Assessing the Dietary Habits of Canadians by Eating Location and Occasion: Findings from the Canadian Community Health Survey, Cycle 2.2



Abstract
:1. Introduction
2. Materials and Methods
3. Results
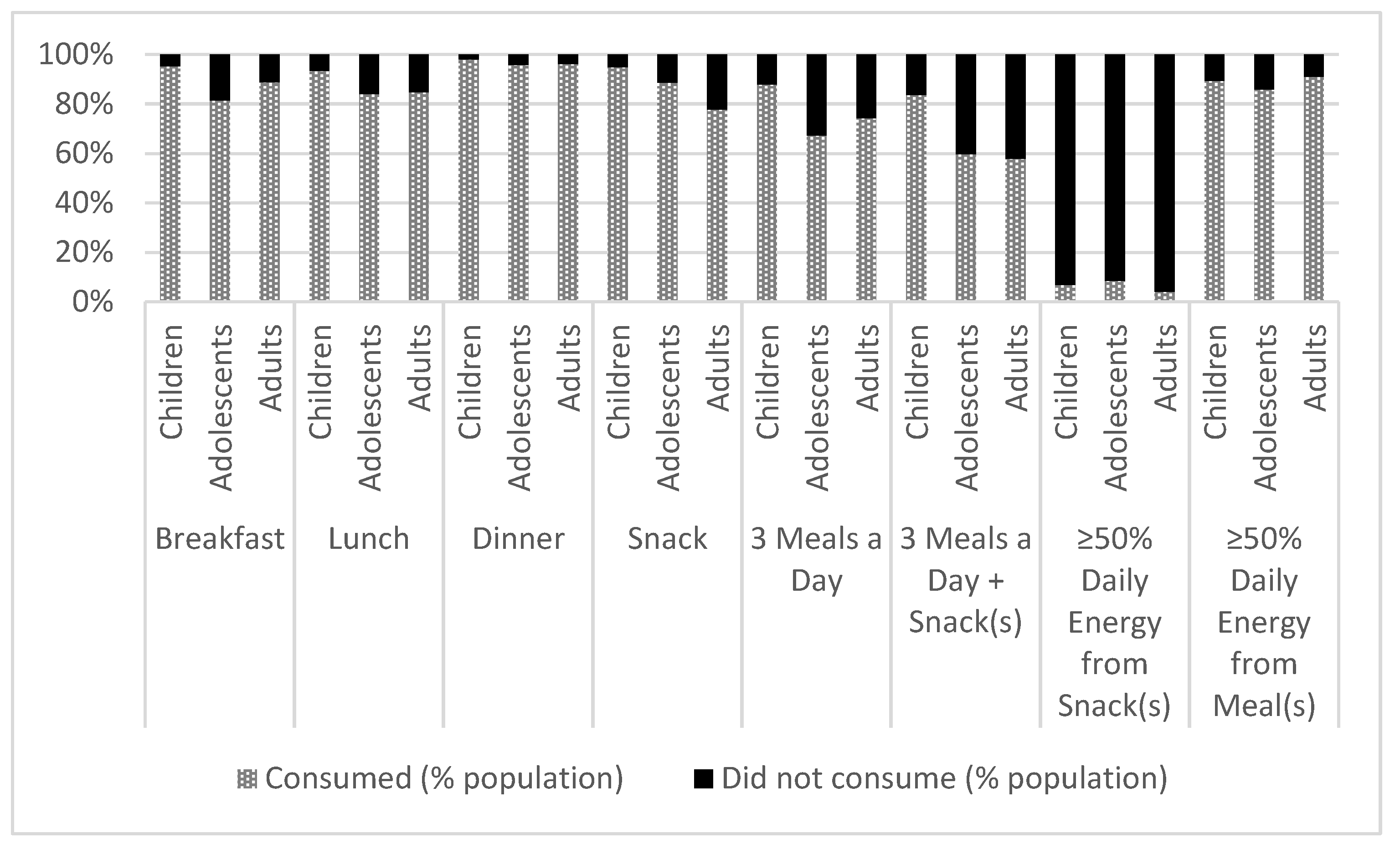
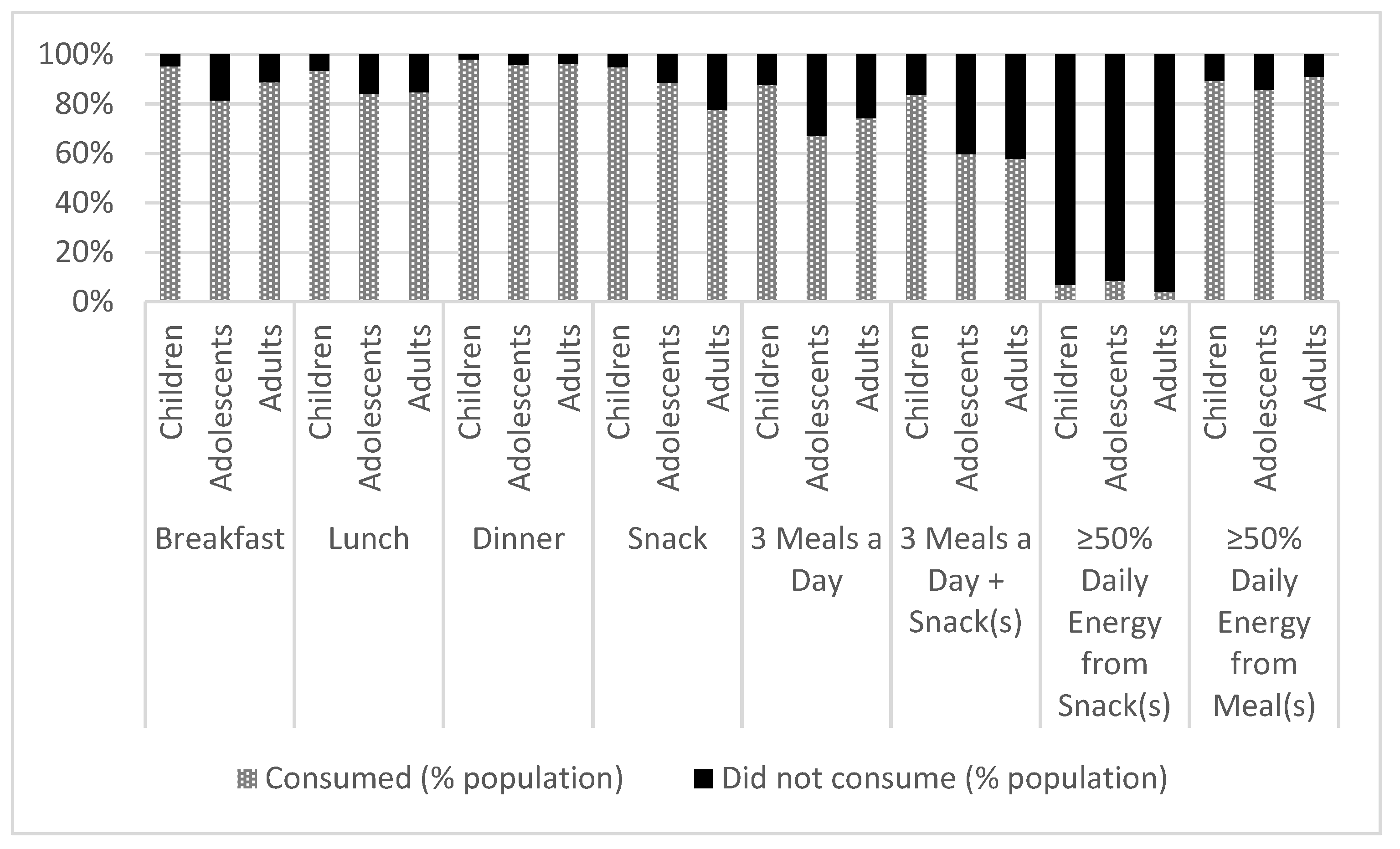
3.1. Eating Occasion
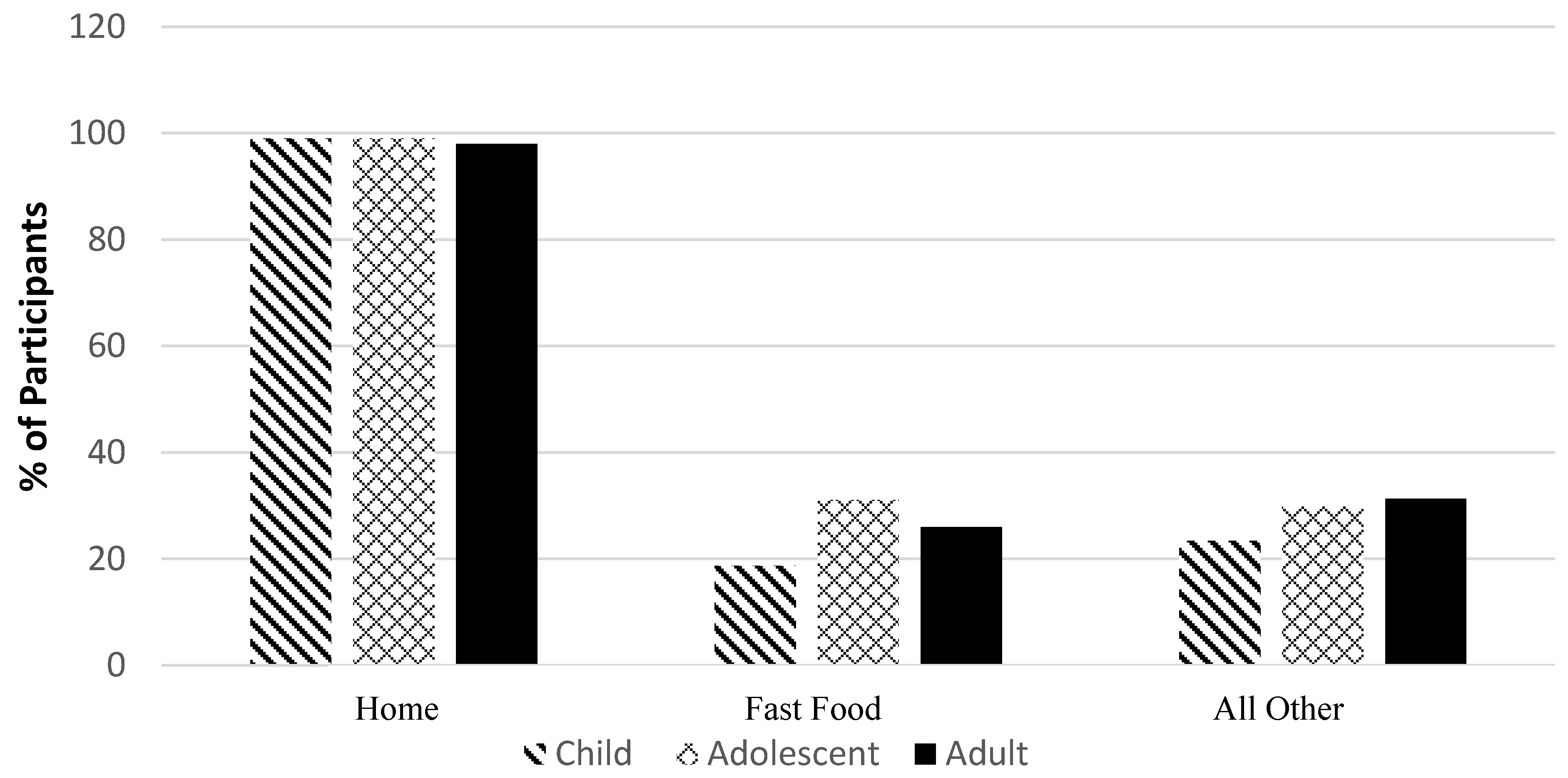
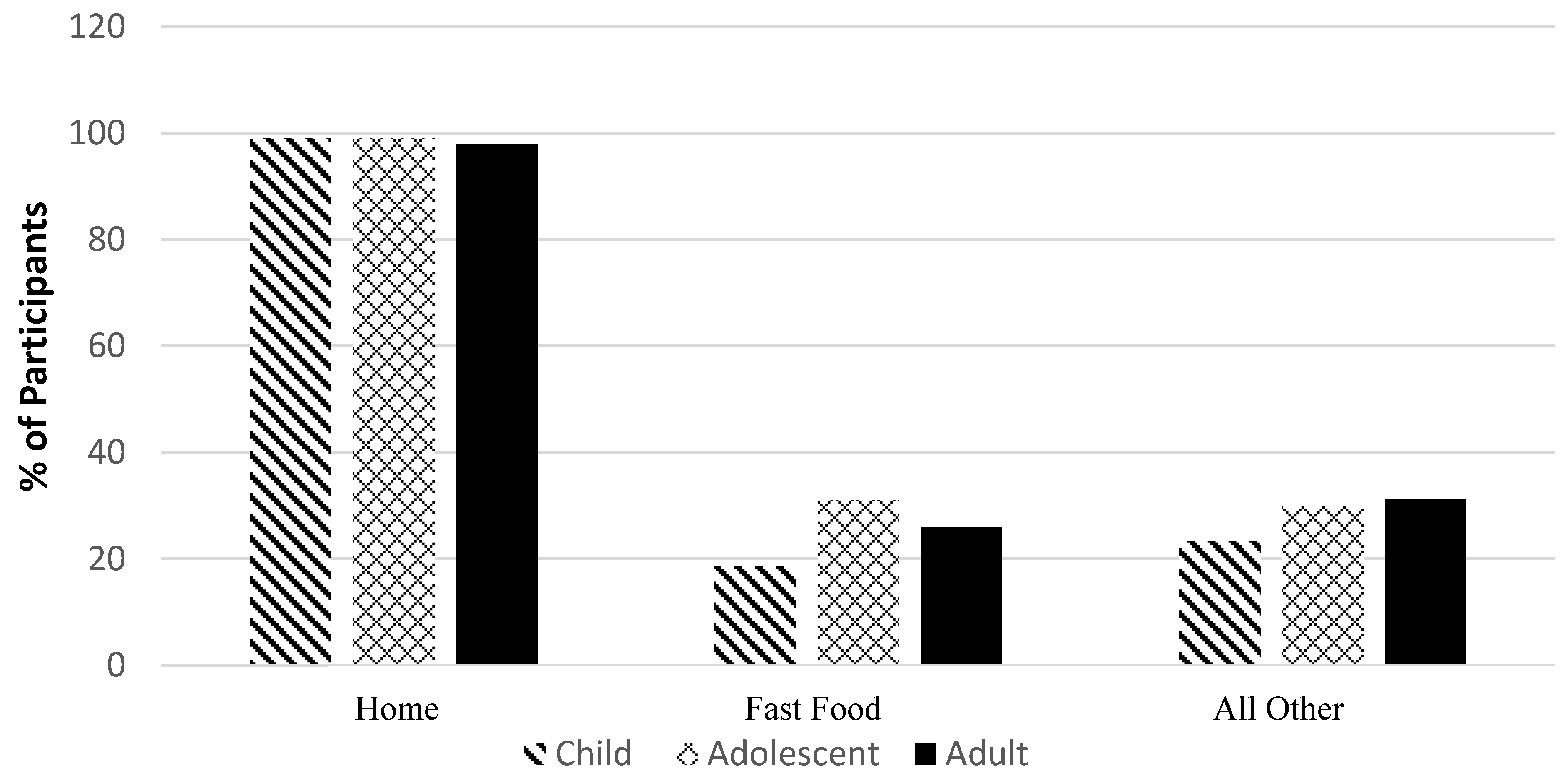
3.2. Eating Location
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Health Canada. Food and Nutrition: Measuring the Food Environment in Canada. Available online: http://www.hc-sc.gc.ca/fn-an/nutrition/pol/som-ex-sum-environ-eng.php (accessed on 23 December 2017).
- World Health Organization (WHO). Healthy Diet. Fact Sheet N394. Updated September 2015. Available online: http://www.who.int/mediacentre/factsheets/fs394/en/ (accessed on 23 December 2017).
- Swinburn, B.; Vandevijvere, S.; Kraak, V.; Sacks, G.; Snowdon, W.; Hawkes, C.; Barquera, S.; Friel, S.; Kelly, B.; Kumanyika, S.; et al. Monitoring and benchmarking government policies and actions to improve the healthiness of food environments: a proposed Government Healthy Food Environment Policy Index. Obes. Rev. 2013, 14 (Suppl. 