
Assessing Regional Public Service Facility Accessibility Using Multisource Geospatial Data: A Case Study of Underdeveloped Areas in China



Abstract
1. Introduction
2. Materials and Methods
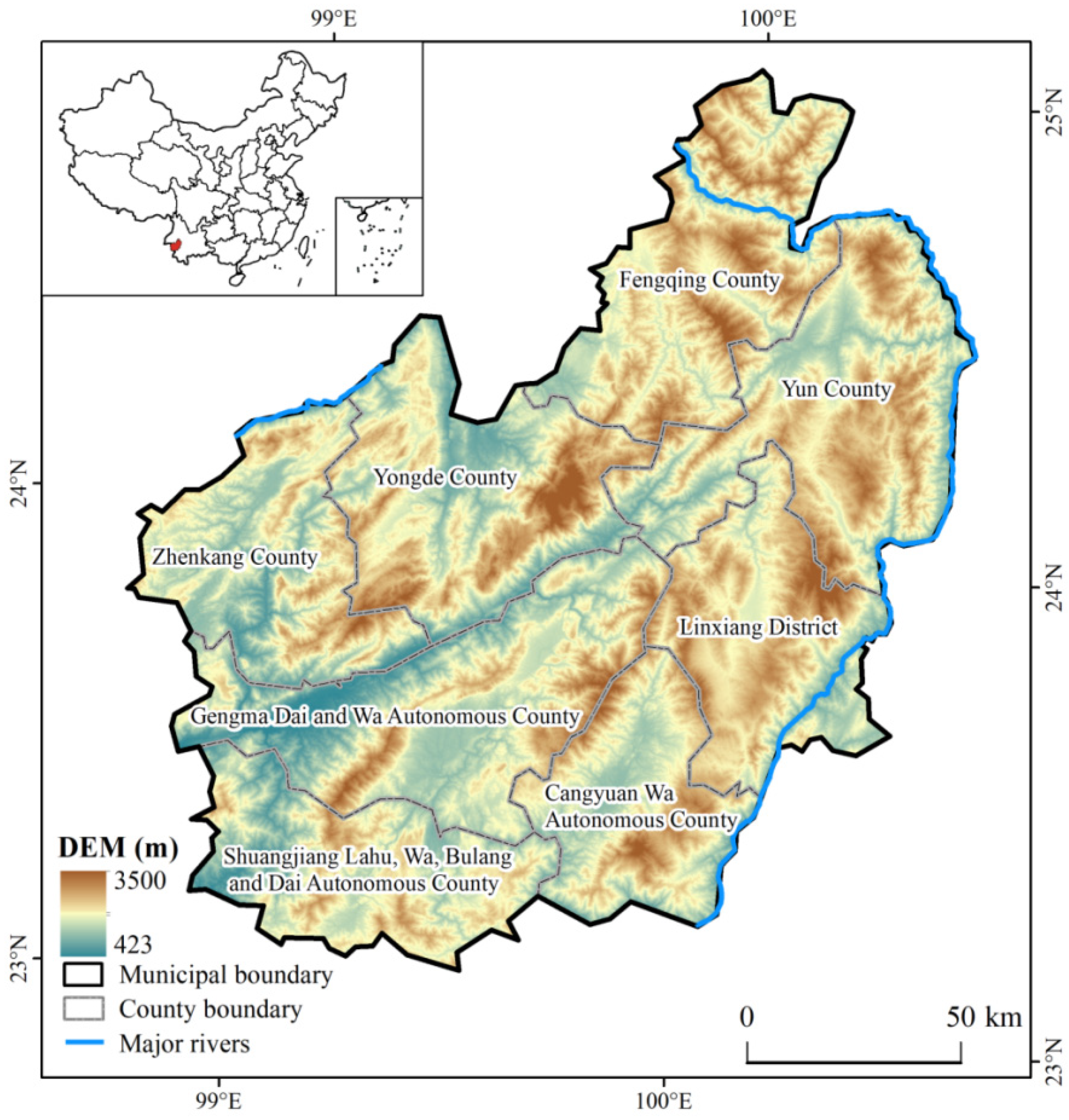
2.1. Study Area
2.2. Data Sources
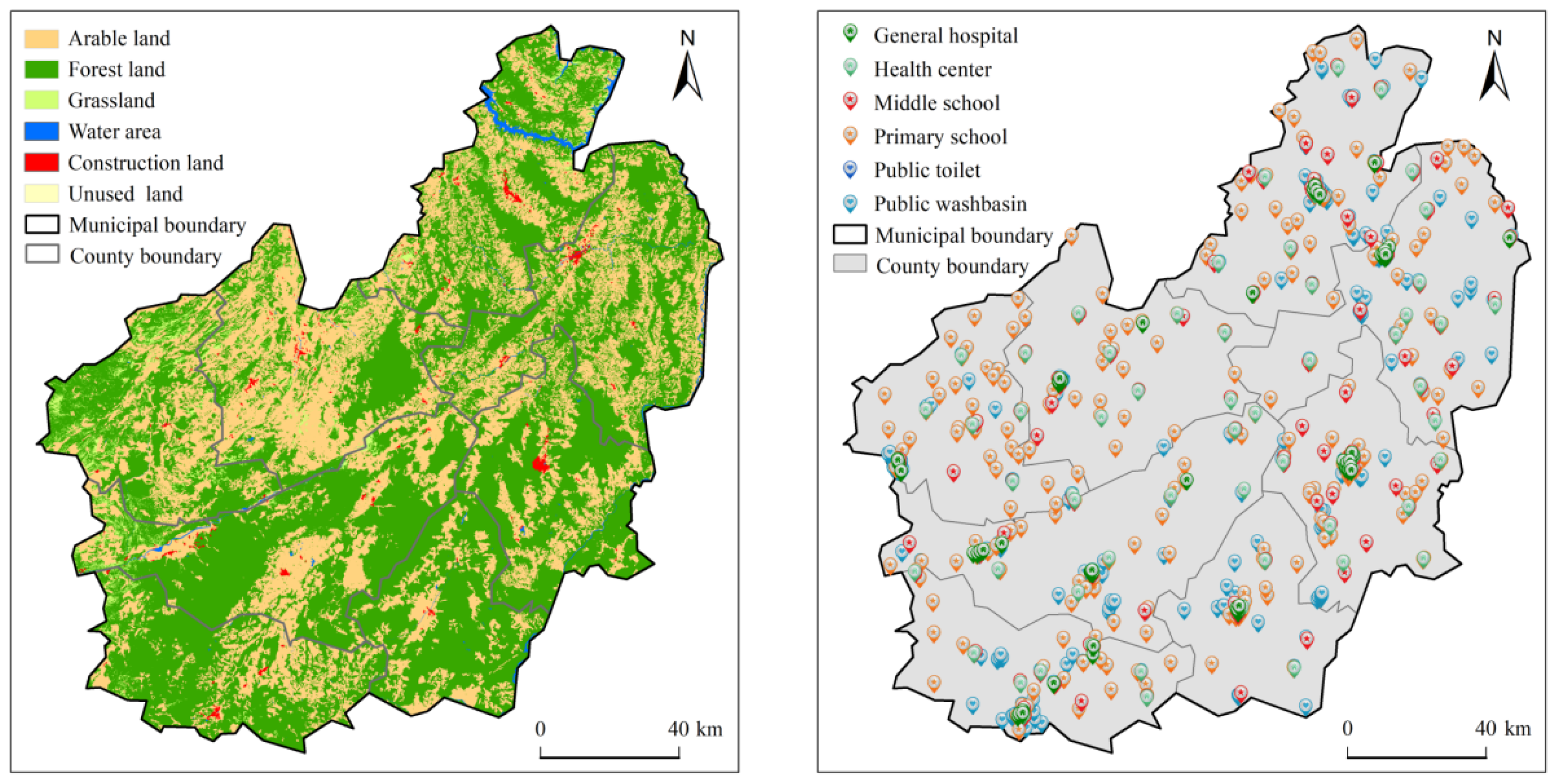
2.2.1. Landuse Data
2.2.2. Elevation Data
2.2.3. Points of Interest (POI) Data
2.2.4. Socioeconomic Statistics
2.2.5. Road and River Network Data
2.3. Method
2.3.1. Public Service Facility Accessibility Assessment
- (1)
- Generate the passing speed raster layer. Railway, river, and road data were extracted from the OSM dataset and the road network dataset provided by the Lincang Transportation Bureau. The corresponding speeds were assigned in the attribute table. Then, they were converted into a raster with a spatial resolution of 30 m. The pixel values were the corresponding traffic speeds of each type of railway, river, and road. For areas not covered by roads and rivers, we extracted land-cover and land-use type data from the Globeland30 dataset and assigned the corresponding traffic speed (walking) to the pixels of each type. Table A1 shows the specific settings of traffic speed for different types of pixels. In the case of multiple underlying surface types in a pixel, the type with the highest speed was preferentially selected to generate the final passing speed raster data.
- (2)
- Calculate the cost raster. The pixel size was divided by the highest passing speed of the 30 m spatial resolution passing speed raster data obtained above to calculate the minimum passing time of each pixel and obtain the cost raster.
- (3)
- Calculate the path distance. We used path distance analysis [51] to calculate the minimum cumulative cost distance (shortest travel time) between each pixel and its nearest public facility combined with the cost raster and elevation as the surface raster, taking into account the surface distance as well as horizontal and vertical cost factors to modify the cost.
- (4)
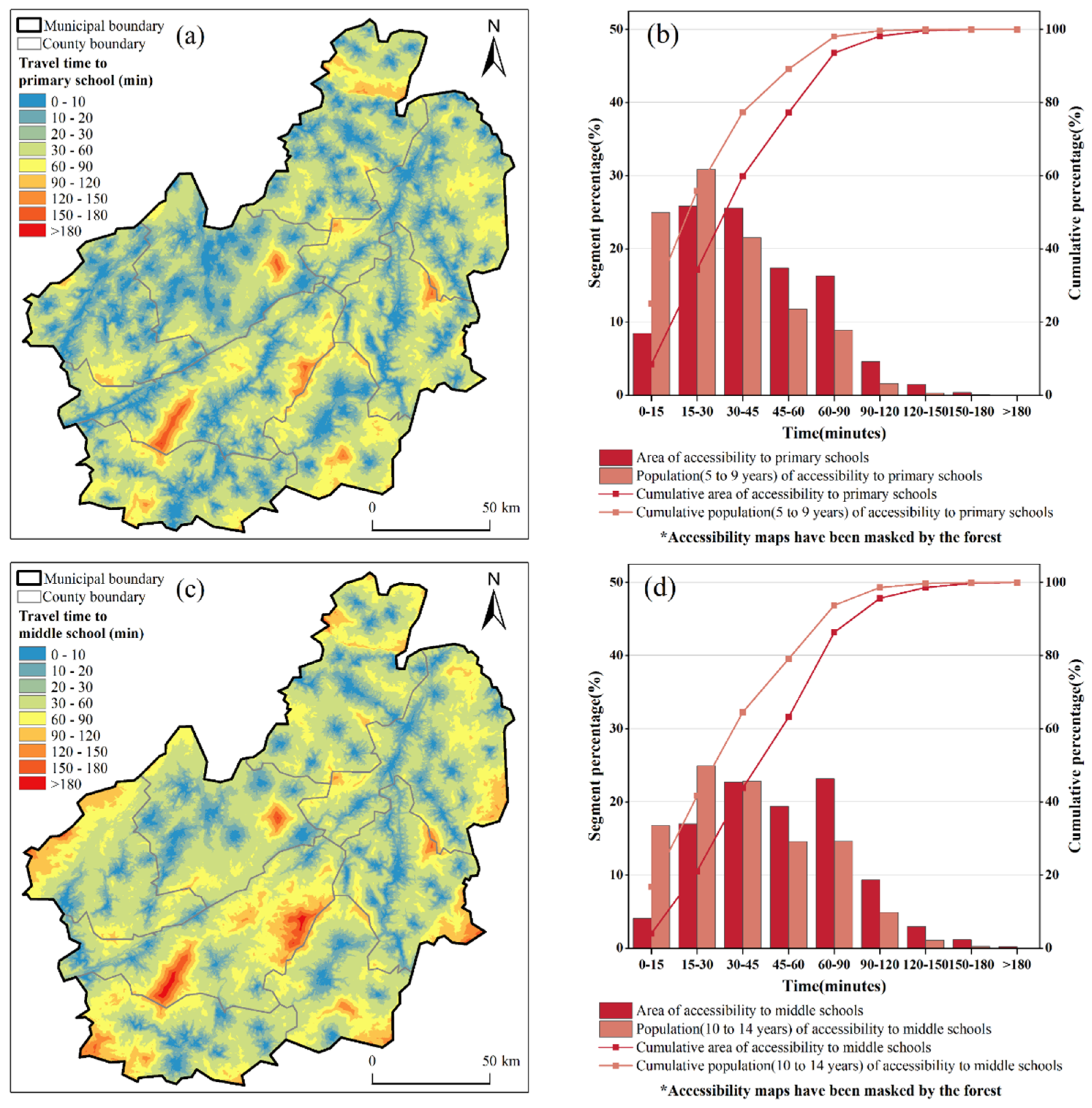
- Map the spatial layout of public facility accessibility. Finally, we completed the accessibility evaluation of three types of infrastructure (healthcare, education, and sanitation) and drew the accessibility map.
- (1)
