New Statistical Approach to Apportion Dietary Sources of Iodine Intake: Findings from Kenya, Senegal and India

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Laboratory Methods
2.2. Kenya
2.3. Senegal
2.4. India
2.5. Data Analyses
3. Results
3.1. Descriptive Findings
3.2. Analytical Findings
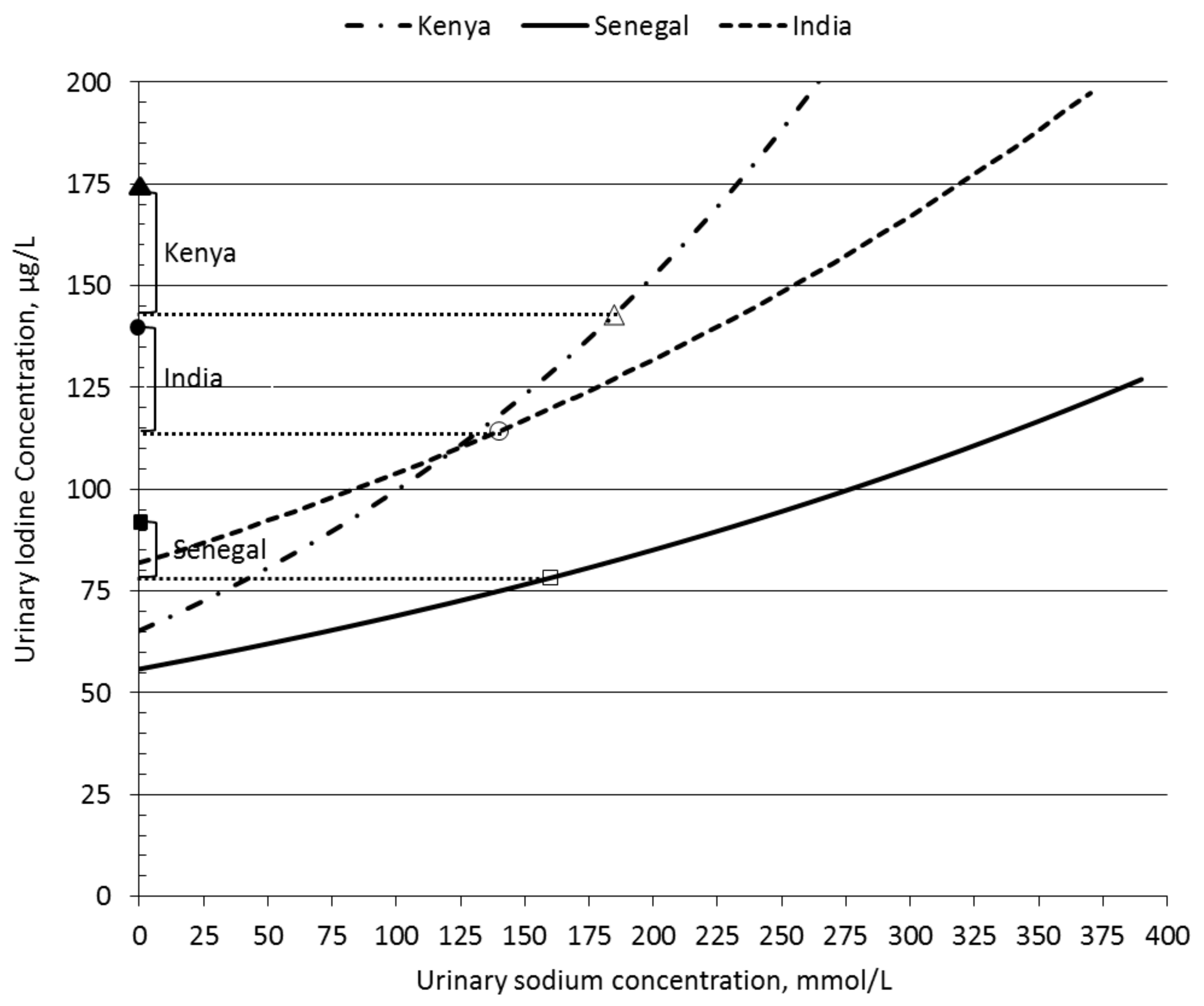
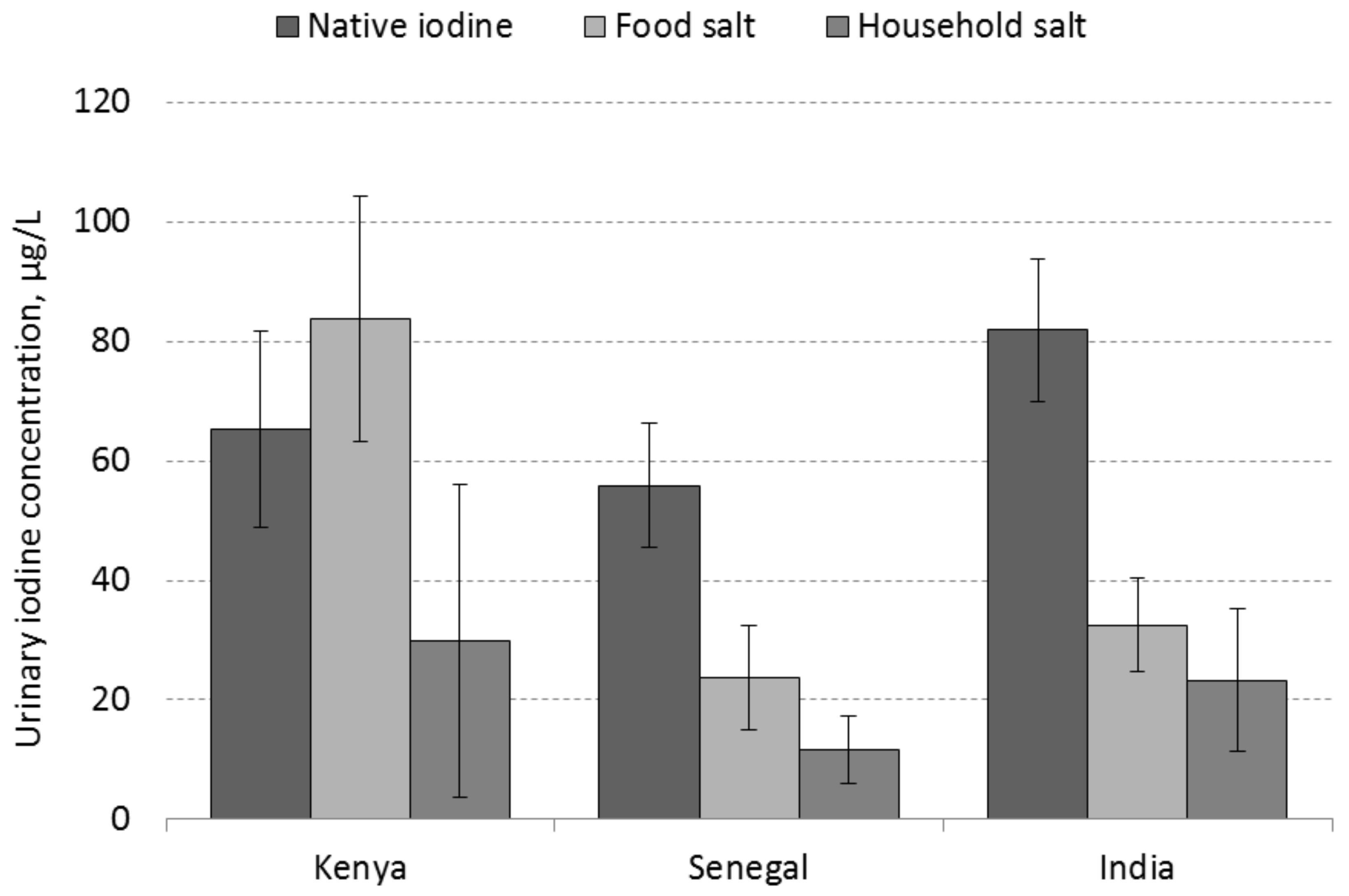
3.3. Estimation of UIC Portions That Correspond to Dietary Sources of Iodine Intake
3.4. Comparison between Countries
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- UNICEF-WHO Joint Committee on Health Policy Special Session. World Summit for Children Mid-Decade Goal: Iodine Deficiency Disorders (IDD); World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- World Health Organization (WHO). Guideline: Fortification of Food-Grade Salt with Iodine for the Prevention and Control of Iodine Deficiency Disorders; World Health Organization: Geneva, Switzerland, 2014; Available online: http://apps.who.int/iris/bitstream/10665/136908/1/9789241507929_eng.pdf (accessed on 20 January 2015).
