Abstract
The study is directed towards the growing importance of active ageing (AA). Active ageing is a concept proposed in 1990 to recognise not only factors related to health care but also other factors influencing the ageing of individuals and populations. In the following years, as the needs of the ageing societies and the possibilities of meeting these needs increased, Healthy Ageing was defined. Active ageing is one of the areas of care for older people in the Decade for Healthy Ageing. In the study, we referred to the pillars of the AA strategy and the active ageing index (AAI) guidelines. Research on active ageing is gaining momentum in conjunction with pursuing the Sustainable Development Goals (SDG 2030 Agenda), especially in social inclusion. The aim of our study was to compare EU countries in terms of seniors’ subjective assessment of AA-related activities and to check whether the similarities and differences in the ratings of seniors from different countries changed in 2020 compared to 2018. As we did not want seniors to participate in a survey directly focused on AA, we chose the European Social Survey database (ESS is a cross-national, representative survey conducted every two years across Europe since 2001), ensuring that the sample was representative. We used questions not directly related to AA. We conducted the analysis by gender and two age groups (65–74 and 75+). In the analysis, we used Kaufman–Rousseeuw normalisation and Ward’s method for clustering. Our analysis resulted in four classifications in each study run. We identified groups of countries where respondents’ assessments are similar. In addition, we identified recurring patterns of behaviour corresponding to AA.
1. Introduction
Population ageing is a global phenomenon which has been observed for several years, and its significance in the socio-economic areas of life of individuals and entire societies is significantly increasing. At the same time, it becomes important to consider the concept of active and healthy ageing [1,2]. Based on the Eurostat population prediction, it should be expected that in 2050 (2100), in the European Union, elderly people (65+) will constitute 52% (57%) of the working-age population (29.5% and 31.2% of the total population, respectively) [3]. Among the ten countries with a population of more than 10 million in 2002, with a proportion of people over 60 in 2025, as many as eight are projected to be European countries [1]. Grześkowiak et al. [4] indicate that EU countries are in an advanced phase of ageing. These authors determined the double ageing index, the ageing index, and the old-age dependency ratio for European countries in 2018. The double ageing index represents an increase in the proportion of the population aged 80+ among the elderly. The highest value of this indicator was recorded for Spain and the lowest for Slovakia. The ageing index does not coincide with the previous index. The lowest value was recorded for Ireland and the highest in Italy, with nearly 169 grandparents for every 100 grandchildren. Apart from Ireland, the number of grandparents is lower than that of grandchildren in Cyprus, Luxembourg and Slovakia. In half of the EU countries, according to the values recorded for the old-age dependency ratio, there were at least 29.6 people of old age for every 100 people of working age. With an ageing population, it is necessary to counteract the observed stereotypes and marginalisation of older people (i.e., aimlessness and dependency, minor role, failing health, social withdrawal) in favour of active rather than passive people. Living longer should not exclude the possibility of participating in society according to an individual’s needs and abilities. As Cahill et al. write [5], we gain maturity and wisdom with age. At the same time, seniors should be guaranteed health care and safety [6]. Thus, the idea of an age-friendly country, i.e., one that is best adapted to the needs of older people, was born. In 2011, 55% of Europeans aged 55 and over said they lived in an age-friendly country [7] and 67% said their local area could be considered age-friendly [7]. The observed increasing activity of the elderly is the result of improved well-being, independence and mobility [8].
The Healthy Ageing Strategy is taking action to preserve well-being in older age [2]. The main direction of this worldview is to develop and maintain functional efficiency for enabling well-being in older age. It also includes Active Ageing, which is focused on three pillars: health, participation and safety of seniors. Healthy and active ageing activities are intertwined and determine the power of taking action under one program based on the effects of the other program. In the tasks carried out in Healthy Aging, the impact of the need to take action and stimulate the support of older people in an ageing society is much more visible. For this reason, WHO introduced the Decade of Health Ageing (2020–2030). This program aims to increase the functional efficiency of older people, i.e., the ability to meet basic needs and to make decisions; mobility; building and maintaining relationships; social participation [9]. For this reason, the topics described in the AA strategy and the indicators described in the AAI, which we have chosen, answer many questions related to assessing the problems identified in the Decade of Healthy Ageing.
The primary assumption of the SDGs (Sustainable Development Goals) is to prevent further rapid, unsustainable economic growth, which could jeopardize the natural environment and, thus, human well-being [10]. Implementing the SDGs is to lead to positive changes in the world and improve living conditions by 2030. The assumptions of this strategy are to end poverty and hunger, fight inequality and injustice, economic, in harmony with nature and technological progress and protect the planet from degradation and climate change. Combined with the active and healthy ageing policy, the expected positive effects for the ageing population are essential. Both in the area of AA and SD (Sustainable Development) strategies, the reduction in poverty and hunger, the fight against inequalities and injustice, technological progress conducted in harmony with nature and the protection of the planet against degradation and climate change are essential determinants of individual actions as well [1,10,11,12,13,14]. It is often indicated in the literature that a change in behaviour (e.g., to a more sustainable one) results not only from self-interest but also from self-concept [15]. In a group of older people, implementing the SD strategy may be difficult due to their decreasing social activity, tendency to withdraw from society or exclusion from society. It seems that self-interest manifested in reluctance to change habits is observed more often in such a situation. Therefore, it is necessary to study how active European seniors are to know what the chances are that the ageing society will want to implement and have an opportunity to implement the SDGs.
The aim of our study is to identify differences between European seniors in the areas of activities of daily living and social participation. The realisation of this objective is not aimed at learning about institutional activities in the execution of active ageing strategies but at checking whether seniors themselves act by this strategy. For this reason, data that were not collected overtly AA-relatedly were selected so that seniors would not react suggestively about the study.
The following research questions were posed:
RQ1: Are there regional, gender and age differences among European seniors in AA self-implementation, and do the differences persist over time?
RQ2: Does social isolation occur among seniors, i.e., does avoiding social contacts (with family, religious community, environment) result in dissatisfaction and thus affect loneliness?
RQ3: Is it possible to distinguish demographic groups that prefer/use adaptive ageing and those that do not cope with changes in ageing?
RQ4: Is physical health determining mental health (satisfaction with the social environment and life)?
RQ5: Are there patterns of behaviour of European seniors in pursuing the needs of physical health, safety and respect?
In the WHO report [2] an elder or older person is a person whose age has passed the median. As we studied the subjective feelings of older people about active ageing, we also defined the age limit when Europeans consider old age based on their subjective feelings (Section 4). In the article, the term senior refers to people aged 65+. Both the terms senior and older person are used interchangeably.