- Prepare the surface raster. Path distance analysis is generally used to calculate the least-cost path between a source and a destination, while accounting for the surface distance and the horizontal and vertical factors [51]. As Lincang is mostly mountainous, the effect of terrain fluctuations on traffic speed needs to be considered. Therefore, we extracted 30 m spatial resolution elevation data from the ASTER GDEM V3 dataset as the surface raster for traffic speed adjustments.
- (2)
- Generate vector point data of public facilities. Based on the latitude and longitude coordinates of public facilities provided in the POI data, vector point data were generated for Lincang General Hospital, the Health Center, primary and secondary schools, public toilets, and public washbasins.
- (3)
- Calculate the minimum cumulative cost distance. The traveling cost between two adjacent nodes depends on the spatial direction of the two nodes and the way the image elements are connected. The three cases included are the adjacent node cost, cumulative perpendicular cost, and diagonal node cost, the specific principles of which are detailed in [51].
2.3.2. Classification of the Inhabitants’ Socioeconomic Attributes
2.3.3. Cluster Identification of Poverty Groups
3. Results
3.1. Spatial Patterns of Accessibility to Public Service Facilities
3.1.1. Accessibility to Healthcare Facilities
3.1.2. Accessibility to Educational Facilities
3.1.3. Accessibility to Sanitation Facilities
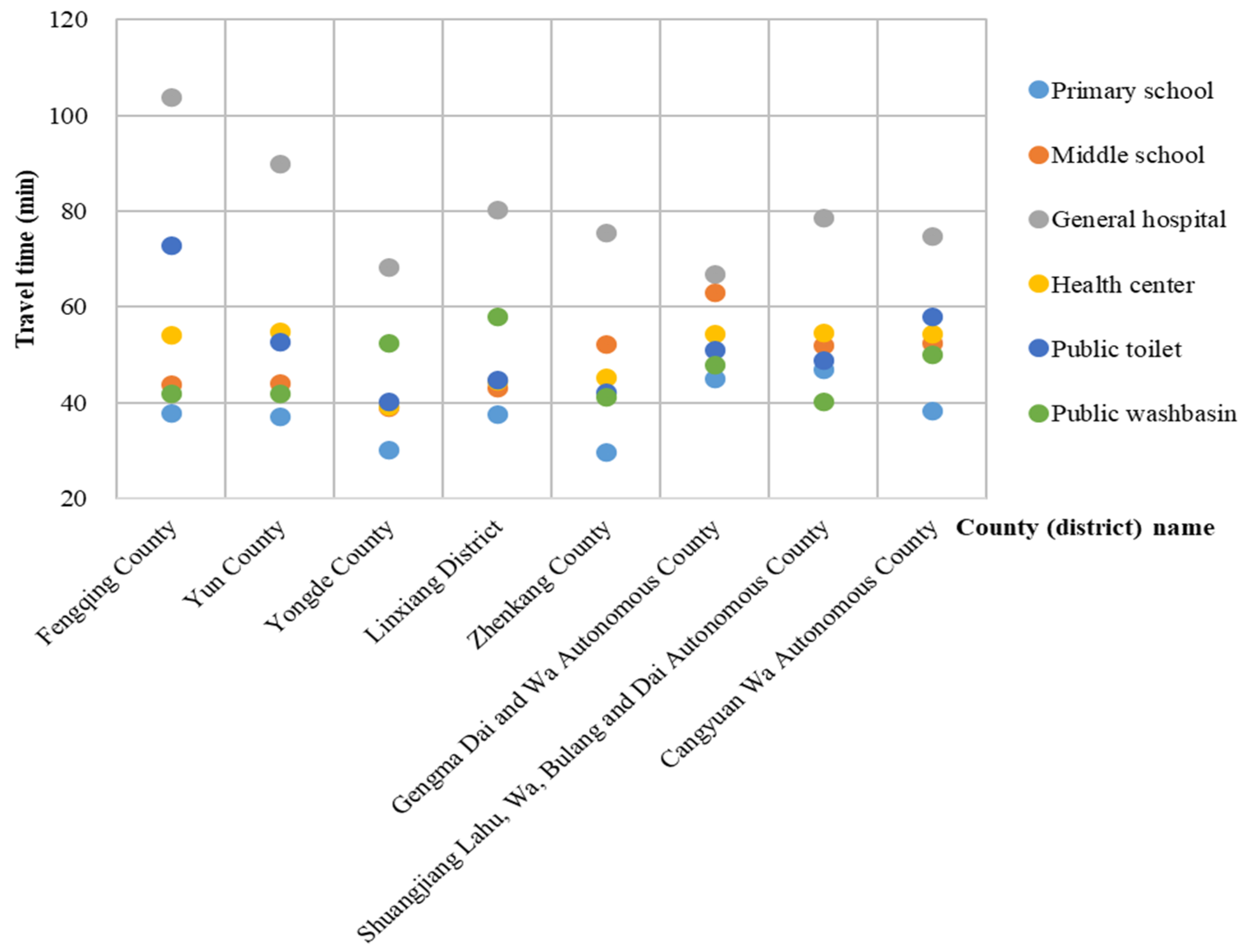
3.1.4. Comparison of Public Facility Accessibility in Lincang’s Counties and Districts
3.2. Public Facility Accessibility Analysis Based on Different Inhabitant Attributes
3.2.1. Correlation Analysis of Inhabitant Attributes and Minimum Cost Distance
3.2.2. Average Analysis of the Accessibility to Public Facilities in Different Inhabitant Clusters
3.3. Public Facility Accessibility Analysis Based on Attributes of Poor Groups
3.3.1. Correlation Analysis of Different Types of Poverty Groups and Least-Cost Distance
3.3.2. Analysis of Average Accessibility to Public Facilities among Different Poor Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Type | Speed (km/h) |
|---|---|---|
| Open Street Map | Railway | 90 |
| River | 1 | |
| Transportation bureau road network data | National highway | 80 |
| Provincial highway | 60 | |
| County highway | 40 | |
| Township road | 30 | |
