
The Relationship between Physical Fitness and Cognitive Functions in Older People: A Systematic Review

 , ,
, ,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Search Strategy
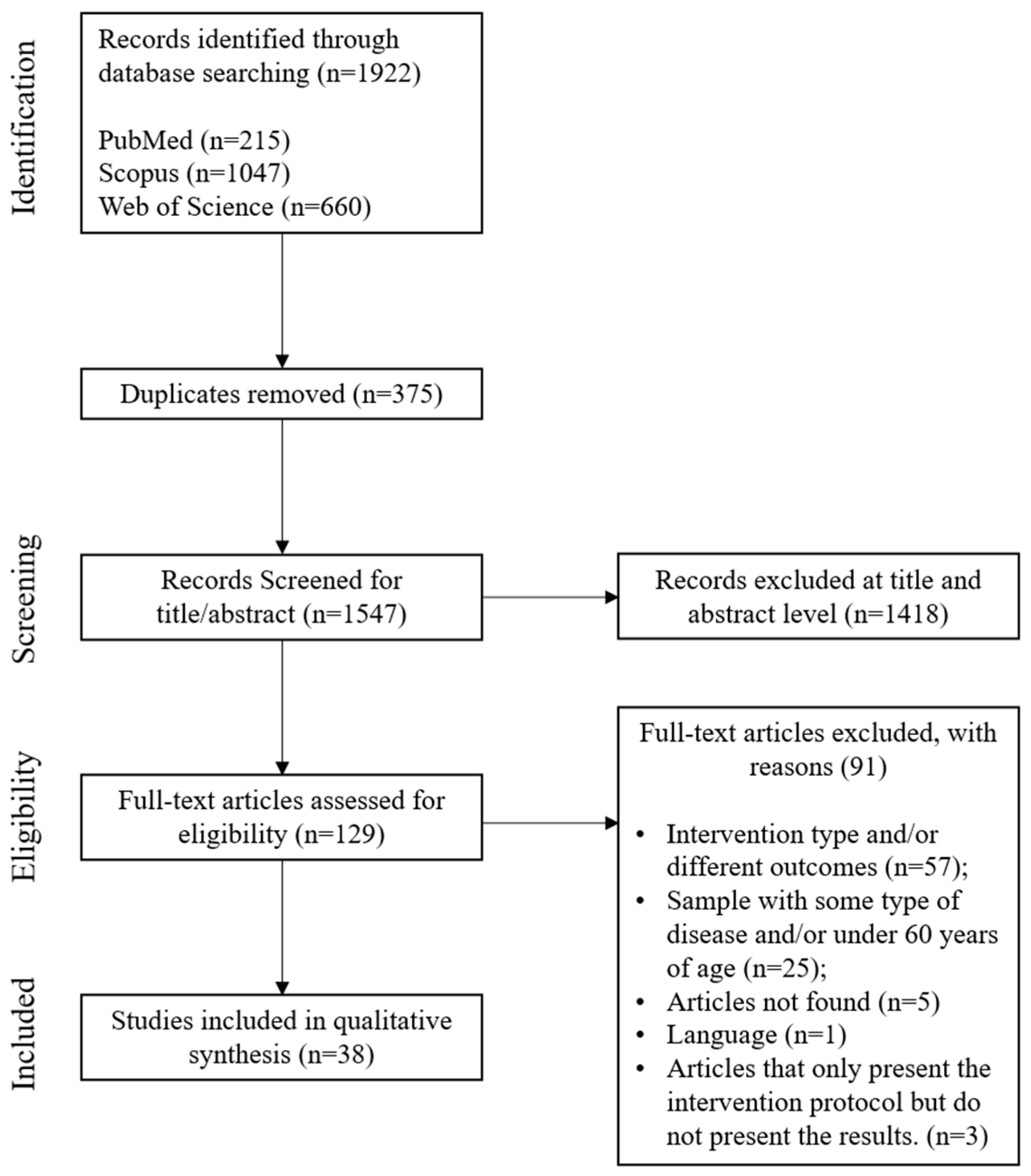
2.3. Screening Strategy and Study Selection
2.4. Data Extraction and Harmonisation
2.5. Study Quality and Risk of Bias
3. Results
3.1. Study Quality and Risk of Bias
3.2. Intervention Characteristics
3.3. Main Results
4. Discussion
4.1. Cognitive Functions and Subdomains
4.2. Intervention Program Types
4.3. Length of Interventions, Frequency, and Time of Sessions
4.4. Clinical Implications
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mana, J.; Bezdicek, O. Cognition in successful aging: Systematic review and future directions. Clin. Gerontol. 2022, 45, 477–485. [Google Scholar] [CrossRef]
- Salthouse, T.A. Trajectories of normal cognitive aging. Psychol. Aging 2019, 34, 17. [Google Scholar] [CrossRef]
- Yiengprugsawan, V.S.; Browning, C.J. Non-communicable diseases and cognitive impairment: Pathways and shared Behavioral risk factors among older Chinese. Front. Public Health 2019, 7, 296. [Google Scholar] [CrossRef]
- Hadley, G.; Zhang, J.; Harris-Skillman, E.; Alexopoulou, Z.; DeLuca, G.C.; Pendlebury, S.T. Cognitive decline and diabetes: A systematic review of the neuropathological correlates accounting for cognition at death. J. Neurol. Neurosurg. Psychiatry 2022, 93, 246–253. [Google Scholar] [CrossRef]
- Hayat, S.A.; Luben, R.; Dalzell, N.; Moore, S.; Hogervorst, E.; Matthews, F.E.; Wareham, N.; Brayne, C.; Khaw, K.-T. Understanding the relationship between cognition and death: A within cohort examination of cognitive measures and mortality. Eur. J. Epidemiol. 2018, 33, 1049–1062. [Google Scholar] [CrossRef]
- de Asteasu, M.L.S.; Martinez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, A.; Izquierdo, M. Role of physical exercise on cognitive function in healthy older adults: A systematic review of randomized clinical trials. Ageing Res. Rev. 2017, 37, 117–134. [Google Scholar] [CrossRef] [PubMed]
- Gates, N.; Singh, M.A.F.; Sachdev, P.S.; Valenzuela, M. The effect of exercise training on cognitive function in older adults with mild cognitive impairment: A meta-analysis of randomized controlled trials. Am. J. Geriatr. Psychiatry 2013, 21, 1086–1097. [Google Scholar] [CrossRef]
- Power, J.D.; Schlaggar, B.L. Neural plasticity across the lifespan. Wiley Interdiscip. Rev. Dev. Biol. 2017, 6, e216. [Google Scholar] [CrossRef]
- Hötting, K.; Röder, B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci. Biobehav. Rev. 2013, 37, 2243–2257. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, M.; Merchant, R.; Morley, J.; Anker, S.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.; Cesari, M. International exercise recommendations in older adults (ICFSR): Expert consensus guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef]
- Firth, J.; Stubbs, B.; Vancampfort, D.; Schuch, F.; Lagopoulos, J.; Rosenbaum, S.; Ward, P.B. Effect of aerobic exercise on hippocampal volume in humans: A systematic review and meta-analysis. Neuroimage 2018, 166, 230–238. [Google Scholar] [CrossRef]
- Young, J.; Angevaren, M.; Rusted, J.; Tabet, N. Aerobic exercise to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst. Rev. 2015, 4, CD005381. [Google Scholar] [CrossRef] [PubMed]
- Cassilhas, R.C.; Tufik, S.; de Mello, M.T. Physical exercise, neuroplasticity, spatial learning and memory. Cell. Mol. Life Sci. 2016, 73, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.X.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 3–25. [Google Scholar] [CrossRef] [PubMed]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- Smith, P.J.; Blumenthal, J.A.; Hoffman, B.M.; Cooper, H.; Strauman, T.A.; Welsh-Bohmer, K.; Browndyke, J.N.; Sherwood, A. Aerobic exercise and neurocognitive performance: A meta-analytic review of randomized controlled trials. Psychosom. Med. 2010, 72, 239. [Google Scholar] [CrossRef]
- Hortobágyi, T.; Vetrovsky, T.; Balbim, G.M.; Silva, N.C.B.S.; Manca, A.; Deriu, F.; Kolmos, M.; Kruuse, C.; Liu-Ambrose, T.; Radák, Z. The impact of aerobic and resistance training intensity on markers of neuroplasticity in health and disease. Ageing Res. Rev. 2022, 80, 101698. [Google Scholar] [CrossRef]
- Numakawa, T.; Adachi, N.; Richards, M.; Chiba, S.; Kunugi, H. Brain-derived neurotrophic factor and glucocorticoids: Reciprocal influence on the central nervous system. Neuroscience 2013, 239, 157–172. [Google Scholar] [CrossRef]
- Walsh, J.J.; Tschakovsky, M.E. Exercise and circulating BDNF: Mechanisms of release and implications for the design of exercise interventions. Appl. Physiol. Nutr. Metab. 2018, 43, 1095–1104. [Google Scholar] [CrossRef]
- Raichlen, D.A.; Bharadwaj, P.K.; Nguyen, L.A.; Franchetti, M.K.; Zigman, E.K.; Solorio, A.R.; Alexander, G.E. Effects of simultaneous cognitive and aerobic exercise training on dual-task walking performance in healthy older adults: Results from a pilot randomized controlled trial. BMC Geriatr. 2020, 20, 83. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Peng, X.; Xiang, W.; Han, J.; Li, K. The effect of resistance training on cognitive function in the older adults: A systematic review of randomized clinical trials. Aging Clin. Exp. Res. 2018, 30, 1259–1273. [Google Scholar] [CrossRef] [PubMed]
- Norouzi, E.; Vaezmosavi, M.; Gerber, M.; Pühse, U.; Brand, S. Dual-task training on cognition and resistance training improved both balance and working memory in older people. Physician Sportsmed. 2019, 47, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Gregory, M.A.; Gill, D.P.; Shellington, E.M.; Liu-Ambrose, T.; Shigematsu, R.; Zou, G.; Shoemaker, K.; Owen, A.M.; Hachinski, V.; Stuckey, M. Group-based exercise and cognitive-physical training in older adults with self-reported cognitive complaints: The Multiple-Modality, Mind-Motor (M4) study protocol. BMC Geriatr. 2016, 16, 17. [Google Scholar] [CrossRef] [PubMed]
- Gavelin, H.M.; Dong, C.; Minkov, R.; Bahar-Fuchs, A.; Ellis, K.A.; Lautenschlager, N.T.; Mellow, M.L.; Wade, A.T.; Smith, A.E.; Finke, C. Combined physical and cognitive training for older adults with and without cognitive impairment: A systematic review and network meta-analysis of randomized controlled trials. Ageing Res. Rev. 2021, 66, 101232. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 105906. [Google Scholar] [CrossRef] [PubMed]
- Adriani, D.; Imran, Y.; Mawi, M.; Amani, P.; Ilyas, E.I.I. Effect of Brain Gym (R) exercises on cognitive function and brain-derived neurotrophic factor plasma level in elderly: A randomized controlled trial. Universa Med. 2020, 39, 34–41. [Google Scholar] [CrossRef]
- Baniqued, P.L.; Gallen, C.L.; Voss, M.W.; Burzynska, A.Z.; Wong, C.N.; Cooke, G.E.; Duffy, K.; Fanning, J.; Ehlers, D.K.; Salerno, E.A.; et al. Brain Network Modularity Predicts Exercise-Related Executive Function Gains in Older Adults. Front. Aging Neurosci. 2018, 9, 426. [Google Scholar] [CrossRef]
- Belleville, S.; Cuesta, M.; Bieler-Aeschlimann, M.; Giacomino, K.; Widmer, A.; Hager, A.G.M.; Perez-Marcos, D.; Cardin, S.; Boller, B.; Bier, N.; et al. Pre-frail older adults show improved cognition with StayFitLonger computerized home-based training: A randomized controlled trial. Geroscience 2023, 45, 811–822. [Google Scholar] [CrossRef]
- Callow, D.D.; Won, J.; Pena, G.S.; Jordan, L.S.; Arnold-Nedimala, N.A.; Kommula, Y.; Nielson, K.A.; Smith, J.C. Exercise Training-Related Changes in Cortical Gray Matter Diffusivity and Cognitive Function in Mild Cognitive Impairment and Healthy Older Adults. Front. Aging Neurosci. 2021, 13, 645258. [Google Scholar] [CrossRef]
- Carta, M.G.; Cossu, G.; Pintus, E.; Zaccheddu, R.; Callia, O.; Conti, G.; Pintus, M.; Aviles Gonzalez, C.I.; Massidda, M.V.; Mura, G.; et al. Moderate Exercise Improves Cognitive Function in Healthy Elderly People: Results of a Randomized Controlled Trial. Clin. Pract. Epidemiol. Ment. Health 2021, 17, 75–80. [Google Scholar] [CrossRef]
- Castano, L.A.A.; de Lima, V.C.; Barbieri, J.F.; de Lucena, E.G.P.; Gaspari, A.F.; Arai, H.; Teixeira, C.V.L.; Coelho, H.J.; Uchida, M.C. Resistance Training Combined with Cognitive Training Increases Brain Derived Neurotrophic Factor and Improves Cognitive Function in Healthy Older Adults. Front. Psychol. 2022, 13, 870561. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.P.; Wu, C.W.W.; Lin, L.J.; Lai, C.H.; Wu, H.Y.; Hsu, A.L.; Chen, C.N. Cognitive Load of Exercise Influences Cognition and Neuroplasticity of Healthy Elderly: An Exploratory Investigation. J. Med. Biol. Eng. 2020, 40, 391–399. [Google Scholar] [CrossRef]