The article consists of six parts, including the introduction, literature review, conclusions and discussion. In the Introduction, the research goal and questions are formulated. The research background concerning the concept, challenges and opportunities of AA are included in Section 2. Section 3 is a literature review focusing on the participation of seniors in AA. The Material and Methods Section presents the database, selection of variables for analysis and methodology. In Section 5, we present a detailed description of the clustering results regarding seniors’ subjective assessment of activity related to AAI and AA. In Section 6, we present the conclusions, discussion and future suggestions. We indicated the limitations of our analysis by presenting the database used in Section 4.
2. Research Background
2.1. Concept of Active Ageing
The concept of active ageing (AA) replaced that of the healthy ageing in the 1990s, extending it to much broader aspects of social participation. The AA strategy is a response to the ageing of the population and thus the increase in life expectancy. These changes in the demographic structure of many societies are the result of changes in economic and living conditions, technological and medical developments [16]. The AA concept is based on the three pillars outlined in the WHO report [1]. These relate to social inclusion, health and safety. The report emphasises the inseparability of the implementation of actions in the indicated pillars.
The implementation of the objective in the health pillar is aimed at extending the period of independence (live independently) of senior citizens, living longer in health while maintaining quality of life, and securing the availability of medical and social services. Activities in the area of participation are intended to ensure that seniors can participate in the labour market, benefit from education and social aspects of life following their needs and preferences. The final pillar of AA is to ensure the social, financial and physical security of seniors, their families and the communities in which they live. This pillar of AA is fundamental when seniors can no longer be independent.
The definition of AA is intended to lead to conclusions that extend to many areas. These conclusions are meant to encourage us to look at the ageing of societies as a factor influencing radical changes not only in the perceptions of older people’s lives but also in the way seniors pursue their lives. However, seniors should not be regarded as individuals isolated from society. Their behaviour and needs have and will increasingly impact social and cultural life, recreation, health care, the economy and much more. New needs will force changes in the availability and variety of many essential services, i.e., social, living and infrastructure services.
It is imperative that AA’s mission is not just a plan to help seniors, but that seniors carry it out in the first place. Reducing loneliness and social isolation enables the development of an age-inclusive society [6,17,18]. With a more holistic, life-course-oriented approach [19,20], AA benefits all generations and societies as a whole and leads to sustainable economic development [21,22]. Currently, it is natural for successive generations to pursue the priorities of good health, active engagement at work and involvement in social activities, being independent in daily life [16,23]. The AA strategy is to enable seniors to remain active and in good health for longer [6,18]. However, much depends on whether people moving into senior or retirement age can create their future [24] or fall into the trap of passivity and withdrawal. Increased free time can lead to a conscious pursuit of personal development, the strengthening of social relationships or social engagement [5]. It is therefore important to point out, as Principi et al. [25] did, that defining AA is not just about promoting longer working lives to the exclusion of other social activities. Another risk when defining AA is the formulation of a single pathway of ageing, disregarding the diversity of preferences, motivations, environment and culture. According to Rybaczewska and Sparks [20], in order to have a good understanding of AA, it is necessary to know the lifestyles and behavioural consequences of ageing and the implementation of daily activities.
2.2. Challenges and Opportunities of AA
Health as a pillar of AA is to provide the opportunity for a long healthy life, access to and use of modern medical technologies and health services, support in situations of illness and physical impairment and access to gender sensitive social services. Actions taken in this area include maintaining independence and preventing disability [1,23]. At the same time, the assumptions of AA are aimed at supporting seniors with problems and effects of progressive physical loss [26,27]. Minghetti et al. [26] indicate that the loss of physical strength in sixty-year-olds is significant, and in the eighth decade of life, isometric strength is 20–40% lower than among 30–40-year-old adults. For this reason, AA can also be considered through the prism of meeting health and social service needs [16]. Physical inactivity, on the other hand, is an important current problem as it leads to negative health consequences including cognitive decline and the occurrence of diseases, which in turn can be considered as a reason to give up active life [17,28,29,30,31]. Thus, physical activity is essential in realising active ageing [32].
Due to the need for the simultaneous implementation of the three pillars of AA, one can agree with the statement that the change in social role, personality, and the experience of a relatively stable and secure income for seniors causes a shift in Maslow’s pyramid [4]. Physiological, safety and esteem need to form coexisting relationships.
Acting within the framework of AA requires looking at seniors from a different perspective and rejecting stereotypes that persist in societies. The most commonly observed stereotypes of seniors’ perceptions mentioned in the literature concern aimlessness and dependence, lack of social roles, illness (ailments), withdrawal, mental and psychical inactivity [16,19,33]. There are even stereotypes indicating how older people should behave [34]. Today’s seniors can no longer be classified as people in decline and excluded from society [35]. Much depends on governments and local authorities in the effectiveness of AA activities [16,36]. Also, seniors should strive to overthrow stereotypes [34] and not accept them as exponents of appropriate behaviour.
Solutions in line with the AA strategy aim to reduce inequality and exclusion, taking into account changing needs and opportunities of seniors [16,17,18,37]. Several major factors limit the socialisation of seniors. These include post-retirement lifestyle changes, distance from family, mobility, new technologies [16], anxiety, fears, inability to organise/plan leisure time [5,31,38], but also personality and behaviour patterns realised during working life [23,39]. These factors point to yet another aspect to be considered in AA: seniors are a heterogeneous group with diverse views and experiences of ageing [5,40].
The diversity of seniors is more apparent than for younger age cohorts. Furthermore, the behaviours and needs of younger people imply the future generation of seniors [41]. Significant differences between seniors result from fewer obstacles in specifying and detailing their own needs than those in the active age group. They do not have to view themselves through the prism of a parent of growing children, the opinion of the environment in which they live, or the opinion of their co-workers [16,39]. Making decisions can only be related to their needs and dreams as they gain decision-making autonomy. Seniors gain the opportunity to enjoy unlimited time and freedom to participate in their personal and social lives life [5,42]. Whether seniors are able to use it is another question [24]. Unfortunately, the decision-making autonomy of seniors is very often disturbed by the strong influence of society, family and the roles performed by individual family members [43]. The family often opposes seniors’ activity for fear of deterioration of their health. Prejudice against older people was studied by Butler in 1969 [44]. The reluctance of the environment to seniors’ activity is strongly associated with negative stereotypes about them [44,45]. The diversity of senior groups, primarily regional, is due to ethnicity, environment [7,16], genetics and gender [16].