| Village road | 30 | |
| Substandard highway | 20 | |
| Accommodation road | 30 | |
| Globeland 30 | Arable land | 2.87 |
| Forest land | 3.068 | |
| Grassland | 4.86 | |
| Shrubland | 3.6 | |
| Wetland | 2 | |
| Water area | 1 | |
| Artificial surface | 5 | |
| Bare area | 3 | |
| ASTER GDEM V3 | Elevation | Surface raster |
| Variable | Dimension | |||
|---|---|---|---|---|
| Family Background | Ethnicity and Self-Development | Geographical Environment | Health and Labor Force | |
| Ethnicity | 0.0068 | 0.8749 | 0.0037 | 0.0016 |
| Age | 0.0206 | 0.7504 | 0.0025 | 0.0074 |
| Education level | 0.0837 | 0.4656 | 0.0214 | 0.1258 |
| Health status | 0.5007 | 0.0049 | 0.0421 | 0.8125 |
| Labor ability | 0.4892 | 0.1684 | 0.0230 | 0.7762 |
| Total family population | 0.7858 | 0.0253 | 0.0047 | 0.0051 |
| Working population in the family | 0.8236 | 0.0027 | 0.0039 | 0.7664 |
| Migrant workers in the family | 0.7859 | 0.0043 | 0.0026 | 0.6355 |
| Distance to the nearest city | 0.0037 | 0.0014 | 0.8572 | 0.0097 |
| Distance to the nearest station | 0.0098 | 0.0036 | 0.8901 | 0.0196 |
| Distance to the nearest public facility | 0.0188 | 0.0025 | 0.8012 | 0.0054 |
References
- Jin, M.; Liu, L.; Tong, D.; Gong, Y.; Liu, Y. Evaluating the Spatial Accessibility and Distribution Balance of Multi-Level Medical Service Facilities. Int. J. Environ. Res. Public Health 2019, 16, 1150. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Sun, L.; Shao, Z.; Zhou, X. Accessibility Evaluation of Public Service Facilities in Villages and Towns Based on POI Data: A Case Study of Suining County, Xuzhou, China. J. Urban Plan. Dev 2023, 149, 05023019. [Google Scholar] [CrossRef]
- Levine, J. A Century of Evolution of the Accessibility Concept. Transp. Res. Part D Transp. Environ. 2020, 83, 102309. [Google Scholar] [CrossRef]
- Park, J.; Goldberg, D.W. A Review of Recent Spatial Accessibility Studies That Benefitted from Advanced Geospatial Information: Multimodal Transportation and Spatiotemporal Disaggregation. ISPRS Int. J. Geo-Inf. 2021, 10, 532. [Google Scholar] [CrossRef]
- Hansen, W.G. How Accessibility Shapes Land Use. J. Am. Inst. Plan. 1959, 25, 73–76. [Google Scholar] [CrossRef]
- Wachs, M.; Kumagai, T.G. Physical Accessibility as a Social Indicator. Socio-Econ. Plan. Sci. 1973, 7, 437–456. [Google Scholar] [CrossRef]