- Codex Alimentarius Commission. Codex Standard for Food-Grade Salt, CX STAN 150-1985, Rev. 1-1997, Amend. 1-1999, Amend. 2-2001, Amend. 3-2006; Food and Agricultural Organization of the United Nations: Rome, Italy, 2006; Available online: http://www.fao.org/fao-who-codexalimentarius/standards/list-of-standards/en/?provide=standards&orderField=fullReference&sort=asc&num1=CODEX (accessed on 12 July 2010).
- Van der Haar, F. Salt iodization in the modern era and beyond. In Iodine Deficiency Disorders and Their Elimination; Pearce, E., Ed.; Springer International Publishing: Cham, Switzerland, 2017; Chapter 7; pp. 91–104. [Google Scholar]
- Institute of Medicine, Academy of Sciences, USA. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium and Zinc; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- World Health Organization (WHO); United Nations Children’s Fund (UNICEF); Iodine Global Network (ICCIDD). Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers, 3rd ed.; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- United Nations Children’s Fund (UNICEF). State of the World’s Children, Data Tables; United Nations Children’s Fund: New York, NY, USA, 2016; Available online: https://data.unicef.org/topic/nutrition/iodine-deficiency/ (accessed on 31 March 2017).
- Rohner, F.; Zimmermann, M.; Jooste, P.; Pandav, C.; Caldwell, K.; Raghaven, R.; Raiten, D.J. Biomarkers of nutrition for development—Iodine review. J. Nutr. 2014, 144, 1322S–1342S. [Google Scholar] [CrossRef] [PubMed]
- Gorstein, J.; van der Haar, F.; Codling, K.; Houston, R.; Knowles, J.; Timmer, A. Performance of rapid test kits to assess household coverage of iodized salt. Publ. Health Nutr. 2016, 19, 2712–2724. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Karumbunathan, V.; Zimmermann, M.B. Global iodine status in 2011 and trends over the past decade. J. Nutr. 2012, 142, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Ategbo, E.A.; Sankar, R.; Schultink, W.; van der Haar, F.; Pandav, C.S. An assessment of progress toward universal salt iodization in Rajasthan, India, using iodine nutrition indicators in school-aged children and pregnant women from the same households. Asia Pac. J. Clin. Nutr. 2008, 17, 56–62. [Google Scholar] [PubMed]
- Shamim, A.A.; Christian, P.; Schulze, K.; Ali, H.; Kabir, A.; Rashid, M.; Labrique, A.; Salamatullah, Q.; West, K.P. Iodine status in pregnancy and household salt iodine content in rural Bangladesh. Matern. Child Nutr. 2012, 8, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Lv, S.; Mu, Z.; Li, W.; Zhang, X.; Wang, Y.; Rutherford, S. Iodised salt contribution to iodine nutrition status of pregnant and lactating women. Brit. J. Nutr. 2015, 114, 126–133. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stanhewicz, A.E.; Kenney, W.L. Determinants of water and sodium intake and output. Nutr. Rev. 2015, 73, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Manz, F.; Johner, S.A.; Wentz, A.; Boeing, H.; Remer, T. Water balance throughout the adult life span in a German population. Brit. J. Nutr. 2012, 107, 1673–1681. [Google Scholar] [CrossRef] [PubMed]