Given the heterogeneity of seniors, it is important to point out that AA must include flexible solutions because new seniors or young seniors differ significantly from old seniors, if only in their ability to use technological solutions which are encroaching with increasing intensity on all areas of everyday life [16,39]. The youngest seniors are longer beneficiaries of better health care, are better educated, live in better conditions and are familiar with the concept and opportunities arising from AA [41,42,46]. The incoming new seniors will create new paradigms of active and healthy ageing [36,47]. The problem becomes even more complicated given the singularity of the person, which is the basis for defining personalised ageing that guarantees the effectiveness of active ageing [48]. Older seniors are becoming much more dependent on family or religious environments, thus wanting to maintain some significant participation in social life [41].
Sociological analyses present two ways of adjusting to ageing: adaptive and maladaptive [49,50]. Those who come to terms with their changing social roles and economic conditions are more able to age actively. They can use their potential to maintain proper mental functions. Pursuits, exercising memory, intellectual, physical and social activities as well as maintaining optimism and internal harmony, and realising dreams and plans all stimulate an active role both in society and family (despite the costs of ageing) [49]. AA is designed to support adaptive ageing. Coping with changes in ageing, understanding these changes and introducing appropriate coping strategies make seniors accept changing social roles and economic, health, physical and intellectual conditions. With this approach, they use AA opportunities appropriately [4,6,19,27,28,39,41,46,51]. Determining strategies to cope with various situations by seniors, their regular physical activity improves health and enables an independent lifestyle, which consequently means a higher level of well-being [49,51,52].
The premise of our study is active ageing, i.e., the active engagement of older people in society [53] and seniors’ view of maintaining social harmony and social contacts as having a positive impact on the quality of life at any age [22,54]. Psychosocial well-being and quality of life depend on biological processes of ageing [26]. Thus, seniors’ social activity can lead to a higher emotional quality of life, life satisfaction, and mental and physical health [17,34,55], while exclusion and social withdrawal limit access to social, cultural, economic, political and environmental resources negatively affecting the wellbeing [17]. Focusing interventions on personal health, well-being and social networks to further enhance social participation can positively affect ability, confidence, and opportunities and again affects individual QoL. This is known as the well-being cycle [56]. Krawczyk-Suszek and Kleinrok [6] pointed out that when defining good ageing, health should be emphasised, especially in the analysis of QoL. However, the intention of our study is not to directly analyse the perception of the AA strategies but to assess, as it were, the preparation or self-interest in active ageing.
3. Participation of Seniors in AA—Literature Review
Research on AA strategy is developing in many directions. They can be divided into those which analyse the strategy and its premises and those which focus on the implementation of AA policy. The latter group also breaks down into the recognition by policy makers of action and self-action and the participation in AA by seniors who want to age actively. Due to the purpose of our study, it is essential to identify solutions derived from research on self-activity by seniors and to identify factors that improve their quality of life and well-being.
Heinonen et al. [57] reviewed the research, pointing out how extensive AA is and how diverse the research directions are. AA is associated with the quality of life or mental health [17,34]. However, the most common factor giving rise to active ageing is physical health and activity dependent on subjective well-being, because physical activity delays the effects of ageing [5,6,38,51,58,59].
Factors indirectly influencing active ageing that contribute significantly to increased physical activity are: “education, social support, perception of benefits and barriers, and self-efficacy” [22] (p. 626). Successful ageing results from the cooperation of family socio-economic factors and lifelong physical activity [5,60,61]. A factor influencing seniors’ activity is the ability to use time in a healthier way. After retirement, seniors’ daily activities focus on passive activities [31,62]. At the same time, it should be noted that the new generation of seniors is more active, spending more time outdoors and exercising [42]. Similar conclusions are presented by Barbaccia et al. [16], indicating that young seniors, apart from being active, also have higher expectations than past cohorts. They do not want to succumb to age stereotypes. Therefore, their self-awareness of the possibility of creating their lives in old age increases. The successive generations entering the senior group and the diversity of seniors discussed above contribute to changes in the perception of ageing in economic and social life [63]. The need for a more flexible AA strategy in the future is also confirmed by analyses of the post-retirement plans of professionally active people [24]. It is crucial to identify and introduce healthy habits and behaviours as well as increase mobility to maintain seniors’ physical and mental health [64]. At this point, it should be noted that new stereotypes are constantly emerging. For example, in relation to the COVID-19 pandemic, ageing was not perceived through AA’s prism but through the risk of disease [65].
Important conclusions are given by Cahill et al. [5]. Activity, together with the general life cycle of seniors, individual characteristics also affecting social and family relationships, builds their life experience. On the other hand, social (as well as physical) activity depends on health status, cognitive abilities, contact with family and friends, and physical fitness. „Such social engagement supports a sense of ‘belonging’, ‘having a role’ and ‘feeling needed’” [5] (p. 97). This is a very important message for the implementation of the AA strategy.
The research presented above corresponds to the examination of the impact of AA activities on subjective QoL, considering changes in roles and conditions (employment, social participation, physical activities and caregiving) and socio-economic, cultural and institutional contexts [66].
According to AA, one of the activities of seniors is volunteering. Research shows that volunteering, as a form of social commitment and socialisation, has positive health benefits to individuals, especially the more sensitive people, and affects their well-being [66,67]. Tanskanen et al. [68] indicated that older people who help relatives and friends by giving informal monetary help and charitable donations, often participate and are more likely to engage in pro-social activity, volunteering and charity.
Talking about AA-related research, the analyses that seek to recognise the causes of inequality in the experience of active ageing should not be overlooked [69]. However, physical and social activities do not only have benefits [70]. In a study of the impact of artistic activities, which are mainly perceived to be associated with social benefits, negative effects were identified alongside positive ones. Seniors’ participation in tourist activities may be limited by the lack of language skills, as they do not speak a second language [39]. The language barrier is also indicated by Eriksson [71] in developing applications and games for seniors.
An important group of studies on the implementation of AA are those that concern seniors with the following diseases: dementia [23,60] and walking difficulties [72]. People struggling with various illnesses may give up or withdraw from social life because, as indicated by Krawczyk-Suszek and Kleinrok [6], bodily pain has a major impact on the physical role performance and quality of life in people aged 65 and older. Activity should make it possible to overcome the psychological barrier associated with the inability to accept the functional decline of the ageing body [73]. However, mobilisation to perform physical activity in the event of unexpected adversity (COVID-19) has also been observed among people with minor walking difficulties to maintain their quality of life [72].
A welcoming place is essential in the implementation of AA policy in the security pillar [65,74]. In order for seniors to willingly implement AA, it is necessary to create the right environment, i.e., guaranteeing safe, close, familiar space for social and physical activities while guaranteeing a sense of control over their lives.
