4.1. Basic Data Characteristics and Pre-Estimation Tests
Before estimating the ARDL models, it is necessary to discuss and perform some pre-estimation tests to determine whether the values of variables are consistent with the theory of the model or not. To do this, we first estimate the descriptive statistics of the variables, which describe the major characteristics of the data.
Table 1 presents the estimated values for key descriptive statistics, including means, maximum and minimum values, and standard deviations for the selected variables. Next, we need to check the stationarity of the variables using unit root tests to avoid spurious regression. Once all model variables passed the stationarity tests, we checked for long-run cointegration among all variables in the model using the bound test to estimate the ARDL model. Finally, after estimating the model, we need to perform several diagnostic tests to ensure that the overall results of the model are correct.
According to the methodology outlined, the bounds test framework is suitable for variables that are either integrated at level I(0) or first difference I(1). To determine the order of integration among the variables and prevent incorrect results, unit root tests were conducted. The null hypothesis of the presence of a unit root test was evaluated against the alternative hypothesis of stationarity using the Augmented Dickey–Fuller (ADF) and Phillips–Perron tests, with the findings presented in
Table 2.
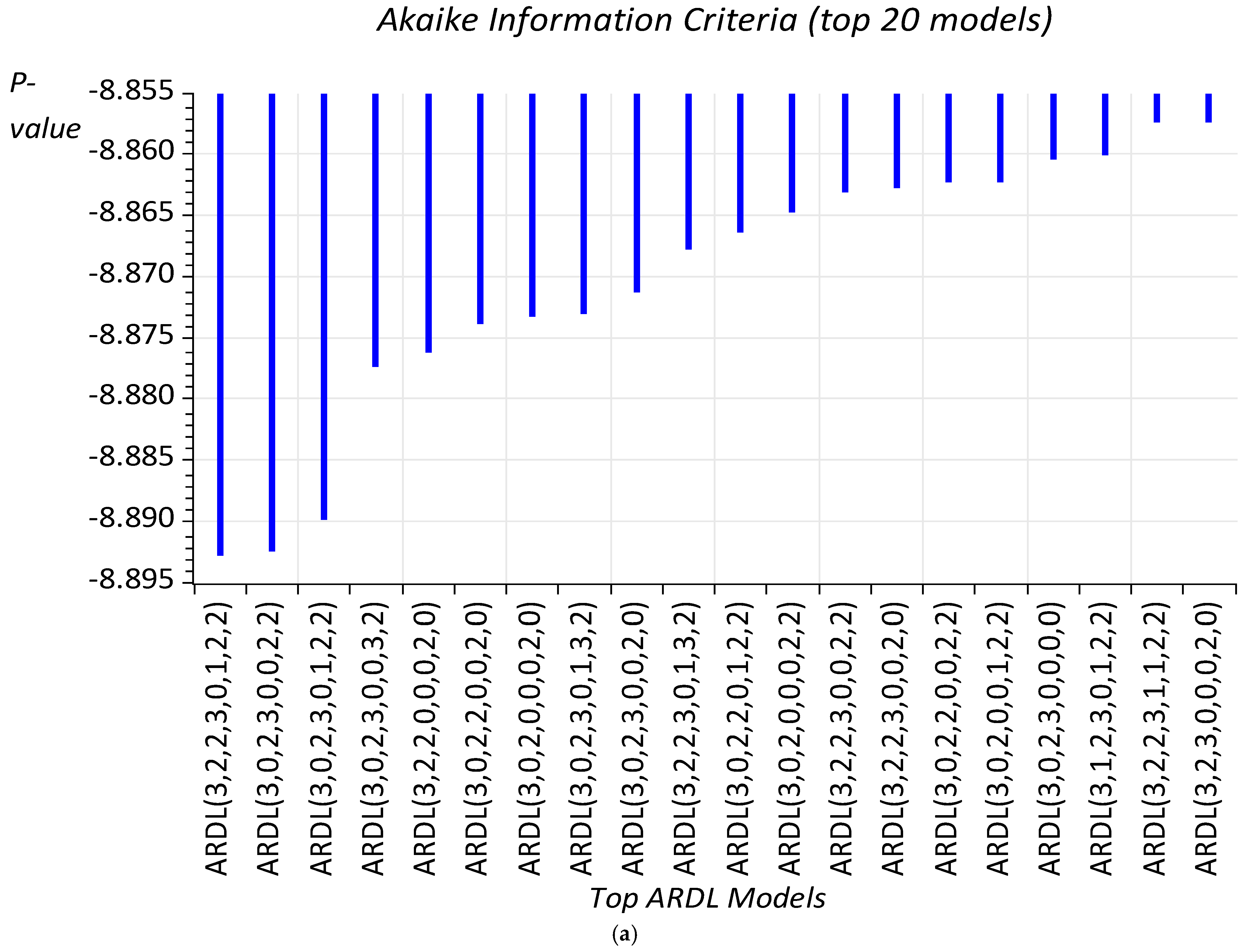
Through unit root testing on the selected variables in our study, we discovered that all variables exhibit stationarity after the first difference, except trade and renewable energy consumption, which are stationary at both I(0) and I(1). Consequently, we can confidently move forward with the ARDL estimation framework, particularly since our dependent variables—life expectancy and mortality—are established as I(1). Given the ample observations, we employed the Akaike Information Criterion (AIC) to determine the optimal lag for the ARDL model.