- Vanacor, R.; Soares, R.; Manica, D.; Furlanetto, T.W. Urinary iodine in 24h is associated with natriuresis and is better reflected by an afternoon sample. Ann. Nutr. Metab. 2008, 53, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Division of Nutrition MoPHS, KEMRI, KNBS, UNICEF Kenya, MI, GAIN, WFP and WHO. Kenya National Micronutrient Survey 2011; Medical Research Institute: Nairobi, Kenya, 2014. [Google Scholar]
- IPDSR Senegal; CLM Senegal; GAIN; UNICEF Dakar. Rapport Final de L’enquête Nationale sur L’utilisation du sel Adéquatement iode et des Bouillons par les Ménages et sur le Statute en iode des Femmes Enceintes et en âge de Procréer Sénégal, 2014. [Final Report of the National Survey of Use of Adequately Iodized Salt and Bouillon in the Households and of the Iodine Status in Pregnant and Reproductive-Age Women. Senegal 2014]; IPDSR: Dakar, Senegal, 2016. [Google Scholar]
- AAIMS; GAIN; UNICEF India; IGN South Asia; Nielsen (India) Pvt. Ltd.; NCSOII, India. National Iodine and Sodium Intake Report India 2015; All-India Institute of Medical Sciences: New Delhi, India, 2015. [Google Scholar]
- Alkire, S.; Roche, J.; Seth, S. Multidimensional Poverty Index 2013. Available online: http://www.ophi.org.uk/multidimensional-poverty-index/mpi-2015/mpi-methodology/ (accessed on 14 November 2016).
- Ministère de la Santé et de la Prévention Médicale, Université Cheikh Anta Diop, Micronutrient Initiative. Etude sur les Troubles dus à la Carance en iode au Sénégal; Ministere de la Sante et de la Prevention Medicale, UCAD and MI: Dakar, Senegal, 2010. [Google Scholar]
- Micronutrient Initiative U.S. Centers for Disease Control and Prevention. Survey Toolkit for Micronutrient Assessment; Micronutrient Initiative: Ottawa, ON, Canada, 2005; Available online: http://surveytoolkit.micronutrient.org/ (accessed on 6 April 2015).
- Pino, S.; Fang, S.L.; Braverman, L.E. Ammonium persulfate: A safe alternative oxidizing reagent for measuring urinary iodine. Clin. Chem. 1996, 42, 239–243. [Google Scholar] [PubMed]
- Ohashi, T.; Yamaki, M.; Pandav, C.S.; Karmarkar, M.G.; Irie, M. Simple microplate method for determination of urinary iodine. Clin. Chem. 2000, 46, 529–536. [Google Scholar] [PubMed]
- Haldimann, M.; Bochud, M.; Burnier, M.; Paccaoud, F.; Dudler, V. Prevalence of iodine inadequacy in Switzerland assessed by the estimated average requirement cut-point method in relation to the impact of iodized salt. Public Health Nutr. 2015, 18, 1333–1342. [Google Scholar] [CrossRef] [PubMed]
- Heeringa, S.G.; West, B.T.; Berglund, P.A. Applied Survey Data Analysis; Taylor & Francis: Boca Raton, FL, USA, 2010. [Google Scholar]
- Whitehead, D.C. The distribution and transformations of iodine in the environment. Environ. Int. 1984, 10, 321–339. [Google Scholar] [CrossRef]
- Johnson, C.C. The Geochemistry of Iodine and Its Application to Environmental Strategies for Reducing the Risks from Iodine Deficiency Disorders (IDD); Commissioned Report CR/03/057N; British Geological Survey: Nottingham, UK, 2003.