As we have already mentioned, older seniors have more significant technological problems than younger people. At the same time, tackling digital exclusion affects seniors’ withdrawal. The solution, for example, is to adapt exergames to solve problems by participating in physical activity [75].
4. Material and Methods
Research on AA most often refers to the three pillars of the AA strategy discussed earlier or to the Active Ageing Index (AAI) [30,63,76]. The structure of AAI includes four domains in two areas. For the actual experience of active ageing, these are employment, participation in society and independent, healthy and secure living. The fourth domain is the capacity for active ageing. It involves the ability and an environment conducive to active ageing. Guided by the purpose of our study, we remain in the area of both AA and AAI, but only selecting activities subjectively performed by the respondents (without knowing that they contribute to AA strategies). Due to the focus of our research on activities performed by seniors aged 65+, we did not include the employment domain. Of the other domains, we only selected those whose levels could be observed for an individual. The European Parliament’s definition is important to us [77], as it directs ageing practices to, among other things, individual lifelong learning activities, being active after retirement and choosing health-sustaining activities and not only working longer, retiring later. In our study, we excluded the employment domain because the need to work longer at the age of 65+ may result from the need to maintain adequate QoL. We also eliminated the employment domain because changes in the labour market require retraining and upskilling. This is not an opportunity for personal development according to one’s needs in response to AA [78].
Our study used European Social Survey (ESS) data from 2018 and 2020 [79,80]. The ESS is a cross-national, representative survey conducted every two years across Europe since 2001. Due to the participation of EU respondents in the survey, it is possible to compare their subjective assessments in the areas of analysis related to the AAI and AA pillars. In addition, we were looking for a chance to check whether there is a change over time in the selected areas, especially since 2020 was the year of the first COVID-19 challenges, which also resulted in decreased social activity.
We chose the European Social Survey database because it guarantees the representativeness of the sample [81]. Following the ESS assumptions for the measurement for each country, the samples must be representative of the entire population of people living in households aged 15 and over, regardless of nationality, citizenship and language. The ESS provides a detailed sampling scheme for each survey round.
The data from the ESS research fulfils another postulate we made when defining the purpose of the study. During the survey, none of the questions indicated a link to the AA strategy. We believe that seniors, when referring directly to this strategy, may give falsely positive answers regarding their activities. Particularly in international comparisons, culturally rooted behaviours are evident (seniors in some countries give truthful answers, in others, they falsely downgrade and in yet another group, they falsely overgrade when the subject of the survey is known).
The questions that appeared in both years and related to selected areas of the three pillars of AA and the three domains of AAI are presented in Table 1. We have retained the question numbers from the EES questionnaire. Responses to the questions were measured on various Likert scales.

Table 1.
The questions related to the pillars of AA and the domains of AAI.
The choice of some questions may not seem obvious. For the analysis, we chose question C16 related to participation in religious ceremonies (other than funerals and weddings) because these are activities of sensitive people and represent a traditional form of integration [9,41] (i.e., family and religions). The availability of healthcare plays an increasingly important role in the assessment of subjective QoL with age [22,66], which is why variable B32 was selected to show the respondents’ healthcare assessment in the countries analysed. Variable A6 was chosen as the respondents’ assessment of the care and volunteering of other members of society [22]. Observing such behaviour in others may lead seniors to engage in similar activities [9,48,68]. The choice of variables A4 and A5 was dictated by the fact that the high score obtained in these areas positively affects psychological well-being and the psychological security.
In our study, we focused on activities undertaken or activity assessments made by seniors aged 65+. There is some debate in the literature about what age should be used to define old age [82,83,84,85,86,87]. However, according to Alén et al. [86] and Przybysz et al. [87], we accept the age limit of 65 as older elderly. Younger people, as indicated in Section 1 and Section 2, pursue active ageing themselves because then they have more significant opportunities to benefit from AA preparation activities. We divided the selected group of seniors into two, distinguishing those aged 75+ because of their increasing health needs. To check how a selected group of seniors assesses at what age people reach old age, we checked the average age reported by Europeans from the countries selected for the analysis (this is question D17 from the ESS 2018 survey). Next, we checked the consistency of the accepted age limit (65) with the mean using the t-test.
In Table 2, an asterisk (*) indicates acceptance of the H0 hypothesis (with a reference p-value 0.05) that the average age that can be considered old age is 65 or 64. These are the opinions of respondents from the four groups distinguished by age and gender. This means that according to women aged 65–74 and 75+, as well as men in these two age groups, people reach old age at 64. Thus, from the age of 65 onwards it is possible to talk about senior citizens. This conclusion allowed the selection of respondents aged 65 and over to be retained in further analysis. In addition, the respondents’ opinions were analysed separately in the group of women and men because, due to the traditional social roles, they do not have the same opportunities to participate in social life [14,41].
Table 2.
Results of t-test on defining old age.
Table 1 lists the lowest Likert value for each question. Before starting the analysis, we changed the scaling so that the lowest value always means the worst score in the area analysed and takes the value 1.
To ensure comparability of the measurements, we used Kaufman–Rousseeuw normalisation [88,89]:
where is the actual rank given by the i-th respondent in the j-th question;
- is the normalized value for the i-th respondent in the j-th question; is the highest rank that can be assigned to the j-th question.
Observation values after Kaufaman–Rousseeuw normalisation are in the range ⟨0;1⟩.
In 2018, in the ESS survey, responses to the questions listed in Table 1 were recorded in 24 European Union countries (no data for Malta, Romania, Greece and Luxembourg). However, the data published ESS10 [80] up to 16 January 2023 only included 19 countries in the selected range of questions (no data for Malta, Romania, Luxembourg, United Kingdom, Ireland, Belgium, Denmark, Latvia and Cyprus).
Based on the normalised (Equation (1)) responses of respondents to the questions presented in Table 1, mean values were determined for each question across all countries in 2018 and 2020, taking into account the age and gender of the respondents. Based on these values, a hierarchical clustering was carried out using the Ward’s method (incremental sum of square clustering). At each stage, the division obtained by merging two clusters is optimised, using the criterion of the minimum increase in the total intra-group sum of squares of deviations of all variables for each object from their group means, which guarantees the least increase in the loss of information which is associated with an increase in the heterogeneity of the objects in the new cluster. Clusterings with Ward’s algorithm are applied after determining the square of the Euclidean distances between objects (in our case, between countries) [90,91,92,93,94].