1), 24–37. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating healthy food and eating environments: policy and environmental approaches. Ann. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Powell, L.M.; Wang, Y. Reduced away-from-home food expenditure and better nutrition knowledge and belief can improve quality of dietary intake among US adults. Public Health Nutr. 2009, 12, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Graubard, B.I. 40-year trends in meal and snack eating behaviors of American adults. J. Acad. Nutr. Diet. 2015, 115, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Jessri, M.; Nishi, S.K.; L’Abbe, M.R. Assessing the nutritional quality of diets of Canadian children and adolescents using the 2014 Health Canada Surveillance Tool Tier System. BMC Public Health. 2016, 16, 381. [Google Scholar] [CrossRef] [PubMed]
- Jessri, M.; Nishi, S.K.; L’Abbe, M.R. Assessing the Nutritional Quality of Diets of Canadian Adults Using the 2014 Health Canada Surveillance Tool Tier System. Nutrients 2015, 7, 10447–10468. [Google Scholar] [CrossRef] [PubMed]
- Jessri, M.; Wolfinger, R.D.; Lou, W.Y.; L’Abbé, M.R. Identification of dietary patterns associated with obesity in a nationally representative survey of Canadian adults: Application of a priori, hybrid, and simplified dietary pattern techniques. Am. J. Clin. Nutr. 2017, 105, 669–684. [Google Scholar] [CrossRef] [PubMed]
- Jessri, M.; Lou, W.Y.; L’Abbé, M.R. The 2015 Dietary Guidelines for Americans is associated with a more nutrient-dense diet and a lower risk of obesity. Am. J. Clin. Nutr. 2016, 104, 1378–1392. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Agriculture. Scientific Report of the 2015 Dietary Guidelines Advisory Committee. Available online: http://www.health.gov/dietaryguidelines/2015-scientific-report/PDFs/Scientific-Report-of-the-2015-Dietary-Guidelines-Advisory-Committee.pdf (accessed on 2 August 2017).