- Douka, S.; Zilidou, V.I.; Lilou, O.; Tsolaki, M. Greek Traditional Dances: A Way to Support Intellectual, Psychological, and Motor Functions in Senior Citizens at Risk of Neurodegeneration. Front. Aging Neurosci. 2019, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, N.; Braun, C.; Kibele, A. Instability Resistance Training improves Working Memory, Processing Speed and Response Inhibition in Healthy Older Adults: A Double-Blinded Randomised Controlled Trial. Sci. Rep. 2020, 10, 2506. [Google Scholar] [CrossRef] [PubMed]
- Esmail, A.; Vrinceanu, T.; Lussier, M.; Predovan, D.; Berryman, N.; Houle, J.; Karelis, A.; Grenier, S.; Vu, T.T.M.; Villalpando, J.M.; et al. Effects of Dance/Movement Training vs. Aerobic Exercise Training on cognition, physical fitness and quality of life in older adults: A randomized controlled trial. J. Bodyw. Mov. Ther. 2020, 24, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, É.R.; Smailagic, A.; Ihle, A.; Marques, A.; Gouveia, B.R.; Cameirão, M.; Sousa, H.; Kliegel, M.; Siewiorek, D. The Efficacy of a Multicomponent Functional Fitness Program Based on Exergaming on Cognitive Functioning of Healthy Older Adults: A Randomized Controlled Trial. J. Aging Phys. Act. 2020, 29, 586–594. [Google Scholar] [CrossRef]
- Guadagni, V.; Drogos, L.L.; Tyndall, A.V.; Davenport, M.H.; Anderson, T.J.; Eskes, G.A.; Longman, R.S.; Hill, M.D.; Hogan, D.B.; Poulin, M.J. Aerobic exercise improves cognition and cerebrovascular regulation in older adults. Neurology 2020, 94, e2245–e2257. [Google Scholar] [CrossRef]
- Inoue, T.; Kobayashi, Y.; Mori, N.; Sakagawa, M.; Xiao, J.Z.; Moritani, T.; Sakane, N.; Nagai, N. Effect of combined bifidobacteria supplementation and resistance training on cognitive function, body composition and bowel habits of healthy elderly subjects. Benef. Microbes 2018, 9, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Jardim, N.Y.V.; Bento-Torres, N.V.O.; Costa, V.O.; Carvalho, J.P.R.; Pontes, H.T.S.; Tomás, A.M.; Sosthenes, M.C.K.; Erickson, K.I.; Bento-Torres, J.; Diniz, C.W.P. Dual-Task Exercise to Improve Cognition and Functional Capacity of Healthy Older Adults. Front. Aging Neurosci. 2021, 13, 589299. [Google Scholar] [CrossRef]
- Ji, Z.; Feng, T.; Wang, H. The Effects of 12-Week Physical Exercise Tapping High-level Cognitive Functions. Adv. Cogn. Psychol. 2020, 16, 59–66. [Google Scholar] [CrossRef]
- Ji, L.; Pearlson, G.D.; Zhang, X.; Steffens, D.C.; Ji, X.; Guo, H.; Wang, L. Physical exercise increases involvement of motor networks as a compensatory mechanism during a cognitively challenging task. Int. J. Geriatr. Psychiatry 2018, 33, 1153–1159. [Google Scholar] [CrossRef]
- Kujach, S.; Chroboczek, M.; Jaworska, J.; Sawicka, A.; Smaruj, M.; Winklewski, P.; Laskowski, R. Judo training program improves brain and muscle function and elevates the peripheral BDNF concentration among the elderly. Sci. Rep. 2022, 12, 13900. [Google Scholar] [CrossRef] [PubMed]
- Kujawski, S.; Kujawska, A.; Kozakiewicz, M.; Jakovljevic, D.G.; Stankiewicz, B.; Newton, J.L.; Kędziora-Kornatowska, K.; Zalewski, P. Effects of Sitting Callisthenic Balance and Resistance Exercise Programs on Cognitive Function in Older Participants. Int. J. Environ. Res. Public Health 2022, 19, 14925. [Google Scholar] [CrossRef]
- Ladawan, S.; Sungkamanee, S.; Maharan, S.; Amput, P.; Srithawong, A.; Burtscher, M. Effects of a 4-movement Qigong exercise on cognitive function and physical performance in elderly women. J. Phys. Educ. Sport. 2022, 22, 495–502. [Google Scholar] [CrossRef]
- Liao, Y.Y.; Chen, I.H.; Hsu, W.C.; Tseng, H.Y.; Wang, R.Y. Effect of exergaming versus combined exercise on cognitive function and brain activation in frail older adults: A randomised controlled trial. Ann. Phys. Rehabil. Med. 2021, 64, 101492. [Google Scholar] [CrossRef] [PubMed]
- Macaulay, T.R.; Pa, J.; Kutch, J.J.; Lane, C.J.; Duncan, D.; Yan, L.; Schroeder, E.T. 12 weeks of strength training improves fluid cognition in older adults: A nonrandomized pilot trial. PLoS ONE 2021, 16, e0255018. [Google Scholar] [CrossRef]
- Matura, S.; Fleckenstein, J.; Deichmann, R.; Engeroff, T.; Füzéki, E.; Hattingen, E.; Hellweg, R.; Lienerth, B.; Pilatus, U.; Schwarz, S. Effects of aerobic exercise on brain metabolism and grey matter volume in older adults: Results of the randomised controlled SMART trial. Transl. Psychiatry 2017, 7, e1172. [Google Scholar] [CrossRef] [PubMed]
- Merchant, R.A.; Tsoi, C.T.; Tan, W.M.; Lau, W.; Sandrasageran, S.; Arai, H. Community-Based Peer-Led Intervention for Healthy Ageing and Evaluation of the ‘HAPPY’ Program. J. Nutr. Health Aging 2021, 25, 520–527. [Google Scholar] [CrossRef]
- Miyazaki, A.; Okuyama, T.; Mori, H.; Sato, K.; Kumamoto, K.; Hiyama, A. Effects of Two Short-Term Aerobic Exercises on Cognitive Function in Healthy Older Adults during COVID-19 Confinement in Japan: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 6202. [Google Scholar] [CrossRef] [PubMed]
- Morita, E.; Yokoyama, H.; Imai, D.; Takeda, R.; Ota, A.; Kawai, E.; Suzuki, Y.; Okazaki, K. Effects of 2-Year Cognitive⁻Motor Dual-Task Training on Cognitive Function and Motor Ability in Healthy Elderly People: A Pilot Study. Brain Sci. 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Muller, P.; Rehfeld, K.; Schmicker, M.; Hokelmann, A.; Dordevic, M.; Lessmann, V.; Brigadski, T.; Kaufmann, J.; Muller, N.G. Evolution of Neuroplasticity in Response to Physical Activity in Old Age: The Case for Dancing. Front. Aging Neurosci. 2017, 9, 56. [Google Scholar] [CrossRef]
- Mundada, P.H.; Dadgal, R.M. Comparison of Dual Task Training Versus Aerobics Training in Improving Cognition in Healthy Elderly Population. Cureus J. Med. Sci. 2022, 14, e29027. [Google Scholar] [CrossRef] [PubMed]
- Murata, S.; Ono, R.; Yasuda, H.; Tanemura, R.; Kido, Y.; Kowa, H. Effect of a Combined Exercise and Cognitive Activity Intervention on Cognitive Function in Community-dwelling Older Adults: A Pilot Randomized Controlled Trial. Phys. Ther. Res. 2021, 24, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Ordnung, M.; Hoff, M.; Kaminski, E.; Villringer, A.; Ragert, P. No Overt Effects of a 6-Week Exergame Training on Sensorimotor and Cognitive Function in Older Adults. A Preliminary Investigation. Front. Hum. Neurosci. 2017, 11, 160. [Google Scholar] [CrossRef]
- Pellegrini-Laplagne, M.; Dupuy, O.; Sosner, P.; Bosquet, L. Effect of simultaneous exercise and cognitive training on executive functions, baroreflex sensitivity, and pre-frontal cortex oxygenation in healthy older adults: A pilot study. Geroscience 2023, 45, 119–140. [Google Scholar] [CrossRef]
- Riegle van West, K.; Stinear, C.; Buck, R. The Effects of Poi on Physical and Cognitive Function in Healthy Older Adults. J. Aging Phys. Act. 2018, 27, 44–52. [Google Scholar] [CrossRef]
- Sexton, C.E.; Betts, J.F.; Dennis, A.; Doherty, A.; Leeson, P.; Holloway, C.; Dall’Armellina, E.; Winkler, A.M.; Demnitz, N.; Wassenaar, T.; et al. The effects of an aerobic training intervention on cognition, grey matter volumes and white matter microstructure. Physiol. Behav. 2020, 223, 112923. [Google Scholar] [CrossRef]
- Shake, M.C.; Crandall, K.J.; Mathews, R.P.; Falls, D.G.; Dispennette, A.K. Efficacy of Bingocize®: A game-centered mobile application to improve physical and cognitive performance in older adults. Games Health J. 2018, 7, 253–261. [Google Scholar] [CrossRef]
- Tsai, C.L.; Pan, C.Y.; Chen, F.C.; Tseng, Y.T. Open- and Closed-Skill Exercise Interventions Produce Different Neurocognitive Effects on Executive Functions in the Elderly: A 6-Month Randomized, Controlled Trial. Front. Aging Neurosci. 2017, 9, 294. [Google Scholar] [CrossRef]
- Welford, P.; Östh, J.; Hoy, S.; Rossell, S.L.; Pascoe, M.; Diwan, V.; Hallgren, M. Effects of Yoga and Aerobic Exercise on Verbal Fluency in Physically Inactive Older Adults: Randomized Controlled Trial (FitForAge). Clin. Interv. Aging 2023, 18, 533–545. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.; Isoda, H.; Okura, T. Evaluation of beneficial effect of a dual-task exercise based on Japanese transitional games in older adults: A pilot study. Aging (Albany NY) 2020, 12, 18957–18969. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Zhao, C.; Li, Y.; Zhao, M.; Wang, L.; Guo, J.; Zhang, L.; Sun, Y.; Ye, X.; Zhu, W. The Effects of Active Video Game Exercise Based on Self-Determination Theory on Physical Fitness and Cognitive Function in Older Adults. J. Clin. Med. 2022, 11, 3984. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. Quality Assessment Tool for Quantitative Studies Dictionary: The Effective Public Health Practice Project (EPHPP); McMaster University: Hamilton, ON, Canada, 2008. [Google Scholar]