The number of clusters was determined based on a diagram of distances connecting successive clusters. A significant increase in the next distance necessary to connect the clusters defines where the dendrogram breaks. We assessed the choice of the number of clusters with the Silhouette index, recognising values above 0.4 as a reasonable class structure [91,95].
Four clusterings were made during both years (F65–74, F, 75+, M65–74, M75+). Clusterings compliance comparisons were made using the Rand coefficient [96,97].This way, similarities between classifications made in the same year were assessed. The Rand coefficient makes it possible to determine whether the assignments of countries to clusters are the same or similar. Still, it does not allow an assessment of the similarity of the obtained clusters’ characteristics. For this reason, it is crucial to provide detailed characteristics of the clusters.
5. Subjective Assessment of Activity during Ageing—Results of the Analysis
As a result of the hierarchical classification in each year, countries considering demographic groups were divided into clusters. Table 3 presents the assessment of each partitioning performed.
Table 3.
The Silhouette Indices.
The Silhouette Index reaches values close to sufficient. Increasing the number of clusters did not result in an increase in the index value, but only a higher number of single-element groups were observed. This is a step away from the classification assumptions. The number of clusters ranged from 5 to 7. The characteristics of the clusters by year, gender and age group are given below. The clusters were ordered from countries with the highest AA-related activities scores to those with the lowest. A detailed description of each class received in both years answers the first research question (RQ1).
In Figure 1, we presented the results of countries’ clusterings (regarding seniors’ age and gender) in 2018.
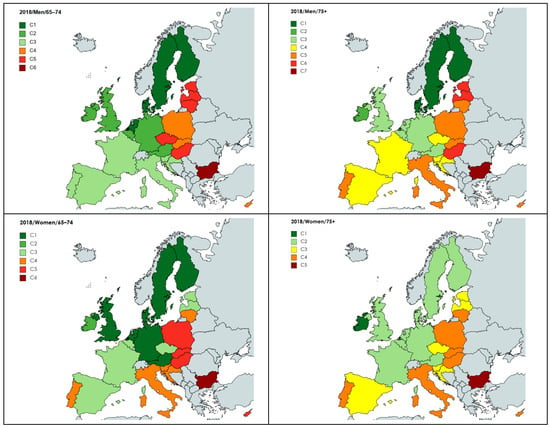
Figure 1.
Clusterings results in 2018. Source: Own elaboration.
5.1. 2018/Men/65–74
Cluster 1 (Denmark, Finland, Netherlands, Sweden): men who scored highest on all aspects of AA showed only the lowest commitment to religious services.
The second cluster comprises residents of Austria, Belgium, Germany, the United Kingdom and Ireland. They show the highest rating for political commitment. They often meet with friends and attend religious services. In other areas of AA, they gave high ratings.
The third cluster includes men from Spain, France, Croatia, Italy, Portugal and Slovenia. They very often meet with friends and participate in religious services despite their low trust in people. They also feel that other people do not want to be helpful. They judge their health poorly and are unconvinced to take a leadership role in a political group.
The fourth cluster consists of inhabitants of Cyprus, Poland and Slovakia. This is the group that most often attends religious meetings and at the same time rarely meets with friends. They have the least trust in other people, as well as a very low assessment of others in terms of helpfulness and honesty. They rate their health well but the health service low. On the other hand, they rate their ability to play an active political role as average.
Czechs, Estonians, Hungarians, Lithuanians and Latvians were placed in cluster five. They have moderate trust in people and rate the willingness to help others as average. They are afraid that other people want to take advantage of them. These fears translate into less frequent meetings with friends. They assess the health service poorly, and their self-assessment of health is the lowest among all groups. Their satisfaction with life, sense of happiness, willingness to participate in political life, participation in religious meetings, sense of security and assessment of their own income are very low.
Bulgarians are in the last cluster among men aged 65–74. They rarely meet with friends and attend religious services. They have very low trust in other people and rate their health very poorly. Their ratings in all other aspects of AA are the lowest.
5.2. 2018/Men/75+
Cluster 1: Denmark, Finland, Sweden. Men from this group report the highest scores in all aspects of psychological well-being. They prefer to meet with friends and rarely attend religious services. They rate the health service very highly while pointing to minor health problems. Their income is sufficient for a comfortable life. They are ready to assume an active role in a political group.
Cluster 2 are Irish. They rate their readiness to take an active political role highest and most often attend religious services. At the same time, they meet their friends very often. They rate their health the best. They have a lot of trust in people and believe that other people want to be very helpful. They are very happy and have great satisfaction with their lives. Their subjective assessment of the healthcare system is average.
Cluster 3: Austria, Belgium, Germany, United Kingdom, Netherlands. Men from this group show a very high belief in people’s honesty and satisfaction with life. They are happy, trust people and say that other people want to be helpful, meet friends and attend religious services. Their income is sufficient for a comfortable life. Their subjective assessment of their health is good. They think they can actively participate in political life.
Cluster 4: Czechia, Spain, France, Croatia, Slovenia. They rate the helpfulness and honesty of people lowly. Also, trust in others is low. However, they feel safe in their neighbourhood. They rate the state of their health care system as good and in other aspects AA is average.
Cluster 5: Cyprus, Italy, Lithuania, Poland, Portugal, Slovakia. This is a group that attends religious services very often and at the same time, rarely meets with friends. They have a very low trust in other people, as well as a very low evaluation of others in terms of helpfulness and honesty. Their life satisfaction and sense of happiness are very low, as are their sense of security and self-rated health. They negatively evaluate the health service and their ability to actively participate in political life.
Cluster 6: Estonia, Hungary, Latvia. They have moderate trust in people and rate the willingness to help others as average. They are least likely to meet friends or attend religious services, but do not want to actively participate in political life. They rate their health service very poorly, and their self-assessment of health is low. Their sense of happiness is low, and they consider their income insufficient for a comfortable life.
Cluster 7 is Bulgarians. They rarely meet with friends and attend religious services. Their ratings of all other AA aspects are the lowest.
5.3. 2018/Women/65–74
Cluster I: Austria, Germany, Denmark, Finland, Sweden, United Kingdom, Netherlands. They value trust in people and their honesty most highly. They have the greatest satisfaction with their lives and feel that their income is sufficient for a comfortable life. This is probably why they feel very safe in their neighbourhood. They mainly meet friends and rarely attend religious services.
Cluster II consists of Irish women. They rate their readiness to take an active political role the highest, attend religious services most often and, at the same time, meet with friends very often. They rate their health the best. They give very high ratings in terms of mental well-being. Their subjective evaluation of the healthcare system is very low. They have a low sense of security.
