
Does Urban Renewal Mitigate the Disease of Cities? An Empirical Study Based on a PSM-DID Model


Abstract
1. Introduction
2. Literature Review and Theoretical Analysis
2.1. Urban Disease
2.2. The Evaluation of Policy Effects on Urban Disease
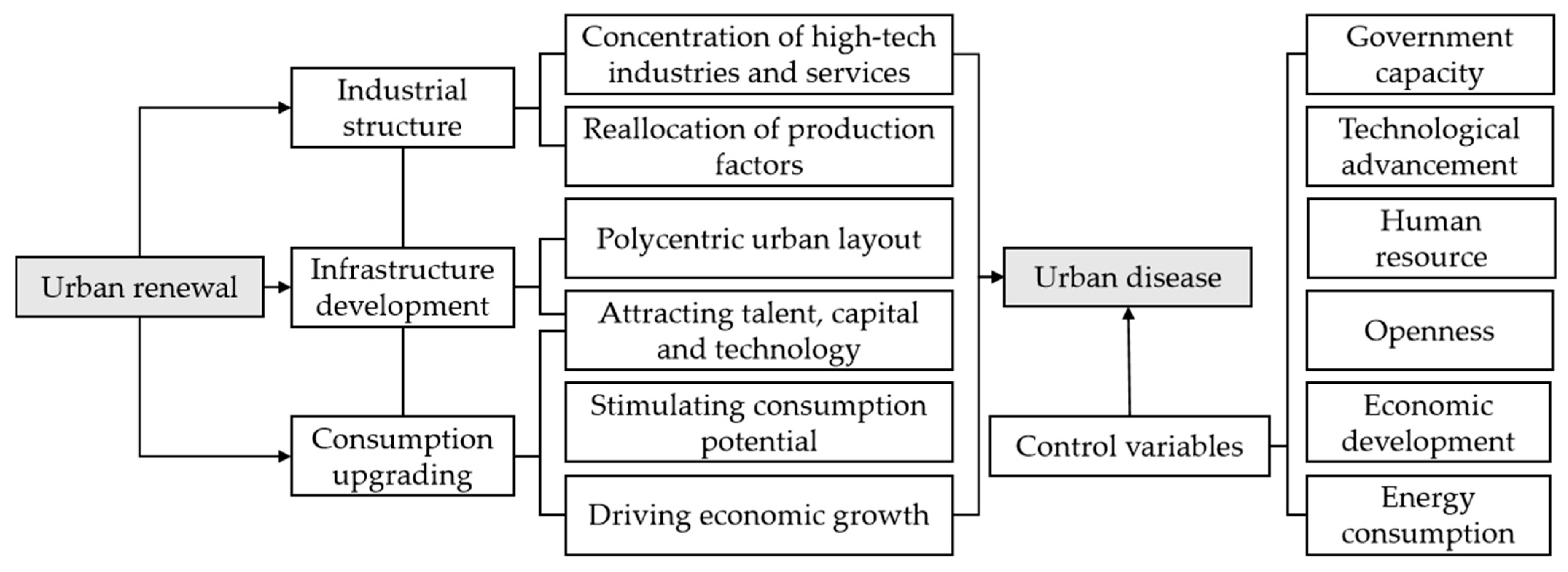
2.3. How Urban Renewal Affects the Disease in Cities
3. Materials and Methods
3.1. Data
3.2. Variable Selection and Data Processing
3.2.1. Urban Disease Indicators
3.2.2. Core Explanatory Variable
3.2.3. Control Variables
3.2.4. Data Processing
3.3. Methodology
4. Results and Discussion
4.1. Urban Disease in China
4.2. Test for Model Assumptions
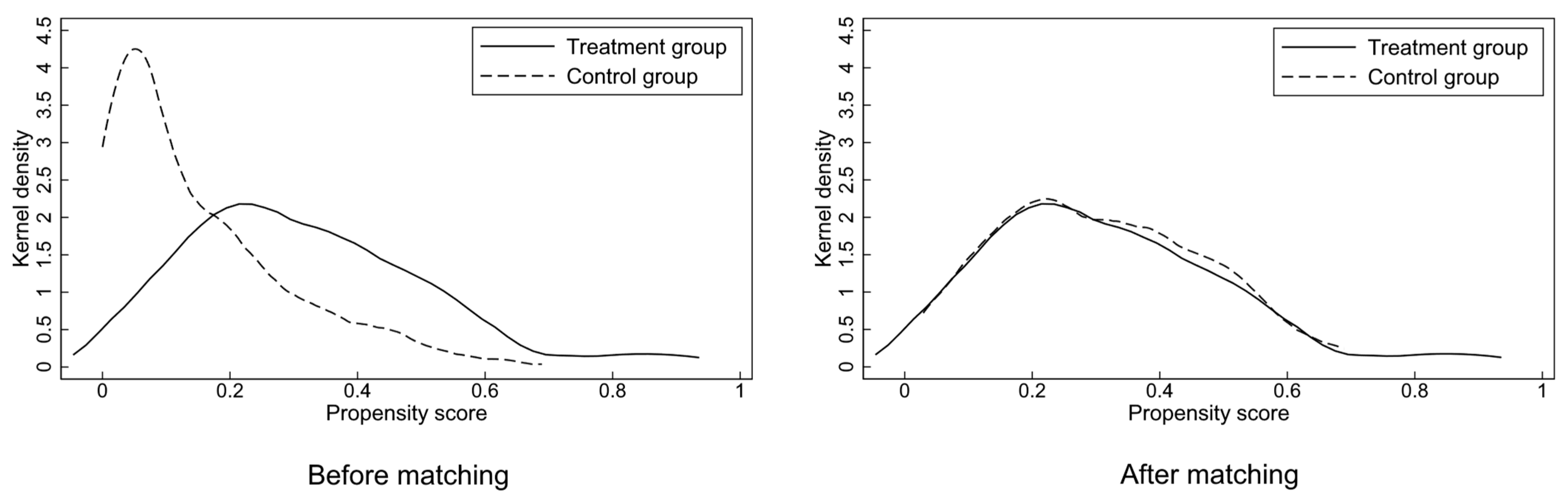
4.2.1. Balance Test
4.2.2. Multicollinearity Test
4.2.3. Hausman Test
4.2.4. Parallel Trend Assumption Test
4.3. Baseline Results
4.4. Robustness Checks
4.5. Heterogeneity Test
4.6. Influence Path Analysis
4.7. Comparison with Other Studies
5. Conclusions and Policy Implications
5.1. Conclusions
- (1)
- The CBER pilot scheme effectively mitigated urban disease in China, and this affect remained significant after a series of robustness tests.
- (2)
- The impact of the CBER pilot scheme was more pronounced in eastern and central regions of China, as well as in cities with high economic development, robust government capacity and abundant human resource.
- (3)
- Industrial structure optimization, infrastructure development and consumption upgrading were all effective pathways for mitigating urban disease through urban renewal.
5.2. Policy Implications
- (1)
- The CBER pilot scheme significantly alleviated urban disease, confirming its effectiveness in concepts and governance methods. Consequently, local governments can address urban problems referring to methods of the CBER pilot scheme. Specifically, the concepts of the CBER scheme can be divided into two aspects. Firstly, governments should restore the degraded