- Hyodo, K.; Suwabe, K.; Yamaguchi, D.; Soya, H.; Arao, T. Comparison between the Effects of Continuous and Intermittent Light-Intensity Aerobic Dance Exercise on Mood and Executive Functions in Older Adults. Front. Aging Neurosci. 2021, 13, 723243. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Hillman, C.H.; Kramer, A.F. Physical activity, brain, and cognition. Curr. Opin. Behav. Sci. 2015, 4, 27–32. [Google Scholar] [CrossRef]
- Watson, N.; Rosano, C.; Boudreau, R.; Simonsick, E.; Ferrucci, L.; Sutton-Tyrrell, K.; Hardy, S.; Atkinson, H.; Yaffe, K.; Satterfield, S. Executive function, memory, and gait speed decline in well-functioning older adults. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2010, 65, 1093–1100. [Google Scholar] [CrossRef]
- Naveh-Benjamin, M.; Cowan, N. The roles of attention, executive function and knowledge in cognitive ageing of working memory. Nat. Rev. Psychol. 2023, 2, 151–165. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P. The nature and organization of individual differences in executive functions: Four general conclusions. Curr. Dir. Psychol. Sci. 2012, 21, 8–14. [Google Scholar] [CrossRef]
- Lee, M.-T.; Jang, Y.; Chang, W.-Y. How do impairments in cognitive functions affect activities of daily living functions in older adults? PLoS ONE 2019, 14, e0218112. [Google Scholar] [CrossRef]
- Tomaszewski Farias, S.; Cahn-Weiner, D.A.; Harvey, D.J.; Reed, B.R.; Mungas, D.; Kramer, J.H.; Chui, H. Longitudinal changes in memory and executive functioning are associated with longitudinal change in instrumental activities of daily living in older adults. Clin. Neuropsychol. 2009, 23, 446–461. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, L. Functional brain imaging of episodic memory decline in ageing. J. Intern. Med. 2017, 281, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Abd Razak, M.; Ahmad, N.; Chan, Y.; Kasim, N.M.; Yusof, M.; Ghani, M.A.; Omar, M.; Abd Aziz, F.; Jamaluddin, R. Validity of screening tools for dementia and mild cognitive impairment among the elderly in primary health care: A systematic review. Public Health 2019, 169, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Hwang, A.B.; Boes, S.; Nyffeler, T.; Schuepfer, G. Validity of screening instruments for the detection of dementia and mild cognitive impairment in hospital inpatients: A systematic review of diagnostic accuracy studies. PLoS ONE 2019, 14, e0219569. [Google Scholar] [CrossRef]
- Ihle, A.; Gouveia, É.R.; Gouveia, B.R.; Kliegel, M. The Cognitive Telephone Screening Instrument (COGTEL): A brief, reliable, and valid tool for capturing interindividual differences in cognitive functioning in epidemiological and aging studies. Dement. Geriatr. Cogn. Disord. Extra 2018, 7, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Fiorenzato, E.; Weis, L.; Falup-Pecurariu, C.; Diaconu, S.; Siri, C.; Reali, E.; Pezzoli, G.; Bisiacchi, P.; Antonini, A.; Biundo, R. Montreal Cognitive Assessment (MoCA) and Mini-Mental State Examination (MMSE) performance in progressive supranuclear palsy and multiple system atrophy. J. Neural Transm. 2016, 123, 1435–1442. [Google Scholar] [CrossRef]
- El-Shafie, N.T.; El-Nahas, N.M.; Elgazzar, R.F. Mini-Mental State Examination as a reliable tool for the diagnosis and treatment follow-up of mild cognitive impairment: A systematic review. Curr. Aging Sci. 2020, 13, 164–174. [Google Scholar]
- Nascimento, M.D.M. Dance, aging, and neuroplasticity: An integrative review. Neurocase 2021, 27, 372–381. [Google Scholar] [CrossRef]
- Hewston, P.; Kennedy, C.C.; Borhan, S.; Merom, D.; Santaguida, P.; Ioannidis, G.; Marr, S.; Santesso, N.; Thabane, L.; Bray, S. Effects of dance on cognitive function in older adults: A systematic review and meta-analysis. Age Ageing 2021, 50, 1084–1092. [Google Scholar] [CrossRef]
- Meng, X.; Li, G.; Jia, Y.; Liu, Y.; Shang, B.; Liu, P.; Bao, X.; Chen, L. Effects of dance intervention on global cognition, executive function and memory of older adults: A meta-analysis and systematic review. Aging Clin. Exp. Res. 2020, 32, 7–19. [Google Scholar] [CrossRef]
- Hamacher, D.; Hamacher, D.; Rehfeld, K.; Hökelmann, A.; Schega, L. The effect of a six-month dancing program on motor-cognitive dual-task performance in older adults. J. Aging Phys. Act. 2015, 23, 647–652. [Google Scholar] [CrossRef]
- Teixeira-Machado, L.; Arida, R.M.; de Jesus Mari, J. Dance for neuroplasticity: A descriptive systematic review. Neurosci. Biobehav. Rev. 2019, 96, 232–240. [Google Scholar] [CrossRef]
- Rehfeld, K.; Lüders, A.; Hökelmann, A.; Lessmann, V.; Kaufmann, J.; Brigadski, T.; Müller, P.; Müller, N.G. Dance training is superior to repetitive physical exercise in inducing brain plasticity in the elderly. PLoS ONE 2018, 13, e0196636. [Google Scholar] [CrossRef]
- Klarod, K.; Singsanan, S.; Thamwiriyasati, N.; Ladawan, S.; Luangpon, N.; Boonsiri, P.; Burtscher, M. Effects of Qigong exercise on muscle strengths and oxidative stress/antioxidant responses in young sedentary females: A quasi-experimental study. J. Exerc. Rehabil. 2020, 16, 418. [Google Scholar] [CrossRef]
- Wehner, C.; Blank, C.; Arvandi, M.; Wehner, C.; Schobersberger, W. Effect of Tai Chi on muscle strength, physical endurance, postural balance and flexibility: A systematic review and meta-analysis. BMJ Open Sport Exerc. Med. 2021, 7, e000817. [Google Scholar] [CrossRef] [PubMed]
- Gallou-Guyot, M.; Mandigout, S.; Bherer, L.; Perrochon, A. Effects of exergames and cognitive-motor dual-task training on cognitive, physical and dual-task functions in cognitively healthy older adults: An overview. Ageing Res. Rev. 2020, 63, 101135. [Google Scholar] [CrossRef] [PubMed]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of combined physical and cognitive training on cognition: A systematic review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef]
- Bleakley, C.M.; Charles, D.; Porter-Armstrong, A.; McNeill, M.D.; McDonough, S.M.; McCormack, B. Gaming for health: A systematic review of the physical and cognitive effects of interactive computer games in older adults. J. Appl. Gerontol. 2015, 34, NP166–NP189. [Google Scholar] [CrossRef] [PubMed]
- Cabral, D.F.; Rice, J.; Morris, T.P.; Rundek, T.; Pascual-Leone, A.; Gomes-Osman, J. Exercise for brain health: An investigation into the underlying mechanisms guided by dose. Neurotherapeutics 2019, 16, 580–599. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Rodríguez, R.; Álvarez-Bueno, C.; Martínez-Ortega, I.A.; Martínez-Vizcaíno, V.; Mesas, A.E.; Notario-Pacheco, B. Immediate effect of high-intensity exercise on brain-derived neurotrophic factor in healthy young adults: A systematic review and meta-analysis. J. Sport Health Sci. 2022, 11, 367–375. [Google Scholar] [CrossRef]
- Chen, F.-T.; Etnier, J.L.; Chan, K.-H.; Chiu, P.-K.; Hung, T.-M.; Chang, Y.-K. Effects of exercise training interventions on executive function in older adults: A systematic review and meta-analysis. Sports Med. 2020, 50, 1451–1467. [Google Scholar] [CrossRef]
- Jahangiri, Z.; Gholamnezhad, Z.; Hosseini, M.; Beheshti, F.; Kasraie, N. The effects of moderate exercise and overtraining on learning and memory, hippocampal inflammatory cytokine levels, and brain oxidative stress markers in rats. J. Physiol. Sci. 2019, 69, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Rogge, A.-K.; Röder, B.; Zech, A.; Hötting, K. Exercise-induced neuroplasticity: Balance training increases cortical thickness in visual and vestibular cortical regions. Neuroimage 2018, 179, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.F.; Erickson, K.I. Capitalizing on cortical plasticity: Influence of physical activity on cognition and brain function. Trends Cogn. Sci. 2007, 11, 342–348. [Google Scholar] [CrossRef]
- Raz, N.; Lindenberger, U.; Rodrigue, K.M.; Kennedy, K.M.; Head, D.; Williamson, A.; Dahle, C.; Gerstorf, D.; Acker, J.D. Regional brain changes in aging healthy adults: General trends, individual differences and modifiers. Cereb. Cortex 2005, 15, 1676–1689. [Google Scholar] [CrossRef]
- Herold, F.; Törpel, A.; Schega, L.; Müller, N.G. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements—A systematic review. Eur. Rev. Aging Phys. Act. 2019, 16, 10. [Google Scholar] [CrossRef]
- Wilke, J.; Giesche, F.; Klier, K.; Vogt, L.; Herrmann, E.; Banzer, W. Acute effects of resistance exercise on cognitive function in healthy adults: A systematic review with multilevel meta-analysis. Sports Med. 2019, 49, 905–916. [Google Scholar] [CrossRef] [PubMed]