- Dalvi, M.Q.; Martin, K.M. The Measurement of Accessibility: Some Preliminary Results. Transportation 1976, 5, 17–42. [Google Scholar] [CrossRef]
- Nelson, A. Travel Time to Major Cities: A Global Map of Accessibility; European Communities: Ispra, Italy, 2008. [Google Scholar]
- Hsiao, S.; Lu, J.; Sterling, J.; Weatherford, M. Use of Geographic Information System for Analysis of Transit Pedestrian Access. Transp. Res. Rec. 1997, 1604, 50–59. [Google Scholar] [CrossRef]
- Kalogirou, S.; Foley, R. Health, Place and Hanly: Modelling Accessibility to Hospitals in Ireland. Ir. Geogr. 2006, 39, 52–68. [Google Scholar] [CrossRef]
- Litman, T. Evaluating Transportation Equity. World Transp. Policy Pract. 2002, 8, 50–65. [Google Scholar]
- Zenk, S.N.; Schulz, A.J.; Israel, B.A.; James, S.A.; Bao, S.; Wilson, M.L. Neighborhood Racial Composition, Neighborhood Poverty, and the Spatial Accessibility of Supermarkets in Metropolitan Detroit. Am. J. Public Health 2005, 95, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Liu, S.; Qi, W. Spatial Differentiation and Influencing Mechanism of Medical Care Accessibility in Beijing: A Migrant Equality Perspective. Chin. Geogr. Sci. 2018, 28, 353–362. [Google Scholar] [CrossRef]
- Guo, Y.; Chang, S.-S.; Chen, M.; Yip, P.S.F. Do Poorer Areas Have Poorer Access to Services in Hong Kong? A Small-Area Analysis Based on Multiple Spatial Accessibility Indicators. Soc. Indic. Res. 2018, 138, 1–21. [Google Scholar] [CrossRef]
- Akhavan, A.; Phillips, N.E.; Du, J.; Chen, J.; Sadeghinasr, B.; Wang, Q. Accessibility Inequality in Houston. IEEE Sens. Lett. 2019, 3, 7102104. [Google Scholar] [CrossRef]
- Chen, Y.; Bouferguene, A.; Shen, Y.; Al-Hussein, M. Assessing Accessibility-Based Service Effectiveness (ABSEV) and Social Equity for Urban Bus Transit: A Sustainability Perspective. Sustain. Cities Soc. 2019, 44, 499–510. [Google Scholar] [CrossRef]
- Wang, H.; Kwan, M.-P.; Hu, M. Social Exclusion and Accessibility among Low- and Non-Low-Income Groups: A Case Study of Nanjing, China. Cities 2020, 101, 102684. [Google Scholar] [CrossRef]
- Estoque, R.C. A Review of the Sustainability Concept and the State of SDG Monitoring Using Remote Sensing. Remote Sens. 2020, 12, 1770. [Google Scholar] [CrossRef]
