Adherence to National Dietary Guidelines in Association with Oral Health Impact on Quality of Life

 , ,
, ,
Abstract
1. Introduction
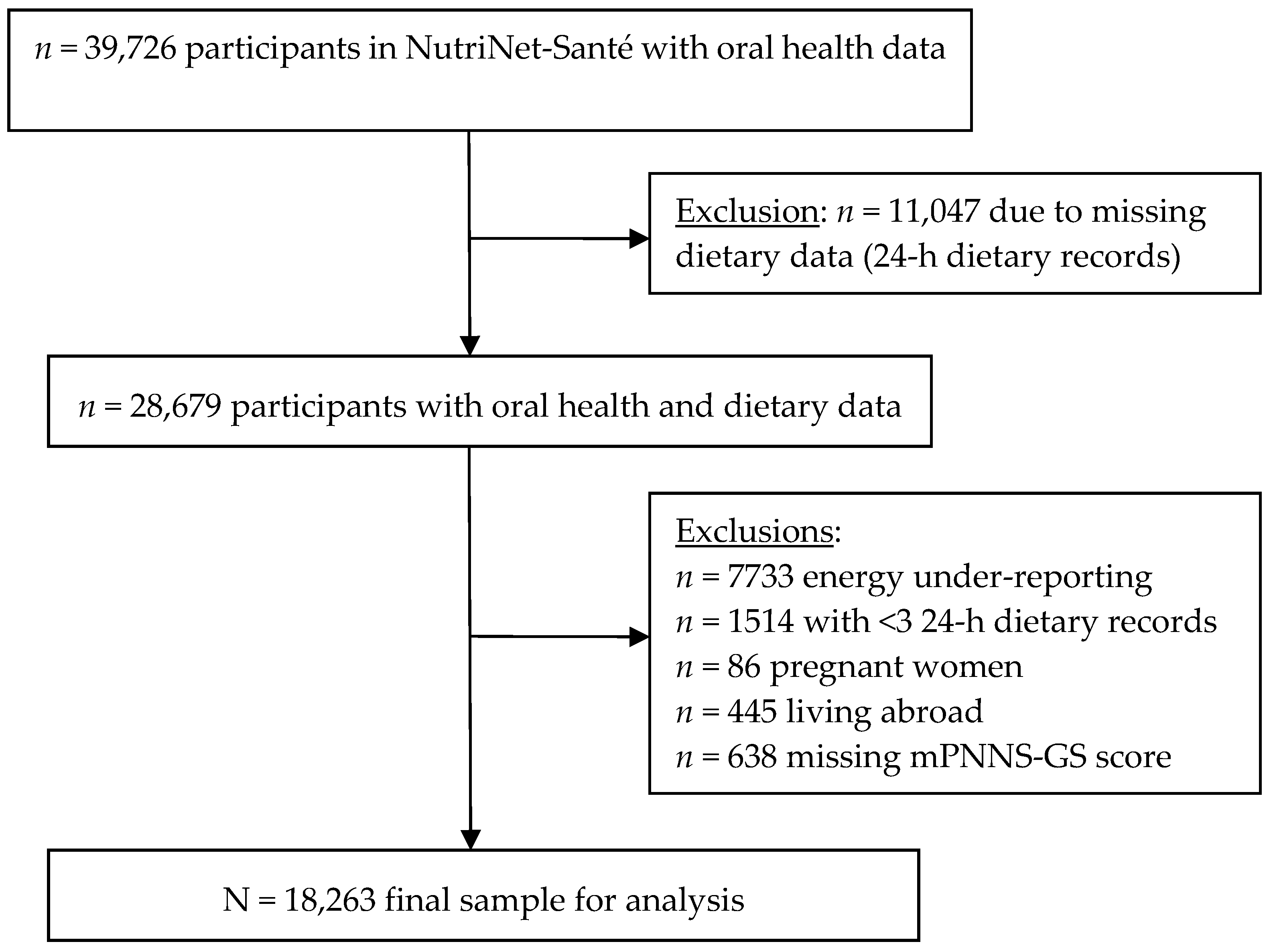
2. Materials and Methods
2.1. NutriNet-Santé e-Cohort
2.2. Oral Health Assessment
2.3. Diet Quality Assessment
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Association between Oral Health-Related QOL and Diet Quality
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Oral Health. Fact Sheet No. 318; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Moynihan, P.; Petersen, P.E. Diet, nutrition and the prevention of dental diseases. Public Health Nutr. 2004, 7, 201–226. [Google Scholar] [CrossRef] [PubMed]
- Ha, D.H.; Spencer, A.J.; Thomson, W.M.; Scott, J.A.; Do, L.G. Commonality of risk factors for mothers’ poor oral health and general health: Baseline analysis of a population-based birth cohort study. Matern. Child Health J. 2018, 22, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Negrato, C.A.; Tarzia, O.; Jovanovic, L.; Chinellato, L.E. Periodontal disease and diabetes mellitus. J. Appl. Oral Sci. 2013, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- De Marchi, R.J.; Hugo, F.N.; Hilgert, J.B.; Padilha, D.M. Association between oral health status and nutritional status in south Brazilian independent-living older people. Nutrition 2008, 24, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; Steele, J.G.; Marcenes, W.; Finch, S.; Walls, A.W. The relationship between oral health status and Body Mass Index among older people: A national survey of older people in Great Britain. Br. Dent. J. 2002, 192, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.J.; Willett, W.C.; Douglass, C.W. The impact of edentulousness on food and nutrient intake. J. Am. Dent. Assoc. 1996, 127, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Sahyoun, N.R.; Lin, C.L.; Krall, E. Nutritional status of the older adult is associated with dentition status. J. Am. Diet. Assoc. 2003, 103, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Nowjack-Raymer, R.E.; Sheiham, A. Numbers of natural teeth, diet, and nutritional status in U.S. adults. J. Dent. Res. 2007, 86, 1171–1175. [Google Scholar] [CrossRef] [PubMed]
- Marcenes, W.; Steele, J.G.; Sheiham, A.; Walls, A.W. The relationship between dental status, food selection, nutrient intake, nutritional status, and body mass index in older people. Cad. Saude Publica 2003, 19, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Guenther, P.M.; Krebs-Smith, S.M.; Reedy, J.; Britten, P.; Juan, W.; Lino, M.; Carlson, A.; Hiza, H.A.; Basiotis, P.P. Healthy Eating Index-2005; USDA, Center for Nutrition Policy and Promotion: Alexandria, VA, USA, 2008.