- Snowden, M.; Steinman, L.; Mochan, K.; Grodstein, F.; Prohaska, T.R.; Thurman, D.J.; Brown, D.R.; Laditka, J.N.; Soares, J.; Zweiback, D.J. Effect of exercise on cognitive performance in community-dwelling older adults: Review of intervention trials and recommendations for public health practice and research. J. Am. Geriatr. Soc. 2011, 59, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Oberlin, L.E.; Jaywant, A.; Wolff, A.; Gunning, F.M. Strategies to promote cognitive health in aging: Recent evidence and innovations. Curr. Psychiatry Rep. 2022, 24, 441–450. [Google Scholar] [CrossRef]
- Sanders, L.M.; Hortobagyi, T.; la Bastide-van Gemert, S.; van der Zee, E.A.; van Heuvelen, M.J. Dose-response relationship between exercise and cognitive function in older adults with and without cognitive impairment: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0210036. [Google Scholar] [CrossRef]

{kind=link}
| Key Search Terms | Related Search Terms |
|---|---|
| Cognitive function | “Cognitive function” OR “Cognitive dysfunction” OR “Cognitive behavio*” OR “Cognitive decline” OR “Cognitive domains” OR Dement * |
| Physical fitness | “Physical activity” OR Exercise OR Sport OR Fitness OR Functional OR Movement |
| Active ageing | Healthy OR “Active ageing” |
| Older adults | “Older adults” OR Senior OR Elder * OR “Older people” |
| Authors and Year | Sample Characteristics | Purpose | Setting and Country | Intervention (Duration; Main Characteristics of the Program) | Cognitive Outcome (Measures) | Main Results |
|---|---|---|---|---|---|---|
| [27] (2020) | 64 F (IG = 32, aged mean 65.48 years old; CG = 32, aged mean 64.77 years old). | Evaluate the effect of “Brain Gym” exercises on cognitive function and plasma brain-derived neurotrophic factor in the elderly. | Public health centre in Jakarta, Indonesia. | IG: 12 weeks; aerobic (mostly core movements); 2×/week; 60 min of exercise. CG: exercise not performed. | Orientation, memory, recall, attention, naming objectives, verbal and written commands, writing and coping with a figure (MMSE) | No significant difference was seen in MMSE scores between treatment and control groups. |
| [28] (2018) | 149 F + 72 M (IG1 = 49, aged mean 64.82 years old; IG2 = 49, aged mean 64.51 years old; IG3 = 59, aged mean 65.58 years old; IG4 = 64, aged mean 65.52 years old). | Examined whether baseline brain network modularity predicted cognitive improvements in older adults after an exercise intervention. | Urbana-Champaign community in Illinois, USA. | IG1: 6 months; aerobic (walking); 3×/week; 60 min of exercise. IG2: 6 months; aerobic (walking + supplementation); 3×/week; 60 min of exercise. IG3: 6 months; stretching, strengthening and stability; 3×/week; 60 min of exercise. IG4: 6 months; aerobic (dance); 3×/week; 60 min of exercise. | Vocabulary, perceptual speed, episodic memory, and fluid reasoning (VCAP) Executive function (switching task and spatial working memory). | IG1, IG2, and IG3 showed greater executive function gains compared to the IG4 group. No group effects were observed for improvements in perceptual speed, episodic memory, and vocabulary. |
| [29] (2023) | 79 F + 41 M (IG = 59, aged mean 70.6 years old; CG = 61, aged mean 72 years old). | Examined the cognitive effects of the home-based computerised multidomain intervention StayFitLonger (SFL), combining physical exercise and cognitive training, compared to an active control condition. | Home in Switzerland, Canada, and Belgium. | IG (StayFitLonger—computerised home-based training). 26 weeks; strength, balance, and mobility + cognitive training; at least 3×/week; 30–45 min exercise. CG: the active control intervention had structure, timing, and organisation similar to the IG. The difference was that they only had a limited number of physical exercises and did not include interactive videos, personalisation, chat rooms, psycho-educational content, or a virtual guide. | Global Cognition (ZAVEN) Executive Function (Letter Fluency Test, TMT, VST and TAP) Memory (CVLT and Logical Memory Task) Processing Speed (TMT, DSST and VST). | They found that pre-frail individuals in the IG improved their global cognition and processing speed scores after the intervention, unlike participants in the active control condition and unlike robust participants enrolled in either intervention. |
| [30] (2021) | 23 F + 9 M (IG1 = 17, aged mean 76.5 years old; IG2 * = 15, aged mean 80.5 years old). | Determine the effects of exercise training on cognition and cortical grey matter microstructure in individuals with MCI vs. cognitively healthy older adults. | Community (retirement communities and recreation centres) in Wisconsin, USA. | IG1 12 weeks; aerobic (treadmill walking); 3×/week; 30 min exercise. IG2: not considered *. | Multiple aspects of cognition (Geriatric Depression Scale, DRS-2, RAVLT, COWAT, Semantic Animal Fluency Test, and the Clock Drawing Test). | IG significantly improved in RAVLT (verbal memory) and COWAT (verbal fluency). |
| [31] (2021) | 63 F + 42 M (IG = 52, aged mean 71.8 years old; CG = 53, aged mean 72.7 years old). | Verify whether medium-intensity physical activity in elderly people living in the community effectively improves cognitive performance. | Community in Cagliari, Italy. | IG: 12 weeks; aerobic, anaerobic, strength, and balance exercises; 3×/week; 65 min exercise. CG: same time of exposure, but this group performed activities focusing on the history of local culture and education of wellness. | Attention, memory, verbal fluency, language, visual-spatial skills (ACE-R) | IG showed improvements in the ACE-R and better performances for the memory and visual-space skills subscales of the ACE-R. |
| [32] (2022) | 18 F + 7 M (IG1 = 13, aged mean 60.3 years old; IG2 = 12, aged mean 70.2 years old). | Compared the effects of traditional resistance training and resistance training combined with cognitive tasks on body composition, physical performance, cognitive function, and plasma brain-derived neurotrophic factor levels in older adults. | Community and does not represent the country. | IG1 (resistance training + cognitive tasks); 16 weeks; resistance (major muscle groups using machines, free weights, and body weight); 2×/week; 60 min of exercise + verbal fluency cognitive task. IG2 (resistance training only). Same resistance training as IG1. | Verbal fluency (VFT) Dual task (TUG + cognitive test) Short-term memory (SPMT) executive function, visual attention, and task switching (TMT). | Exclusive improvements in cognitive function were observed only in IG1. The improvements were only in verbal fluency and dual-task tests. Short-term memory and executive function did not present significant improvements. |
| [33] (2020) | 16 F + 12 M (IG1 = 10, aged mean 68.8 years old; IG2 = 9, aged mean 71.2 years old; CG = 9, aged mean 67.7 years old) | Explored the effects of exercise with either a high cognitive load (IG1) or low cognitive load (IG2) on cognitive performance and neuroplasticity in healthy elderly. | Community in Taiwan, China. | IG1: 4 months; aerobic (dance); 3×/week; 50 min exercise. IG2: 4 months; aerobic (walking on treadmill); 3×/week; 50 min exercise. CG: exercise not performed. | Attention, orientation, short-term memory, long-term memory, language, drawing, abstract thinking and judgment, mental manipulation, and animal name fluency (CASI 2.0). | IG1 had a significantly higher score on the CASI test demonstrating that a high-cognitive load, but not exercise with a low-cognitive load, improved the overall cognitive function of healthy, elderly individuals. |
| [34] (2019) | N/S F + N/S M (IG1= 30, aged mean 65.5 years old; IG2 * = 30, aged mean 67.5 years old). | Demonstrated the importance of traditional Greek dances in improving both the cognitive and physical health of the senior citizens. | Greek Association of Alzheimer’s Disease and Relative Disorders and Daycare Centres in Thessaloniki, Greece. | IG1 24 weeks; aerobic (traditional Greek dance); 2×/week; 60 min exercise. IG2: not considered *. | Cognitive performance (CDR), attention (TEA), executive function (TMT and FUCAS), memory (ROCF, RAVLT, and RBMT), verbal fluency (VFT). | After the intervention was verified, positive changes occurred for attention, executive function, immediate memory, and delayed recall. |