Cluster III: Belgium, Czechia, Estonia, Spain, France, Latvia. They rate all aspects of mental well-being as good, as do their health and income. They meet with friends and are the least likely to participate in religious services. They are reluctant to take an active part in political life.
Cluster IV: Croatia, Italy, Lithuania, Portugal, Slovenia. They rate the helpfulness and honesty of people as low. Also, trust in others is low. However, they feel safe in their neighbourhood. They rate the state of their health care as good and in other activities as average.
Cluster V: Cyprus, Hungary, Poland, Slovakia. Their sense of security is high; they often attend religious services and rate the state of their health care well, while believing that other people do not want to be helpful. Other aspects of AA are rated low.
Cluster VI: Bulgaria. They rarely meet with friends and attend religious meetings. Their life satisfaction, happiness, security and income ratings are the lowest. On the other hand, they gave low ratings in all other aspects of AA.
5.4. 2018/Women/75+
Cluster 1: Ireland. They rate their readiness to take an active political role the highest, attend religious services most often and, at the same time, meet with friends very often. They rate their health as average. Like the younger Irish women, they rate their mental well-being very highly. Their subjective assessment of the healthcare system is average. They have a low sense of security.
Cluster 2: Austria, Belgium, Germany, Denmark, Finland, Sweden, United Kingdom, Netherlands, France. They value trust in people and their honesty the highest. They rate life satisfaction the highest and feel that their income is sufficient for a comfortable life. This is probably why they feel very safe in their neighbourhood. They most often meet friends and least often attend religious services. They rate the health care service very highly while pointing to minor health problems. They are ready to take a political leadership role.
Cluster 3: Czechia, Estonia, Spain, Latvia, Croatia, Slovenia. They rate all aspects of mental well-being as average, as do their health and income. The frequency of meetings with friends or religious people is average. They feel very safe in their neighbourhood. They rate the state their health service as good. They do not want to take an active part in political life.
Cluster 4: Cyprus, Hungary, Italy, Lithuania, Poland, Portugal, Slovakia. They rate all aspects of mental well-being as low. They often attend religious services but rarely meet with friends. However, they feel very safe in their neighbourhood. They rate other aspects of AA low.
Cluster 5: Bulgaria. They rarely meet with friends and attend religious services. They consider the possibility of active participation in political life. On the other hand, they gave the lowest ratings in all other aspects of AA.
In Figure 2, we presented the results of countries’ clusterings (regarding seniors’ age and gender) in 2020.
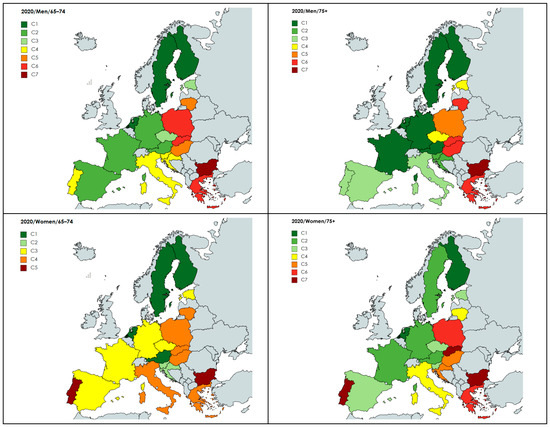
Figure 2.
Clusterings results in 2020. Source: Own elaboration.
5.5. 2020/Men/65–74
The first cluster comprises residents of Finland, the Netherlands and Sweden. They scored highest on all aspects of AA except for religious services (they participate in these events sporadically).
The second cluster includes men from Austria, Germany, Spain and France. They show very high ratings for political commitment. Although they have average trust in people, they highly rate other MWB domains. They rarely attend religious services and, at the same time, very often meet with friends. Their income provides them with a comfortable life. Their subjective assessment of the health system is good, and they assess their health very well.
Cluster 3 (Czechia and Estonia): men who scored mental well-being and physical safety in AAI high. Their satisfaction with life and sense of happiness is average, as well as their subjective income rating. Their willingness to participate in political life is low. This group rarely meets with friends and even less often attends religious meetings.
The fourth cluster consists of Cyprus, Italy, Portugal and Slovenia inhabitants. It is a cluster of men who are satisfied and happy with their lives, but at the same time, they evaluate other aspects of mental well-being as low. Nevertheless, they feel very safe in their neighbourhood. They rate the health service and their health as average. Their income is sufficient for a good life. They often participate in religious services but rarely meet with friends.
Cluster 5: Hungary and Lithuania. Men from this group very often participate in religious services, and at the same time, they meet with friends the least. They show a very high trust in other people, and in terms of helpfulness and honesty, they assess others as average. Their life satisfaction and sense of happiness are low, as is their sense of security and income. They have the lowest health self-esteem.
Cluster 6: Greece, Poland and Slovakia. Men in this age group rarely meet with friends and most often participate in religious services. They want to participate in political life actively. They assess their health as satisfactory. The assessment of the others area of AA is shallow.
5.6. 2020/Men/75+
The first cluster includes Austrians, Germans, Finns, Dutch, Swedes and French. They show the highest mental well-being, political participation and financial security ratings. Occasionally attend religious services but more often meet with friends.
Cluster 2 is Croats and Slovenes. They rate safety very highly. Their ratings of income, health and satisfaction with life, as well as other aspects of mental well-being, are high. Their social connectedness is average. They do not want to play an active role in political groups.
Group 3: Italy, Spain, Portugal. They are very happy, often meet with friends and participate in religious services. They have a sufficient income. Other aspects of mental well-being are assessed as average. They show some security concerns but are not convinced to play an active role in political groups.
Cluster 4 is Czechs and Estonians. They rate their happiness and life satisfaction as low, but at the same time, they highly rate other aspects of mental well-being. They indicate an average level of sense of security. Among the respondents at this age, they assess their health as the worst, but the health service as very good. They claim that their income is too low for a comfortable life. They do not participate in religious services and rarely socialise with friends.
Poles are in cluster 5. They most often participate in religious services and rarely meet with friends. The respondents rate their health as good, even though the level of health care is assessed as the worst. They feel safe in their surroundings. They have high satisfaction with life but have a very low opinion of trust in people, their helpfulness and honesty. They will gladly take an active role in political life.
Cluster 6 are Greeks, Hungarians, Lithuanians, and Slovaks. They least often participate in meetings with friends, very often attend religious services, and they do not feel a clear need to participate in political life actively. Of all the respondents, they feel the least safe in their neighbourhood. In other aspects of AA, the ratings given are low.
The last cluster is Bulgarians. They meet with friends most often and very rarely participate in religious meetings. They indicate poor health. They consider active participation in political groups. Their ratings for other aspects of AA are the lowest.