- Jessri, M.; Ng, A.P.; L’Abbé, M.R. Adapting the Healthy Eating Index 2010 for the Canadian Population: Evidence from the Canadian National Nutrition Survey. Nutrients 2017, 9, 910. [Google Scholar] [CrossRef] [PubMed]
- Brisbois, T.D.; Marsden, S.L.; Anderson, G.H.; Sievenpiper, J.L. Estimated intakes and sources of total and added sugars in the Canadian diet. Nutrients 2014, 6, 1899–1912. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [PubMed]
- Garriguet, D. Canadians’ eating habits. Health Rep. 2007, 18, 17–32. [Google Scholar] [PubMed]
- Louie, J.C.; Flood, V.; Turner, N.; Everingham, C.; Gwynn, J. Methodology for adding glycemic index values to 24-hour recalls. Nutrition 2011, 27, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Flood, J.E.; Roe, L.S.; Rolls, B.J. The effect of increased beverage portion size on energy intake at a meal. J. Ame. Diet. Assoc. 2006, 106, 1984–1990. [Google Scholar] [CrossRef] [PubMed]
- Foster-Powell, K.; Holt, S.H.; Brand-Miller, J.C. International table of glycemic index and glycemic load values: 2002. Am. J. Clin. Nutr. 2002, 76, 5–56. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Canadian Community Health Survey Cycle 2.2 Nutrition (2004)—A Guide to Accessing and Interpreting the Data. Available online: http://www.hc-sc.gc.ca/fn-an/surveill/nutrition/commun/cchs_guide_escc-eng.php (accessed on 11 January 2018).
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids; National Academy Press: Washington, DC, USA, 2005. [Google Scholar]
- Leech, R.M.; Worsley, A.; Timperio, A.; McNaughton, S.A. Understanding meal patterns: definitions, methodology and impact on nutrient intake and diet quality. Nutr. Res. Rev. 2015, 28, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; Worsley, A.; Timperio, A.; McNaughton, S.A. Characterizing eating patterns: a comparison of eating occasion definitions. Am. J. Clin. Nutr. 2015, 102, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. The Development and Use of a Surveillance Tool: The Classification of Foods in the Canadian Nutrient File According to Eating Well with Csanada’s Food Guide, 2014. Available online: http://pulications.gc.ca/collections/collection_2014/sc-hc/H164-158-2-2014-eng.pdf (accessed on 11 January 2018).
- Statistics Canada. Surveys and Statistical Programs. Canadian Community Health Survey—Annual Component (CCHS). Last Modified: 24 June 2016. Available online: http://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=3226 (accessed on 2 August 2017).
- Institute of Medicine. Dietary Reference Intakes: Water, Potassium, Sodium, Chloride, and Sulfate. National Academy Press: Washington, DC, USA, 2005. Available online: http://www.nationalacademies.org/hmd/Reports/2004/Dietary-Reference-Intakes-Water-Potassium-Sodium-Chloride-and-Sulfate.aspx (accessed on 20 December 2017).
- Deshmukh-Taskar, P.; Nicklas, T.A.; Radcliffe, J.D.; O’Neil, C.E.; Liu, Y. The relationship of breakfast skipping and type of breakfast consumed with overweight/obesity, abdominal obesity, other cardiometabolic risk factors and the metabolic syndrome in young adults. The National Health and Nutrition Examination Survey (NHANES): 1999–2006. Public Health Nutr. 2013, 16, 2073–2082. [Google Scholar] [PubMed]
- Amigo-Vazquez, I.; Busto-Zapico, R.; Errasti-Perez, J.M.; Pena-Suarez, E. Skipping breakfast, sedentarism and overweight in children. Psychol. Health Med. 2016, 21, 819–826. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture, Agricultural Research Service; Beltsville Human Nutrition Research Center. Snacking patterns of U.S. adolescents: What We Eat in America, NHANES 2005–2006. Food Surveys Research Group Dietary Data Brief (cited 2015 Sep 2). Available online: http://ars.usda.gov/Services/docs.htm?docid=19476 (accessed on 11 January 2018).
