
Current and Future Sustainability Traits of Digestive Endoscopy


Abstract
:1. Introduction
- Gastroenterology (digestive endoscopy);
- Orthopaedic surgery (arthroscopy);
- Pulmonology and thoracic surgery (bronchoscopy and mediastinoscopy);
- Urology (cystoscopy and urethroscopy);
- Gynaecology (hysteroscopy);
- Various types of surgery (laparoscopy);
- Otolaryngology (laryngoscopy) [15].
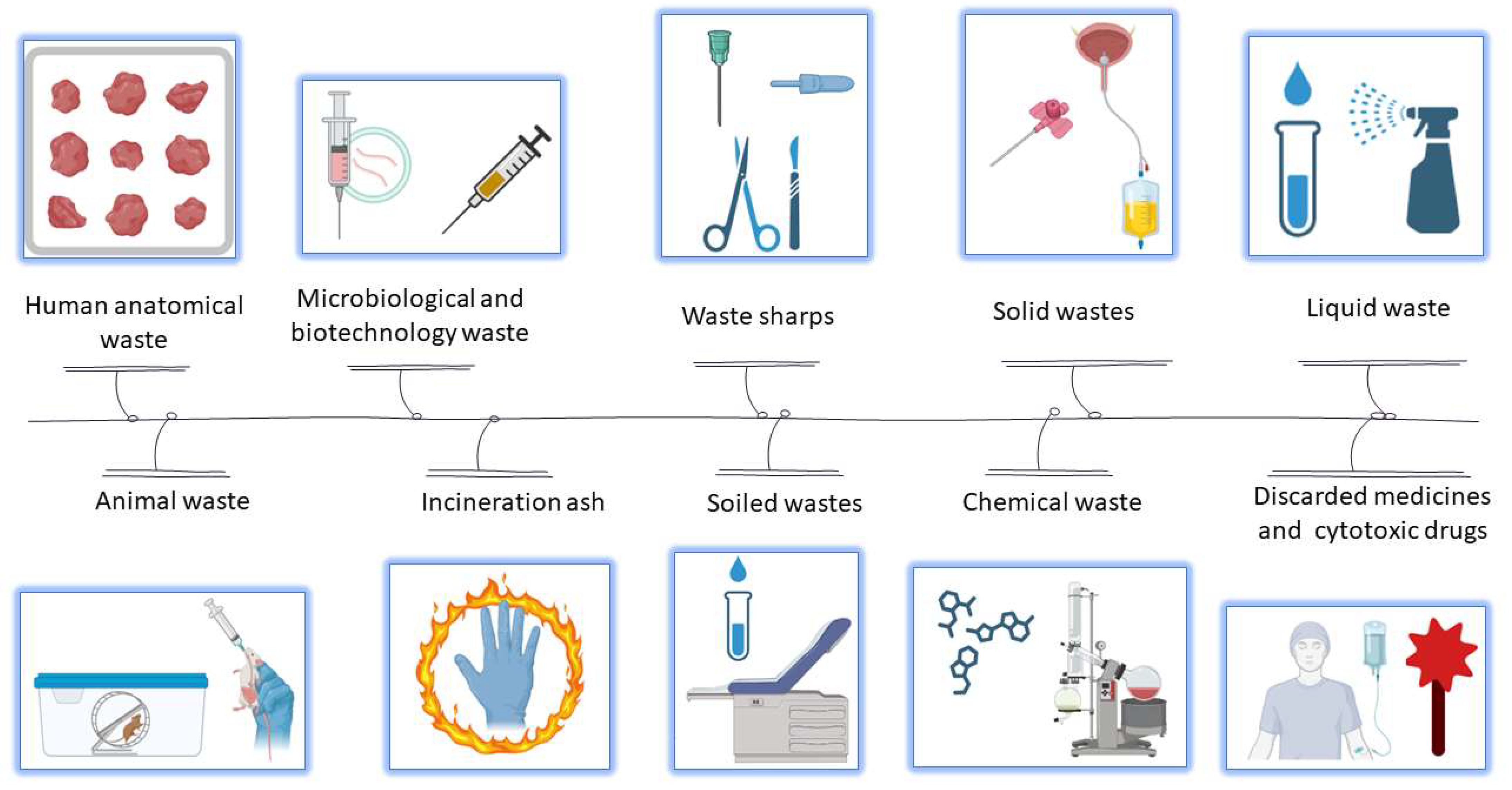
2. Last Stage of a Medical/Pharmaceutical Product
- Elimination of waste generation;
- Reuse of waste;
- Emphasizing waste recycling;
- Energy recovery;
- Compliant disposal.
- A lack of coherent, clear legislation with simple procedures, easily applicable by both citizens and medical and pharmaceutical units;
- High costs are incurred in the collection of sanitary waste from patients, pharmacies, and medical units;
- Personnel responsible for the initial selection of this waste face a lack of sufficient information.
- Effective and complex waste reduction policies and the establishment of clear responsibilities for the personnel who handle it;
- A continuous information system for nurses and pharmacists regarding the effective management of the resulting waste;
- Awareness of patients and health personnel regarding the importance of correct management of medical-pharmaceutical waste;
- Removing or reducing the financial impact of waste storage;
- Risk identification, etc. [26].