5.7. 2020/Women/65–74
The first cluster comprises Austrian, Finnish, Dutch and Swedish women. In 2020, mental well-being was rated the highest among all respondents in this age group. They rarely attend religious services, and, at the same time, they often meet with friends. They assess their income and health aspects as the best. They are the most willing to assume an active political role.
The second cluster includes Croatians and Slovenians. They rate their happiness and life satisfaction highly, and average ratings are given to other people’s behaviour. They place their health well but give a lower rating to the health service. They rarely meet with friends and attend religious services a little more often. Their safety rating is the highest of all respondents in this age group. They assess the level of their income well. They are not ready to assume an active political role.
Cluster 3: Czechia, Germany, Estonia, Spain, France. Although they assess their happiness and life satisfaction as average, they rate other mental well-being aspects as high. This group includes women who hardly ever participate in religious meetings and do not feel safe in their neighbourhood. In the remaining aspects of the AAI analysed, the ratings are average.
Cluster 4: Greece, Hungary, Italy, Lithuania, Poland, Slovakia. They very often attend religious services but very rarely meet friends. All aspects of the capacity and enabling environment for active ageing are rated very low, as is access to health services and financial security.
Cluster 5: Bulgaria and Portugal. They meet with friends most often and often participate in religious meetings. On the other hand, their ratings in all other aspects of AA are the lowest.
5.8. 2020/Women/75+
The first cluster consists of Finnish and Dutch women. They rated mental well-being, access to health services and financial security the highest among all women in this age group. They attend religious services least often, but they meet with friends most often. They feel very safe in their neighbourhood and are considering taking an active role in a political group.
Cluster 2: Austria, Germany, France, Sweden. They scored access to health services and financial security very high. They are very satisfied with life and happy. They rate society very highly in terms of helpfulness, trust and honesty. They often meet with friends but very rarely participate in religious meetings. They rate their readiness to participate in political groups the highest.
Cluster 3: Czechia, Estonia and Slovenia. Women from these countries are very happy. They rarely participate in religious services but more often meet with friends. Their assessment of mental well-being, health, financial situation and political participation is high.
Cluster 4: Italy and Lithuania. Female respondents in this group assessed the aspects of mental well-being as average. They very often participate in religious services but rarely meet with friends. They rate their income well. They have significant security concerns. They rather do not want to engage in an active political role.
Cluster 5: Croatia and Hungary. Among all women aged 75+ in 2020, they assess the level of security as the highest, despite the low assessment of trust, helpfulness and honesty of other people, as well as very low assessment of satisfaction with life and happiness. They very rarely meet with friends but more often participate in religious services. They are not satisfied with their income. They rate their ability to function actively in a political group the highest of all.
Cluster 6: Greece and Poland. This group comprises women most often participating in religious services but also the least likely to meet friends. They highly value their ability to participate in a political group actively. They believe that people cannot be trusted and furthermore, do not show any desire to help others. Women of this group are also the least satisfied with the state of health care.
The last cluster is formed by residents of Bulgaria, Portugal and Slovakia. They very often meet with friends and often participate in religious meetings. They rate all other aspects of corresponding to the AAI very low or even the lowest of all women aged 75+ in 2020.
5.9. Rand Coefficients
After the hierarchical clustering, the Rand coefficients were calculated, assessing the similarities between the partitionings made in one year. The results are presented in Table 4.
Table 4.
Rand coefficients.
The values of the Rand coefficients indicate that the most significant similarities in countries’ affiliation to clusters were observed in 2018 among both men in both age groups and women in both age groups. High similarity is also visible in the clustering of countries in the analysis of ratings by younger women and men in 2018. In 2020, the Rand coefficients are significantly higher than in 2018. It can be concluded that all results of the four clusterings carried out this year produce convergent results.
6. Conclusions and Discussion
The results of our analysis indicate that the division of countries into three groups, as carried out in the Active Aging Index 2014: Analytical Report [30], is insufficient. This report determined the country groups after considering all AAI domains with the proposed weights. On the other hand, looking at the problem from the perspective chosen in our study (i.e., assessing the readiness of seniors to adopt AA activities and checking whether they are already implementing these demands) shows the complexity of the problem. Based on the databases we used, it is impossible to consider the predispositions, needs and implementation of the surveyed activities among people with disabilities. For this reason, further research should be focused on this social group which requires exceptional support. Our study meets the demands of seniors as presented by Heinonen et al. [57] or Boudiny [78]. Seniors want to be treated individually as heterogeneous individuals. They demand to see that many seniors undertake activities and socialisation on their own in order to maintain their physical well-being, remain active in society, and not be alone. Limiting the assessment of AA only to economic engagement or physical activity is an oversimplification. As postulated in [7,16], the results of our clusterings confirm the regional diversity of senior groups as well as that of gender and age (RQ1).
Our study on AA and AAI aimed to understand the differences between men and women from two age groups of seniors from different countries. The study is in line with the Decade of Healthy Aging postulates. The DHA Program focuses on an individual view of older people and recommends disaggregating studies by age, gender, place of residence and other socio-economic factors [9,14].
In the course of the analysis, it was observed that two countries formed one-element clusters in 2018: Ireland (M75+, F65–74, F75+) and Bulgaria (M65–74, M75+, F65–74, F75+). The characteristics of the distinguished groups by age and gender for Ireland are similar. These are individuals who socialise very often with friends and also attend religious events. Their ratings in the area of mental well-being, regarding their own happiness and their assessment of society, are very high. Only women, compared to men, indicate that they do not feel safe. On the other hand, the residents of Bulgaria differ significantly from other seniors, indicating very poor ratings in all AA-related areas analysed.
In 2020, due to the lack of data, Ireland was not included in the analyses, while the ratings given by Bulgarians continued to be ranked in the lowest groups.
During the analysis, the following correlations were repeatedly observed between respondents’ assessments of AA areas. Low ratings of mental well-being as a reaction to the surrounding society (A4, A5, A6) were associated with a higher willingness to actively participate in political groups. Such an interaction between mental health and social participation is indicated by Lakomý [66]. Very often, a high frequency of attending religious services was associated with a lower frequency of meeting friends (and vice versa). Also, Baeriswyl and Oris [41] looked for associations between social participation in and individual life satisfaction among the elderly. They pointed out that private forms of social participation are important for the elderly’s life satisfaction while, traditional forms (family and religion) are important for vulnerable people. For this reason, the answer to the second research question is affirmative and, as indicated in the research [6,17,18], social isolation and dissatisfaction with life situations often occur together (RQ2, RQ4). However, it is important to indicate the willingness to play an active social role.