- Sebastian, R.S.; Cleveland, L.E.; Goldman, J.D. Effect of snacking frequency on adolescents' dietary intakes and meeting national recommendations. J. Adolesc. Health 2008, 42, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.; Story, M. A review of snacking patterns among children and adolescents: what are the implications of snacking for weight status? Childhood Obes. 2013, 9, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Eidner, M.B.; Lund, A.S.; Harboe, B.S.; Clemmensen, I.H. Calories and portion sizes in recipes throughout 100 years: an overlooked factor in the development of overweight and obesity? Scand. J. Public Health 2013, 41, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Muharemovic, K.; Taboul, N.; Hakansson, A. Home cooking trends and dietary illness: nutritional compliance of recipes in a Swedish food magazine 1970–2010. Scand. J. Public Health 2016, 44, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Byers, T. Dietary assessment resource manual. J. Nutr. 1994, 124 (Suppl. 11), 2245s–2317s. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
| Energy (kcal) | Saturated Fat (g) | Added Sugars (g) | Sodium (mg) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DRI | Breakfast | Lunch | Dinner | Snack | Breakfast | Lunch | Dinner | Snack | Breakfast | Lunch | Dinner | Snack | Breakfast | Lunch | Dinner | Snack |
| Boys & Girls, 2–3 year | 294 (7) | 361 (9) | 395 (11) | 391 (15) | 3.7 (0.2) | 4.8 (0.2) | 5.2 (0.2) | 5.2 (0.3) | 23.1 (0.8) | 17.6 (0.9) | 16.3 (0.7) | 36.9 (1.5) | 357 (11) | 641 (24) | 623 (23) | 340 (15) |
| Boys & Girls, 4–8 year | 337 (5) | 486 (8) | 558 (11) | 454 (10) | 3.8 (0.1) | 6.5 (0.2) | 7.3 (0.2) | 5.9 (0.2) | 25.8 (0.5) | 26.4 (0.8) | 22.9 (0.6) | 39.3 (1.0) | 424 (8) | 862 (19) | 911 (31) | 435 (14) |
| Boys, 9–13 year | 420 (11) | 608 (19) | 755 (17) | 565 (18) | 4.6 (0.2) | 8.0 (0.3) | 9.6 (0.3) | 7.1 (0.3) | 32.7 (1.3) | 30.7 (1.3) | 30.6 (1.1) | 46.8 (1.7) | 541 (18) | 1049 (31) | 1232 (34) | 572 (26) |
| Girls, 9–13 year | 336 (9) | 503 (12) | 650 (16) | 482 (15) | 3.7 (0.2) | 6.3 (0.2) | 8.3 (0.3) | 6.1 (0.3) | 24.5 (0.9) | 26.8 (0.9) | 26.7 (0.9) | 42.1 (1.7) | 442 (14) | 911 (34) | 1976 (39) | 471 (20) |
| Boys, 14–18 year | 458 (14) | 653 (18) | 910 (18) | 718 (25) | 5.3 (0.3) | 8.0 (0.3) | 11.8 (0.4) | 9.4 (0.4) | 32.5 (1.3) | 33.5 (1.2) | 35.3 (1.3) | 52.3 (2.3) | 616 (24) | 1123 (36) | 1476 (41) | 814 (39) |
| Girls, 14–18 year | 321 (10) | 475 (12) | 668 (13) | 486 (18) | 3.5 (0.2) | 5.7 (0.2) | 7.8 (0.2) | 6.5 (0.4) | 22.9 (1.0) | 24.2 (0.9) | 27.2 (1.1) | 39.2 (1.7) | 398 (16) | 866 (31) | 1104 (30) | 500 (23) |
| Men, 19–30 year | 430 (16) | 605 (21) | 952 (27) | 515 (23) | 5.2 (0.3) | 7.0 (0.3) | 11.3 (0.5) | 6.4 (0.3) | 26.4 (1.2) | 26.7 (1.4) | 30.3 (1.1) | 34.2 (1.8) | 602 (33) | 1136 (63) | 1624 (74) | 584 (32) |
| Women, 19–30 year | 316 (12) | 445 (17) | 628 (16) | 379 (16) | 3.7 (0.3) | 5.3 (0.3) | 7.8 (0.3) | 4.7 (0.3) | 22.2 (1.1) | 19.4 (0.9) | 22.4 (0.9) | 28.6 (1.4) | 399 (20) | 852 (53) | 1009 (29) | 384 (23) |
| Men, 31–50 year | 414 (12) | 622 (18) | 886 (21) | 409 (18) | 5.3 (0.3) | 7.9 (0.3) | 10.6 (0.4) | 5.2 (0.3) | 23.3 (1.0) | 24.6 (1.1) | 25.7 (1.0) | 30.0 (1.6) | 572 (24) | 1117 (38) | 1407 (45) | 423 (26) |
| Women, 31–50 year | 303 (8) | 417 (12) | 684 (18) | 340 (13) | 3.8 (0.2) | 5.0 (0.2) | 8.2 (0.3) | 4.7 (0.3) | 17.5 (0.8) | 17.6 (0.9) | 20.8 (0.9) | 25.2 (1.1) | 403 (14) | 810 (27) | 1165 (34) | 327 (17) |