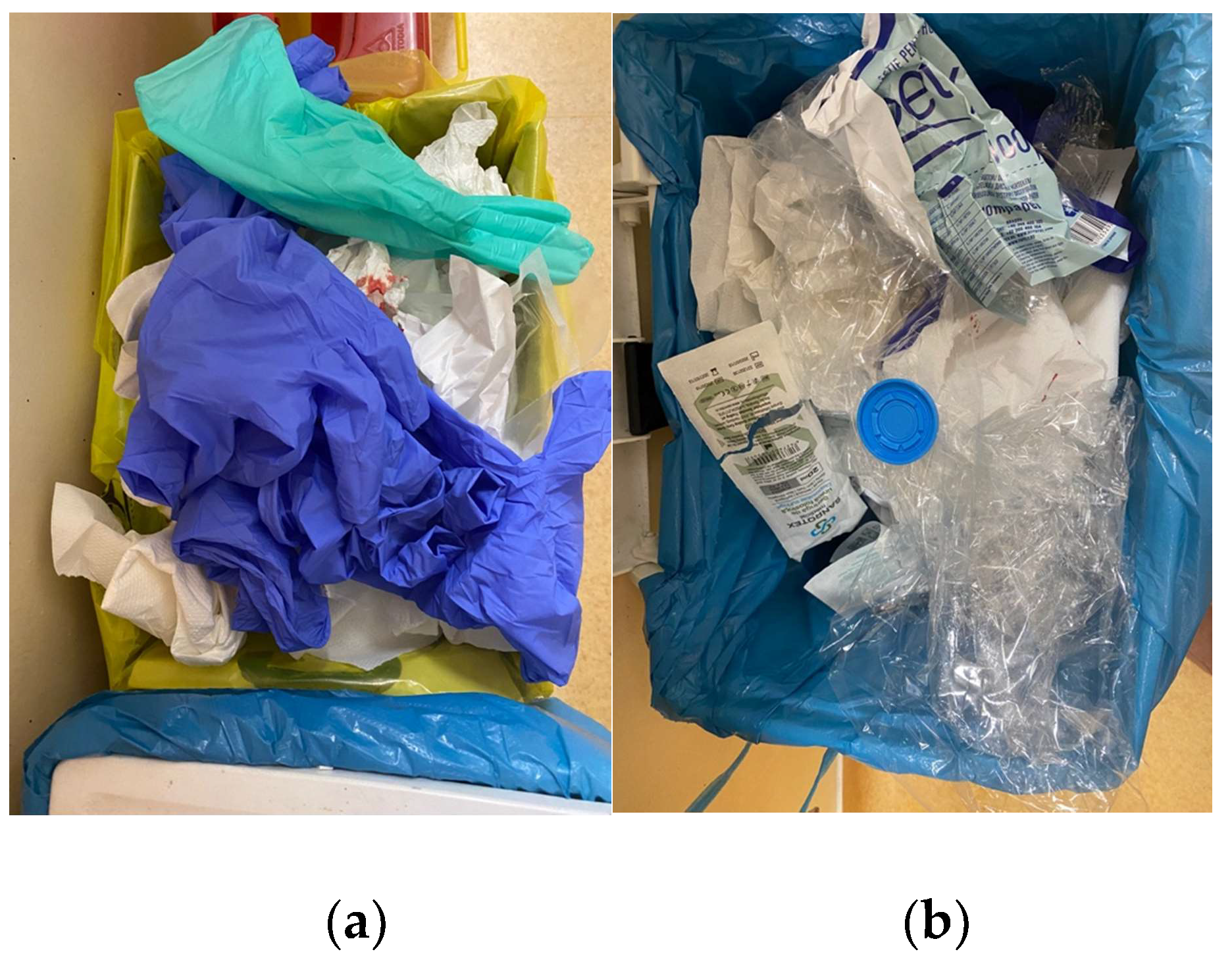
The Context of Waste and Packaging Materials in the Endoscopy Suite
3. Means and Ways Digestive Endoscopy Produces Pollution
3.1. Air and Water Pollution
3.2. Pollution Produced through the Reprocessing Sequence
3.3. Chemicals Used in Disinfection Process of Digestive Endoscopes
- Glutaraldehyde (2.4–3.5%), which is not expensive, and it is highly effective and readily available, with practically no damage to the endoscopes. Unfortunately, glutaraldehyde elicits adverse effects on individuals involved in its manipulation, and substantial reductions in atmospheric levels of glutaraldehyde have been recommended. Due to this major disadvantage, this agent was withdrawn from use in some countries. Also, its disposal is a concern, and it should not be directly emptied into the sewage system [51].
- Orthophthal aldehyde (OPA) (0.55–0.60%) is a more stable alternative disinfectant that has a lower vapor pressure than glutaraldehyde, but it is more expensive. It has a barely perceptible odor. It is advisable that sprays, mists, and aerosols are not used during the use of OPA. All OPA solutions must be neutralized to inactivate the disinfectant before disposal into the sewer [53].
- Peracetic acid is a highly effective disinfectant that may prove to be a suitable alternative to glutaraldehyde or OPA. It is considered a sustainable disinfectant because it decomposes in oxygen, water, and biodegradable acetic acid, thus not affecting the environment [54,55] (Table 2). Thus, it offers many sustainability advantages, like decomposition in environmentally friendly compounds, as mentioned above; toxic by-products are not generated during its use; and due to its potency, it is resource efficient [56].
- Hydrogen peroxide (2–7.5%), also used in the terminal disinfection of endoscopes, is usually found in a dual formula that comprises vaporized hydrogen peroxide and ozone. It assures high-level disinfection of all types of digestive endoscopes, including duodenoscopes [57]. Hydrogen peroxide is largely considered eco-friendly as it decomposes in water and oxygen (Table 2). However, in high amounts, hydrogen peroxide can be toxic if ingested, inhaled, or through contact with the skin or eyes, or if it is evacuated into the water, especially for phytoplankton. The toxicity level of exposure varies with the duration and exposure dose [58].