- Pennington, J.A.T.; Schoen, S.A.; Salmon, G.D.; Young, B.; Johnson, R.D.; Marts, R.W. Composition of core foods in the U.S. food supply. III. Copper, magnesium, selenium and iodine. J. Food Comp. Anal. 1995, 8, 171–217. [Google Scholar] [CrossRef]
- Fordyce, F.M. Database of the Iodine Content of Food and Diets Populated with Data from Published Literature; Report CR/03/84N; British Geological Survey: Nottingham, UK, 2003.
- Zimmermann, M.B.; Andersson, M. Assessment of iodine nutrition in populations—Past, present and future. Nutr. Rev. 2012, 70, 553–570. [Google Scholar] [CrossRef] [PubMed]
- Ershow, A.G.; Skeaff, S.A.; Merkel, J.M.; Pehrsson, P.R. Development of databases on iodine in foods and dietary supplements. Nutrients 2018, 10, 100. [Google Scholar] [CrossRef] [PubMed]
- Caggiula, A.W.; Wing, R.R.; Nowalk, M.P.; Milas, M.C.; Lee, S.; Langford, H. The measurement of sodium and potassium intake. Am. J. Clin. Nutr. 1985, 42, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Spohrer, R.; Garrett, G.S.; Timmer, A.; Sankar, R.; Kar, B.; Rasool, F.; Locatelli-Rossi, L. Processed foods as an integral part of universal salt iodization programs: A review of global experience and analyses of Bangladesh and Pakistan. Food Nutr. Bull. 2012, 33, S272–S280. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Hussein, I.; Al Ghannami, S.; El Badawi, S.; Al Hamad, N.M.; Hajj, B.A.; Al-Thani, M.; Al-Thani, A.A.; Winichagoon, P.; Pongcharoen, T.; et al. Estimation of the prevalence of deficient and excessive iodine intakes in school-age children from the adjusted distribution of urinary iodine concentrations from population surveys. J. Nutr. 2016, 146, 1204–1211. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, M.E.; Maalouf, J.; Elliott, P.; Loria, C.M.; Patel, S.; Bowman, B.A. Use of urine biomarkers to assess sodium intake: Challenges and opportunities. Ann. Rev. Nutr. 2015, 35, 349–387. [Google Scholar] [CrossRef] [PubMed]
- Conkle, J.; van der Haar, F. The use and interpretation of sodium concentrations in casual (spot) urine collections for population surveillance and partitioning of dietary intake sources. Nutrients 2017, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.R.; Correa-Rotter, R.; Cappuccio, F.P.; Webster, J.; Lackland, D.T.; Neal, B.; MacGregor, G.A. Proposed nomenclature for salt intake and for reductions in dietary salt. J. Clin. Hypertens. (Greenwich) 2015, 17, 247–251. [Google Scholar] [CrossRef] [PubMed]
- United Nations Children’s Fund (UNICEF). Sustainable Elimination of Iodine Deficiency; UNICEF: New York, NY, USA, 2008. [Google Scholar]
- Van der Haar, F.; Gerasimov, G.; Tyler, V.Q.; Timmer, A. Universal salt iodization in the Central and Eastern Europe, Commonwealth of Independent States (CEE/CIS) region during the decade 2000-09: Experiences, achievements and lessons learned. Food Nutr. Bull. 2011, 20, S175–S294. [Google Scholar] [CrossRef] [PubMed]
- Bland, M. Regression and Correlation. In An Introduction to Medical Statistics, 4th ed.; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Rothman, K.J. Using Regression Models in Epidemiologic Analysis. In Epidemiology, an Introduction, 2nd ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Snedecor, G.W.; Cochran, W.G. Regression. In Statistical Methods, 6th ed.; Iowa State University Press: Ames, IA, USA, 1967. [Google Scholar]