| Men, 51–70 year | 371 (9) | 504 (14) | 823 (19) | 358 (14) | 4.4 (0.2) | 6.4 (0.3) | 9.7 (0.3) | 4.7 (0.3) | 21.3 (0.7) | 20.3 (0.9) | 25.0 (1.0) | 25.0 (1.2) | 518 (15) | 1060 (39) | 1318 (38) | 364 (18) |
| Women, 51–70 year | 311 (8) | 416 (11) | 620 (12) | 264 (9) | 3.3 (0.1) | 5.2 (0.2) | 7.3 (0.2) | 3.2 (0.2) | 18.8 (0.6) | 17.0 (0.6) | 20.5 (0.7) | 21.2 (0.8) | 404 (11) | 799 (31) | 1067 (26) | 237 (12) |
| Men, >70 year | 406 (10) | 483 (16) | 676 (20) | 237 (12) | 4.5 (0.2) | 5.9 (0.3) | 8.1 (0.4) | 3.1 (0.2) | 25.8 (1.2) | 18.5 (0.9) | 25.6 (1.2) | 18.8 (1.1) | 521 (18) | 962 (35) | 1138 (42) | 204 (15) |
| Women, >70 year | 318 (7) | 416 (11) | 526 (11) | 208 (8) | 3.2 (0.1) | 5.3 (0.3) | 6.1 (0.2) | 2.8 (0.2) | 21.4 (0.7) | 17.3 (0.7) | 21.4 (0.7) | 17.0 (0.7) | 406 (15) | 807 (33) | 878 (26) | 176 (8) |
| Children (≥2 to <12 years, n = 4215) | Adolescents (≥12 to <19 years, n = 4649) | Adults (aged ≥ 19 years, n = 11538) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Units | <50% kcal/d from snacks * | ≥50% kcal/d from snacks † | Pr > F | <50% kcal/d from snacks * | ≥50% kcal/d from snacks † | Pr > F | <50% kcal/d from snacks * | ≥50% kcal/d from snacks † | Pr > F |
| Energy | Kcal | 1771 (12) | 1935 (55) | 0.005 | 2490 (24) | 2741 (95) | 0.008 | 2418 (19) | 2488 (64) | 0.258 |
| Protein | %Energy | 16.0 (0.1) | 12.8 (0.3) | <0.0001 | 14.4 (0.1) | 11.7 (0.4) | <0.0001 | 14.8 (0.1) | 12.6 (0.4) | <0.0001 |
| Fat | %Energy | 31.3 (0.2) | 33.6 (0.6) | 0.000 | 29.7 (0.2) | 28.2 (0.8) | 0.048 | 31.9 (0.2) | 35.2 (0.9) | 0.000 |
| Saturated Fat | %Energy | 10.9 (0.1) | 9.6 (0.4) | 0.004 | 10.5 (0.1) | 10.7 (0.4) | 0.677 | 10.3 (0.1) | 10.8 (0.4) | 0.237 |
| Carbohydrate | %Energy | 55.9 (0.3) | 60.1 (0.9) | <0.0001 | 53.7 (0.3) | 55.5 (1.0) | 0.059 | 48.5 (0.3) | 50.0 (0.9) | 0.122 |
| MUFA | %Energy | 11.3 (0.1) | 11.0 (0.4) | 0.418 | 12.2 (0.1) | 12.4 (0.3) | 0.465 | 12.7 (0.1) | 14.6 (0.5) | 0.001 |
| PUFA | %Energy | 4.6 (0.1) | 4.9 (0.2) | 0.183 | 5.2 (0.1) | 5.7 (0.3) | 0.054 | 5.7 (0.1) | 6.7 (0.3) | 0.000 |
| Fiber | g/1000 kcal | 7.4 (0.1) | 7.7 (0.4) | 0.290 | 6.7 (0.1) | 6.8 (0.2) | 0.677 | 8.9 (0.1) | 8.1 (0.4) | 0.023 |
| Alcohol | %Energy | 0.0 (0.0) | 0.0 (0.0) | 0.258 | 0.6 (0.1) | 0.1 (0.1) | 0.032 | 3.0 (0.2) | 1.8 (0.6) | 0.060 |
| Vitamin A | RE/1000 kcal | 319 (6) | 266 (14) | 0.000 | 280 (6) | 246 (24) | 0.181 | 370 (10) | 298 (16) | <0.0001 |
| Vitamin D | ug/1000 kcal | 3.3 (0.1) | 2.4 (0.2) | <0.0001 | 2.7 (0.1) | 2.0 (0.1) | <0.0001 | 3.0 (0.1) | 2.2 (0.2) | <0.0001 |
| Thiamin | mg/1000 kcal | 0.9 (0.0) | 0.7 (0.0) | <0.0001 | 0.9 (0.0) | 0.8 (0.0) | 0.000 | 0.8 (0.0) | 0.7 (0.0) | <0.0001 |
| Riboflavin | mg/1000 kcal | 1.1 (0.0) | 0.9 (0.0) | <0.0001 | 1.0 (0.0) | 0.8 (0.0) | <0.0001 | 1.0 (0.0) | 0.9 (0.0) | 0.003 |
| Niacin | NE/1000 kcal | 15.9 (0.2) | 13.7 (0.4) | <0.0001 | 16.6 (0.2) | 14.1 (0.5) | <0.0001 | 19.8 (0.2) | 16.0 (0.5) | <0.0001 |
| Vitamin B6 | mg/1000 kcal | 0.8 (0.0) | 0.8 (0.0) | 0.155 | 0.8 (0.0) | 0.6 (0.0) | <0.0001 | 1.0 (0.0) | 0.8 (0.0) | <0.0001 |
| Folate | ug/1000 kcal | 94.7 (2.1) | 90.5 (6.8) | 0.529 | 90.7 (1.6) | 82.3 (4.3) | 0.047 | 120 (2) | 100 (5) | <0.0001 |
| Vitamin B12 | ug/1000 kcal | 1.9 (0.0) | 1.5 (0.2) | 0.053 | 1.8 (0.0) | 1.4 (0.1) | <0.0001 | 2.2 (0.1) | 1.4 (0.1) | <0.0001 |
| Vitamin C | mg/1000 kcal | 77.7 (2.8) | 77.6 (7.7) | 0.990 | 67.4 (2.1) | 54.9 (4.1) | 0.006 | 63.1 (1.1) | 58.1 (6.3) | 0.446 |
| Calcium | mg/1000 kcal | 552 (8) | 446 (19) | <0.0001 | 473 (7) | 413 (16) | 0.000 | 416 (4) | 373 (17) | 0.009 |
| Phosphorus | mg/1000 kcal | 669 (7) | 591 (17) | <0.0001 | 619 (6) | 565 (15) | 0.001 | 664 (5) | 575 (16) | <0.0001 |