- Hypochlorous acid (HOCL) is basically a weak acid that results when chlorine is dissolved into water (Table 2). Due to this behaviour, it becomes clear that it represents no harm for the medical personnel and can be disposed of with no risk of producing toxic waste. Thus, hypochlorous acid 650–675 ppm is another potent disinfectant. It was declared by WHO, in 2021 during the Corona Virus pandemic, as the most potent and environmentally safe disinfectant available with a wide range of efficacy against many human pathogens, including the SARS-CoV-2 coronavirus, and it can also be used in digestive endoscopy [59]. The beneficial effects of HOCL as well as its safety for medical personnel and the environment depend on the purity of the solution and the avoidance of contaminating molecular species of aqueous chlorine (such as hypochlorite a.s.o.) [60]. HOCL can be degraded into an anion called hypochlorite (CIO-). Usually, this compound can be combined with cations to form salts like sodium and calcium hypochlorite (NaClO). These hypochlorite solutions (i.e., bleach, as commonly known and widely used as a whitening, cleaning, and disinfectant agent) represent toxic compounds, which prompts the usage of personal protective equipment and special disposal measures, as they are an environmental hazard. If the manufacturing process is not properly performed according to strict regulations, HOCl products may lack stability in storage, lose part of their antiseptic efficacy, or even cause toxicity through contaminants that can be harmful to the environment and people [61,62].
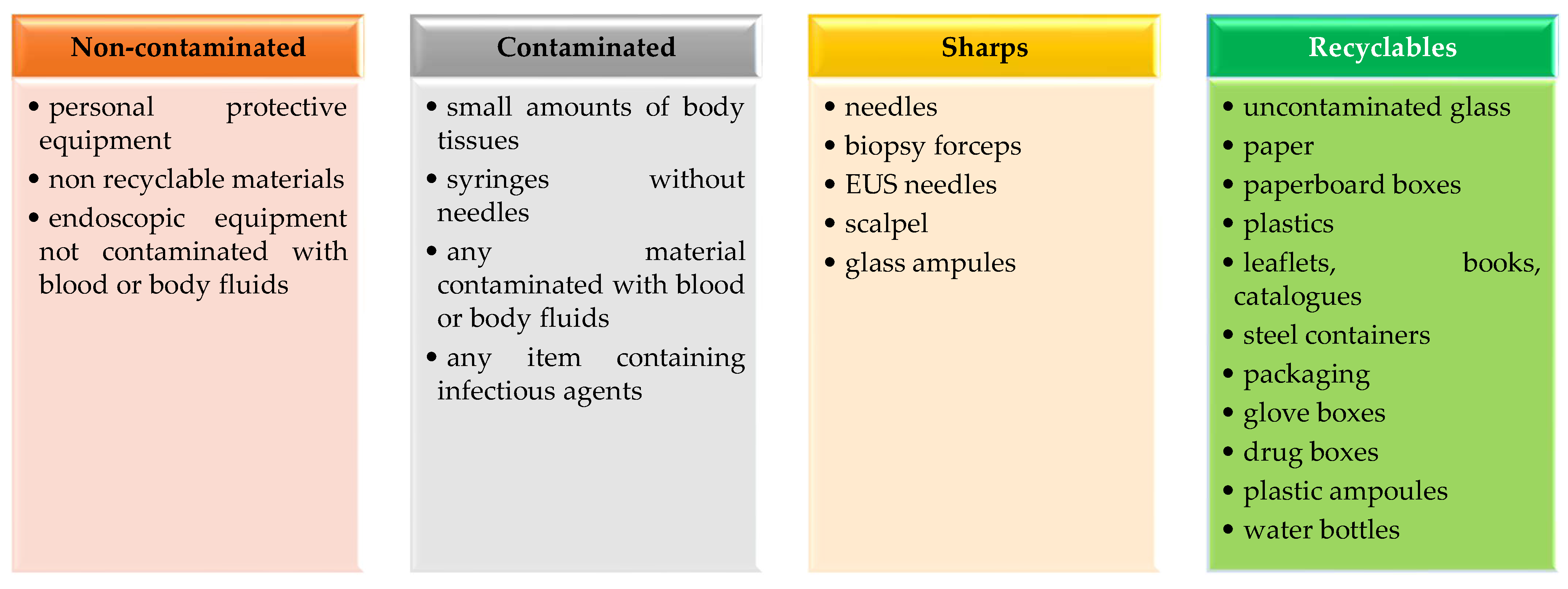
3.4. Waste through Disposable Materials and Instruments
- Non contaminated/regular waste;
- Contaminated waste;
- Sharps;
- Recyclable waste.