- Lawal, O.; Anyiam, F.E. Modelling Geographic Accessibility to Primary Health Care Facilities: Combining Open Data and Geospatial Analysis. Geo-Spat. Inf. Sci. 2019, 22, 174–184. [Google Scholar] [CrossRef]
- Evans, D.B.; Hsu, J.; Boerma, T. Universal Health Coverage and Universal Access. Bull. World Health Organ. 2013, 91, 546A. [Google Scholar] [CrossRef]
- Ashiagbor, G.; Ofori-Asenso, R.; Forkuo, E.K.; Agyei-Frimpong, S. Measures of Geographic Accessibility to Health Care in the Ashanti Region of Ghana. Sci. Afr. 2020, 9, e00453. [Google Scholar] [CrossRef]
- Salvacion, A.R. Measuring Spatial Accessibility of Healthcare Facilities in Marinduque, Philippines. ISPRS Int. J. Geo-Inf. 2022, 11, 516. [Google Scholar] [CrossRef]
- Alegana, V.A.; Wright, J.A.; Pentrina, U.; Noor, A.M.; Snow, R.W.; Atkinson, P.M. Spatial Modelling of Healthcare Utilisation for Treatment of Fever in Namibia. Int. J. Health Geogr. 2012, 11, 6. [Google Scholar] [CrossRef]
- Weiss, D.J.; Nelson, A.; Gibson, H.S.; Temperley, W.; Peedell, S.; Lieber, A.; Hancher, M.; Poyart, E.; Belchior, S.; Fullman, N.; et al. A Global Map of Travel Time to Cities to Assess Inequalities in Accessibility in 2015. Nature 2018, 553, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.J.; Nelson, A.; Vargas-Ruiz, C.A.; Gligorić, K.; Bavadekar, S.; Gabrilovich, E.; Bertozzi-Villa, A.; Rozier, J.; Gibson, H.S.; Shekel, T.; et al. Global Maps of Travel Time to Healthcare Facilities. Nat. Med. 2020, 26, 1835–1838. [Google Scholar] [CrossRef] [PubMed]
- Pizzol, B.; Giannotti, M.; Tomasiello, D.B. Qualifying Accessibility to Education to Investigate Spatial Equity. J. Transp. Geogr. 2021, 96, 103199. [Google Scholar] [CrossRef]
- Moreno-Monroy, A.I.; Lovelace, R.; Ramos, F.R. Public Transport and School Location Impacts on Educational Inequalities: Insights from São Paulo. J. Transp. Geogr. 2018, 67, 110–118. [Google Scholar] [CrossRef]
- Gao, Y.; He, Q.; Liu, Y.; Zhang, L.; Wang, H.; Cai, E. Imbalance in Spatial Accessibility to Primary and Secondary Schools in China: Guidance for Education Sustainability. Sustainability 2016, 8, 1236. [Google Scholar] [CrossRef]
- United Nations. Report of the Independent Expert on the Issue of Human Rights Obligations Related to Access to Safe Drinking Water and Sanitation, Catarina de Albuquerque: Addendum. 2010. Available online: https://digitallibrary.un.org/record/685823 (accessed on 16 April 2023).