- Savoca, M.R.; Arcury, T.A.; Leng, X.; Chen, H.; Bell, R.A.; Anderson, A.M.; Kohrman, T.; Frazier, R.J.; Gilbert, G.H.; Quandt, S.A. Severe tooth loss in older adults as a key indicator of compromised dietary quality. Public Health Nutr. 2010, 13, 466–474. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Oral health report. In Eurobarometer 72.3; European Commission: Brussels, Belgium, 2010. [Google Scholar]
- El Osta, N.; Hennequin, M.; Tubert-Jeannin, S.; Abboud Naaman, N.B.; El Osta, L.; Geahchan, N. The pertinence of oral health indicators in nutritional studies in the elderly. Clin. Nutr. 2014, 33, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E. Mini nutritional assessment. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Agence Nationale de la Recherche. ALIMASSENS: Toward Offering Healthy Food Products Better Adapted to Elderly People; Agence Nationale de la Recherche: Paris, France, 2014. [Google Scholar]
- Hercberg, S.; Castetbon, K.; Czernichow, S.; Malon, A.; Mejean, C.; Kesse, E.; Touvier, M.; Galan, P. The NutriNet-Santé study: A web-based prospective study on the relationship between nutrition and health and determinants of dietary patterns and nutritional status. BMC Public Health 2010, 10, 242. [Google Scholar] [CrossRef] [PubMed]
- Atchison, K.A.; Dolan, T.A. Development of the Geriatric Oral Health Assessment Index. J. Dent. Educ. 1990, 54, 680–687. [Google Scholar] [PubMed]
- Tubert-Jeannin, S.; Riordan, P.J.; Morel-Papernot, A.; Porcheray, S.; Saby-Collet, S. Validation of an oral health quality of life index (GOHAI) in France. Community Dent. Oral Epidemiol. 2003, 31, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Kishi, M.; Aizawa, F.; Matsui, M.; Yokoyama, Y.; Abe, A.; Minami, K.; Suzuki, R.; Miura, H.; Sakata, K.; Ogawa, A. Oral health-related quality of life and related factors among residents in a disaster area of the Great East Japan Earthquake and giant tsunami. Health Qual. Life Outcomes 2015, 13, 143. [Google Scholar] [CrossRef] [PubMed]
- Santé Publique France. PNNS: Un Plan Pour Améliorer L’état de Santé de la Population; Santé Publique France: Saint Denis, France, 2018. [Google Scholar]
- Le Moullec, N.; Deheeger, M.; Preziosi, P.; Seraphim, P.M.; Valeix, P.; Rolland-Cachera, M.; Courcy, J.; Christidès, J.-P.; Cherouvrier, F.; Galan, P.; et al. Validation du manuel photos utilisé pour l'enquête alimentaire de l'étude SU.VI.MAX. Cahier Nutr. Diétét. 1996, 31, 158–164. [Google Scholar]