| Potassium | mg/1000 kcal | 1404 (15) | 1305 (54) | 0.047 | 1308 (14) | 1164 (37) | 0.000 | 1583 (12) | 1359 (36) | <0.0001 |
| Sodium | mg/1000 kcal | 1434 (18) | 1319 (63) | 0.064 | 1466 (14) | 1365 (39) | 0.014 | 1544 (18) | 1405 (45) | 0.003 |
| Magnesium | mg/1000 kcal | 138 (2) | 133 (4) | 0.070 | 131 (1) | 124 (3) | 0.039 | 167 (1) | 153 (5) | 0.004 |
| Iron | mg/1000 kcal | 6.9 (0.1) | 6.5 (0.2) | 0.182 | 6.8 (0.1) | 6.0 (0.2) | <0.0001 | 7.0 (0.1) | 6.2 (0.2) | 0.000 |
| Zinc | mg/1000 kcal | 5.0 (0.1) | 4.1 (0.2) | 0.000 | 4.9 (0.1) | 4.2 (0.1) | <0.0001 | 5.6 (0.1) | 4.5 (0.1) | <0.0001 |
| Added Sugar | %Energy | 13.2 (0.4) | 17.5 (1.3) | 0.000 | 14.4 (0.3) | 16.9 (1.1) | 0.024 | 9.1 (0.2) | 13.5 (0.9) | <0.0001 |
| Glycemic Index | GI | 54.7 (0.2) | 55.7 (0.5) | 0.064 | 55.8 (0.2) | 56.1 (0.6) | 0.655 | 52.6 (0.2) | 53.4 (0.7) | 0.248 |
| Glycemic Load | GL | 136 (1) | 168 (7) | <0.0001 | 188 (2) | 215 (8) | 0.001 | 155 (2) | 171 (7) | 0.034 |
| Energy Density | kcal/g | 2.0 (0.0) | 2.1 (0.1) | 0.061 | 2.1 (0.0) | 2.3 (0.1) | 0.005 | 1.8 (0.0) | 2.3 (0.1) | <0.0001 |
| Energy (kcal) | Saturated Fat (g) | Added Sugars (g) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| DRI | Home * | Fast Food † | All Other ‡ | Home * | Fast Food † | All Other ‡ | Home * | Fast Food † | All Other ‡ |
| Boys & Girls, 2–3 year | 1411 (23) | 377 (29) | 505 (36) | 19.0 (0.4) | 5.0 (0.5) | 7.1 (0.6) | 98 (2) | 21 (3) | 31 (2) |
| Boys & Girls, 4–8 year | 1689 (19) | 529 (23) | 502 (27) | 21.5 (0.4) | 7.0 (0.4) | 6.7 (0.4) | 109 (2) | 33 (2) | 33 (2) |
| Boys, 9–13 year | 2090 (35) | 761 (31) | 812 (83) | 25.7 (0.6) | 10.4 (0.5) | 11.3 (1.4) | 130 (3) | 46 (3) | 59 (6) |
| Girls, 9–13 year | 1786 (29) | 617 (29) | 588 (41) | 21.8 (0.5) | 7.6 (0.5) | 8.7 (1.0) | 113 (2) | 37 (2) | 41 (3) |
| Boys, 14–18 year | 2307 (45) | 1082 (38) | 795 (40) | 28.5 (0.7) | 13.4 (0.6) | 10.9 (0.8) | 134 (3) | 68 (4) | 57 (3) |
| Girls, 14–18 year | 1615 (28) | 692 (26) | 673 (42) | 19.1 (0.5) | 8.7 (0.4) | 8.6 (0.7) | 99 (2) | 44 (3) | 43 (4) |
| Men, 19–30 year | 2038 (48) | 958 (48) | 1014 (57) | 23.3 (0.8) | 12.0 (0.7) | 11.5 (0.7) | 103 (3) | 52 (3) | 49 (5) |
| Women, 19–30 year | 1498 (36) | 651 (30) | 598 (35) | 17.5 (0.7) | 8.7 (0.5) | 6.9 (0.4) | 87 (2) | 33 (2) | 32 (2) |
| Men, 31–50 year | 2036 (38) | 767 (43) | 722 (44) | 24.0 (0.7) | 10.8 (0.7) | 9.1 (0.6) | 97 (3) | 36 (2) | 34 (2) |
| Women, 31–50 year | 1509 (31) | 498 (23) | 720 (42) | 18.3 (0.6) | 7.4 (0.5) | 8.5 (0.5) | 78 (2) | 24 (2) | 30 (2) |
| Men, 51–70 year | 1892 (31) | 504 (32) | 715 (41) | 21.9 (0.6) | 7.4 (0.6) | 10.0 (0.8) | 89 (2) | 23 (2) | 28 (2) |
| Women, 51–70 year | 1464 (22) | 484 (39) | 580 (32) | 16.8 (0.4) | 7.4 (0.7) | 6.8 (0.5) | 76 (1) | 18 (1) | 27 (2) |
| Men, >70 year | 1676 (35) | 464 (37) | 785 (105) | 19.5 (0.7) | 6.2 (0.7) | 10.4 (1.7) | 87 (2) | 17 (2) | 30 (8) |
| Women, >70 year | 1383 (22) | 370 (30) | 608 (42) | 16.1 (0.4) | 4.8 (0.4) | 7.7 (0.5) | 77 (2) | 16 (2) | 26 (2) |
| Sodium (mg) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DRI | Home | Someone Else’s Home | Restaurant, Fast Food/Pizza | Take-Out | Restaurant with Waiter | Bar/Tavern/Lounge | Vending Machine | Restaurant No Additional Info | Cafeteria, Not At School | Cafeteria, at School | Child Care Centre | Family/Adult Care Centre | Other | Store ° | At Work |
| Boys & Girls, 2–3 year | 1731(40) | 27(7) | 76(14) | 0(.) | 5.7(1.5) | 0.2(0.1) | 0.8(0.4) | 1.4(1.0) | 4.2(2.0) | 80.2(11.3) | 2.3(1.1) | 123.8(21.5) | 3.0(1.8) | 4.0(1.7) | 0(0) |