natural environment and topography to enhance the living quality of residents using the concept of ecological regeneration. Then, they can rehabilitate urban infrastructure, spatial environment and landscape aesthetic to improve characteristics and vitality of cities using the concept of urban renewal and infill.
- (2)
- (3)
- The effects of the CBER pilot scheme exhibited regional heterogeneity. The variation in these mitigating effects was associated with the selection of pilot cities, with a denser distribution of pilot cities in regions where mitigating effects were better. Consequently, reasonable policy piloting can leverage the driving force of advantageous cities and eliminate regional barriers, facilitating urban problems addressing. Moreover, the development of economic levels, improvement of government functions and expansion of talent introduction are effective means to enhance the effects of urban renewal policies.
- (4)
- Governments should explore multi-dimensional pathways for urban renewal to alleviate urban disease. The potential of industrial innovation, infrastructure development and consumption upgrading can be fully harnessed to address problems in cities by combining urban renewal with them. For example, driving the concentration of high-tech industries and services in city centers through urban renewal can promote a transformation of urban industrial structure towards advancement, reducing pollution emissions and increasing production efficiency.
5.3. Limitations
- (1)
- The measurement of urban disease in this study has been limited to three dimensions constrained by the accessibility of data. The challenges faced by urban development are diverse. Some scholars have considered difficulties and well-being of residents as indicators for assessing urban disease. Future research can adopt a more comprehensive system of indicators to measure urban disease.