Table 3 presents the estimated bound tests for both models, which have undergone several diagnostic evaluations successfully (see
Table 4 for details). The F-test results in
Table 3 provide compelling evidence of cointegration, indicating a long-term relationship among life expectancy or mortality, trade, gross fixed capital formation, household expenditure, public health expenditure, renewable energy consumption, and transport CO
2 emissions—as an indicator for biofuel consumption in New Zealand’s transport sector—at a significance level of 1% (see Table 6 for further insights). Additionally,
Table 4 indicates that the ARDL results meet all diagnostic criteria, with the optimal ARDL lag structure determined based on the lowest AIC, as illustrated in
Figure 3.
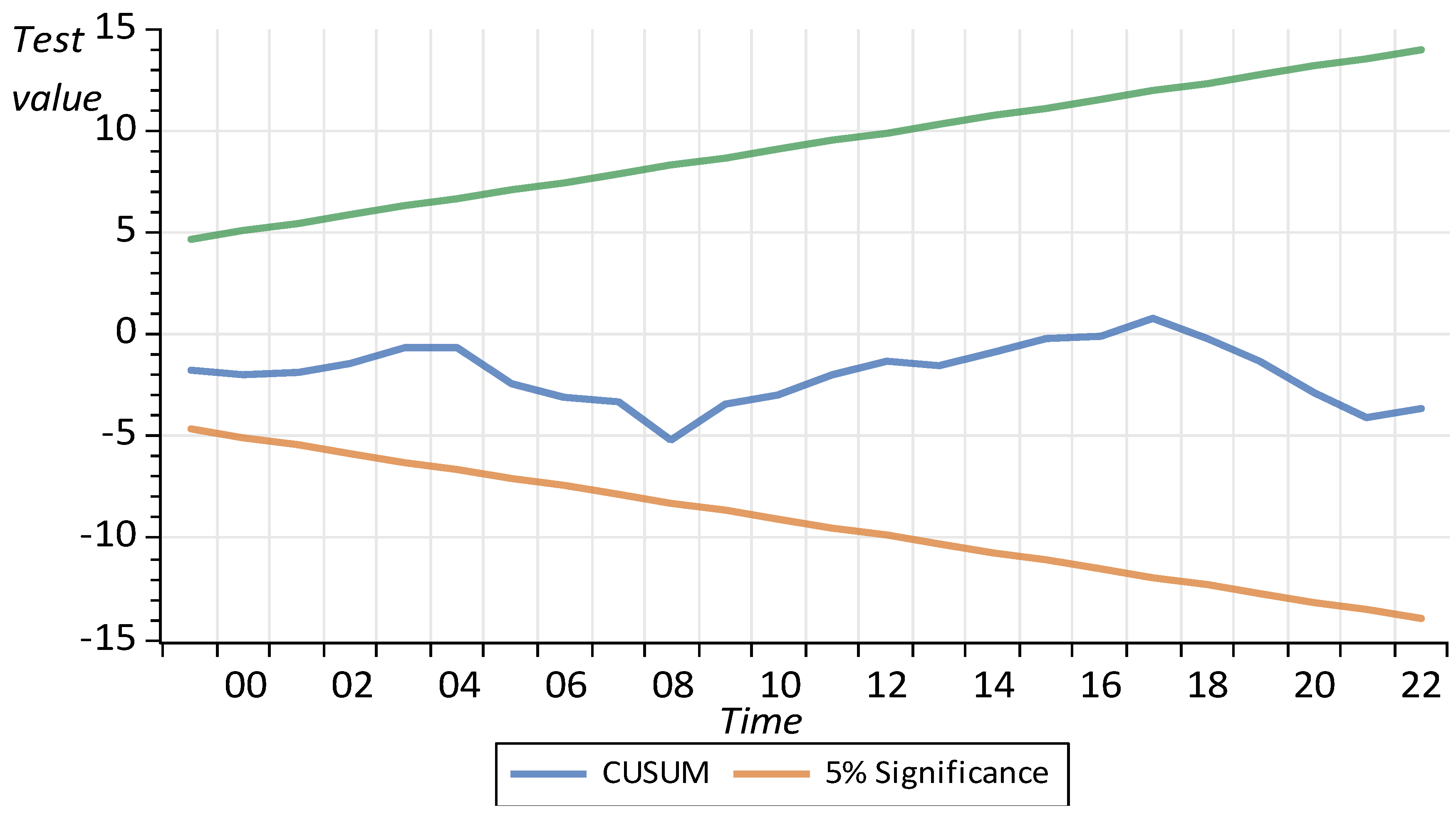
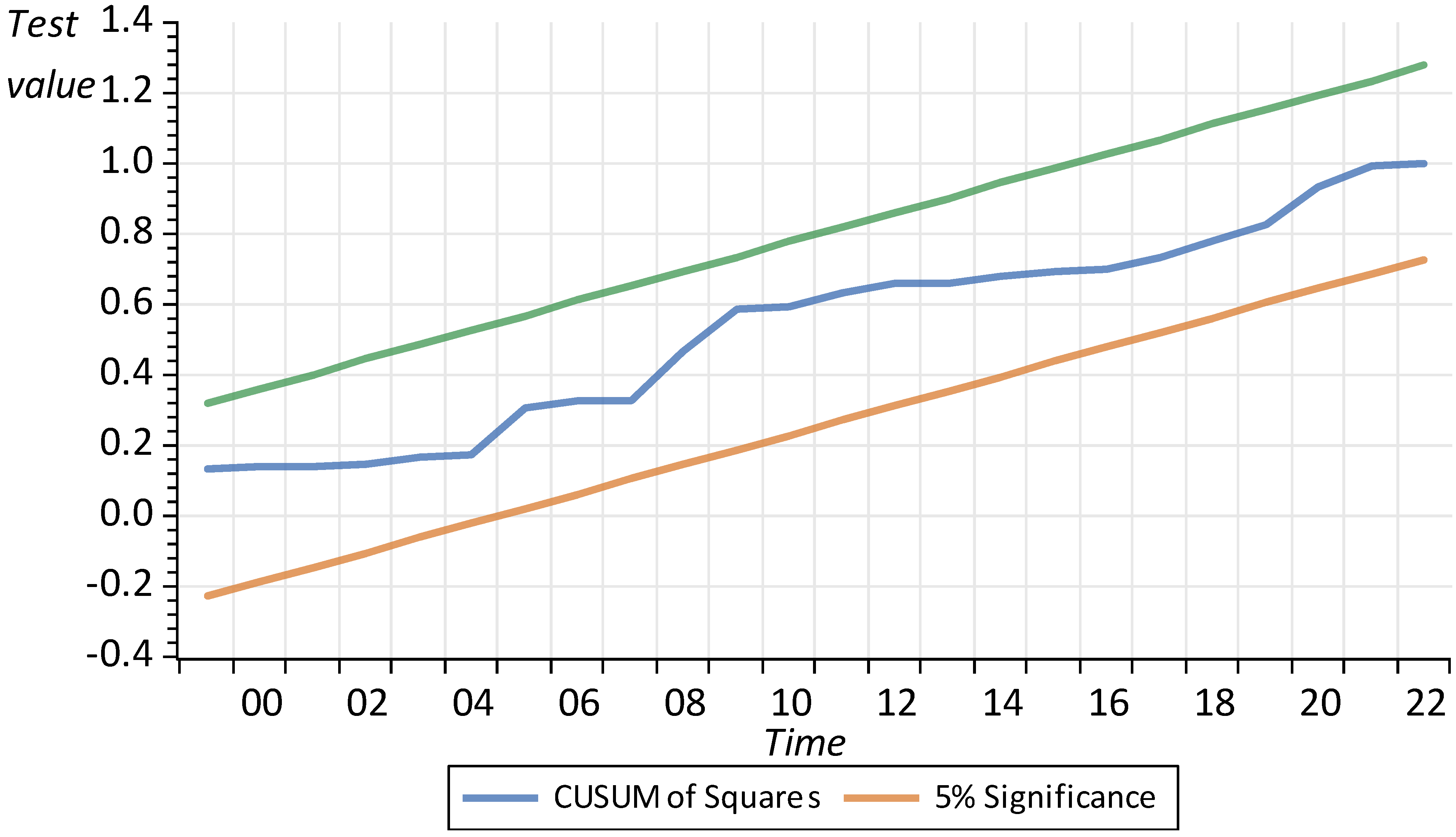
To evaluate the structural changes in the New Zealand economy, we employ the cumulative sum (CUSUM) and cumulative sum of squares (CUSUMSQ) tests developed by Brown et al. [
59]. These tests assess the stability of both short- and long-run coefficients.
Figure 4 and
Figure 5 illustrate the CUSUM and CUSUMSQ test statistics for both models, which consistently fall within the critical bounds at the 5% significance level. This indicates that the estimated parameters remain stable over time, reinforcing the robustness of our statistical findings.
4.2. The ARDL Results for Life Expectancy Model