- Liu, K. Measurement error and its impact on partial correlation and multiple linear regression analyses. Am. J. Epidemiol. 1988, 127, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Hutcheon, J.A.; Chiolero, A.; Hanley, J.A. Random measurement error and regression dilution bias. BMJ 2010, 340, c2289. [Google Scholar] [CrossRef] [PubMed]
- Spohrer, R.; Knowles, J.; Jallier, V.; Ndiaye, B.; Indorf, C.; Guinot, P.; Kupka, R. Estimation of population iodine intake from iodized salt consumed through boullion seasoning in Senegal. Ann. N. Y. Acad. Sci. 2015, 1357, 8–28. [Google Scholar] [CrossRef] [PubMed]
- Bukania, Z. Kenya USI Gap Assessment Report; Micronutrient Initiative: Nairobi, Kenya, 2017. [Google Scholar]
- Knowles, J.; Garrett, G.S.; Gorstein, J.; Kupka, R.; Situma, R.; Yadav, K.; Yusufali, R.; Pandav, C.; Aaron, G.J. Universal Salt Iodization Coverage Survey Team. Household coverage with adequately iodized salt varies greatly between countries and by residence type and socioeconomic status within countries: Results from 10 national coverage surveys. J. Nutr. 2017, 147, 1004S–1014S. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.G.; Kaye, A.E.; Druce, E. Sources and intakes of sodium in the United Kingdom diet. Eur. J. Clin. Nutr. 1989, 43, 855–861. [Google Scholar] [PubMed]
- Harnack, L.J.; Cogswell, M.E.; Shikany, J.M.; Gardner, C.D.; Gillespie, C.; Loria, C.M.; Zhou, X.; Yuan, K.; Steffen, L.M. Sources of sodium in US adults from 3 geographic regions. Circulation 2017, 135, 1775–1783. [Google Scholar] [CrossRef] [PubMed]
- McLean, R. Measuring population sodium intake: A review of methods. Nutrients 2014, 6, 4651–4662. [Google Scholar] [CrossRef] [PubMed]
- Mente, A.; O’Donnell, M.J.; Yusuf, S. Measuring sodium intake in populations: Simple is best? Am. J. Hypertens. 2015, 28, 1303–1305. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hawkes, C.; Webster, J. National approaches to monitoring population salt intake: A trade-off between accuracy and practicality? PLoS ONE 2012, 10, e46727. [Google Scholar] [CrossRef] [PubMed]
- Dyer, A.; Elliott, P.; Chee, D.; Stamler, J. Urinary biochemical markers of dietary intake in the INTERSALT study. Am. J. Clin. Nutr. 1997, 65, 1246S–1253S. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.; Praveen, D.; Pope, A.; Raj, T.S.; Pillai, R.N.; Land, M.A.; Neal, B. Mean population salt consumption in India: A systematic review. J. Hypertens. 2017, 35, 3–9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| UIC (µg/L) | UnaC (mmol/L) | SI (mg/kg) | ||||
|---|---|---|---|---|---|---|
| Median | IQR | Mean | SD | Mean | SD | |
| Kenya (n = 382) | ||||||
| Urban | 187 | 203 | 204 | 91 | 38.0 | 18.4 |
| Rural | 164 | 161 | 177 | 102 | 32.3 | 17.9 |
| All WRA Kenya | 172 | 199 | 185 | 97 | 34.4 | 18.3 |
| Senegal (n = 1110) | ||||||
| Urban | 116 | 132 | 168 | 76 | 18.1 | 13.0 |
| Rural, salt producing | 106 | 118 | 172 | 72 | 8.8 | 16.3 |