- (2)
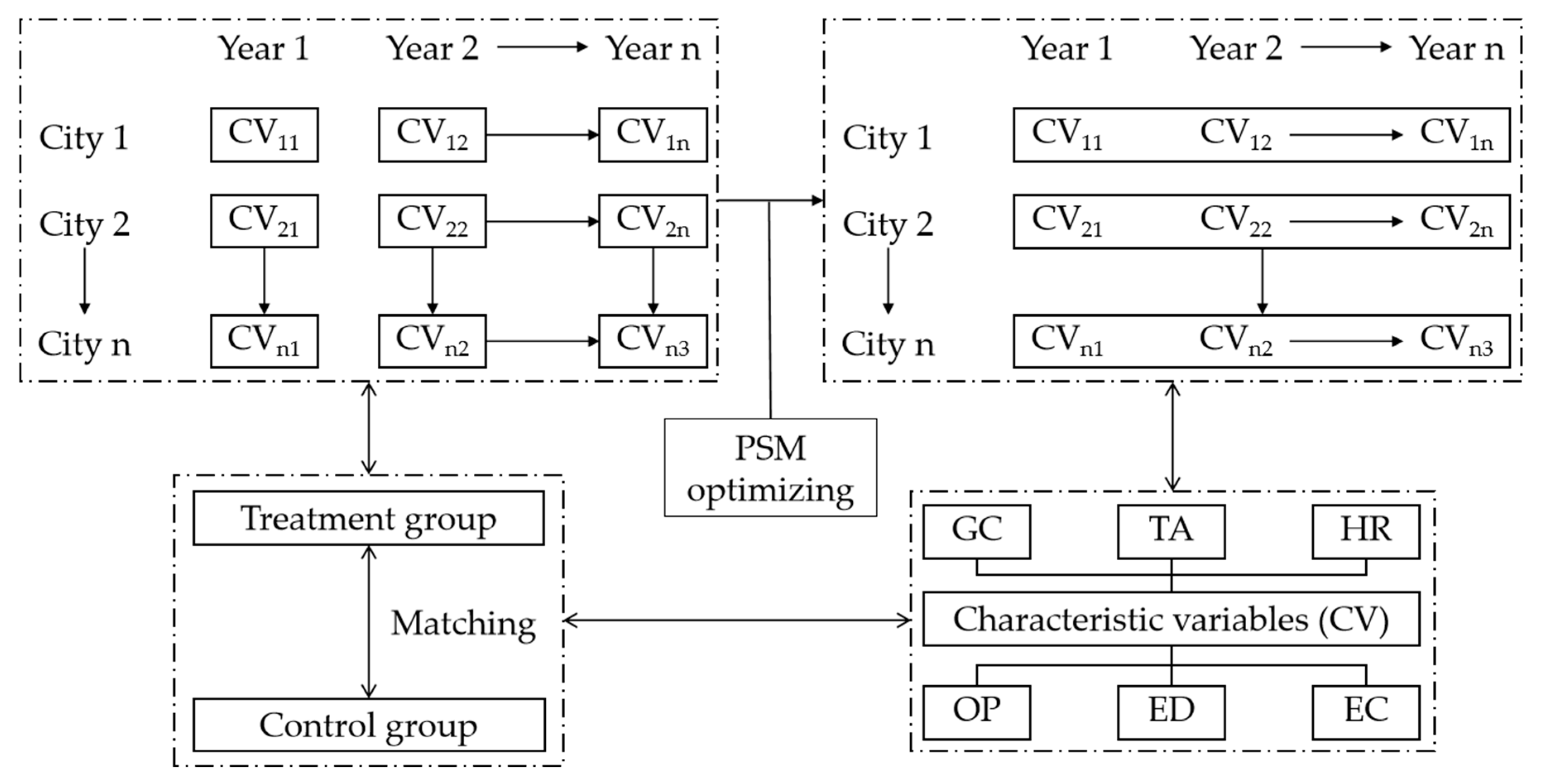
- This study employed an optimized PSM method to match samples, considering overall characteristics of cities in pre-policy years as criteria for propensity score calculating. However, selected characteristic variables still inadequately reflect the propensity of a city being chosen as a pilot city. Future research should endeavor to align with real conditions. By using criteria used by governments for pilot cities selecting, propensity score calculating can better serve in the PSM-DID model.
- (3)
- This study revealed that the effects of urban renewal in alleviating urban disease exhibited heterogeneity. The relationship between urban renewal and urban disease features spatial interaction and phase-specific characteristics. Many regression models can be employed to investigate these issues. For example, future research can consider exploring this relationship using spatial autocorrelation models and threshold effect models.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CBER | The City Betterment and Ecological Restoration |
| UD | Urban Disease |
| PC | Population Congestion |
| RS | Resource Scarcity |
| AP | Air Pollution |
| RARQ | Renovation of Aged Residential Quarters |
| GC | Government Capacity |
| TA | Technological Advancement |
| HR | Human Resource |
| OP | Openness |
| ED | Economic Development |
| EC | Energy Consumption |
References
- Li, M.; Li, C.; Zhang, M. Exploring the spatial spillover effects of industrialization and urbanization factors on pollutants emissions in China’s Huang-Huai-Hai region. J. Clean. Prod. 2018, 195, 154–162. [Google Scholar] [CrossRef]
- Wu, G.; Miao, Z.; Shao, S.; Jiang, K.; Geng, Y.; Li, D.; Liu, H. Evaluating the construction efficiencies of urban wastewater transportation and treatment capacity: Evidence from 70 megacities in China. Resour. Conserv. Recy. 2018, 128, 373–381. [Google Scholar] [CrossRef]
- Wang, Y.; Li, X.; Kang, Y.; Chen, W.; Zhao, M.; Li, W. Analyzing the impact of urbanization quality on CO2 emissions: What can geographically weighted regression tell us? Renew. Sust. Energ. Rev. 2019, 104, 127–136. [Google Scholar] [CrossRef]
- Gasana, J.; Dillikar, D.; Mendy, A.; Forno, E.; Vieira, E.R. Motor vehicle air pollution and asthma in children: A meta-analysis. Environ. Res. 2012, 117, 36–45. [Google Scholar] [CrossRef]
- Shah, A.S.; Langrish, J.P.; Nair, H.; McAllister, D.A.; Hunter, A.L.; Donaldson, K.; Newby, D.E.; Mills, N.L. Global association of air pollution and heart failure: A systematic review and meta-analysis. Lancet 2013, 382, 1039–1048. [Google Scholar] [CrossRef]
- Yang, X.J. China’s rapid urbanization. Science 2013, 342, 310. [Google Scholar] [CrossRef]
- Guan, X.; Wei, H.; Lu, S.; Dai, Q.; Su, H. Assessment on the urbanization strategy in China: Achievements, challenges and reflections. Habit. Int. 2018, 71, 97–109. [Google Scholar] [CrossRef]
- Northam, R.M. Urban Geography; Wiley: Hoboken, NJ, USA, 1979. [Google Scholar]
- Wang, X.; Li, S. Progress and prospects of diagnostic analysis and risk prediction of urban problems based on multiple perspectives. Prog. Geogr. 2017, 36, 231–243. (In Chinese) [Google Scholar]
- Adams, D.; Hastings, E.M. Urban renewal in Hong Kong: Transition from development corporation to renewal authority. Land Use Policy 2001, 18, 245–258. [Google Scholar] [CrossRef]
- Lee, G.K.L.; Chan, E.H.W. The analytic hierarchy process (AHP) approach for assessment of urban renewal proposals. Soc. Indic. Res. 2008, 89, 155–168. [Google Scholar] [CrossRef]
- Ho, D.C.W.; Yau, Y.; Poon, S.W.; Liusman, E. Achieving sustainable urban renewal in Hong Kong: Strategy for dilapidation assessment of high rises. J. Urban Plan Dev. 2012, 138, 153–165. [Google Scholar] [CrossRef]