- Kumar, S.; Vollmer, S. Does Access to Improved Sanitation Reduce Childhood Diarrhea in Rural India? Health Econ. 2013, 22, 410–427. [Google Scholar] [CrossRef]
- Verma, A.; Megiddo, I.; Nandi, A.; Laxminarayan, R.; Ashok, A. Reduced Burden of Childhood Diarrheal Diseases through Increased Access to Water and Sanitation in India: A Modeling Analysis. Soc. Sci. Med. 2017, 180, 181–192. [Google Scholar] [CrossRef]
- Gentry-Shields, J.; Bartram, J. Human Health and the Water Environment: Using the DPSEEA Framework to Identify the Driving Forces of Disease. Sci. Total Environ. 2014, 468–469, 306–314. [Google Scholar] [CrossRef]
- Cheng, S.; Li, Z.; Uddin, S.M.N.; Mang, H.-P.; Zhou, X.; Zhang, J.; Zheng, L.; Zhang, L. Toilet Revolution in China. J. Environ. Manag. 2018, 216, 347–356. [Google Scholar] [CrossRef]
- Korah, P.I.; Nunbogu, A.M.; Ahmed, A. Measuring Access to Health Facilities in Ghana: Implications for Implementation of Health Interventions and the Sustainable Development Goal 3. Appl. Geogr. 2023, 158, 103026. [Google Scholar] [CrossRef]
- Sahitya, K.S.; Prasad, C.S.R.K. Evaluation of Opportunity Based Urban Road Network Accessibility Using GIS. Spat. Inf. Res. 2020, 28, 487–493. [Google Scholar] [CrossRef]
- Benenson, I.; Ben-Elia, E.; Rofe, Y.; Geyzersky, D. The Benefits of a High-Resolution Analysis of Transit Accessibility. Int. J. Geogr. Inf. Sci. 2017, 31, 213–236. [Google Scholar] [CrossRef]
- Delamater, P.L.; Messina, J.P.; Shortridge, A.M.; Grady, S.C. Measuring Geographic Access to Health Care: Raster and Network-Based Methods. Int. J. Health Geogr. 2012, 11, 15. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Zheng, J.; Pei, X. Measurement Method and Influencing Mechanism of Urban Subdistrict Vitality in Shanghai Based on Multisource Data. Remote Sens. 2023, 15, 932. [Google Scholar] [CrossRef]
- Rogers, G.; Koper, P.; Ruktanonchai, C.; Ruktanonchai, N.; Utazi, E.; Woods, D.; Cunningham, A.; Tatem, A.J.; Steele, J.; Lai, S.; et al. Exploring the Relationship between Temporal Fluctuations in Satellite Nightlight Imagery and Human Mobility across Africa. Remote Sens. 2023, 15, 4252. [Google Scholar] [CrossRef]
- Forget, Y.; Shimoni, M.; Gilbert, M.; Linard, C. Mapping 20 Years of Urban Expansion in 45 Urban Areas of Sub-Saharan Africa. Remote Sens. 2021, 13, 525. [Google Scholar] [CrossRef]
- You, D.; Wang, S.; Wang, F.; Zhou, Y.; Wang, Z.; Wang, Y.; Wang, J.; Xiong, Y.; Ji, J. Monitoring and Analyzing the Effectiveness of the Effective Refuge Area of Emergency Shelters by Using Remote Sensing: A Case Study of Beijing’s Fifth Ring Road. Remote Sens. 2023, 15, 3646. [Google Scholar] [CrossRef]
- Wang, K.; Zhang, L.; Cai, M.; Liu, L.; Wu, H.; Peng, Z. Measuring Urban Poverty Spatial by Remote Sensing and Social Sensing Data: A Fine-Scale Empirical Study from Zhengzhou. Remote Sens. 2023, 15, 381. [Google Scholar] [CrossRef]
- Cui, H.; Wu, L.; Hu, S.; Lu, R. Measuring the Service Capacity of Public Facilities Based on a Dynamic Voronoi Diagram. Remote Sens. 2021, 13, 1027. [Google Scholar] [CrossRef]
- Guo, Y.; Zhou, Y.; Cao, Z. Comprehensive Measurement of County Poverty in China and Targeting Poverty Reduction after 2020. J. Geogr. Sci. 2018, 28, 1810–1824. [Google Scholar]
- Guo, Y.; Zhou, Y.; Liu, Y. Targeted Poverty Alleviation and Its Practices in Rural China: A Case Study of Fuping County, Hebei Province. J. Rural Stud. 2022, 93, 430–440. [Google Scholar] [CrossRef]
- Bruun, H.H.; Nelson, A.; Chomitz, K.M. Effectiveness of Strict vs. Multiple Use Protected Areas in Reducing Tropical Forest Fires: A Global Analysis Using Matching Methods. PLoS ONE 2011, 6, e22722. [Google Scholar] [CrossRef]
- Schmitz, C.; Biewald, A.; Lotze-Campen, H.; Popp, A.; Dietrich, J.P.; Bodirsky, B.; Krause, M.; Weindl, I. Trading more food: Implications for land use, greenhouse gas emissions, and the food system. Glob. Environ. Chang. 2012, 22, 189–209. [Google Scholar] [CrossRef]
- Gilbert, M.; Golding, N.; Zhou, H.; Wint, G.R.W.; Robinson, T.P.; Tatem, A.J.; Lai, S.; Zhou, S.; Jiang, H.; Guo, D.; et al. Predicting the risk of avian influenza A H7N9 infection in live-poultry markets across Asia. Nat. Commun. 2014, 5, 4116. [Google Scholar] [CrossRef]
- Bhatt, S.; Weiss, D.J.; Cameron, E.; Bisanzio, D.; Mappin, B.; Dalrymple, U.; Battle, K.E.; Moyes, C.L.; Henry, A.; Eckhoff, P.A.; et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015, 526, 207–211. [Google Scholar] [CrossRef]
- Frelat, R.; Lopez-Ridaura, S.; Giller, K.E.; Herrero, M.; Douxchamps, S.; Djurfeldt, A.A.; Erenstein, O.; Henderson, B.; Kassie, M.; Paul, B.K.; et al. Drivers of household food availability in sub-Saharan Africa based on big data from small farms. Proc. Natl. Acad. Sci. USA 2015, 113, 458–463. [Google Scholar] [CrossRef]
- Esri. ArcGIS Help Document: How the Path Distance Tools Work. 2021. Available online: https://desktop.arcgis.com/en/arcmap/latest/tools/spatial-analyst-toolbox/how-the-path-distance-tools-work.htm (accessed on 10 April 2023).