| [35] (2020) | 41 F + 27 M (IG1 = 21, aged mean 71.3 years old; IG2 = 24, aged mean 69.5 years old; IG3 = 23, aged mean 69.9 years old). | Tested the effects of unstable vs. stable resistance training on executive functions. | Community in Kassel, Germany. | IG1: 10 weeks; resistance (instability free weights); 2×/week; 60 min exercise. IG2: 10 weeks; resistance (stable machine-based exercise); 2×/week; 60 min exercise. CG: 10 weeks; resistance (stable machine-based adductor/abductor training); 2×/week; 60 min exercise. | Neuropsychological (DSST), memory (DMT), selective attention and processing speed (Stroop), visual attention and task switching (TMT). | IG1 (instability resistance training), improved working memory, processing speed, and response inhibition. In contrast, improvements in executive functions for IG2 and IG3 were not verified. |
| [36] (2020) | 31 F + 9 M (IG1 = 12, aged mean 68.08 years old; IG2 = 15, aged mean 67.2 years old; CG = 14, aged mean 67.2 years old). | Compared the effects of dance/movement training to aerobic exercise training on cognition, physical fitness, and health-related quality of life in healthy, inactive, elderly individuals. | Community in Canada. | IG1: 12 weeks; aerobic (dance movement); 3×/week; 60 min exercise. IG2: 12 weeks; aerobic (recumbent bicycle); 3×/week; 60 min exercise. CG: exercise not performed. | Executive functions (dual-task, N-back, and Digit Stroop); global cognition (MoCA) | Executive and non-executive composite scores significantly increased, but no group difference or interaction was verified. There was no time effect, group difference, or interaction for the MoCA. |
| [37] (2021) | 22 F + 9 M (IG = 15, aged mean 67.6 years old; CG = 16, aged mean 69.1 years old). | Investigated the effect of a physical exercise multicomponent training based on exergames on cognitive function in older adults. | Local senior gymnasium in Madeira, Portugal. | IG 12 weeks; functional exercise (group training sessions) + exergames fitness program; 2×/week (1-day functional fitness + 1-day exergames); 45 min exercise. CG: 12 weeks; functional exercise (group training sessions); 2×/week; 45 min exercise. | Prospective memory, verbal short-term memory, long-term memory, working memory, verbal fluency, and inductive reasoning (COGTEL). | Both groups obtained significant short-term memory, long-term memory, and COGTEL total scores. However, at the follow-up session (4 weeks later), only the IG group showed a significant improvement in short-term memory and long-term memory. |
| [38] (2020) | 105 F + 101 M aged mean 65.9 years old. | Investigated the effects of a 6-month aerobic exercise intervention on cognition and cerebrovascular regulation. | Community in Calgary, Alberta, Canada. | 6 months; aerobic (aerobic training); 3×/week; the exercise duration increased from 20 to 40 min as participants progressed in the program. | Processing speed (Symbol Digit Modalities Test), executive functions (Cart Sorting Test and Colour and Word Inference Test), verbal memory (Buschke Selective Reminding Test), figural memory (Medical College of Georgia Complex Figure), fluency (Verbal Fluency Test), attention (Auditory Consonant Trigram Test). | After the intervention, positive changes were seen in the executive functions (processing speed and concept formation), verbal memory, and fluency. The figural memory domain showed a negative change, and no changes were found for complex attention. |
| [39] (2021) | 24 F + 14 M (IG1 = 20, aged mean 69.9 years old; IG2 = 18, aged mean 70.9 years old). | Whether a combination of Bifidobacterium spp. supplementation and moderate resistance training improved cognitive function and other health-related parameters in healthy, elderly subjects. | Public liberal art school in Hyogo, Japan. | IG1: probiotic group: 12 weeks; resistance training (combination of latex band training, squats, and Tai Chi); 90 min. Participants were encouraged to perform daily exercises at home, such as stretching, squatting, or walking, and record the types and durations of each exercise session. IG 2: placebo group: same training as IG1. | Global cognition (MoCA); response accuracy reaction time (Flanker task test). | MoCA scores showed a significant increase in both groups, while the flanker task scores for the probiotic group increased more significantly than those for the placebo group. |
| [40] (2021) | 61 F + 11 M (IG = 41, aged mean 67.39 years old; CG = 31, aged mean 67.87 years old). | Analysed the effects of dual-task multimodal physical exercise at a moderate intensity and cognitive stimulation on cognitive and physical functions on healthy, older adults. | Community in Brazil. | IG1: exercise + cognitive stimulation (dual task), 12 weeks; aerobic, resistance and flexibility training (walking, functional circuits, agility, balance, coordination, dance, and global resistance exercises, such as squats and bench press); 2×/week; 75 min exercise. CG: educational materials on health-related topics. | Cognitive performance (CANTAB), ability to understand and complete tasks (Motor Screening Test), episodic memory (PAL test), visual attention (RVT test). | Intervention positively influenced episodic memory (PAL test) and sustained visual attention (RVP test). |
| [41] (2020) | 53 F + 43 M (IG1 = 24, aged mean 65.45 years old; G2 = 25, aged mean 66.52 years old; IG3 = 22, aged mean 65.53 years old; CC = 25, aged mean 66.34 years old). | Investigated the effects of physical exercise tapping high-level cognitive functions on both cognitive function and fitness in older adults. | Community in Shanghai, China. | IG1: the same training as IG2 + cognitive training. IG2: 12 weeks; aerobic training (treadmill walking); 3×/week; 60 min exercise. IG3: cognitive training—program designed to improve executive function and memory. CC: received physical exercise materials but did not participate in a cognitive or exercise programme. | Processing speed (computerised modified Stroop). | IG1, IG2, and IG3 improved executive function performance, but only IG1 showed a general facilitative effect on nonexecutive control. |
| [42] (2018) | 13 F + 13 M (aged mean 74.24 years old). | Verified if 6-week exercise training improved physical fitness in gait speed and cognition in the memory domain in older adults. | Retired professors (education for 16–19 years) from Beijing, China. | 6 weeks; aerobic (dance training exercise program); 4×/week; 45 min exercise. | Verbal memory (RAVLT), verbal episodic memory (WMS—LM), working memory (WAIS-III Digit-Symbol Substitution Modality Test and Digit Span), executive function (TMT), visual memory (BVMT). | After the exercise program, participants showed significantly improved memory performances in the Logical Memory Test (WMS—LM) and Rey Auditory Verbal Learning Test. The WAIS-III Digit Span showed a marginally significant increase. |
| [43] (2022) | 33 F + 7 M (IG = 20, aged mean 67.5 years old; CG = 20, aged mean 67.6 years old). | Determined the effect of 12-week Judo training on cognitive processing and muscle function among the elderly. | Health Promotion Center in Poland. | IG: 12 weeks; strength and resistance (Judo); 3×/week; 45 min of exercise. CG: did not undertake any exercises during the experiment. | Processing speed (Stroop Test) | IG-improved Stroop performance reflected by shortening the response time related to the Stroop “naming” interference. |
| [44] (2022) | 51 F + 4 M (IG1 = 28, aged mean 67.7 years old; IG2 = 27, aged mean 64.6 years old). | Analysed the influence of sitting callisthenic balance and resistance training on cognitive function and the mediating role of the change in the level of neurotrophic factors and strength in older, healthy participants. | Community in Bydgoszcz, Poland. | IG1 (sitting callisthenic balance): 3 months; stretching, mobility exercises, basic core-strength, and balance exercises (without additional weights); 2×/week; 45 min of exercise. IG2 (resistance training): 3 months; strength and resistance (machine and non-machine-based exercises); 2×/week; 50 min of exercise. | Global cognitive function (MoCA), cognitive function (Sprawnosci Operacyjnej Test), executive function (TMT B), auditory attention (DST), working memory (DST Backwards). | Both IG1 and IG2 influenced multiple cognitive domains. The IG2 program improved global cognitive functioning, decision making, and visual attention. In IG1, set shifting and the short-term visual memory processing speed of simple. visual stimuli were improved. |