- Etude NutriNet-Santé. Table de Composition des Aliments; Économica: Paris, France, 2013; ISBN 978-2-7178-6537-0. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39, S5–S41. [Google Scholar]
- Estaquio, C.; Kesse-Guyot, E.; Deschamps, V.; Bertrais, S.; Dauchet, L.; Galan, P.; Hercberg, S.; Castetbon, K. Adherence to the French Programme National Nutrition Sante Guideline Score is associated with better nutrient intake and nutritional status. J. Am. Diet. Assoc. 2009, 109, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- Hercberg, S.; Chat-Yung, S.; Chaulia, M. The French National Nutrition and Health Program: 2001-2006-2010. Int. J. Public Health 2008, 53, 68–77. [Google Scholar] [CrossRef] [PubMed]
- IPAQ Group. IPAQ Scoring Protocol. Available online: www.ipaq.ki.se (accessed on 18 April 2018).
- Shinkai, R.S.; Hatch, J.P.; Sakai, S.; Mobley, C.C.; Saunders, M.J.; Rugh, J.D. Oral function and diet quality in a community-based sample. J. Dent. Res. 2001, 80, 1625–1630. [Google Scholar] [CrossRef] [PubMed]
- Irz, X.; Fratiglioni, L.; Kuosmanen, N.; Mazzocchi, M.; Modugno, L.; Nocella, G.; Shakersain, B.; Traill, W.B.; Xu, W.; Zanello, G. Sociodemographic determinants of diet quality of the EU elderly: A comparative analysis in four countries. Public Health Nutr. 2014, 17, 1177–1189. [Google Scholar] [CrossRef] [PubMed]
- Ervin, R.B.; Dye, B.A. The effect of functional dentition on Healthy Eating Index scores and nutrient intakes in a nationally representative sample of older adults. J. Public Health Dent. 2009, 69, 207–216. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ageing and Health. Fact Sheet No. 404; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization. Noncommunicable Diseases. Fact Sheet; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Bernstein, M.; Munoz, N.; Academy of Nutrition and Dietetics. Position of the Academy of Nutrition and Dietetics: Food and nutrition for older adults: Promoting health and wellness. J. Acad. Nutr. Diet. 2012, 112, 1255–1277. [Google Scholar] [CrossRef] [PubMed]
- Bartali, B.; Salvini, S.; Turrini, A.; Lauretani, F.; Russo, C.R.; Corsi, A.M.; Bandinelli, S.; D’Amicis, A.; Palli, D.; Guralnik, J.M.; et al. Age and disability affect dietary intake. J. Nutr. 2003, 133, 2868–2873. [Google Scholar] [CrossRef] [PubMed]