3.5. Single-Use Devices and Endoscopes versus Reusable Ones
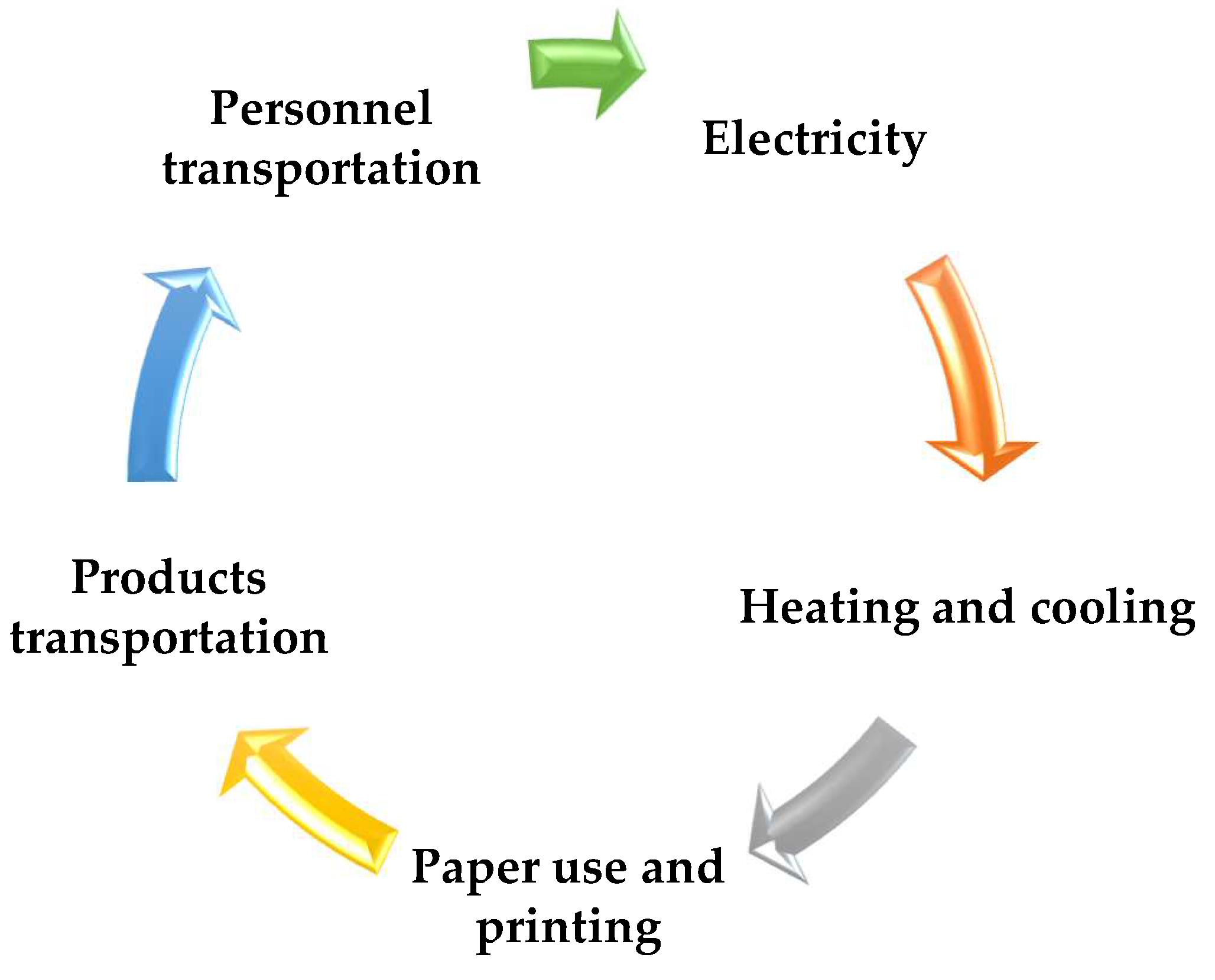
3.6. Other Sources of Increased Carbon Footprint from Digestive Endoscopy
4. What Can We Do to Increase Digestive Endoscopy Sustainability?
- Use eco-friendly substances, materials, and devices;
- Reduce the unnecessary consumption of water and all possible materials, devices, energy, etc.;
- Reuse those components that can be safely reinserted in the endoscopic circuit;
- Recycle everything that is possible.
- Raising perceptions among medical personnel and the auxiliary team about the risks and long-term implications of waste and pollution;
- Establishing clear standards for indoor air quality in the endoscopy unit and performing specific measurements for air quality checks, maybe even CO2 monitoring devices;
- Performing all the disinfection stages of the endoscopes in a dedicated room or space with proper ventilation or even with air extraction devices;
- Making more efforts to reduce the waste quantity;
- Better understanding of sorting out the waste;
- Improving the standards of disposal practices;
- Stewardship towards safer and greener methods for the sterilization of medical devices (autoclaving, etc.) over incineration;
- Work education of the personnel regarding hazards associated with manoeuvring, storing, transporting, and processing wastes;
- Following guidelines;
- Promoting continuously wise resource distribution and safer practice.
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Russell, V.S. Pollution: Concept and Definition. Biol. Conserv. 1974, 6, 157–161. [Google Scholar] [CrossRef]
- Ukaogo, P.O.; Ewuzie, U.; Onwuka, C. V Environmental Pollution: Causes, Effects, and the Remedies. In Microorganisms for Sustainable Environment and Health; Chowdhary, P., Raj, A., Verma, D., Akhter, Y.B.T.-M., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 419–429. [Google Scholar]
- Perera, F. Pollution from Fossil-Fuel Combustion Is the Leading Environmental Threat to Global Pediatric Health and Equity: Solutions Exist. Int. J. Environ. Res. Public Health 2017, 15, 16. [Google Scholar] [CrossRef] [PubMed]
- Fayomi, G.U.; Mini, S.E.; Fayomi, O.S.I.; Oyeleke, O.; Omole, D.O.; Akinwumi, I.I. Overview of Industrial Pollution Activities and Its Curbing Mechanisms. IOP Conf. Ser. Mater. Sci. Eng. 2019, 640, 012097. [Google Scholar] [CrossRef]
- Matei, O.-R.; Dumitrescu Silaghi, L.; Dunca, E.-C.; Bungau, S.G.; Tit, D.M.; Mosteanu, D.-E.; Hodis, R. Study of Chemical Pollutants and Ecological Reconstruction Methods in the Tismana I Quarry, Rovinari Basin, Romania. Sustainability 2022, 14, 7160. [Google Scholar] [CrossRef]
- Tit, D.M.; Bungau, S.G.; Nistor-Cseppento, D.C.; Copolovici, D.M.; Buhas, C.L. Disposal of Unused Medicines Resulting from Home Treatment in Romania. J. Environ. Prot. Ecol. 2016, 17, 1425–1433. [Google Scholar]
- Prada, M.; Prada, I.F.; Cristea, M.; Popescu, D.E.; Bungău, C.; Aleya, L.; Bungău, C.C. New Solutions to Reduce Greenhouse Gas Emissions through Energy Efficiency of Buildings of Special Importance—Hospitals. Sci. Total Environ. 2020, 718, 137446. [Google Scholar] [CrossRef]
- Bungau, C.C.; Bungau, T.; Prada, I.F.; Prada, M.F. Green Buildings as a Necessity for Sustainable Environment Development: Dilemmas and Challenges. Sustainability 2022, 14, 13121. [Google Scholar] [CrossRef]
- Bungau, S.; Tit, D.M.; Behl, T.; Aleya, L.; Zaha, D.C. Aspects of Excessive Antibiotic Consumption and Environmental Influences Correlated with the Occurrence of Resistance to Antimicrobial Agents. Curr. Opin. Environ. Sci. Heal. 2021, 19, 100224. [Google Scholar] [CrossRef]
- Behl, T.; Kaur, I.; Sehgal, A.; Singh, S.; Sharma, N.; Bhatia, S.; Al-Harrasi, A.; Bungau, S. The Dichotomy of Nanotechnology as the Cutting Edge of Agriculture: Nano-Farming as an Asset versus Nanotoxicity. Chemosphere 2022, 288, 132533. [Google Scholar] [CrossRef]
- Capon, T.; Malik, A.; Pencheon, D.; Weisz, H.; Lenzen, M. Health Care Has a Huge Environmental Footprint, Which Then Harms Health. This Is a Matter of Ethics. Available online: https://theconversation.com/health-care-has-a-huge-environmental-footprint-which-then-harms-health-this-is-a-matter-of-ethics-142651 (accessed on 1 September 2023).