| [45] (2022) | 26 F (IG = 13, aged mean 62.5 years old; CG = 13, aged mean 69.5 years old). | Assessed the effects of 4-movement Qigong on cognitive function and physical performance. | Community in Innsbruck, Austria. | IG: 8 weeks; function and flexibility (4-movement Qigong); 3×/week; 45 min of exercise. CG: maintained their usual activities of daily living throughout the study period. | Executive function (TMT-A and TMT-B); memory function (DST Forwards and Backwards). | IG significantly improved TMT-A and TMT-B. |
| [46] (2021) | 31 F + 15 M (IG1 = 25, aged mean 79.6 years old; IG2 = 21, aged mean 83.8 years old). | Compared the effects of Kinect-based exergaming and combined physical exercise training on cognitive function and brain activation in frail, older adults. | Care centres for communities in Taiwan, China. | IG1: exergames, 12 weeks; resistance (upper and lower extremity movements using 3D Space), aerobic (swimming and running in a 3D space), and balance (balance exercises and Tai Chi) training; 3×/week; 60 min exercise. IG2: physical exercise, 12 weeks; resistance (upper and lower extremity movements using Theraband), aerobic (stepping variations), and balance (balance exercises and Tai Chi) training; 3×/week; 60 min exercise. | Global cognition (MoCA), executive function (EXIT 25), verbal memory (CCVLT), attention (CWT), working memory (spatial n-back task test). | Both groups improved significantly in global cognition, executive function, and attention after the 12-week intervention. Only the IG1 group showed significant improvements in verbal and working memory after the intervention. |
| [47] (2021) | 14 F + 6 M (aged mean 69.1 years old). | Determined whether a 12-week strength training program could improve fluid cognition in healthy, older adults and explore concomitant physiological and psychological changes. | Community in Los Angeles, USA. | 12 weeks; resistance training (total body strength using machine-based exercises); 3×/week; 60 min exercise. | NIHTB-CB fluid cognition (inhibitory control and attention, episodic memory, working memory, executive function, and processing speed). NIHTB-CB crystallised cognition (vocabulary and reading recognition). | NIHTB-CB fluid composite scores significantly increased from pre- to post-interventions, while NIHTB-CB crystallised composite scores did not. Performances on individual fluid instruments, including executive function, attention, working memory, and processing speed, also significantly improved. |
| [48] (2017) | 25 F + 28 M (IG = 29, aged mean 73.3 years old; CG = 24, aged mean 77 years old). | Understood the effect of aerobic training on cerebral metabolism and cerebral grey matter volume in older adults. | Assisted living facilities in Frankfurt am Main, Germany. | IG: 12 weeks; aerobic (bicycle); 3×/ week; 30 min of exercise. | Memory (VLMT early recall, VLMT late recall, VLMT recognition, and CERAD figure recall), executive control (Stroop interference), working memory (Digit span forwards, Digit span backwards), verbal fluency (semantic fluency and phonematic fluency). | The analysis did not reveal a significant effect of any cognitive domains assessed in this study. |
| [49] (2021) | 148 F + 49 M (females were 75% of the participants and were considered people ≥ 60 years old). | Observed if the Healthy Ageing Promotion Program for You, promoted improvements in cognition, frailty status, functional status, perceived health, and reduction in social isolation. | Community in Singapore. | 3 months; dual-task exercises (resistance, balance, aerobic, and cognitive tasks); 1 or 2×/week; 60 min exercise. | Global cognition (MoCa). | There was significant improvement in the MoCA scores at 3 months for the entire group. |
| [50] (2023) | 24 F + 62 M (IG1 = 27, aged mean 67.9 years old; IG2 = 30, aged mean 67.2 years old; CG = 29, aged mean 68.3 years old). | Analysed the effects of two short-term aerobic exercises on cognitive function in healthy, older adults during COVID-19. | Home in Tokyo and Kanagawa, Japan. | IG1 (walking group): 4 weeks; aerobic (walking with Nordic ski poles in both hands) 3×/week; 30 min of exercise. IG2 (dance): 4 weeks; aerobic (dance) 3×/week; 30 min of exercise. CG: maintained their usual activities of daily living throughout the study period. All groups consumed amino acid-containing foods 3×/week. | Global cognitive functioning (MoCA); executive function (FAB). | The results show that both exercise intervention groups (IG1 and IG2) improved executive function, while the dance group (IG2) showed an additional improvement in global cognitive function. |
| [51] (2018) | 17 F + 2 M (IG = 8, aged mean 75.0 years old; CG = 11, aged mean 71.9 years old). | Examined the effect of 2-year cognitive-motor dual-task training on the cognitive function and motor ability of healthy, elderly people without marked cognitive impairments. | Community dwellers in Sumiyoshi-ku, Osaka City, Japan. | IG: 2 years; mental gymnastics, resistance training, aerobic exercise, and flexibility exercises; 1×/week; 60min of exercise. | Registration and recall, long-term memory, orientation, attention, verbal fluency and understanding, word retrieval, visuospatial skills, abstract meaning (Modified MMSE—3MS). Proc. Speed (TMT). | Participation in IG maintained the scores in almost all domains of cognitive function, as well as the total 3MS scores. 3MS scores decreased in CG. |
| [52] (2017) | 10 F + 12 M (IG1 = 12, aged mean 68.25 years old; IG2 = 10, aged mean 68.6 years old). | Assessed whether a dance training program that stressed the constant learning of new movement patterns was superior in terms of neuroplasticity to conventional fitness activities, | Community in Germany. | First 6 months: IG1: aerobic training (dance), 2×/week; 90 min exercise. IG2: strength and endurance training (cycle ergometer and exercises for all body parts), 2×/week; 90 min exercise. Last 12 months: same training for both groups, but only 1×/week. | Verbal short- and long-term memory (RAVLT); attention (TAP) | Both groups showed significant improvements in attention after 6 months and verbal memory after 18 months. In terms of cognitive ability, no group differences emerged. |
| [53] (2022) | 16 F + 24 M (IG1 = 20, aged mean 64.05 years old; IG2 = 20, aged mean 65.50 years old). | Compared the efficiency of dual-task training versus aerobic exercise training in improving cognitive function in healthy, older individuals. | Community in Wardha, Maharashtra, India. | IG: 6 weeks; dual-task training (cognitive + motor activities); 3×/week; 45 min. IG2: 6 weeks; aerobic training (treadmill, bicycle, and walking exercises); 5×/week; 45 min. | Working memory (TMT-A), executive Function (TMT-B), general global cognitive function (MoCA). | Both groups noted post-intervention improvements in TMT-A, TMT-B, and MoCA scores. However, the difference was more significant for group IG1 than group IG2. |
| [54] (2021) | 17 F + 16 M (IG = 17, aged mean 77.35 years old; CG = 16, aged mean 76.81 years old). | Investigated the effect of an intervention combining exercise and cognitive activity on cognitive function in healthy, older adults. | Community in Kobe city, Japan. | IG: 3 mounts, stretching, muscle strength, and dual-task aerobic exercises, 1×/week; 50 min exercise. Also had a homework cognitive task twice a week. CG: no received intervention. | Cognitive impairment (MMSE), long- and short-term memory (Logical Memory IIA), executive function (TMT), motor speed, attention, visual perception (DSST). | A significant improvement in long-term and short-term memory was observed in the IG at follow-up and five or six months after the conclusion of the intervention. Additionally, the decline in MMSE scores in the IG was lower than in the CG. |
| [55] (2017) | 15 F + 14 M (IG = 14, aged mean 69.7 years old; CG = 15, aged mean 68.6 years old). | Investigated the effects of exergame training over 6 weeks on healthy, old participants’ cognitive, motor, and sensory functions. | Community in Leipzig, Germany. | IG: exergames 6 weeks; strength (hurdles, javelin throwing, 100 m running), aerobic (swimming, hammer throwing), and coordination (trampoline, high diving, archery, mountain biking), 2×/week; 60 min exercise. IG2: no received intervention | Attention (TAP 2.3), working memory (N-back task), alertness and simple reaction time (reaction time to a visual stimuli), response inhibition (response triggered by an external stimulus). | IG showed significant performance improvements in alertness and simple reaction time from baseline to post-measurement. These improvements did not result in differential performance improvements when comparing IG and CG. |