- Chan, E.H.W.; Yung, E.H.K. Is the development control legal framework conducive to a sustainable dense urban development in Hong Kong? Habitat Int. 2004, 28, 409–426. [Google Scholar] [CrossRef]
- Couch, C.; Dennemann, A. Urban regeneration and sustainable development in Britain: The example of the Liverpool Ropewalks Partnership. Cities 2000, 17, 137–147. [Google Scholar] [CrossRef]
- Grossman, G.M.; Krueger, A.B. Economic growth and the environment. Q. J. Econ. 1995, 110, 353–377. [Google Scholar] [CrossRef]
- Sun, B.; Fang, C.; Liao, X.; Guo, X.; Liu, Z. The relationship between urbanization and air pollution affected by intercity factor mobility: A case of the Yangtze River Delta region. Environ. Impact Asses. 2023, 100, 107092. [Google Scholar] [CrossRef]
- Wang, X.; Tian, G.; Yang, D.; Zhang, W.; Lu, D.; Liu, Z. Responses of PM2.5 pollution to urbanization in China. Energ. Policy 2018, 123, 602–610. [Google Scholar] [CrossRef]
- Martínez-Zarzoso, I.; Maruotti, A. The impact of urbanization on CO2 emissions: Evidence from developing countries. Ecol. Econ. 2011, 70, 1344–1353. [Google Scholar] [CrossRef]
- Wolman, A. The metabolism of cities. Sci. Am. 1965, 213, 178–193. [Google Scholar] [CrossRef]
- Du, M.; Antunes, J.; Wanke, P.; Chen, Z. Ecological efficiency assessment under the construction of low-carbon city: A perspective of green technology innovation. J. Environ. Plann. Man. 2022, 65, 1727–1752. [Google Scholar] [CrossRef]
- Zucaro, A.; Ripa, M.; Mellino, S.; Ascione, M.; Ulgiati, S. Urban resource use and environmental performance indicators. An application of decomposition analysis. Ecol. Indic. 2014, 47, 16–25. [Google Scholar] [CrossRef]
- Zhang, Y.; Xia, L.; Fath, B.D.; Yang, Z.; Yin, X.; Su, M.; Liu, G.; Li, Y. Development of a spatially explicit network model of urban metabolism and analysis of the distribution of ecological relationships: Case study of Beijing, China. J. Clean. Prod. 2016, 112, 4304–4317. [Google Scholar] [CrossRef]
- Fu, Y.; He, C.; Luo, L. Does the low-carbon city policy make a difference? Empirical evidence of the pilot scheme in China with DEA and PSM-DID. Ecol. Indic. 2021, 122, 107238. [Google Scholar] [CrossRef]
- Xie, G.; Chen, W.; Cao, S.; Lu, C.; Xiao, Y.; Zhang, C.; Li, N.; Wang, S. The outward extension of an ecological footprint in city expansion: The case of Beijing. Sustainability 2014, 6, 9371–9386. [Google Scholar] [CrossRef]
- Gao, Y.; Feng, Z.; Li, Y.; Li, S. Freshwater ecosystem service footprint model: A model to evaluate regional freshwater sustainable development—A case study in Beijing–Tianjin–Hebei, China. Ecol. Indic. 2014, 39, 1–9. [Google Scholar] [CrossRef]
- Burkhard, B.; Kroll, F.; Nedkov, S.; Müller, F. Mapping ecosystem service supply, demand and budgets. Ecol. Indic. 2012, 21, 17–29. [Google Scholar] [CrossRef]
- Zhao, C.; Wang, B. How does new-type urbanization affect air pollution? Empirical evidence based on spatial spillover effect and spatial Durbin model. Environ. Int. 2022, 165, 107304. [Google Scholar] [PubMed]
- Ewing, R.; Tian, G.; Lyons, T. Does compact development increase or reduce traffic congestion? Cities 2018, 72, 94–101. [Google Scholar] [CrossRef]
- Chow, A.H.F.; Santacreu, A.; Tsapakis, I.; Tanasaranond, G.; Cheng, T. Empirical assessment of urban traffic congestion. J. Adv. Transport. 2014, 48, 1000–1016. [Google Scholar]
- Levy, J.I.; Buonocore, J.J.; Stackelberg, K.V. Evaluation of the public health impacts of traffic congestion: A health risk assessment. Environ. Health 2010, 9, 65. [Google Scholar] [CrossRef]