- Padmanabhan, K.K.; Barik, D. Health Hazards of Medical Waste and Its Disposal. In Energy from Toxic Organic Waste for Heat and Power Generation; Woodhead Publishing: Cambridge, UK, 2019; pp. 99–118. [Google Scholar]
- Moore, L.E. The Advantages and Disadvantages of Endoscopy. Clin. Tech. Small Anim. Pract. 2003, 18, 250–253. [Google Scholar] [CrossRef]
- Baddeley, R.; de Santiago, E.R.; Maurice, J.; Siddhi, S.; Dhar, A.; Thomas-Gibson, S.; Hayee, B. Sustainability in Gastrointestinal Endoscopy. Lancet. Gastroenterol. Hepatol. 2022, 7, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Boese, A.; Wex, C.; Croner, R.; Liehr, U.B.; Wendler, J.J.; Weigt, J.; Walles, T.; Vorwerk, U.; Lohmann, C.H.; Friebe, M.; et al. Endoscopic Imaging Technology Today. Diagnostics 2022, 12, 1262. [Google Scholar] [CrossRef] [PubMed]
- Gulati, S.; Patel, M.; Emmanuel, A.; Haji, A.; Hayee, B.; Neumann, H. The Future of Endoscopy: Advances in Endoscopic Image Innovations. Dig. Endosc. 2020, 32, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Almomani, H.; Obaidat, M.; Khazaleh, A.; Muneizel, O.; Afyouni, N.; Fayyad, S. Review of Medical Waste Management in Jordanian Health Care Organisations. Br. J. Healthc. Manag. 2019, 25, 1–8. [Google Scholar] [CrossRef]
- Eren, E.; Tuzkaya, U.R. Occupational Health and Safety-Oriented Medical Waste Management: A Case Study of Istanbul. Waste Manag. Res. 2019, 37, 876–884. [Google Scholar] [CrossRef]
- Fadaei, A. Comparison of Medical Waste Management Methods in Different Countries: A Systematic Review. Rev. Environ. Health 2023, 38, 339–348. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Safe Management of Waste from Healthcare Activity; WHO: Geneva, Switzerland, 2014; pp. 1–242. [Google Scholar]
- Mbongwe, B.; Mmereki, B.T.; Magashula, A. Healthcare Waste Management: Current Practices in Selected Healthcare Facilities, Botswana. Waste Manag. 2008, 28, 226–233. [Google Scholar] [CrossRef]
- Singh, Z.; Bhalwar, R.; Jayaram, J.; Tilak, V.W. An Introduction to Essentials of Bio-Medical Waste Management. Med. J. Armed Forces India 2001, 57, 144–147. [Google Scholar] [CrossRef]
- Bungau, S.; Bungau, C.; Tit, D.M. Studies on the Last Stage of Product Lifecycle Management for a Pharmaceutical Product. J. Environ. Prot. Ecol. 2015, 16, 56–62. [Google Scholar]
- Kwikiriza, S.; Stewart, A.G.; Mutahunga, B.; Dobson, A.E.; Wilkinson, E. A Whole Systems Approach to Hospital Waste Management in Rural Uganda. Front. Public Heal 2019, 7, 136. [Google Scholar] [CrossRef]
- Preparation of National Health-Care Waste Management Plans in Sub-Saharan Countries Guidance Manual Secretariat of the Basel Convention and World Health Organization. Available online: https://apps.who.int/iris/bitstream/handle/10665/43118/924154662X.pdf?sequence=1 (accessed on 2 September 2023).