| [56] (2023) | 19 F + 16 M (IG1 = 7, aged mean 63.7 years old; IG2 = 11, aged mean 63.1 years old; IG3 = 17, aged mean 64.6 years old). | Investigated the effects of simultaneous exercise and cognitive training on several cognitive domains in healthy, older adults compared to training alone. | Does not present this information. | IG1: exercise training: 24 weeks; aerobic (stationary bicycle); 2×/week; 30 min of exercise. IG2: cognitive training: 24 weeks; cognitive games; 2×/week; 30 min of exercise. IG3: exercise + cognitive training. Combine IG1 and IG2 interventions. | Executive functions (TMT and Computerised Modified Stroop task), verbal memory (Rey Words test), working memory (2-back test). | All groups improved their executive performances, including flexibility or working memory. Simultaneous exercise and cognitive training ere more efficient than either training alone to improve executive function. |
| [21] (2020) | 57 F + 27 M (IG1 = 20, aged mean 67.6 years old; IG2 = 21, aged mean 66.3 years old; IG3 = 19, aged mean 68.1 years old; IG4 = 14, aged mean 69.2 years old). | Evaluated the effects of simultaneous aerobic exercise and cognitive training intervention on dual-task walking performance on healthy, older adults. | Community, in Tucson, Arizona, USA. | IG1: aerobic exercise and cognitive training, combined IG2 and IG3 conditions described below. IG2: cognitive training, 12 weeks; cognitive training, 3×/week; 30 min exercise. IG3: aerobic exercise, 12 weeks; aerobic training (stationary recumbent bicycle), 3×/week; progressively increased exercise from 15 to 30 min. IG4: video-watching control, 12 weeks; watching videos, 3×/week; 30 min. | Serial subtraction during two-minute walk (DTWT) | IG1, IG2, and IG3 groups significantly improved in the cognitive aspect of the DTWT following the full 12-week intervention. The improvements in IG1 were twice as much as in the other groups and were significant at 6 weeks. |
| [57] (2018) | 28 F + 9 M (IG1 = 18, aged mean 67.6 years old; IG2 = 19, aged mean 69.1 years old). | Compared the effects of Poi and Tai Chi on physical and cognitive functions in healthy, older adults. | Does not present this information. | IG1: Poi (a weight on the end of a cord that is swung in circular patterns around the body), 4 weeks, Poi exercise (strength/functional), 2×/week, 60 min. IG2: Tai Chi , 4 weeks, Tai Chi exercise, 2×/week, 60 min. | Verbal memory and visual memory, finger tapping, symbol digit coding, Stroop test, shifting attention, and continuous performance (CNS Vital Signs) | Both groups increased simple attention, complex attention, cognitive flexibility, psychomotor speed, and executive function. Both groups declined in composite memory and visual memory tests. |
| [58] (2020) | 29 F + 17 M (IG = 23, aged mean 65.5 years old; CG = 23, aged mean 67.7 years old). | Compared the effects of 12 weeks of aerobic training versus control condition on cardiorespiratory fitness, cognition, and magnetic resonance imaging. | Community in Oxford, England. | IG: 12 weeks, aerobic exercise (cycling), 3×/week, 30 min. CG: continued with their normal routines and did not begin a PA programme. | Executive function (TMT B and COGSTATE Two-Back), memory (HVLT-R and RCF), processing speed (TMT A. Digit Coding and CNTABRTTT). | There were no significant differences in cognitive measures between the aerobic training and control groups. |
| [59] (2018) | 90 F + 15 M (IG = 60, aged mean 73.59 years old; CG = 45, aged mean 73.22 years old). | Examined whether Bingocize (Game Centerer Mobile Application) could improve aspects of physical and cognitive performances. | Senior centres in Kentucky and Tennessee, USA. | IG: Bingo + health education + exercise, 10 weeks, 12 exercises of cardiovascular, strength, balance, and flexibility exercises, 2×/week; 60 min CG: Bingo + health education, 10 weeks, 2×/week; 60 min. | Monitoring and adjusting working memory contents, switching flexibly between tasks, and deliberately overriding dominant/prepotent responses (EXAMINER cognitive battery). | IG performed better than the control group in the “updating” (executive function) task of the EXAMINER battery. However, this was subsumed by a significant interaction. |
| [60] (2017) | 64 M (IG1 = 22, aged mean 66.88 years old; IG2 = 21, aged mean 66.15 years old; IG3 = 21, aged mean 65.7 years old). | Explored the effects of 6-month open- and closed-skill exercise interventions on the neurocognitive performance of the elderly when performing the task-switching paradigm and N-back task. | Community in Taiwan. | IG1: 24 weeks, skill training (table-tennis games), 3×/week, 40 min). IG2: 24 weeks, aerobic exercise (treadmill or cycling), 3×/week, 40 min. IG3: 24 weeks, balance and stretching, 3×/week, 40 min. | Switching capacity (task-switching paradigm); working memory (N-back task). | IG1 and IG2 did not increase their accuracy rates in the task-switching paradigm but presented significantly faster responses than IG3 in the switch trials. In terms of the N-back task, the two exercise groups significantly increased their accuracy rates in the 1-back condition, and IG1 also showed an improvement in the accuracy rate in the 2-back condition. |
| [61] (2023) | 63 F + 19 M (IG1 = 27, aged mean 72.1 years old; IG2 = 29, aged mean 73.3 years old; CG = 26, aged mean 72.1 years old). | Compared the effects of a supported yoga-based exercise intervention on verbal fluency to an aerobic exercise intervention and a wait-list control group. | Community in Stockholm, Sweden. | IG1 (yoga): 12 weeks; yoga; ≥3×/week; 60 min of exercise. IG2 (aerobic): 12 weeks; aerobic (cycling/spinning, dance-based exercise) ≥3×/week; 60 min of exercise. CG: maintained their usual activities of daily living throughout the study period. | Verbal fluency (total FAS, animals, and verbs) | Participation in yoga or aerobic exercises was associated with estimated improvements in verbal fluency compared to a non-active control group. |
| [62] (2020) | 12 F + 14 M (IG = 15, aged mean 69.7 years old; CG = 9, aged mean 71.9 years old). | Observed the effect of dual-task exercise (Synapsology) to improve physical and cognitive functions. | Community in Tsukuba, Japan. | IG: 8 weeks, dual-task exercises (stretching, lower body exercises, and walking + cognitive tasks), 2×/ week; 60 min. CG: no received intervention. | Executive function (TMPT, 25-hole peg test). | Cognitive function results in the 25-hole trail-making peg test had a statistically significant difference within the IG. However, the differences in the TMPT between the IG and CG were insignificant. |
| [63] (2022) | 24 F + 14M (IG = 13, aged mean 62.5 years old; CG = 13, aged mean 69.5 years old). | Explored the effects of an active videogame intervention on fitness and cognitive functions in older adults. | Community in Xian Province and Shaanxi Province, China. | IG (videogame exercises): 12 weeks; aerobic (Zumba, aerobic boxing, and virtual tennis); 3×/week; 50–55 min of exercise. CG: maintained their usual activities of daily living throughout the study period. | Processing speed, spatial ability, working memory, language ability, and associative memory (specific software) | The results show improvements in cognition (spatial cognition) in the IG. |
| Authors | Selection Bias | Design | Confounders | Blinding | Data Collection Methods | Withdrawals and Drop-Outs | Overall |
|---|---|---|---|---|---|---|---|
| [27] | Fair | Good | Good | Poor | Good | Good | Moderate |
| [28] | Fair | Good | Good | Poor | Good | Good | Moderate |
| [29] | Good | Good | Good | Good | Good | Good | Strong |
| [30] | Fair | Fair | Good | Poor | Good | Good | Moderate |
| [31] | Fair | Good | Good | Good | Good | Good | Strong |
| [32] | Fair | Good | Good | Poor | Good | Good | Moderate |
| [33] | Poor | Good | Good | Poor | Good | Good | Weak |
| [34] | Poor | Fair | Good | Poor | Good | Poor | Weak |
| [35] | Fair | Good | Good | Good | Good | Good | Strong |
| [36] | Good | Good | Good | Fair | Good | Fair | Strong |
| [37] | Fair | Good | Good | Fair | Good | Good | Strong |
| [38] | Good | Fair | N/a | Poor | Good | Good | Moderate |
| [39] | Poor | Good | Good | Good | Good | Good | Moderate |
| [40] | Good | Fair | Good | Poor | Good | Fair | Moderate |
| [42] | Poor | Fair | N/a | Poor | Good | Good | Weak |
| [41] | Good | Good | Good | Poor | Good | Good | Moderate |
| [43] | Poor | Good | Good | Poor | Good | Good | Weak |
| [44] | Good | Good | Good | Fair | Good | Fair | Strong |
| [45] | Fair | Good | Good | Poor | Good | Good | Moderate |
| [46] | Fair | Good | Good | Fair | Good | Fair | Strong |
| [47] | Poor | Fair | N/a | Poor | Good | Good | Weak |