- Tada, A.; Miura, H. Systematic review of the association of mastication with food and nutrient intake in the independent elderly. Arch. Gerontol. Geriatr. 2014, 59, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Shatenstein, B.; Gauvin, L.; Keller, H.; Richard, L.; Gaudreau, P.; Giroux, F.; Gray-Donald, K.; Jabbour, M.; Morais, J.A.; Payette, H. Baseline determinants of global diet quality in older men and women from the NuAge cohort. J. Nutr. Health Aging 2013, 17, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Thiele, S.; Mensink, G.B.; Beitz, R. Determinants of diet quality. Public Health Nutr. 2004, 7, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Grech, A.; Sui, Z.; Siu, H.Y.; Zheng, M.; Allman-Farinelli, M.; Rangan, A. Socio-demographic determinants of diet quality in Australian adults using the validated Healthy Eating Index for Australian Adults (HEIFA-2013). Healthcare 2017, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- De Andrade, F.B.; Lebrao, M.L.; Santos, J.L.F.; Duarte, Y.A.; Teixeira, D.S. Factors related to poor self-perceived oral health among community-dwelling elderly individuals in São Paulo, Brazil. Cad. Saúde Pública 2012, 28, 1965–1975. [Google Scholar] [CrossRef]
- Touger-Decker, R.; Mobley, C.; Academy of Nutrition & Dietetics. Position of the Academy of Nutrition and Dietetics: Oral health and nutrition. J. Acad. Nutr. Diet. 2013, 113, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Nam, D.S.; Kong, C. Variability in nutrient composition of cereal grains from different origins. Springerplus 2016, 5, 419. [Google Scholar] [CrossRef] [PubMed]
- Pegon-Machat, E.; Faulks, D.; Eaton, K.A.; Widström, E.; Hugues, P.; Tubert-Jeannin, S. The healthcare system and the provision of oral healthcare in EU Member States: France. Br. Dent. J. 2016, 220, 197–203. [Google Scholar] [CrossRef] [PubMed]
- LaMonte, M.J.; Genco, R.J.; Hovey, K.M.; Wallace, R.B.; Freudenheim, J.L.; Michaud, D.S.; Mai, X.; Tinker, L.F.; Salazar, C.R.; Andrews, C.A.; et al. History of periodontitis diagnosis and edentulism as predictors of cardiovascular disease, stroke, and mortality in postmenopausal women. J. Am. Heart Assoc. 2017, 6, e004518. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| GOHAI Score | p1 | ||||||
|---|---|---|---|---|---|---|---|
| 57–60 (n = 7233) | 51–56 (n = 7667) | ≤50 (n = 3363) | |||||
| Sex | 0.63 | ||||||
| Men | 1909 | (26.4) | 2058 | (26.8) | 916 | (27.2) | |
| Women | 5324 | (73.6) | 5609 | (73.2) | 2447 | (72.8) | |
| Age, mean (SD) | 54.3 | (14.2) | 56.4 | (13.6) | 59.8 | (12.5) | <0.0001 |
| GOHAI scores, mean (SD) | <0.0001 | ||||||
| Overall score | 58.4 | (1.1) | 53.9 | (1.7) | 47.3 | (2.8) | |
| Physical function subscore | 19.9 | (0.3) | 19.0 | (1.3) | 16.6 | (1.7) | |