Table 5 presents the dynamic ARDL simulation results for model 1, illustrating the effects of the various variables on life expectancy in New Zealand. The findings reveal that while trade has a positive relationship with life expectancy in the short term, its long-term relationship is positive yet insignificant. Specifically, a 1% increase in trade may correlate with a 0.02% rise in life expectancy in the short run. This suggests that increased trade activities may enhance household welfare, leading to improved life expectancy. Given the limited research on the relationship between trade and life expectancy, we draw on GDP as an alternative variable to support our findings, as trade is one of the main components of GDP calculation. These results align with the existing literature, including the study by Murthy et al. [
15], which demonstrates a positive relationship between economic growth and life expectancy in D-8 countries; Shaari et al. [
50] reached a similar conclusion.
Gross fixed capital formation, which means saving and investment in infrastructure, has a positive and insignificant relationship with life expectancy in the long run, but it has a negative and still insignificant impact in the short run. Household expenditure may have a positive impact on life expectancy in the long run, suggesting that a 1% increase in household expenditures is associated with a 0.005% increase in life expectancy. It may also have a short-term positive impact on life expectancy, although of a smaller magnitude (0.002). Given that consumption is the primary component of the household’s utility function, an increase in household expenditure on goods and services indicates that households want to improve their welfare assuming inflation remains constant.