- Escofier, B.; Pagès, J. Multiple Factor Analysis (AFMULT Package). Comput. Stat. Data Anal. 1994, 18, 121–140. [Google Scholar] [CrossRef]
- Park, H.-S.; Jun, C.-H. A Simple and Fast Algorithm for K-Medoids Clustering. Expert Syst. Appl. 2009, 36, 3336–3341. [Google Scholar] [CrossRef]
- Sauder, D.C.; Demars, C.E. An Updated Recommendation for Multiple Comparisons. Adv. Methods Pract. Psychol. Sci. 2019, 2, 26–44. [Google Scholar] [CrossRef]
- Perneger, T.V. What’s Wrong with Bonferroni Adjustments. BMJ 1998, 316, 1236–1238. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhang, G.; Zhou, C. Differences in Accessibility of Public Health Facilities in Hierarchical Municipalities and the Spatial Pattern Characteristics of Their Services in Doumen District, China. Land 2021, 10, 1249. [Google Scholar] [CrossRef]
- Ermagun, A.; Tilahun, N. Equity of Transit Accessibility across Chicago. Transp. Res. Part D Transp. Environ. 2020, 86, 102461. [Google Scholar] [CrossRef]
- Jang, S.; Lee, S. Study of the Regional Accessibility Calculation by Income Class Based on Utility-Based Accessibility. J. Transp. Geogr. 2020, 84, 102697. [Google Scholar] [CrossRef]
- Tao, S.; Cheng, L.; He, S.; Witlox, F. Examining the Non-Linear Effects of Transit Accessibility on Daily Trip Duration: A Focus on the Low-Income Population. J. Transp. Geogr. 2023, 109, 103600. [Google Scholar] [CrossRef]
- Marques, J.L.; Wolf, J.; Feitosa, F. Accessibility to Primary Schools in Portugal: A Case of Spatial Inequity? Reg. Sci. Policy Pract. 2021, 13, 693–707. [Google Scholar] [CrossRef]
- Xu, Y.; Song, W.; Liu, C. Social-Spatial Accessibility to Urban Educational Resources under the School District System: A Case Study of Public Primary Schools in Nanjing, China. Sustainability 2018, 10, 2305. [Google Scholar] [CrossRef]
- Dutton, D. Financial, Organizational and Professional Factors Affecting Health Care Utilization. Soc. Sci. Med. 1986, 23, 721–735. [Google Scholar] [CrossRef]
- Strauss, A.L. Medical Organization, Medical Care and Lower Income Groups. Soc. Sci. Med. 1969, 3, 143–177. [Google Scholar] [CrossRef]
- Ricciardi, A.M.; Xia, J.; Currie, G. Exploring Public Transport Equity between Separate Disadvantaged Cohorts: A Case Study in Perth, Australia. J. Transp. Geogr. 2015, 43, 111–122. [Google Scholar] [CrossRef]
- Rawl, J. A Theory of Justice. Bamforth N 1971, 14, 26–28. [Google Scholar] [CrossRef]
- Akbar, M.; Abdullah; Naveed, A.; Syed, S.H. Does an Improvement in Rural Infrastructure Contribute to Alleviate Poverty in Pakistan? A Spatial Econometric Analysis. Soc. Indic. Res. 2022, 162, 1. [Google Scholar] [CrossRef]
- Fereira, S.B.; Cateia, J.V. Trade reform, infrastructure investment, and structural transformation in Africa: Evidence from Guinea-Bissau. Emerg. Mark. Rev. 2023, 55, 101027. [Google Scholar] [CrossRef]
- Xiao, H.; Zheng, X.Y.; Xie, L.Y. Promoting pro-poor growth through infrastructure investment: Evidence from the Targeted Poverty Alleviation program in China. China Econ. Rev. 2022, 71, 101729. [Google Scholar] [CrossRef]
- Tao, Z.; Wang, Q. Facility or Transport Inequality? Decomposing Healthcare Accessibility Inequality in Shenzhen, China. Int. J. Environ. Res. Public Health 2022, 19, 6897. [Google Scholar] [CrossRef]



| Socioeconomic Attributes | Indicators | Classification Criteria | Inhabitants’ Classification |
|---|---|---|---|
| Population density | People/km2 | General density (<100) | Gd-C |
| High density (≥100) | Hd-C | ||
| Registered residence structure | Registered residents/total population | Foreign population (<25%) | Fp-C |
| Mixed population (25%–75%) | Mp-C | ||
| Local population (≥75%) | Lp-C | ||
| Age structure | People over 60 years old/total population | Nonaging (<10%) | N-C |
| Aging (≥10%) | A-C | ||
| Income level | Yuan/person | Low income (<10,000) | L-C |
| Middle income (10,000–30,000) | M-C | ||
| High income (≥30,000) | H-C |
| Population Density | Age Structure | Registered Residence Structure | Income Level | Designation | Population Density | Age Structure | Registered Residence Structure | Income Level | Designation |
|---|---|---|---|---|---|---|---|---|---|
| General density | Nonaging | Foreign | Low | Gd-N-Fp-L | High density | Nonaging | Foreign | Low | Hd-N-Fp-L |
| Middle | Gd-N-Fp-M | Middle | Hd-N-Fp-M | ||||||
| High | Gd-N-Fp-H | High | Hd-N-Fp-H | ||||||
| Mixed | Low | Gd-N-Mp-L | Mixed | Low | Hd-N-Mp-L | ||||