| [48] | Good | Good | Good | Fair | Good | Good | Strong |
| [49] | Good | Fair | N/a | Poor | Good | Fair | Moderate |
| [50] | Good | Good | Good | Fair | Good | Good | Strong |
| [51] | Fair | Good | Good | Poor | Good | Good | Moderate |
| [53] | Poor | Good | Good | Fair | Good | Good | Moderate |
| [52] | Fair | Good | Good | Poor | Good | Poor | Weak |
| [54] | Fair | Good | Good | Fair | Good | Good | Strong |
| [55] | Poor | Good | Good | Poor | Good | Good | Weak |
| [56] | Poor | Good | Good | Poor | Good | Poor | Weak |
| [21] | Fair | Good | Good | Fair | Good | Fair | Strong |
| [57] | Poor | Good | Good | Fair | Good | Good | Moderate |
| [58] | Poor | Good | Good | Fair | Good | Good | Moderate |
| [59] | Good | Good | Good | Good | Good | Good | Strong |
| [60] | Fair | Fair | Good | Fair | Good | Good | Strong |
| [61] | Good | Good | Good | Fair | Good | Good | Strong |
| [62] | Fair | Good | Good | Poor | Good | Good | Moderate |
| [63] | Good | Good | Good | Poor | Good | Good | Moderate |
| Authors | Cognitive Instruments Used | Outcomes | Main Categories | Effects of the Intervention on Executive Function Domains | Effects of the Intervention on Memory Domains | Effects of the Intervention on Global Performance |
|---|---|---|---|---|---|---|
| [27] | MMSE | Global performance (final score) | GP | N/a | N/a | Not improved |
| [28] | (1) VCAP; (2) Switching Task and Spatial Working Memory Task | Proc. speed, vocabulary, fluid reasoning, and working memory | EF | Improved | N/a | N/a |
| [29] | (1) ZAVEN; (2) Letter Fluency Test; (3) TMT; (4) VST and CVLT; (5) TAP; (6) Logical Memory Task; (7) DSST | Global performance, executive function, memory and proc. Speed | GP, EF, MF | Improved | Not improved | Improved |
| [30] | (1) RAVLT; (2) COWAT; (3) Animal Fluency Test | Verbal memory and verbal fluency | EF and MF | Improved | Improved | N/a |
| [31] | ACE-R | Attention, memory, verbal fluency, language and visual spatial skills | EF and MF | Improved | Improved | N/a |
| [32] | (1) VFT; (2) TUG + Cognitive Test; (3) SPMT; (4) TMT | Verbal fluency, short-term memory, executive function | EF and MF | Improved | Not improved | N/a |
| [33] | CASI 2.0 | Global performance score | GP | N/a | N/a | Improved |
| [34] | (1) CDR; (2) FUCAS; (3) TEA; (4) TMT; (5) RAVLT; (6) VFT | Attention, memory, orientation, verbal fluency | EF and MF | Improved | Improved | N/a |
| [35] | (1) DSST; (2) DMT; (3) Stroop; (4) TMT | Proc. speed, working memory, visuospatial processing, attention | EF | Improved | N/a | N/a |
| [36] | (1) Dual Task; (2) N-Back Task; (3) Digit Stroop Task; (4) MoCA | Working memory, attention, proc. speed, reaction time, global performance score (MoCA) | EF and GP | Improved | N/a | Not improved |
| [37] | COGTEL | Prospective memory, verbal short-term memory, long-term memory, working memory, verbal fluency, inductive reasoning | GP, EF, MF | Not improved | Improved | Improved |
| [38] | (1) Symbol Digit Modalities Test; (2) Cart Sorting Test; (3) Colour and Word Inference Test; (4) Buschke Selective Reminding Test; (5) MCGCF; (6) VFT; (7) Memory (Medical College of Georgia Complex Figure); (8) Auditory Consonant Trigram Test | Proc. speed, verbal memory, visual memory, verbal fluency and attention | EF and MF | Improved | Improved | N/a |
| [39] | (1) MoCA; (2) Flanker Task Test | Global performance score (MoCA) and proc. speed | EF and GP | Improved | N/a | Improved |
| [40] | (1) Motor Screening Test; (2) PAL Test; (3) RVT Test | Episodic memory, visual attention, proc. speed | EF and MF | Improved | Improved | N/a |
| [42] | (1) RAVLT; (2) WMS—LM; (3) WAIS III Digit Span; (4) TMT—A and BVMT | Verbal memory, verbal episodic memory, working memory, visual memory | EF and MF | Marginals improvements | Improved | N/a |
| [41] | Computerised Modified Stroop Test | Proc. speed | EF | Improved | N/a | N/a |
| [43] | Stroop Test | Proc. speed | EF | Improved | N/a | N/a |
| [44] | (1) MoCA; (2) Sprawnosci Operacyjnej Test; (3) TMT B; (4) DST and DST Backwards | Global performance, executive function, auditory attention, working memory | EF, MF, GP | Improved | Improved | Improved |
| [45] | (1) TMT-A and TMT-B; (2) DST Forwards and Backwards | Executive function and memory function | EF and MF | Improved | Not improved | N/a |
| [46] | (1) MoCA; (2) EXIT 25; (3) CCVLT; (4) CWT; (5) Spacial N-Back Task Test | Global performance score (MoCA), verbal memory, attention, working memory | EF, MF, GP | Improved | Improved | Improved |
| [47] | (1) NIHTB-CB Fluid Cognition; (2) NIHTB-CB Crystallised Cognition | Attention, working memory, episodic memory proc. speed, vocabulary and reading recognition | EF and MF | Improved | Not improved | N/a |
| [48] | (1) VLMT; (2) CERAD; (3) STROOP Interference; (4) Digit Span—Forwards and Backwards; (5) Semantic Fluency Test | Memory recall, executive control, working memory, and verbal fluency | EF and MF | Not improved | Not improved | N/a |
| [49] | MoCa | Global performance score | GP | N/a | N/a | Improved |
| [50] | (1) MoCA; (2) FAB | Global performance and executive function | EF and GP | Improved | N/a | Improved |
| [51] | (1) Modified MMSE—3MS; (2) TMT | Registration and recall, long-term memory, orientation, attention, verbal fluency and understanding, word retrieval, visuospatial skills, abstract meaning, proc. speed | EF and MF | Not improved | Not improved | N/a |
| [52] | (1) RAVLT; (2) TAP | Short- and long-term memory and attention | EF and MF | Improved | Improved | N/a |
| [53] | (1) TMT-A; (2) TMT-B; (3) MoCA | Global performance, executive function and working memory | EF and GP | Improved | N/a | Improved |
| [54] | (1) MMSE; (2) Logical Memory IIA; (3) TMT; (4) DSST | Global performance score (MMSE), long- and short-term memory, attention, proc. speed | EF, MF, GP | Not improved | Improved | Not improved |
| [55] | (1) TAP 2.3; (2) N-Back Task; (3) Simple Reaction-Time Task; (4) Response Inhibition Talk | Attention, working memory, proc. speed, reaction time, response inhibition | EF | Improved | N/a | N/a |
| [56] | (1) TMT; (2) Computerised Modified Stroop Task; (3) Rey Words Test; (4) 2-Back Test | Executive function, verbal memory, working memory | EF and MF | Improved | Not improved | N/a |
| [21] | Serial Subtraction during a Two-Minute Walk | Working memory and proc. speed | EF | Improved | N/a | N/a |
| [57] | CNS Vital Signs | Verbal memory, visual memory, proc. speed, attention and reaction times | EF and MF | Improved | Not improved | N/a |
| [58] | (1) TMT—A and B; (2) GOGSTATE Two Back: (3) HVLT-R; (4) ROCF; (5) CNTABRTTT | Attention, working memory, proc. speed, reaction time, memory | EF and MF | Not improved | Not improved | N/a |
| [59] | EXAMINER Cognitive Battery—EF Domains | Working memory, switching flexibly between tasks, deliberately overriding dominant/prepotent responses | EF | Improved | N/a | N/a |
| [60] | (1) Task-Switching Paradigm; (2) N-Back Test | Working memory and proc. speed | EF | Improved | N/a | N/a |
| [61] | Total FAS, Animals, and Verbs | Verbal fluency | EF | Improved | N/a | N/a |
| [62] | TMPT—25-Hole Peg Test | Proc. speed and visual attention | EF | Improved | N/a | N/a |
| [63] | Tasks on a Specific Software | Processing speed, spatial ability, working memory, language ability, associative memory | EF and MF | Improved | Not improved | N/a |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tinôco, M.A.; Nascimento, M.d.M.; Marques, A.; Gouveia, É.R.; Miguel, S.; Santos, F.; Ihle, A. The Relationship between Physical Fitness and Cognitive Functions in Older People: A Systematic Review. Sustainability 2023, 15, 16314. https://doi.org/10.3390/su152316314
Tinôco MA, Nascimento MdM, Marques A, Gouveia ÉR, Miguel S, Santos F, Ihle A. The Relationship between Physical Fitness and Cognitive Functions in Older People: A Systematic Review. Sustainability. 2023; 15(23):16314. https://doi.org/10.3390/su152316314
Chicago/Turabian StyleTinôco, Maria Antonieta, Marcelo de Maio Nascimento, Adilson Marques, Élvio Rúbio Gouveia, Salvador Miguel, Francisco Santos, and Andreas Ihle. 2023. "The Relationship between Physical Fitness and Cognitive Functions in Older People: A Systematic Review" Sustainability 15, no. 23: 16314. https://doi.org/10.3390/su152316314
APA StyleTinôco, M. A., Nascimento, M. d. M., Marques, A., Gouveia, É. R., Miguel, S., Santos, F., & Ihle, A. (2023). The Relationship between Physical Fitness and Cognitive Functions in Older People: A Systematic Review. Sustainability, 15(23), 16314. https://doi.org/10.3390/su152316314