Public health expenditures emerge as a significant factor that can positively influence life expectancy. As illustrated in
Table 5, these expenditures yield beneficial effects in both the short and long term; however, the long-run coefficient lacks statistical significance. Specifically, the short-run coefficient of public health expenditure is 0.046, indicating that a 1% increase in public health spending is associated with a 0.05% rise in life expectancy within the nation. These findings align with the research conducted by Murthy et al. [
15] concerning D-8 countries. Furthermore, studies by Owusu et al. [
60] and Ahmad et al. [
29] support the notion that enhanced health expenditure contributes to increased life expectancy.
The findings indicate that urbanisation influences life expectancy primarily over the long term, with a clear positive relationship between the two. It suggests that a 1% rise in urbanisation is associated with a 0.43% increase in life expectancy in the long run. As urban areas expand, they offer enhanced facilities, including diverse educational opportunities at all levels, high-quality transportation systems, professional healthcare services, and various recreational spaces like parks. These improvements significantly boost overall welfare and longevity. This aligns with the study by Mahalik et al. [
16], which confirmed that urbanisation can positively impact life expectancy across developed, emerging, and developing nations. Additionally, Tripathi and Maiti [
30] emphasised that sustainable urbanisation, when effectively managed, can lead to improved health outcomes.
Two other crucial factors influencing life expectancy are renewable energy consumption and transport-related CO
2 emissions. The ARDL analysis presented in
Table 5 reveals a positive relationship between renewable energy consumption and life expectancy, both in the short and long run. Specifically, a 1% increase in renewable energy consumption correlates with a 0.03% increase in life expectancy over the long run and a 0.02% increase in the short run. These findings are consistent with research conducted by Guo et al. [
49] and Shaari et al. [
50], which also identifies the positive effects of renewable energy consumption on life expectancy.
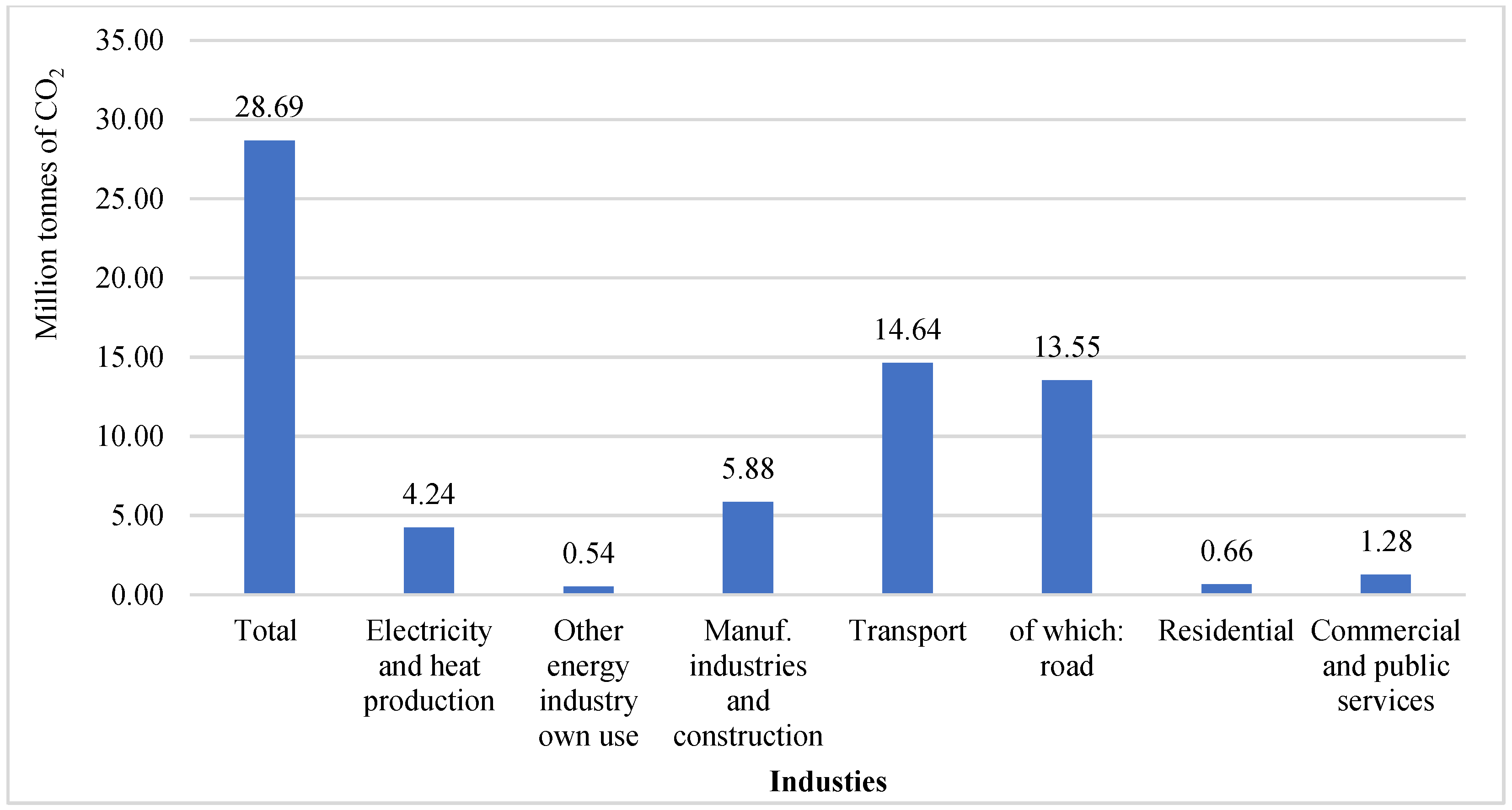
Transport-related CO2 emissions, as highlighted in the introduction, influence life expectancy and mortality by generating air pollutants and toxic gases. Consequently, their impact is indirect. Transport CO2 emissions can diminish life expectancy, both in the short and long term. Specifically, a 1% increase in transport CO2 emissions correlates with a decrease in life expectancy of 0.07% in the long run and 0.05% in the short run. This issue primarily arises from the reliance on non-clean fuels, such as fossil fuels, which significantly increase emissions in the environment. Living in areas with high air pollution and toxic gases exacerbates health issues for households, resulting in increased healthcare expenditures. Consequently, households will have less disposable income for leisure and other activities, leading to a decline in their welfare and life expectancy.