| Rural, non-salt producing | 76 | 104 | 165 | 85 | 10.4 | 10.6 |
| All WRA Senegal | 101 | 124 | 167 | 80 | 14.9 | 13.0 |
| India (n = 2373) | ||||||
| Urban | 168 | 187 | 138 | 67 | 27.7 | 17.1 |
| Rural | 149 | 183 | 143 | 70 | 23.3 | 15.1 |
| All WRA India | 159 | 183 | 140 | 69 | 25.7 | 16.9 |
| Estimate 2 | 95% CI | t-Statistic | p Value | |
|---|---|---|---|---|
| Kenya | ||||
| Intercept | 4.112 | 3.477, 4.747 | 26.4 | 0.000 |
| UNaC | 0.0042 | 0.0034, 0.0050 | 10.5 | 0.000 |
| SI | 0.0056 | 0.0002, 0.0109 | 2.03 | 0.044 |
| Rural areas 3 | 0.0436 | −0.0171, 0.2585 | 0.40 | 0.690 |
| Senegal | ||||
| Intercept | 4.026 | 3.786, 4.267 | 33.2 | 0.000 |
| UNaC | 0.0021 | 0.0012, 0.0030 | 4.6 | 0.000 |
| SI | 0.0112 | 0.0053, 0.0170 | 3.8 | 0.000 |
| Rural 3—salt processing | 0.0655 | −0.1395, 0.2705 | 0.63 | 0.528 |
| Rural 3—non salt processing | −0.0736 | −0.3009, 0.1537 | −0.64 | 0.522 |
| MPI—Education | 0.0060 | −0.2110, 0.2227 | 0.05 | 0.956 |
| MPI—Health | −0.2699 | −0.6605, 0.1207 | −1.37 | 0.174 |
| MPI—Living standards | −0.2018 | −0.6345, 0.2328 | −0.92 | 0.359 |
| Bouillon consumption | 0.0092 | −0.0082, 0.0140 | 0.52 | 0.602 |
| India | ||||
| Intercept | 4.432 | 4.276, 4.588 | 55.8 | 0.000 |
| UNaC | 0.0024 | 0.0018, 0.0030 | 7.6 | 0.000 |
| SI | 0.0073 | 0.0032, 0.0114 | 3.5 | 0.001 |
| Rural areas 3 | −0.0532 | −0.1531, 0.0467 | −1.05 | 0.296 |
| MPI—Education | 0.0055 | −0.1617, 0.1726 | 0.06 | 0.949 |
| MPI—Health | 0.0544 | −0.1430, 0.2518 | 0.54 | 0.588 |
| MPI—Living standards | −0.5141 | −0.7477, −0.2806 | −4.3 | 0.000 |
| Kenya (n = 382) | Senegal (n = 1110) | India (n = 2373) | ||||
|---|---|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | |
| Native iodine | 65 | 49, 82 | 56 | 46, 66 | 82 | 70, 94 |
| Food salt | 84 | 63, 104 | 24 | 15, 33 | 33 | 25, 40 |
| Household salt | 30 | 4, 56 | 12 | 6, 17 | 23 | 11, 35 |
| Total UIC | 179 | 160, 197 | 91 | 85, 98 | 138 | 131, 144 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van der Haar, F.; Knowles, J.; Bukania, Z.; Camara, B.; Pandav, C.S.; Mwai, J.M.; Toure, N.K.; Yadav, K. New Statistical Approach to Apportion Dietary Sources of Iodine Intake: Findings from Kenya, Senegal and India. Nutrients 2018, 10, 430. https://doi.org/10.3390/nu10040430
Van der Haar F, Knowles J, Bukania Z, Camara B, Pandav CS, Mwai JM, Toure NK, Yadav K. New Statistical Approach to Apportion Dietary Sources of Iodine Intake: Findings from Kenya, Senegal and India. Nutrients. 2018; 10(4):430. https://doi.org/10.3390/nu10040430
Chicago/Turabian StyleVan der Haar, Frits, Jacky Knowles, Zipporah Bukania, Boubacar Camara, Chandrakant S. Pandav, John Maina Mwai, Ndeye Khady Toure, and Kapil Yadav. 2018. "New Statistical Approach to Apportion Dietary Sources of Iodine Intake: Findings from Kenya, Senegal and India" Nutrients 10, no. 4: 430. https://doi.org/10.3390/nu10040430
APA StyleVan der Haar, F., Knowles, J., Bukania, Z., Camara, B., Pandav, C. S., Mwai, J. M., Toure, N. K., & Yadav, K. (2018). New Statistical Approach to Apportion Dietary Sources of Iodine Intake: Findings from Kenya, Senegal and India. Nutrients, 10(4), 430. https://doi.org/10.3390/nu10040430