| Middle | Gd-N-Mp-M | Middle | Hd-N-Mp-M | ||||||
| High | Gd-N-Mp-H | High | Hd-N-Mp-H | ||||||
| Local | Low | Gd-N-Lp-L | Local | Low | Hd-N-Lp-L | ||||
| Middle | Gd-N-Lp-M | Middle | Hd-N-Lp-M | ||||||
| High | Gd-N-Lp-H | High | Hd-N-Lp-H | ||||||
| Aging | Foreign | Low | Gd-A-Fp-L | Aging | Foreign | Low | Hd-A-Fp-L | ||
| Middle | Gd-A-Fp-M | Middle | Hd-A-Fp-M | ||||||
| High | Gd-A-Fp-H | High | Hd-A-Fp-H | ||||||
| Mixed | Low | Gd-A-Mp-L | Mixed | Low | Hd-A-Mp-L | ||||
| Middle | Gd-A-Mp-M | Middle | Hd-A-Mp-M | ||||||
| High | Gd-A-Mp-H | High | Hd-A-Mp-H | ||||||
| Local | Low | Gd-A-Lp-L | Local | Low | Hd-A-Lp-L | ||||
| Middle | Gd-A-Lp-M | Middle | Hd-A-Lp-M | ||||||
| High | Gd-A-Lp-H | High | Hd-A-Lp-H |
| Group | Group Name | Group Characteristics |
|---|---|---|
| Group 1 | Ethnic minorities and large-scale families | Highest proportion of ethnic minorities; family size is large |
| Group 2 | Young, with superior geographical conditions | Highest proportion of young and middle-aged people, superior geographical environment, convenient transportation |
| Group 3 | Old and less educated | Highest proportion of aging population; low education levels |
| Group 4 | Sick, disabled, and lonely | Highest proportion of population with diseases and disabilities; family size is small |
| Inhabitant Attributes | Minimum Cost Distance for Public Facilities | ||
|---|---|---|---|
| Healthcare Facilities | Educational Facilities | Sanitary Facilities | |
| Population density | −0.528 ** | −0.601 *** | −0.497 ** |
| Registered residence ratio | −0.315 * | −0.376 * | −0.102 |
| Aging level | −0.480 ** | −0.301 * | −0.320 * |
| Income level | −0.574 *** | −0.533 ** | −0.515 ** |
| Inhabitant Attributes | Minimum Cost Distance for Public Facilities | |||
|---|---|---|---|---|
| Healthcare Facilities | Educational Facilities | Sanitary Facilities | Weighted Average Min Cost Distance | |
| Gd-N-Fp-M | 65.89 | 38.22 | 35.76 | 46.62 |
| Gd-N-Fp-H | 60.52 | 32.76 | 33.28 | 42.19 |
| Gd-N-Mp-M | 66.72 | 39.04 | 36.48 | 47.41 |
| Gd-N-Mp-H | 62.08 | 34.57 | 34.55 | 43.73 |
| Gd-N-Lp-L | 72.70 | 44.32 | 37.32 | 51.45 |
| Gd-N-Lp-M | 67.64 | 41.65 | 35.09 | 48.13 |
| Gd-A-Mp-L | 53.52 | 49.55 | 47.93 | 50.33 |
| Gd-A-Mp-M | 50.67 | 46.87 | 45.72 | 47.75 |
| Gd-A-Lp-L | 59.21 | 48.29 | 49.24 | 52.25 |
| Gd-A-Lp-M | 53.68 | 45.52 | 46.77 | 48.66 |
| Hd-N-Fp-H | 46.80 | 30.09 | 30.91 | 35.93 |
| Hd-N-Mp-M | 44.52 | 28.51 | 33.50 | 35.51 |
| Hd-N-Mp-H | 42.04 | 26.46 | 32.38 | 33.63 |
| Hd-A-Mp-L | 48.75 | 48.72 | 40.22 | 45.90 |
| Hd-A-Lp-L | 58.97 | 50.28 | 42.59 | 50.61 |
| Poverty Groups | Minimum Cost Distance for Public Facilities | ||
|---|---|---|---|
| Healthcare Facilities | Educational Facilities | Sanitary Facilities | |
| Group 1 | 0.472 ** | 0.489 ** | 0.275 * |
| Group 2 | 0.311 * | 0.470 ** | 0.138 |
| Group 3 | 0.502 ** | 0.568 *** | 0.208 * |
| Group 4 | 0.625 *** | 0.397 ** | 0.289 * |
| Poverty Groups | Minimum Cost Distance for Public Facilities (Minutes) | |||
|---|---|---|---|---|
| Healthcare Facilities | Educational Facilities | Sanitary Facilities | Weighted Average Min Cost Distance | |
| Group 1 | 58.32 | 47.88 | 60.20 | 55.47 |
| Group 2 | 43.04 | 39.65 | 40.22 | 40.97 |
| Group 3 | 59.28 | 52.80 | 56.95 | 56.34 |
| Group 4 | 63.64 | 62.85 | 63.72 | 63.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.; Feng, Y.; Wei, Y.; Sun, D.; Li, X.; Zhong, F. Assessing Regional Public Service Facility Accessibility Using Multisource Geospatial Data: A Case Study of Underdeveloped Areas in China. Remote Sens. 2024, 16, 409. https://doi.org/10.3390/rs16020409
Huang C, Feng Y, Wei Y, Sun D, Li X, Zhong F. Assessing Regional Public Service Facility Accessibility Using Multisource Geospatial Data: A Case Study of Underdeveloped Areas in China. Remote Sensing. 2024; 16(2):409. https://doi.org/10.3390/rs16020409
Chicago/Turabian StyleHuang, Chunlin, Yaya Feng, Yao Wei, Danni Sun, Xianghua Li, and Fanglei Zhong. 2024. "Assessing Regional Public Service Facility Accessibility Using Multisource Geospatial Data: A Case Study of Underdeveloped Areas in China" Remote Sensing 16, no. 2: 409. https://doi.org/10.3390/rs16020409
APA StyleHuang, C., Feng, Y., Wei, Y., Sun, D., Li, X., & Zhong, F. (2024). Assessing Regional Public Service Facility Accessibility Using Multisource Geospatial Data: A Case Study of Underdeveloped Areas in China. Remote Sensing, 16(2), 409. https://doi.org/10.3390/rs16020409