; Félix, P.V.; Mattei, J.; Fisberg, R.M. Differences over 12 Years in Food Portion Size and Association with Excess Body Weight in the City of São Paulo, Brazil. Nutrients 2018, 10, 696. https://doi.org/10.3390/nu10060696
Pereira JL, Félix PV, Mattei J, Fisberg RM. Differences over 12 Years in Food Portion Size and Association with Excess Body Weight in the City of São Paulo, Brazil. Nutrients. 2018; 10(6):696. https://doi.org/10.3390/nu10060696
Chicago/Turabian StylePereira, Jaqueline Lopes, Paula Victória Félix, Josiemer Mattei, and Regina Mara Fisberg. 2018. "Differences over 12 Years in Food Portion Size and Association with Excess Body Weight in the City of São Paulo, Brazil" Nutrients 10, no. 6: 696. https://doi.org/10.3390/nu10060696
APA StylePereira, J. L., Félix, P. V., Mattei, J., & Fisberg, R. M. (2018). Differences over 12 Years in Food Portion Size and Association with Excess Body Weight in the City of São Paulo, Brazil. Nutrients, 10(6), 696. https://doi.org/10.3390/nu10060696