| Psychosocial function subscore | 24.3 | (0.8) | 21.9 | (1.6) | 18.8 | (2.0) | |
| Discomfort/pain subscore | 14.2 | (0.8) | 12.9 | (1.3) | 11.2 | (1.5) | |
| Marital status | 0.0003 | ||||||
| Married/cohabiting | 5554 | (76.8) | 5708 | (74.4) | 2479 | (73.7) | |
| Living alone | 1679 | (23.2) | 1959 | (25.6) | 884 | (26.3) | |
| Educational level | <0.0001 | ||||||
| Up to high school | 2012 | (27.8) | 2377 | (31.0) | 1385 | (41.2) | |
| Undergraduate degree | 2263 | (31.3) | 2403 | (31.3) | 1003 | (29.8) | |
| Graduate degree | 2958 | (40.9) | 2887 | (37.7) | 975 | (29.0) | |
| Occupational status | <0.0001 | ||||||
| Manual/blue collar | 885 | (12.2) | 877 | (11.4) | 382 | (11.4) | |
| Office work/administrative | 1172 | (16.2) | 1140 | (14.9) | 386 | (11.5) | |
| Professional/executive staff | 1765 | (24.4) | 1627 | (21.2) | 488 | (14.5) | |
| Retired | 2788 | (38.6) | 3361 | (43.8) | 1790 | (53.2) | |
| Household income (monthly) | <0.0001 | ||||||
| <1200 € | 553 | (7.7) | 578 | (7.5) | 297 | (8.8) | |
| 1200 €–1799 € | 1253 | (17.3) | 1416 | (18.5) | 734 | (21.8) | |
| 1800 €–2699 € | 1909 | (26.4) | 2040 | (26.6) | 901 | (26.8) | |
| ≥2700 € | 2606 | (36.0) | 2666 | (34.8) | 979 | (29.1) | |
| Missing/no response | 912 | (12.6) | 967 | (12.6) | 452 | (13.4) | |
| Physical activity 2 | 0.06 | ||||||
| Low | 2701 | (37.3) | 2829 | (36.9) | 1339 | (39.8) | |
| Moderate | 2965 | (41.0) | 3196 | (41.7) | 1332 | (39.6) | |
| Vigorous | 1567 | (21.7) | 1642 | (21.4) | 692 | (20.6) | |
| Smoking status | <0.0001 | ||||||
| Never | 3976 | (55.0) | 3836 | (50.0) | 1513 | (45.0) | |
| Former | 2693 | (37.2) | 3149 | (41.1) | 1542 | (45.8) | |
| Current | 564 | (7.8) | 682 | (8.9) | 308 | (9.2) | |
| Body Mass Index, kg/m2, mean (SD) | 23.7 | (4.1) | 23.8 | (4.2) | 24.5 | (4.6) | <0.0001 |
| Diabetes 3 | 191 | (2.6) | 252 | (3.3) | 173 | (5.2) | <0.0001 |
| Cancer 4 | 656 | (9.3) | 808 | (10.7) | 394 | (12.0) | 0.0002 |
| Hypertension 5 | 391 | (5.4) | 439 | (5.7) | 234 | (7.0) | 0.01 |
| Major cardiovascular disease 6 | 107 | (1.5) | 114 | (1.5) | 79 | (2.4) | 0.0009 |
| Interval between sociodemographic and oral health data collection, years, mean (SD) | 3.7 | (5.4) | 3.7 | (5.5) | 3.7 | (5.2) | 0.96 |
| GOHAI Score | p | ||||||
|---|---|---|---|---|---|---|---|
| 57–60 (n = 7233) | 51–56 (n = 7667) | ≤50 (n = 3363) | |||||
| Total energy, kcal/d | 1905.2 | (494.3) | 1912.0 | (491.5) | 1906.5 | (494.3) | 0.68 |
| % energy from fat | 40.5 | (6.4) | 40.3 | (6.4) | 40.2 | (6.6) | 0.15 |
| % energy from protein | 17.4 | (3.5) | 17.5 | (3.4) | 17.5 | (3.5) | 0.72 |