Research by Emodi et al. [
48] and Osabohien et al. [
45] supports these findings, demonstrating the adverse effects of CO
2 emissions on life expectancy across various countries. Similarly, Mahalik et al. [
16] identified a negative correlation between CO
2 emissions and life expectancy in a study encompassing 65 countries. However, Das and Debanth [
44] reported that CO
2 emissions are not associated with an adverse effect on life expectancy in India.
The coefficient of the error correction term (ECT(-1)) has a negative sign and is statistically significant. The analysis indicates that 15% of error correction takes place annually, moving towards long-run equilibrium, as evidenced by the negative and highly significant nature of the error correction term (ECT). This confirms a causal relationship between trade, gross fixed capital formation, household expenditure, public health expenditure, renewable energy consumption, and transport CO2 emissions with life expectancy.
Table 6 showcases the results from the dynamic ARDL simulation method, supporting the findings presented in
Table 5. This model has been developed to assess the influence of shocks in renewable energy consumption and transport-related CO
2 emissions on life expectancy. The simulation outcomes indicate that a 1% rise in public health expenditure and renewable energy consumption can be associated with increases in life expectancy of approximately 0.04% and 0.01% in the long run, respectively. However, the short-term effects of these variables are not statistically significant.
We employed the dynamic ARDL simulation model to simulate the long-run effects of a 5% change (increase and decrease) in renewable energy consumption and transport CO