| Boys & Girls, 4–8 year | 2270(41) | 35(6) | 115(14) | 0(0) | 31.9(5.8) | 0.9(0.3) | 4.8(2.1) | 4.4(1.7) | 37.3(6.6) | 38.1(7.5) | 8.2(5.4) | 111.7(11.5) | 7.0(1.6) | 12.3(4.3) | 0.1(0.1) |
| Boys, 9–13 year | 2876(57) | 145(33) | 175(16) | 3.3(2.3) | 62.8(11.9) | 1.8(0.6) | 4.6(2.7) | 15.5(5.0) | 61.7(16.3) | 7.3(4.0) | 2.5(1.6) | 96.5(12.9) | 13.0(5.0) | 17.0(3.8) | 0(0) |
| Girls, 9–13 year | 2498(62) | 78(17) | 125(12) | 0.1(0.1) | 33.3(5.8) | 1.3(0.4) | 10.0(5.2) | 11.4(4.2) | 47.5(7.6) | 3.9(2.0) | 0.4(0.2) | 125.5(15.9) | 11.9(4.1) | 12.8(4.2) | 0(0) |
| Boys, 14–18 year | 3196(75) | 144(18) | 401(29) | 5.0(2.1) | 101.5(16.0) | 18.3(8.1) | 6.2(2.0) | 17.8(4.5) | 85.5(12.1) | 0(0) | 0.6(0.4) | 101.6(13.7) | 19.5(8.3) | 24.9(4.7) | 3.4(1.9) |
| Girls, 14–18 year | 2171(52) | 116(16) | 294(25) | 1.1(0.5) | 60.8(8.9) | 4.5(1.1) | 13.2(4.4) | 19.4(4.8) | 98.2(12.6) | 0.1(0.1) | 2.5(1.6) | 102.8(13.3) | 18.2(4.7) | 25.8(7.1) | 4.1(1.9) |
| Men, 19–30 year | 2896(108) | 287(31) | 438(35) | 37.6(11.5) | 122.4(20.5) | 18.4(7.9) | 11.8(3.3) | 25.3(6.1) | 43.5(24.2) | 0.2(0.2) | 0.4(0.3) | 104.7(20.7) | 9.5(3.8) | 56.5(15.7) | 11.6(3.2) |
| Women, 19–30 year | 2000(71) | 187(21) | 245(21) | 7.8(2.7) | 110.5(21.1) | 5.2(1.5) | 9.9(4.7) | 13.5(2.8) | 21.9(6.4) | 1.7(1.0) | 4.2(1.5) | 89.3(17.6) | 10.8(4.3) | 17.6(3.7) | 13.0(3.6) |
| Men, 31–50 year | 2781(70) | 202(22) | 274(26) | 14.8(3.3) | 76.9(12.6) | 27.4(13.4) | 9.5(5.1) | 50.8(9.5) | 2.5(1.2) | 0(0) | 0.7(0.4) | 94.2(25.1) | 23.5(11.3) | 30.8(7.7) | 19.4(4.4) |
| Women, 31–50 year | 2140(55) | 227(27) | 150(16) | 5.1(1.8) | 59.8(9.2) | 4.6(1.5) | 14.4(4.1) | 52.8(11.4) | 11.4(5.3) | 1.7(1.4) | 3.1(1.8) | 63.7(12.8) | 5.7(2.3) | 16.6(2.7) | 15.9(3.3) |
| Men, 51–70 year | 2772(58) | 270(34) | 115(14) | 7.4(2.3) | 43.0(9.4) | 3.2(1.1) | 15.3(7.0) | 25.2(5.7) | 0.8(0.6) | 0(0) | 1.0(0.4) | 38.9(7.2) | 12.5(4.5) | 21.3(8.0) | 7.4(1.6) |
| Women, 51–70 year | 2140(47) | 162(17) | 91(13) | 9.6(4.4) | 23.1(3.9) | 1.3(0.3) | 7.8(2.4) | 24.4(5.1) | 0.7(0.3) | 0(0) | 6.6(2.5) | 70.8(9.5) | 15.8(7.0) | 10.9(2.4) | 6.9(1.9) |
| Men, >70 year | 2483(65) | 165(32) | 75(17) | 4.4(2.1) | 14.8(4.3) | 0.4(0.4) | 1.0(0.8) | 10.6(3.3) | 0(.) | 0(0) | 48.0(29.2) | 42.4(8.9) | 15.0(5.5) | 4.5(1.9) | 0.1(0.1) |
| Women, >70 year | 2033(54) | 106(14) | 37(6) | 1.0(0.5) | 11.1(4.2) | 0.3(0.2) | 4.6(2.2) | 17.2(4.3) | 0.8(0.7) | 0(0) | 26.8(7.3) | 50.2(8.0) | 8.9(4.5) | 3.1(1.1) | 0.1(0) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishi, S.K.; Jessri, M.; L’Abbé, M. Assessing the Dietary Habits of Canadians by Eating Location and Occasion: Findings from the Canadian Community Health Survey, Cycle 2.2. Nutrients 2018, 10, 682. https://doi.org/10.3390/nu10060682
Nishi SK, Jessri M, L’Abbé M. Assessing the Dietary Habits of Canadians by Eating Location and Occasion: Findings from the Canadian Community Health Survey, Cycle 2.2. Nutrients. 2018; 10(6):682. https://doi.org/10.3390/nu10060682
Chicago/Turabian StyleNishi, Stephanie K., Mahsa Jessri, and Mary L’Abbé. 2018. "Assessing the Dietary Habits of Canadians by Eating Location and Occasion: Findings from the Canadian Community Health Survey, Cycle 2.2" Nutrients 10, no. 6: 682. https://doi.org/10.3390/nu10060682
APA StyleNishi, S. K., Jessri, M., & L’Abbé, M. (2018). Assessing the Dietary Habits of Canadians by Eating Location and Occasion: Findings from the Canadian Community Health Survey, Cycle 2.2. Nutrients, 10(6), 682. https://doi.org/10.3390/nu10060682