- Bungau, S.G.; Suciu, R.N.; Bumbu, A.G.; Cioca, G.; Tit, D.M. Study on Hospital Waste Management in Medical Rehabilitation Clinical Hospital, Baile Felix. J. Environ. Prot. Ecol. 2015, 16, 980–987. [Google Scholar]
- Pyhälä, M.; Zandaryaa, S.; Andresmaa, E.; Korsjukov, M.; Reisner, R.; Susanne Boutrup, D.; Päivi Fjäder, F.; Mehtonen, J.; Äystö, L.; Hein, A.; et al. Pharmaceuticals in the Aquatic Environment of the Baltic Sea Region: A Status Report. UNESCO: Paris, France, 2017. [Google Scholar]
- Chisholm, J.M.; Zamani, R.; Negm, A.M.; Said, N.; Abdel Daiem, M.M.; Dibaj, M.; Akrami, M. Sustainable Waste Management of Medical Waste in African Developing Countries: A Narrative Review. Waste Manag. Res. 2021, 39, 1149–1163. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, S.; Dhar, A.; Baddeley, R.; Donnelly, L.; Haddock, R.; Arasaradnam, R.; Coulter, A.; Disney, B.R.; Griffiths, H.; Healey, C.; et al. Green Endoscopy: British Society of Gastroenterology (BSG), Joint Accreditation Group (JAG) and Centre for Sustainable Health (CSH) Joint Consensus on Practical Measures for Environmental Sustainability in Endoscopy. Gut 2023, 72, 12–26. [Google Scholar] [PubMed]
- de Melo, S.W.; Taylor, G.L.; Kao, J.Y. Packaging and Waste in the Endoscopy Suite. Tech. Innov. Gastrointest. Endosc. 2021, 23, 371–375. [Google Scholar] [CrossRef]
- Choi, H.H.; Cho, Y.-S. Endoscope Reprocessing: Update on Controversial Issues. Clin. Endosc. 2015, 48, 356–360. [Google Scholar] [CrossRef]
- Larsen, S.; Russell, R.V.; Ockert, L.K.; Spanos, S.; Travis, H.S.; Ehlers, L.H.; Mærkedahl, A. Rate and Impact of Duodenoscope Contamination: A Systematic Review and Meta-Analysis. EClinicalMedicine 2020, 25, 100451. [Google Scholar] [CrossRef]
- Brown, G.; Ong, A.; Juliebø-Jones, P.; Davis, N.F.; Skolarikos, A.; Somani, B. Single-Use Ureteroscopy and Environmental Footprint: Review of Current Evidence. Curr. Urol. Rep. 2023, 24, 281–285. [Google Scholar] [CrossRef]
- Agrawal, D.; Shoup, V.; Montgomery, A.; Wosik, J.; Rockey, D.C. Disposal of Endoscopic Accessories After Use: Do We Know and Do We Care? Gastroenterol. Nurs. 2017, 40, 13–18. [Google Scholar] [CrossRef]
- Vaccari, M.; Tudor, T.; Perteghella, A. Costs Associated with the Management of Waste from Healthcare Facilities: An Analysis at National and Site Level. Waste Manag. Res. 2018, 36, 39–47. [Google Scholar] [CrossRef]
- Haddock, R.; Gopfert, A.; van Hove, M.; Stableforth, W. The Case for Sustainable Endoscopy as a Professional Priority. Tech. Innov. Gastrointest. Endosc. 2021, 23, 337–343. [Google Scholar] [CrossRef]
- Vaziri, S.M.; Rezaee, B.; Monirian, M.A. Utilizing Renewable Energy Sources Efficiently in Hospitals Using Demand Dispatch. Renew. Energy 2020, 151, 551–562. [Google Scholar] [CrossRef]
- Coelho, P.M.; Corona, B.; ten Klooster, R.; Worrell, E. Sustainability of Reusable Packaging–Current Situation and Trends. Resour. Conserv. Recycl. X 2020, 6, 100037. [Google Scholar] [CrossRef]
- Donnelly Endoscopy, L. Green Endoscopy: Practical Implementation. Frontline Gastroenterol. 2022, 13, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Ratcliff, A.; Burns, C.; Gwinnutt, C.L. The Contribution of Medical Nitrous Oxide to the Greenhouse Effect. Health Trends 1991, 23, 119–120. [Google Scholar]
- World Health Organization. Regional Office for Europe. Evolution of WHO Air Quality Guidelines: Past, Present and Future. Available online: https://apps.who.int/iris/handle/10665/341912 (accessed on 2 September 2023).
- Nechifor, A.C.; Cotorcea, S.; Bungău, C.; Albu, P.C.; Pașcu, D.; Oprea, O.; Grosu, A.R.; Pîrțac, A.; Nechifor, G. Removing of the Sulfur Compounds by Impregnated Polypropylene Fibers with Silver Nanoparticles-Cellulose Derivatives for Air Odor Correction. Membranes 2021, 11, 256. [Google Scholar] [CrossRef]
- Glevitzky, M.; Aleya, L.; Vică, M.L.; Dumitrel, G.A.; Avram, M.; Tit, D.M.; Popa, M.; Popa, V.C.; Behl, T.; Bungau, S. Assessing the Microbiological Contamination along with Environmental Factors of Old Books in the 1490-Founded Bistrița Monastery, Romania. Environ. Sci. Pollut. Res. 2021, 28, 8743–8757. [Google Scholar] [CrossRef]
- Bungau, C.C.; Hanga Prada, F.I.; Bungau, T.; Bungau, C.; Bendea, G.; Prada, M.F. Web of Science Scientometrics on the Energy Efficiency of Buildings to Support Sustainable Construction Policies. Sustainability 2023, 15, 8772. [Google Scholar] [CrossRef]
- Bungău, C.C.; Prada, I.F.; Prada, M.; Bungău, C. Design and Operation of Constructions: A Healthy Living Environment-Parametric Studies and New Solutions. Sustainability 2019, 11, 6824. [Google Scholar] [CrossRef]
- Bang, C.S.; Lee, K.; Choi, J.H.; Soh, J.S.; Hong, J.Y.; Baik, G.H.; Kim, D.J. Ambient Air Pollution in Gastrointestinal Endoscopy Unit; Rationale and Design of a Prospective Study. Medicine 2018, 97, e13600. [Google Scholar] [CrossRef]
- Bang, C.S.; Lee, K.; Yang, Y.J.; Baik, G.H. Ambient Air Pollution in Gastrointestinal Endoscopy Unit. Surg. Endosc. 2020, 34, 3795–3804. [Google Scholar] [CrossRef]
- Sivananthan, A.; Glover, B.; Ayaru, L.; Patel, K.; Darzi, A.; Patel, N. The Evolution of Lower Gastrointestinal Endoscopy: Where Are We Now? Ther. Adv. Gastrointest. Endosc. 2020, 13, 2631774520979591. [Google Scholar] [CrossRef] [PubMed]
- Af Petersens, M.; Andersson Fenger-Krog, F.; Jakobsson, J.G. Workplace Exposure to Carbon Dioxide during Routine Laparoscopy—Is It Safe? F1000Research 2020, 9, 571. [Google Scholar] [CrossRef] [PubMed]
- Speer, T.; Alfa, M.; Jones, D.; Vickery, K.; Griffiths, H.; Sáenz, R.; LeMair, A. WGO Guideline-Endoscope Disinfection Update. J. Clin. Gastroenterol. 2023, 57, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.; Alfa, M.J. Cleaning and Disinfecting Gastrointestinal Endoscopy Equipment. In Clinical Gastrointestinal Endoscopy., 3rd, ed.; Chandrasekhara, V., Elmunzer, B.J., Khashab, M.A., Muthusamy, V.R.B.T.-C.G.E., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 32–50.e5. [Google Scholar]
- Endoscope Disinfection Update: A Guide to Resource-Sensitive Reprocessing. Available online: https://www.worldgastroenterology.org/UserFiles/file/guidelines/endoscope-disinfection-english-2019.pdf (accessed on 1 September 2023).