2 emissions on life expectancy. The results of these simulations are presented in
Figure 6 and
Figure 7.
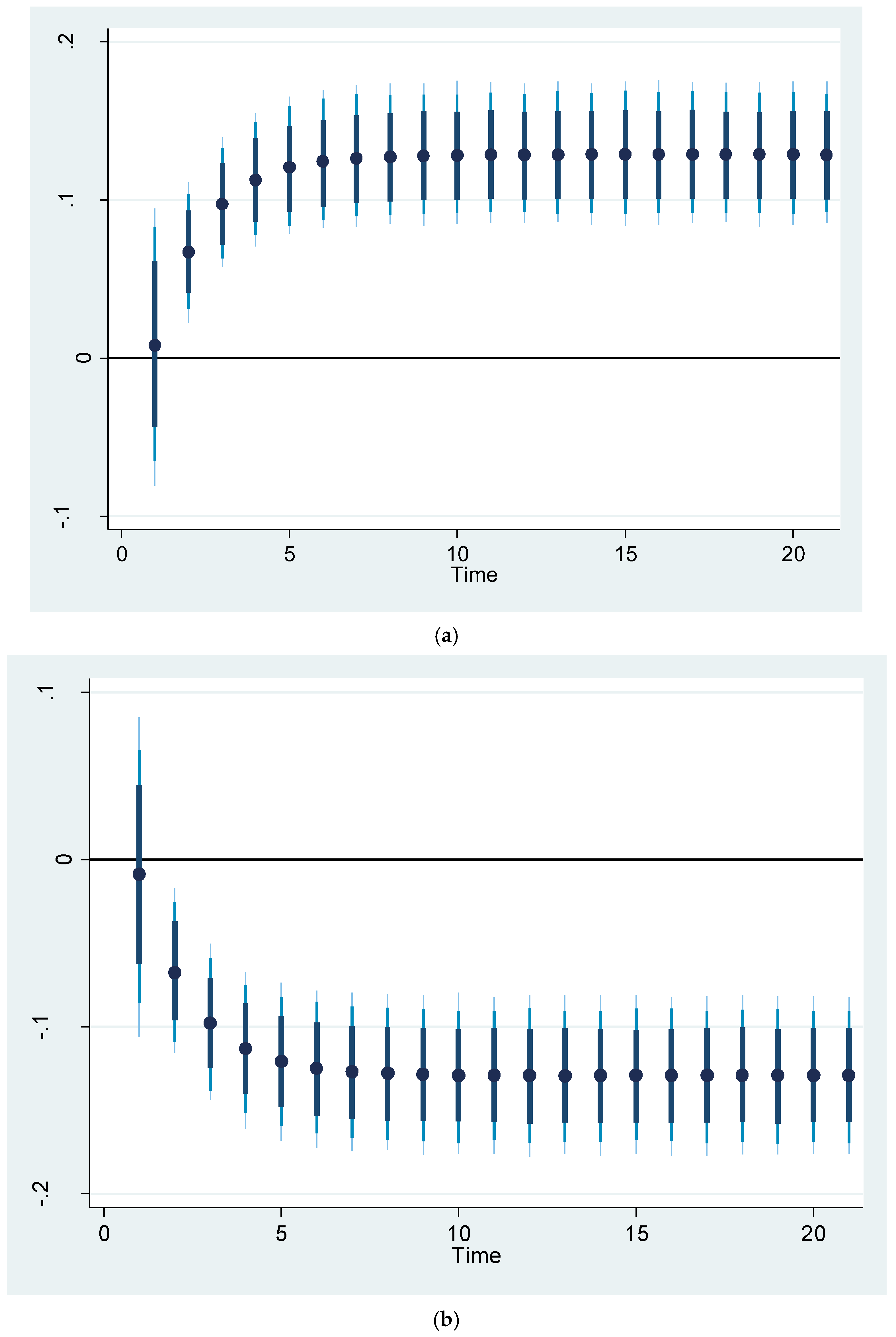
Figure 6 shows the impact of a 5% increase and decrease in renewable energy consumption on life expectancy. It shows that increasing or decreasing renewable energy consumption by 5% can be associated with a corresponding increase or decrease in life expectancy of approximately 1.2%. It should be noted that the shock at the first stage may either increase or decrease the life expectancy, depending on the circumstances. The values are higher than the coefficients of this variable in
Table 5 and
Table 6 because of the magnitude of the shock inflicted on this variable. In
Figure 6, the black dot (●) represents the predicted life expectancy resulting from a 5% shock in renewable energy consumption in a log-log model. The dark, light blue, and dark blue spikes indicate 75%, 90%, and 95% confidence intervals, respectively.
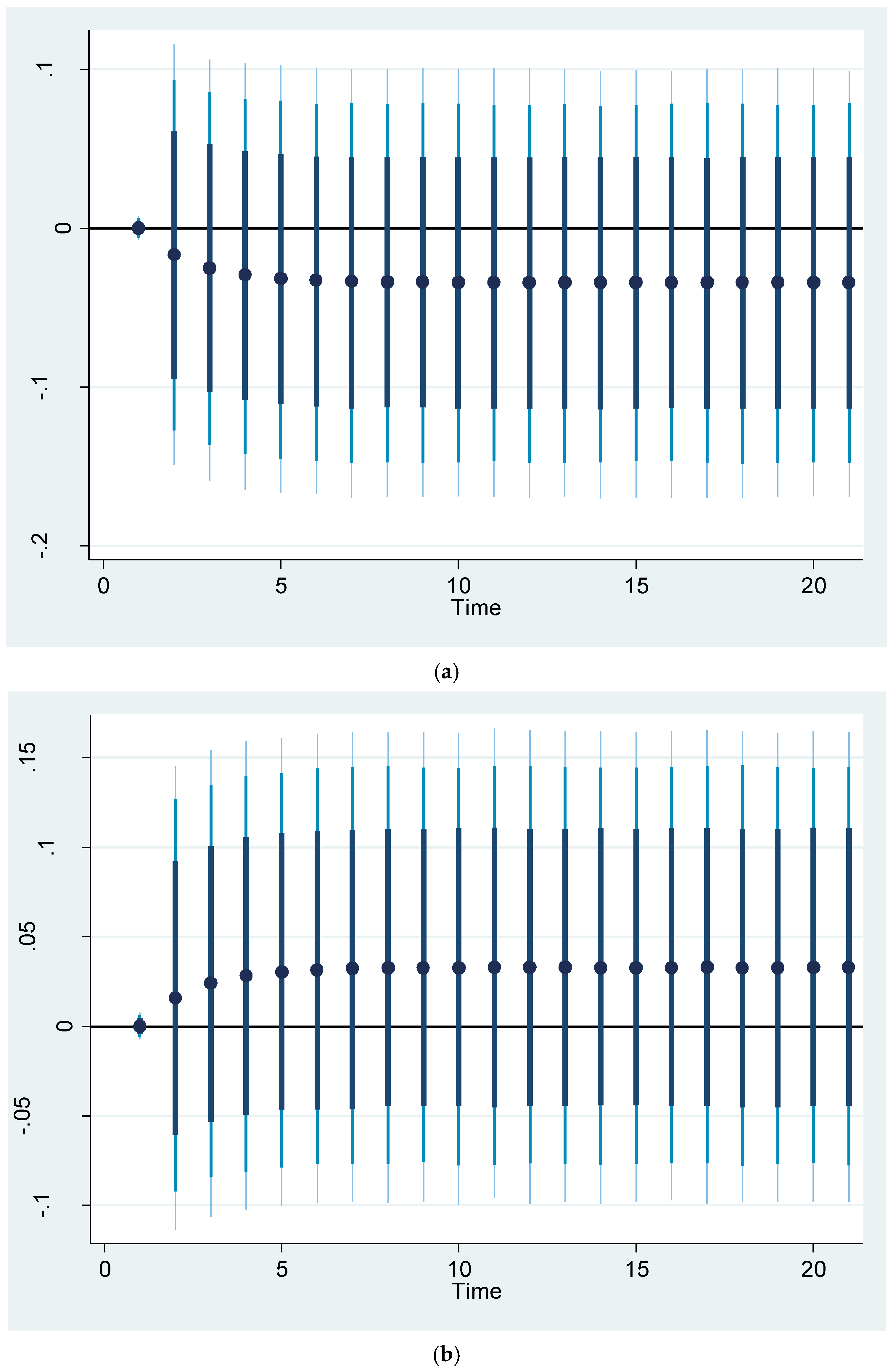
The simulation model presented in
Figure 7 shows the effects of a 5% increase and decrease in transport CO
2 emissions on life expectancy. The findings show that a 5% increase or decrease in CO
2 emissions from the transportation sector is expected to result in a decrease or increase in New Zealanders’ life expectancy of nearly 0.04%, respectively. It is worth noting that the shock at the first stage may not change the life expectancy. The values are greater than the coefficient of this variable in
Table 5 and
Table 6 in the long run. This is because of the magnitude of the shock that affected life expectancy. The impact of renewable energy consumption on life expectancy is greater than the transport CO
2 emissions because it includes all renewable energy sources.