- Xu, A.; Song, M.; Wu, Y.; Luo, Y.; Zhu, Y.; Qiu, K. Effects of new urbanization on China’s carbon emissions: A quasi-natural experiment based on the improved PSM-DID model. Technol. Forecast. Soc. 2024, 200, 123164. [Google Scholar] [CrossRef]
- Ryan, A.M.; Burgess Jr, J.F.; Dimick, J.B. Why we should not be indifferent to specification choices for difference-in-differences. Health. Serv. Res. 2015, 50, 1211–1235. [Google Scholar] [CrossRef]
- Xiao, R.; Tan, G.; Huang, B.; Li, J.; Luo, Y. Pathways to sustainable development: Regional integration and carbon emissions in China. Energy Rep. 2022, 8, 5137–5145. [Google Scholar] [CrossRef]
- Luo, C.; Qiang, W.; Lee, H.F. Does the low-carbon city pilot policy work in China? A company-level analysis based on the PSM-DID model. J. Environ. Manage 2023, 337, 117725. [Google Scholar] [CrossRef]
- Liu, H.; Liu, J.; Li, M.; Gou, P.; Cheng, Y. Assessing the evolution of PM2.5 and related health impacts resulting from air quality policies in China. Environ. Impact Assess. 2022, 93, 106727. [Google Scholar] [CrossRef]
- Yang, X.; Lin, S.; Li, Y.; He, M. Can high-speed rail reduce environmental pollution? Evidence from China. J. Clean. Prod. 2019, 239, 118135. [Google Scholar] [CrossRef]
- Fan, F.; Zhang, X. Transformation effect of resource-based cities based on PSM-DID model: An empirical analysis from China. Environ. Impact Asses. 2021, 91, 106648. [Google Scholar] [CrossRef]
- Zhou, A.; Wang, S.; Chen, B. Impact of new energy demonstration city policy on energy efficiency: Evidence from China. J. Clean. Prod. 2023, 422, 138560. [Google Scholar] [CrossRef]
- Huang, G.; Xu, D. The last mile matters: Impact of dockless bike-sharing services on traffic congestion. Transp. Res. Part D Transp. Environ. 2023, 121, 103836. [Google Scholar] [CrossRef]
- Guo, Y.; Tang, Z.; Guo, J. Could a smart city ameliorate urban traffic congestion? A quasi-natural experiment based on a smart city pilot program in China. Sustainability 2020, 12, 2291. [Google Scholar] [CrossRef]
- Yuan, C.; Jiang, H.; Chen, C. Differences in returns to cross-border and domestic mergers and acquisitions: Empirical evidence from China using PSM-DID. Financ. Res. Lett. 2023, 55, 103961. [Google Scholar] [CrossRef]
- Ye, M.; Liao, L.; Fu, T.; Lan, S. Do establishment of protected areas and implementation of regional policies both promote the forest NPP? Evidence from Wuyi Mountain in China based on PSM-DID. Glob. Ecol. Conserv. 2024, 55, e03210. [Google Scholar] [CrossRef]
- Heckman, J.J.; Ichimura, H.; Todd, P.E. Matching as an econometric evaluation estimator: Evidence from evaluating a job training programme. Rev. Econ. Stud. 1997, 64, 605–654. [Google Scholar] [CrossRef]
- Yu, Y.; Chen, X.; Zhang, N. Innovation and energy productivity: An empirical study of the innovative city pilot policy in China. Technol. Forecast. Soc. Change 2022, 176, 121430. [Google Scholar] [CrossRef]
- Xie, S.; Fan, P.; Wan, Y. Improvement and application of classical PSM-DID model. Stat. Res. 2021, 38, 146–160. [Google Scholar]
- Li, X.; Zhang, G.; Li, W.; Xie, J. Some issues in urban regeneration from industrial development viewpoint. Planners 2021, 2021, 34–40. (In Chinese) [Google Scholar]
- Chang, J.; Wang, W.; Liu, J. Industrial upgrading and its influence on green land use efficiency. Sci. Rep. 2023, 13, 2813. [Google Scholar] [CrossRef]
- Dai, M.; Zhang, H.; Luo, W. The theory and practice of urban development and transformation. With a discussion on Shenzhen’s developmental transformation. Urban Issues 2013, 2013, 84–88. (In Chinese) [Google Scholar]
- Banister, D.; Anderton, K.; Bonilla, D.; Givoni, M.; Schwanen, T. Transportation and the environment. Annu. Rev. Env. Resour. 2011, 36, 247–270. [Google Scholar] [CrossRef]