- Rutala, W.A.; Weber, D.J. Disinfection, Sterilization, and Control of Hospital Waste. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases; Elsevier Health Sciences: New York, NY, USA, 2015; pp. 3294–3309.e4. [Google Scholar]
- Wang, Y.-W.; Liao, M.-S.; Shu, C.-M. Thermal Hazards of a Green Antimicrobial Peracetic Acid Combining DSC Calorimeter with Thermal Analysis Equations. J. Therm. Anal. Calorim. 2015, 119, 2257–2267. [Google Scholar] [CrossRef]
- Carrasco, G.; Urrestarazu, M. Green Chemistry in Protected Horticulture: The Use of Peroxyacetic Acid as a Sustainable Strategy. Int. J. Mol. Sci. 2010, 11, 1999–2009. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, G.; Russell, A.D. Antiseptics and Disinfectants: Activity, Action, and Resistance. Clin. Microbiol. Rev. 1999, 12, 147–179. [Google Scholar] [CrossRef]
- Molloy-Simard, V.; Lemyre, J.L.; Martel, K.; Catalone, B.J. Elevating the Standard of Endoscope Processing: Terminal Sterilization of Duodenoscopes Using a Hydrogen Peroxide–Ozone Sterilizer. Am. J. Infect. Control 2019, 47, 243–250. [Google Scholar] [CrossRef]
- Mahaseth, T.; Kuzminov, A. Potentiation of Hydrogen Peroxide Toxicity: From Catalase Inhibition to Stable DNA-Iron Complexes. Mutat. Res. Rev. Mutat. Res. 2017, 773, 274–281. [Google Scholar] [CrossRef]
- World Health Organization. Cleaning and Disinfection of Environmental Surfaces in the Context of COVID-19. Available online: https://www.who.int/publications/i/item/cleaning-and-disinfection-of-environmental-surfaces-inthe-context-of-covid-19 (accessed on 3 September 2023).
- Busch, M.; Simic, N.; Ahlberg, E. Exploring the Mechanism of Hypochlorous Acid Decomposition in Aqueous Solutions. Phys. Chem. Chem. Phys. 2019, 21, 19342–19348. [Google Scholar] [CrossRef]
- World Health Organization. Applications for the 23rd WHO Expert Committee on Selection and Use of Essential Medicines Available for Public Review and Comment. Available online: https://www.who.int/news/item/19-04-2021-applications-for-the-23rd-who-expert-committee-on-selection-and-use-of-essential-medicines-available-for-public-review-and-comment (accessed on 1 September 2023).
- World Health Organization. Hypochlorous Acid (HOCl) for Disinfection, Antisepsis, and Wound Care in Core Categories 15.1, 15.2, and 13. Available online: https://cdn.who.int/media/docs/default-source/essential-medicines/2021-eml-expert-committee/applications-for-addition-of-new-medicines/a.18_hypochlorous-acid.pdf?sfvrsn=35222172_4 (accessed on 4 September 2023).
- Society of Gastroenterology Nurses and Associates. Guideline for Use of High-Level Disinfectants & Sterilants in the Gastroenterology Setting. Available online: https://www.sgna.org/portals/0/hld__final.pdf (accessed on 2 September 2023).
- Peery, A.F.; Crockett, S.D.; Murphy, C.C.; Lund, J.L.; Dellon, E.S.; Williams, J.L.; Jensen, E.T.; Shaheen, N.J.; Barritt, A.S.; Lieber, S.R.; et al. Burden and Cost of Gastrointestinal, Liver, and Pancreatic Diseases in the United States: Update 2018. Gastroenterology 2019, 156, 254–272.e11. [Google Scholar] [CrossRef]
- Namburar, S.; von Renteln, D.; Damianos, J.; Bradish, L.; Barrett, J.; Aguilera-Fish, A.; Cushman-Roisin, B.; Pohl, H. Estimating the Environmental Impact of Disposable Endoscopic Equipment and Endoscopes. Gut 2022, 71, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Gayam, S. Environmental Impact of Endoscopy: “Scope” of the Problem. Am. J. Gastroenterol. 2020, 115, 1931–1932. [Google Scholar] [CrossRef] [PubMed]
- Rizan, C.; Reed, M.; Bhutta, M.F. Environmental Impact of Personal Protective Equipment Distributed for Use by Health and Social Care Services in England in the First Six Months of the COVID-19 Pandemic. J. R. Soc. Med. 2021, 114, 250–263. [Google Scholar] [CrossRef] [PubMed]
- Bortoluzzi, F.; Sorge, A.; Vassallo, R.; Montalbano, L.M.; Monica, F.; La Mura, S.; Canova, D.; Checchin, D.; Fedeli, P.; Marmo, R.; et al. Sustainability in Gastroenterology and Digestive Endoscopy: Position Paper from the Italian Association of Hospital Gastroenterologists and Digestive Endoscopists (AIGO). Dig. Liver Dis. 2022, 54, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Endoscopes Evolve to Meet Increased Safety Demands. Available online: https://connectorsupplier.com/endoscopes-evolve-to-meet-increased-safety-demands/ (accessed on 3 September 2023).