| % energy from carbohydrates | 42.1 | (7.2) | 42.2 | (7.3) | 42.3 | (7.2) | 0.67 |
| Diet quality (mPNNS-GS) | 7.8 | (1.6) | 7.7 | (1.6) | 7.7 | (1.6) | 0.02 |
| Number of 24-h dietary records | 3.9 | (1.3) | 3.8 | (1.3) | 3.9 | (1.3) | 0.91 |
| 18–64 Years | ≥65 Years | |||||
|---|---|---|---|---|---|---|
| β | 95% CI | p | β | 95% CI | p | |
| Overall GOHAI score | ||||||
| Model 1 | ||||||
| Score ≤ 50 | −0.09 | (−0.17, −0.00) | 0.047 | −0.07 | (−0.16, 0.02) | 0.11 |
| Score 51–56 | −0.03 | (−0.09, 0.04) | 0.432 | −0.26 | (−0.36, −0.16) | <0.0001 |
| Score 57–60 | (reference category) | (reference category) | ||||
| Model 2 | ||||||
| Score ≤ 50 | −0.18 | (−0.26, −0.09) | <0.0001 | −0.08 | (−0.16, 0.01) | 0.08 |
| Score 51–56 | −0.05 | (−0.11, 0.01) | 0.077 | −0.23 | (−0.33, −0.13) | <0.0001 |
| Score 57–60 | (reference category) | (reference category) | ||||
| GOHAI physical function | ||||||
| Model 1 | 0.01 | (−0.01, 0.03) | 0.169 | 0.05 | (0.03, 0.07) | <0.0001 |
| Model 2 | 0.03 | (0.01, 0.04) | 0.005 | 0.04 | (0.02, 0.06) | 0.0002 |
| GOHAI psychosocial function | ||||||
| Model 1 | 0.02 | (0.00, 0.03) | 0.016 | 0.04 | (0.02, 0.05) | <0.0001 |
| Model 2 | 0.03 | (0.02, 0.04) | <0.0001 | 0.04 | (0.02, 0.05) | <0.0001 |
| GOHAI discomfort/pain | ||||||
| Model 1 | −0.00 | (−0.02, 0.02) | 0.718 | 0.03 | (0.00, 0.05) | 0.03 |
| Model 2 | 0.01 | (−0.01, 0.03) | 0.324 | 0.02 | (0.00, 0.04) | 0.06 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreeva, V.A.; Kesse-Guyot, E.; Galan, P.; Feron, G.; Hercberg, S.; Hennequin, M.; Sulmont-Rossé, C. Adherence to National Dietary Guidelines in Association with Oral Health Impact on Quality of Life. Nutrients 2018, 10, 527. https://doi.org/10.3390/nu10050527
Andreeva VA, Kesse-Guyot E, Galan P, Feron G, Hercberg S, Hennequin M, Sulmont-Rossé C. Adherence to National Dietary Guidelines in Association with Oral Health Impact on Quality of Life. Nutrients. 2018; 10(5):527. https://doi.org/10.3390/nu10050527
Chicago/Turabian StyleAndreeva, Valentina A., Emmanuelle Kesse-Guyot, Pilar Galan, Gilles Feron, Serge Hercberg, Martine Hennequin, and Claire Sulmont-Rossé. 2018. "Adherence to National Dietary Guidelines in Association with Oral Health Impact on Quality of Life" Nutrients 10, no. 5: 527. https://doi.org/10.3390/nu10050527
APA StyleAndreeva, V. A., Kesse-Guyot, E., Galan, P., Feron, G., Hercberg, S., Hennequin, M., & Sulmont-Rossé, C. (2018). Adherence to National Dietary Guidelines in Association with Oral Health Impact on Quality of Life. Nutrients, 10(5), 527. https://doi.org/10.3390/nu10050527