- Sun, C.; Luo, Y.; Yao, X. Transport infrastructure and urban air pollution. Empirical evidence from China. Econ. Res. 2019, 54, 136–151. (In Chinese) [Google Scholar]
- Zhao, J.; Zhu, Y. The influence of the change of residents’ consumption structure on environmental efficiency from the perspective of investment. Resour. Sci. 2021, 43, 1764–1777. (In Chinese) [Google Scholar]
- Chen, Z.; Ma, Y. A study on the influence of urban renewal on residents’ well-being in China. Based on genetic algorithm projection pursuit and panel spatial quantile model. Manag. Rev. 2022, 34, 43–53. (In Chinese) [Google Scholar]
- Hammer, M.S.; Van Donkelaar, A.; Li, C.; Lyapustin, A.; Sayer, A.M.; Hsu, N.C.; Levy, R.C.; Garay, M.J.; Kalashnikova, O.V.; Kahn, R.A.; et al. Global estimates and long-term trends of fine particulate matter concentrations (1998–2018). Environ. Sci. Technol. 2020, 54, 7879–7890. [Google Scholar] [CrossRef] [PubMed]
- Hodge, D.C. Urban congestion: Reshaping urban life. Urban Geogr. 1992, 13, 577–588. [Google Scholar] [CrossRef]
- Furnham, A.; McClelland, A. The allocation of scarce resources: Social housing. Soc. Behav. Personal. 2004, 32, 45–53. [Google Scholar] [CrossRef]
- Li, J.; Lu, M.; Lu, T. Constructing compact cities: How urban regeneration can enhance growth and relieve congestion. Econ. Model. 2022, 113, 105828. [Google Scholar] [CrossRef]
- Airgood-Obrycki, W.; McCue, D. The Housing Shortage Is Still Out There. Hous. Policy Debate 2024, 2024, 1–5. [Google Scholar] [CrossRef]
- Mayer, H. Air pollution in cities. Atmos. Environ. 1999, 33, 4029–4037. [Google Scholar] [CrossRef]
- Gan, T.; Liang, W.; Yang, H.; Liao, X. The effect of Economic Development on haze pollution (PM2.5) based on a spatial perspective: Urbanization as a mediating variable. J. Clean. Prod. 2020, 266, 121880. [Google Scholar] [CrossRef]
- Jiang, L.; Zhou, H.; Bai, L.; Zhou, P. Does foreign direct investment drive environmental degradation in China? An empirical study based on air quality index from a spatial perspective. J. Clean. Prod. 2018, 176, 864–872. [Google Scholar] [CrossRef]
- Liu, Q.; Wang, S.; Zhang, W.; Li, J.; Dong, G. The effect of natural and anthropogenic factors on PM2.5: Empirical evidence from Chinese cities with different income levels. Sci. Total Environ. 2019, 653, 157–167. [Google Scholar] [CrossRef]
- Feng, Y.; Li, G. Interaction between urbanization and eco-environment in the Tibetan Plateau. J. Geogr. Sci. 2021, 31, 298–324. [Google Scholar] [CrossRef]
- Yu, B. Ecological effects of new-type urbanization in China. Renew. Sust. Energ. Rev. 2021, 135, 110239. [Google Scholar] [CrossRef]
- Yang, L.; Sun, Z.C. The development of western new-type urbanization level evaluation based on entropy method. Econ. Probl. 2015, 3, 115–119. (In Chinese) [Google Scholar]
- Xu, Y. Generalized synthetic control method: Causal inference with interactive fixed effects models. Polit. Anal. 2017, 25, 57–76. [Google Scholar] [CrossRef]
- Wang, J.; Ran, M.; Li, Y.; Zhan, H. Is venture capital a catalyst for innovative entrepreneurship in China? Empirical analysis based on the PSM-DID method. Manag. Decis. Econ. 2022, 43, 1039–1058. [Google Scholar] [CrossRef]
- Kovács, P.; Petres, T.; Tóth, L. A new measure of multicollinearity in linear regression models. Int. Stat. Rev. 2005, 73, 405–412. [Google Scholar] [CrossRef]
- Hausman, J.A. Specification tests in econometrics. Econome. J. Econ. Soc. 1978, 46, 1251–1271. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, S.; Xing, J.; Wang, Y.; Chen, W.; Ding, D.; Wu, Y.; Wang, S.; Duan, L.; Hao, J. Progress of air pollution control in China and its challenges and opportunities in the ecological civilization era. Engineering 2020, 6, 1423–1431. [Google Scholar] [CrossRef]