4.3. The ARDL Results for the Mortality Model
Table 7 reports the estimated results of the ARDL model for mortality (model 2). It shows the short- and long-run impacts of trade, gross fixed capital formation, household expenditure, government health expenditures, urbanisation, renewable energy consumption, and transport CO
2 emissions on mortality in New Zealand. The results indicate that trade has a negative and statistically significant correlation with mortality in both the short and long run. This means that a 1% increase in trade can reduce mortality by 0.59% in the long run and 0.20% in the short run. Trade not only enriches the economy and boosts household incomes, but it also enhances access to essential medicines and health-related resources. This reduces poverty levels and improves overall welfare. Mejia [
61] found that trade can have a negative but insignificant impact on mortality. Byaro et al. [
62] also found that more trade contributes to health improvement and a decline in the mortality rate.
The long-term coefficient for gross fixed capital formation is not only negative but also statistically significant, indicating that increased investment, particularly in public infrastructure and healthcare facilities, such as clean water, sanitation, and transportation systems, can substantially reduce mortality rates [
42]. Berman et al. [
41] demonstrated that in low-income countries, investing in healthcare infrastructure is significantly associated with reductions in maternal and child mortality rates. These findings are also supported by the research by Eboh et al. [
63], who found that gross fixed capital formation can have a positive and significant impact on under-five child mortality. In contrast, research conducted by Sial et al. [
64] and Kiross et al. [
65] highlighted the negative relationship between capital formation and mortality.
Household expenditure has a negligible and statistically insignificant effect on mortality in both the short and long run. This suggests that while increases in household spending may correlate with decreases in mortality during these periods, the relationship is not strong enough to be considered meaningful. Increased household spending on high-quality food, leisure activities, and medical care does not necessarily result in lower overall mortality rates, particularly among adults. This is due to significant factors such as car accidents and various types of cancer, which are prevalent in New Zealand and other countries.
The urbanisation variable may also have a negative and statistically significant impact on mortality in the long run, but not in the short run. Because of the high accessibility to facilities and healthcare centres in cities, urbanisation can have a negative impact on mortality. Similar results were obtained by Guo et al. [
49], showing that urbanisation can reduce infant mortality in SAARC countries. Tripathi and Maiti [
30] showed that well-managed urbanisation can be beneficial for achieving higher health outcomes. However, high-density urbanisation may increase mortality [
66].
Another variable that may have a negative impact on mortality is public health expenditures. The results in
Table 7 show that public health expenditure has a negative correlation with mortality in both the short and long run, but the short-run coefficient is not statistically significant. The long-run coefficient of public health expenditure is −0.524, indicating that a 1% increase in public health expenditure is associated with a 0.52% decline in mortality. Khatri et al. [
54] pointed out that economic growth and health expenditure can help reduce child mortality in Nepal. Owusu et al. [
60] and Onofrei et al. [
67] also found a negative relationship between health expenditure and mortality.
Renewable energy consumption and CO
2 emissions from transportation are two other important factors that may influence mortality. The results presented in
Table 7 indicate that renewable energy consumption may lead to reduced mortality rates in both the short and long run. This variable shows that living in an environment with lower air pollution can reduce the risk of disease-related air quality issues. Statistics reveal that approximately 43% of New Zealand’s total energy supply in 2023 was derived from renewable energy sources, such as geothermal and hydropower [
68]. Similar results were obtained by Guo et al. [
49], showing that renewable energy consumption can reduce infant mortality in SAARC countries. Byaro and Rwezaula [
34] and Koengkan et al. [
69] also found similar results in their study for 26 sub-Saharan African countries.
In contrast, transport CO
2 emissions may have a positive and statistically significant impact on mortality in both the long and short run. The findings reveal that a 1% rise in transport CO
2 emissions is associated with a 1.6% increase in mortality over the long term and a 0.29% increase in the short term. These results support the results of the studies conducted by Guo et al. [
49], Erdogan et al. [
13], and Adeleye et al. [
52], suggesting that a positive correlation between CO
2 emissions and mortality. Emodi et al. [
48] also showed that transport CO
2 emissions may increase the number of deaths in developing countries.
The coefficient of the error correction term (ECT(-1)) has a negative sign and is statistically significant. It shows the rate of short-run adjustment towards the long-run equilibrium in the event of an equilibrium deviation.