- Pang, S.; England, R.W.; Solomon, A.; Hong, K.; Singh, H. Single-Use versus Reusable Endoscopes for Percutaneous Biliary Endoscopy with Lithotripsy: Technical Metrics, Clinical Outcomes, and Cost Comparison. J. Vasc. Interv. Radiol. 2022, 33, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Mouritsen, J.M.; Ehlers, L.; Kovaleva, J.; Ahmad, I.; El-Boghdadly, K. A Systematic Review and Cost Effectiveness Analysis of Reusable vs. Single-Use Flexible Bronchoscopes. Anaesthesia 2020, 75, 529–540. [Google Scholar] [CrossRef]
- Agrawal, D.; Tang, Z. Sustainability of Single-Use Endoscopes. Tech. Innov. Gastrointest. Endosc. 2021, 23, 353–362. [Google Scholar] [CrossRef]
- Petersen, B.T. Advantages of Disposable Endoscopic Accessories. Gastrointest. Endosc. Clin. N. Am. 2000, 10, 341–348. [Google Scholar] [CrossRef]
- Wolfsen, H.C. Advantages of Reusable Accessories. Gastrointest. Endosc. Clin. N. Am. 2000, 10, 349–359. [Google Scholar] [CrossRef]
- Schroeder, K.; Thompson, T.D.B.; Frith, K.; Pencheon, D. Sustainable Healthcare; Wiley-Blackwell: Hoboken, NJ, USA, 2012; ISBN 978-0470656716. [Google Scholar]
- Shrank, W.H.; Rogstad, T.L.; Parekh, N. Waste in the US Health Care System: Estimated Costs and Potential for Savings. JAMA 2019, 322, 1501–1509. [Google Scholar] [CrossRef]
- Komilis, D.; Katsafaros, N.; Vassilopoulos, P. Hazardous Medical Waste Generation in Greece: Case Studies from Medical Facilities in Attica and from a Small Insular Hospital. Waste Manag. Res. 2011, 29, 807–814. [Google Scholar] [PubMed]
- Bdour, A.; Altrabsheh, B.; Hadadin, N.; Al-Shareif, M. Assessment of Medical Wastes Management Practice: A Case Study of the Northern Part of Jordan. Waste Manag. 2007, 27, 746–759. [Google Scholar] [PubMed]
- Sepetis, A.; Zaza, P.N.; Rizos, F.; Bagos, P.G. Identifying and Predicting Healthcare Waste Management Costs for an Optimal Sustainable Management System: Evidence from the Greek Public Sector. Int. J. Environ. Res. Public Health 2022, 19, 9821. [Google Scholar] [PubMed]
- Lee, S.M.; Lee, D. Effective Medical Waste Management for Sustainable Green Healthcare. Int. J. Environ. Res. Public Health 2022, 19, 14820. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Spaulding Classification | Examples of Devices | Risk of Infection Transmission | Disinfection Level |
|---|---|---|---|
| Critical (enters tissues or vascular system) | Implants, scalpels, needles, other surgical instruments, etc. | High | Sterilization |
| Semi critical (touches mucous membranes) | Flexible endoscopes, endotracheal tubes | Medium | High-level |
| Noncritical (touches intact skin) | Stethoscopes, bed pans, etc. | Low | Intermediate or low |
| Disinfectant | Advantages | Disadvantages |
|---|---|---|
| Glutaraldehyde (3.5%) * | Over 30 years of use in medical sector Excellent biocidal activity Cheap | Healthcare personnel exposure Air pollution Water pollution (requires neutralization) |
| Ortho-phal-aldehyde (0.55%) | Fast acting Excellent microbiocidal activity (superior to GA) Better material compatibility | More expensive Healthcare personnel exposure Air pollution Water pollution (may require neutralization before exposure) |
| Peracetic acid | Short time of action even at low temperatures Environmentally friendly Compatibility with many materials | More expensive Can corrode some types of material Unstable when diluted Serious eye and skin damage at high concentration |
| Hydrogen peroxide | Active against a wide range of microorganism No disposal issues | Material compatibility issues |
| Health care personnel issues (excessive exposure may produce irreversible tissue damage, and vapours can severely affect the respiratory system) | ||
| Hypochlorous acid/hypochlorite | Cheap Efficient against many pathogens, including SarsCov2 | If turned into hypochlorite, it can corrode some types of material Hypochlorite solutions can cause health care issues |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilias, T.I.; Hocopan, C.S.; Brata, R.; Fratila, O. Current and Future Sustainability Traits of Digestive Endoscopy. Sustainability 2023, 15, 15872. https://doi.org/10.3390/su152215872
Ilias TI, Hocopan CS, Brata R, Fratila O. Current and Future Sustainability Traits of Digestive Endoscopy. Sustainability. 2023; 15(22):15872. https://doi.org/10.3390/su152215872
Chicago/Turabian StyleIlias, Tiberia Ioana, Cristian Sergiu Hocopan, Roxana Brata, and Ovidiu Fratila. 2023. "Current and Future Sustainability Traits of Digestive Endoscopy" Sustainability 15, no. 22: 15872. https://doi.org/10.3390/su152215872
APA StyleIlias, T. I., Hocopan, C. S., Brata, R., & Fratila, O. (2023). Current and Future Sustainability Traits of Digestive Endoscopy. Sustainability, 15(22), 15872. https://doi.org/10.3390/su152215872