- Mehdipanah, R.; Marra, G.; Melis, G.; Gelormino, E. Urban renewal, gentrification and health equity: A realist perspective. Eur. J. Public Health 2018, 28, 243–248. [Google Scholar] [CrossRef]
- Anelli, D.; Morano, P.; Tajani, F.; Sabatelli, E. Impacts of Urban Decay on the Residential Property Market: An Application to the City of Rome (Italy). In Proceedings of the International Conference on Computational Science and Its Applications, Hanoi, Vietnam, 1–4 July 2024; pp. 36–48. [Google Scholar]
- Maculan, L.S.; Dal Moro, L. Strategies for inclusive urban renewal. In Sustainable Cities and Communities; Springer: Berlin/Heidelberg, Germany, 2020; pp. 662–672. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Std. Dev. | Mean | Min | Max | Count |
|---|---|---|---|---|---|
| PC | 0.643 | 8.819 | 0.989 | 10 | 3135 |
| RS | 0.606 | 4.245 | 1.686 | 8.619 | 3135 |
| AP | 0.510 | 1.481 | 0.340 | 7.265 | 3135 |
| lnGC | 1.054 | 13.999 | 10.101 | 18.358 | 3135 |
| lnTA | 1.438 | 4.881 | 1.772 | 9.409 | 3135 |
| lnHR | 1.329 | 10.636 | 4.187 | 14.214 | 3135 |
| lnOP | 3.244 | 9.053 | 5.726 | 33.504 | 3135 |
| lnED | 0.552 | 11.028 | 8.327 | 15.675 | 3135 |
| lnEC | 0.966 | 6.382 | 1.535 | 16.323 | 3135 |
| Variables | Specific Indicators | Weighting Values |
|---|---|---|
| PC | Per capita residential land area | 0.897 |
| Per capita urban road surface area | 0.103 | |
| RS | Per capita electricity consumption | 0.033 |
| The number of doctors per thousand individuals | 0.092 | |
| The student-to-teacher ratio in secondary education | 0.158 | |
| The student-to-teacher ratio in primary education | 0.717 | |
| AP | PM2.5 concentrations | 0.306 |
| Sulfur dioxide emissions | 0.167 | |
| Particulate matter emissions | 0.527 |
| Year | 2012 | 2013 | 2014 | 2015 | 2016 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Status | Bias (%) | RP | Bias (%) | RP | Bias (%) | RP | Bias (%) | RP | Bias (%) | RP |
| lnGC | Unmatching | 56.8 | 97.1 | 61.3 | 90.6 | 58.0 | 99.1 | 61.1 | 93.8 | 62.7 | 95.4 |
| Matching | 1.6 | 5.8 | 0.5 | 3.8 | 2.9 | ||||||
| lnTA | Unmatching | 56.9 | 97.5 | 60.1 | 87.4 | 63.9 | 98.6 | 61.6 | 98.5 | 61.7 | 92.4 |
| Matching | 1.4 | 7.6 | −0.9 | 0.9 | 4.7 | ||||||
| lnHR | Unmatching | 77.1 | 93.6 | 76.9 | 90.6 | 78.3 | 92.4 | 77.5 | 93.6 | 73.5 | 92.1 |
| Matching | −5.0 | −7.2 | −5.9 | −5.0 | −5.8 | ||||||
| lnOP | Unmatching | 11.2 | 20.8 | 17.2 | 46.3 | 25.7 | 62.0 | 29.9 | 71.4 | 32.5 | 74.7 |
| Matching | −8.9 | −9.3 | −9.8 | −8.5 | −8.2 | ||||||
| lnED | Unmatching | 57.7 | 72.5 | 65.4 | 85.2 | 62.0 | 78.8 | 68.4 | 88.7 | 49.1 | 96.2 |
| Matching | 15.9 | 9.7 | 13.1 | 7.7 | −1.9 | ||||||
| lnEC | Unmatching | 31.6 | 23.8 | 26.9 | 16.0 | 21.6 | 2.0 | 25.8 | 23.2 | 22.4 | 10.5 |
| Matching | 24.1 | 22.6 | 21.2 | 19.8 | 20.0 |
| Variables | VIF | 1/VIF |
|---|---|---|
| lnGC | 3.74 | 0.2675 |
| lnTA | 2.43 | 0.4122 |
| lnHR | 2.57 | 0.3898 |
| lnOP | 1.61 | 0.6211 |
| lnED | 2.00 | 0.5005 |
| lnEC | 1.15 | 0.8668 |
| TREAT×TIME | 1.12 | 0.8923 |
| Mean VIF | 2.09 |
| Dependent Variable | UD | |||
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| CBER pilot scheme | −0.207 *** (0.020) | −0.253 *** (0.017) | −0.045 ** (0.020) | −0.041 ** (0.020) |
| Constant | 4.914 *** (0.011) | 4.927 *** (0.007) | 4.999 *** (0.017) | 3.715 *** (0.533) |
| City fixed effects | No | Yes | Yes | Yes |
| Time fixed effects | No | No | Yes | Yes |
| Control variables | No | No | No | Yes |
| R2 | 0.0831 | 0.1839 | 0.4025 | 0.4165 |
| Hausman test | 16.51 *** | 22.15 *** | 21.49 *** |
| Dependent Variable | PC | RS | AP |