Table 8 presents the results of the dynamic ARDL simulation method. The results support the findings of the ARDL model presented in
Table 7. This model is estimated to simulate the effects of a shock on renewable energy consumption, transport CO
2 emissions, and mortality.
The dynamic ARDL simulation model simulates the long-term effects of a 5% change (increase and decrease) in renewable energy consumption and transport CO
2 emissions on mortality. The results of these simulations are presented in
Figure 8 and
Figure 9.
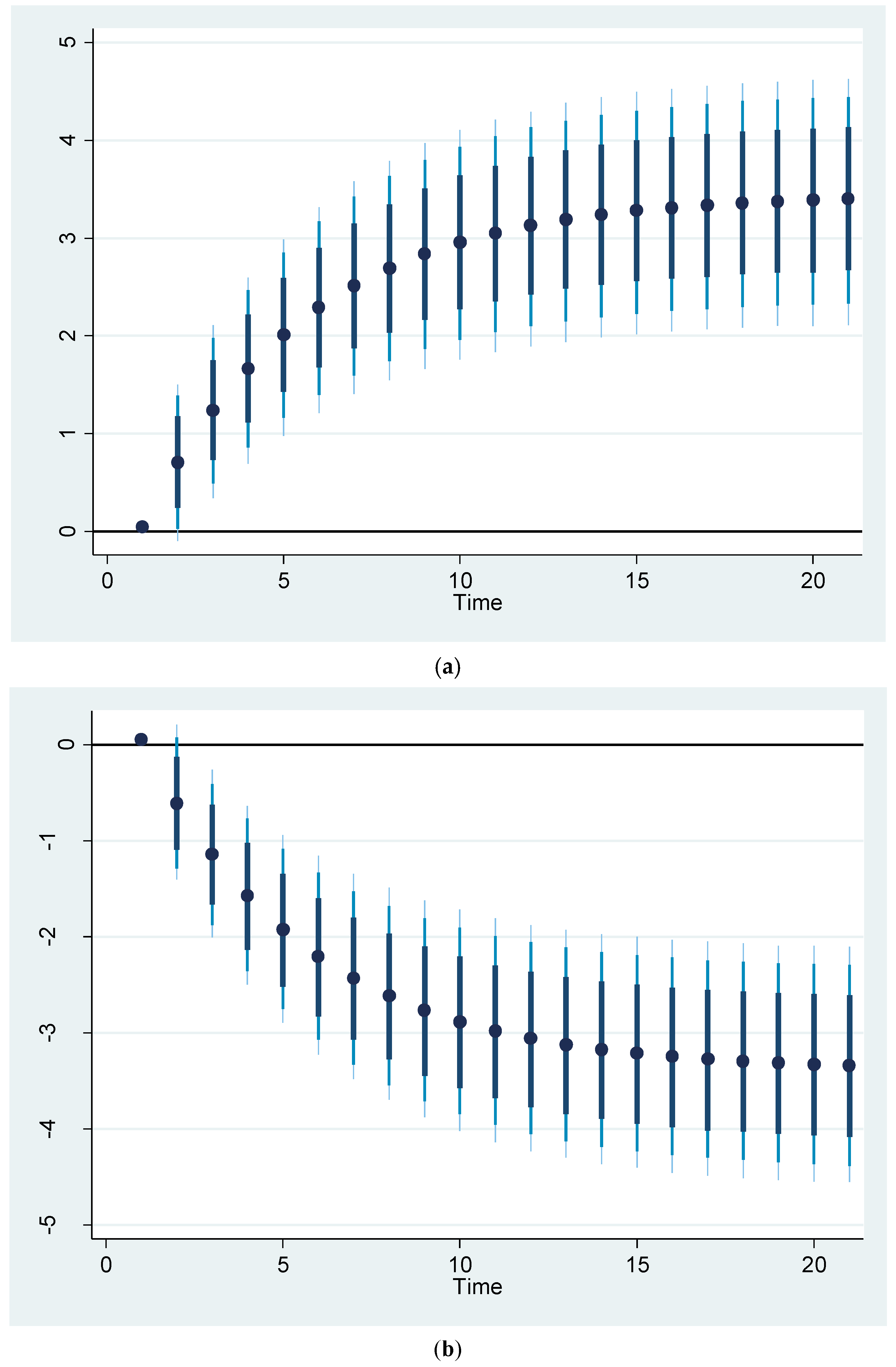
Figure 8 illustrates the effect of a 5% increase and decrease in renewable energy consumption on mortality. The findings indicate that a 5% increase or decrease in renewable energy consumption is expected to be associated with a nearly 2% decrease or increase in mortality rates among New Zealanders. It should be noted that the shock at the first stage may increase or decrease the mortality rate, depending on the circumstances. The values exceed the coefficients for this variable presented in
Table 7 and
Table 8, owing to the intensity of the shock applied to it.
The simulation results illustrated in
Figure 9 demonstrate how a 5% variation—either an increase or decrease—in transport CO
2 emissions may impact mortality rates. The findings reveal a significant correlation: a 5% increase or decrease in CO
2 emissions from the transportation sector may correspond to a nearly 3.3% change in New Zealand’s mortality rate. It should be noted that the shock at the first stage may not affect the mortality rate. In the long run, the values are greater than the coefficient of this variable in
Table 7 and
Table 8. This is because of the magnitude of the shock that affected mortality.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}