|---|---|---|---|
| (1) | (2) | (3) | |
| CBER pilot scheme | −0.057 * (0.032) | −0.065 ** (0.034) | −0.010 (0.019) |
| Constant | 6.835 *** (0.491) | 5.949 *** (0.523) | 0.951 *** (0.298) |
| City fixed effects | Yes | Yes | Yes |
| Time fixed effects | Yes | Yes | Yes |
| Control variables | Yes | Yes | Yes |
| R2 | 0.0593 | 0.0344 | 0.6886 |
| Dependent Variable | UD | |||
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| CBER pilot scheme | −0.043 (0.035) | −0.011 (0.023) | −0.045 (0.023) | −0.018 (0.035) |
| Constant | 3.730 *** (0.534) | 3.717 *** (0.534) | 3.693 *** (0.533) | 3.708 *** (0.534) |
| City fixed effects | Yes | Yes | Yes | Yes |
| Time fixed effects | Yes | Yes | Yes | Yes |
| Control variables | Yes | Yes | Yes | Yes |
| R2 | 0.4151 | 0.4143 | 0.4165 | 0.4144 |
| Dependent Variable | UD | ||
|---|---|---|---|
| (1) | (2) | (3) | |
| CBER pilot scheme | −0.042 * (0.022) | −0.039 * (0.020) | −0.039 * (0.021) |
| RARQ scheme | −0.024 (0.031) | ||
| Constant | 4.126 *** (0.612) | 3.772 *** (0.538) | 3.712 *** (0.533) |
| City fixed effects | Yes | Yes | Yes |
| Time fixed effects | Yes | Yes | Yes |
| Control variables | Yes | Yes | Yes |
| R2 | 0.3449 | 0.4169 | 0.4146 |
| Dependent Variable | UD | |||
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| CBER pilot scheme | −0.060 ** (0.028) | −0.049 ** (0.024) | −0.055 ** (0.023) | −0.037 * (0.022) |
| Constant | 4.144 *** (0.886) | 4.456 *** (0.731) | 3.647 *** (0.705) | 3.660 *** (0.618) |
| City fixed effects | Yes | Yes | Yes | Yes |
| Time fixed effects | Yes | Yes | Yes | Yes |
| Control variables | Yes | Yes | Yes | Yes |
| R2 | 0.1244 | 0.2955 | 0.3620 | 0.4063 |
| Dependent Variable | UD | ||
|---|---|---|---|
| (1) | (2) | (3) | |
| CBER pilot scheme | −0.026 * (0.025) | −0.156 *** (0.035) | 0.112 (0.041) |
| Constant | 5.006 *** (0.768) | 3.137 *** (0.905) | 4.304 *** (0.853) |
| City fixed effects | Yes | Yes | Yes |
| Time fixed effects | Yes | Yes | Yes |
| Control variables | Yes | Yes | Yes |
| R2 | 0.5980 | 0.5062 | 0.4386 |
| Dependent Variable | Indust. Struc. | UD | Infras. Dev. | UD | Consu. Upg. | UD |
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | |
| CBER pilot scheme | 0.048 * (0.029) | −0.045 *** (0.017) | 0.037 * (0.028) | −0.046 *** (0.017) | 0.013 * (0.009) | −0.044 *** (0.017) |
| Indust. Struc. | −0.021 ** (0.011) | |||||
| Infras. Dev. | −0.049 *** (0.022) | |||||
| Consu. Upg. | −0.032 *** (0.011) | |||||
| Constant | 3.847 *** (0.453) | 4.660 *** (0.263) | 1.926 *** (0.438) | 4.675 *** (0.260) | 6.846 *** (0.449) | 4.798 *** (0.270) |
| City fixed effects | Yes | Yes | Yes | Yes | Yes | Yes |
| Time fixed effects | Yes | Yes | Yes | Yes | Yes | Yes |
| Control variables | Yes | Yes | Yes | Yes | Yes | Yes |
| R2 | 0.4194 | 0.3474 | 0.2456 | 0.3512 | 0.3433 | 0.3485 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, T.; Yan, H.; Guo, Z. Does Urban Renewal Mitigate the Disease of Cities? An Empirical Study Based on a PSM-DID Model. Sustainability 2025, 17, 5214. https://doi.org/10.3390/su17115214
Liu T, Yan H, Guo Z. Does Urban Renewal Mitigate the Disease of Cities? An Empirical Study Based on a PSM-DID Model. Sustainability. 2025; 17(11):5214. https://doi.org/10.3390/su17115214
Chicago/Turabian StyleLiu, Tianyi, Hang Yan, and Zeyuan Guo. 2025. "Does Urban Renewal Mitigate the Disease of Cities? An Empirical Study Based on a PSM-DID Model" Sustainability 17, no. 11: 5214. https://doi.org/10.3390/su17115214
APA StyleLiu, T., Yan, H., & Guo, Z. (2025). Does Urban Renewal Mitigate the Disease of Cities? An Empirical Study Based on a PSM-DID Model. Sustainability, 17(11), 5214. https://doi.org/10.3390/su17115214