Even though, as the proverb goes, money does not make happiness, in our study, we observed that higher income scores resulted in higher mental well-being scores, including levels of happiness and life satisfaction. If the respondents rarely met friends, they also indicated low ratings of trust, helpfulness and honesty from society (RQ5). Many times, high ratings of mental well-being corresponded with high ratings of the state of one’s own health and health care. When the ratings in physical safety decreased, the ratings of mental well-being were also lower (RQ4). It is consistent with the results of other studies [17,34].
As Lakomý [66] points out, regional differences in the EU translate into socio-economic or cultural differences, which in a broader context highlights other research problems. When analysing clusters affiliation, the following similarities between countries were observed. In our study, we found similar assessments of seniors from different countries (RQ1). Both younger and older women and younger and older men from Denmark, Finland and Sweden in 2018 were always in the same cluster. Similar observations were made in four other country groups: (1) Austria, Germany and United Kingdom, (2) Croatia and Slovenia, (3) Estonia and Latvia, (4) Poland and Slovakia. As well as in 2020 for: (1) Finland and Netherland, (2) Germany and France, (3) Czechia and Estonia.
Although the analysis in 2018 and 2020 included a different number of countries (due to the availability of data), one can notice differences in the assessment made by the inhabitants of these countries belonging to the four surveyed demographic groups in 2018 and 2020. In 2018, the youngest German women belonged to a cluster of people satisfied with their lives, highly evaluating society and social participation, and rarely participating in religious services. However, in 2020 they belonged to a cluster of people who were averagely satisfied with their health system, their life and financial situation, and limiting contacts with friends and during religious services. On the other hand, the oldest Germans indicated higher scores in areas of the AAI (except for attending religious services) in 2020 concerning 2018 compared to other respondents. The ratings given by 65–74 years German seniors (men) in 2018 and 2020 are similar to those of older German women. Therefore, the reasons for the ratings issued cannot be sought in the threat caused by COVID-19 and the related restrictions. A change in the assessment of areas related to AAI can also be observed among Spaniards and French aged 65–74 in 2020 compared to 2018. Despite less frequent participation in religious services, all other AAI areas in 2020 were rated higher. In 2020, the scores given by Portuguese women aged 75+ in all areas of the AAI, except for meetings with family and during religious services, dropped significantly.
In 2018, the following characteristics were visible in all demographic groups. Clusters 1 and 2 consist of people who are satisfied with their lives, evaluate the environment in which they live well and are satisfied with their income, often meet with friends and rarely participate in religious services (implementation of the postulates of adaptive ageing—RQ3). In subsequent clusters, the ratings for access to health services, physical safety, financial security, political participation and mental well-being are lower and lower, contacts with friends became less frequent, and the frequency of attending religious services increased. However, in the last cluster, social meetings were also rated the lowest (maladaptive ageing—RQ3). In 2020, clusters 1 and 2 among women and men in both age groups are still characterised by those who live actively and participate in social life to the highest degree. On the other hand, the last clusters are represented by people who are the least satisfied with their environment and their material and health situation, but social contacts are quite different. Unlike in 2018, they most often contact friends, and women also frequently participate in religious services. Among the men in the last groups in 2020 are Bulgarians, but compared to 2018, these are the respondents who most often meet friends. Among the women in the last group are all Bulgarian and Portuguese women and older Slovak women. Out of all women, these respondents most often contacted friends and participated in religious services in 2020. Moreover, 2020 is the early period of the COVID-19 pandemic, which saw the most extraordinary restrictions, including a long-term lockdown. Observed differences may result from different compliance with government regulations. They can also be the result of the effectiveness of law enforcement in individual countries.
Summing up the study, we would like to point out that the analysis made it possible to identify differences and similarities between age and gender groups in EU countries in 2018 and 2020 separately. The analysis also showed that only some seniors had a consistent, strong pattern of behaviour in 2018, which was repeated in 2020. For most seniors, the unexpected event of the outbreak of the COVID-19 pandemic caused a change in the ratings in the AAI domains.
The results of our cluster analysis can be used as a modification of the weights in the AAI. It is possible to check the differences in the AAI after introducing weights based on the clusterings in 2018 and 2020. In such a situation, cluster membership can indicate areas that need to be improved in terms of AA. This is because our detailed analysis showed the existence of deficit areas referring to the guidelines of the AA strategy. An analogous analysis to the one we conducted can be performed for younger people who will reach the age of 65+ in the next few years. Thanks to this, the directions in which regional AA policies should be heading will be known, and the prediction of AA in the demographic groups of individual countries. These are the determinants of our subsequent research: modification of the AAI weights based on the classification of countries due to the subjective assessment of AAI domains among seniors and future seniors.
As indicated by Li and Shao [54], activity results from prosocial behaviours acquired throughout life. Therefore, encouraging seniors to remain active from the period of their working life is very important. However, convincing previously inactive seniors to adopt AA is quite challenging. Profiguration may be a solution to the problem [98]. Starting from using natural interdependencies between family members and their environment at different stages of life, one can strive to avoid loneliness and ageing by introducing active ageing as an essential part of the quality of life.
A block to the introduction of AA into everyday life may be the common view that ageing can be used to win the race of competitiveness of economies [47]. Another barrier to the individuals introducing AA into their lives may also be the reluctance to look ahead and plan continuously [37]. When creating senior activation programme offers, it should be remembered that the realisation of seniors’ well-being should follow their needs [53]. Seniors are willing to participate in AA activities if they are not advertised as “for seniors”.
Author Contributions
Conceptualization, K.P. and A.S.; methodology, K.P. and A.S.; software, K.P. and A.S.; validation, K.P. and A.S.; formal analysis, K.P. and A.S.; investigation, K.P. and A.S.; resources, K.P. and A.S.; data curation, K.P. and A.S.; writing—original draft preparation, K.P. and A.S.; writing—review and editing, K.P. and A.S.; visualization, K.P. and A.S.; supervision, K.P. and A.S.; project administration, K.P. and A.S.; funding acquisition, K.P. and A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of t his study are available from the corresponding author and from [79,80].
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- World Health Organization [WHO]. Active Ageing. A Policy Framework; World Health Organization: Geneva, Switzerland, 2002; Available online: https://apps.who.int/iris/bitstream/handle/10665/67215/WHO_NMH_NPH_02.8.pdf;jsessionid=30B9E6B9C57A8CF4A643AE76160D7DEE?sequence=1 (accessed on 30 October 2022).
- World Health Organization [WHO]. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/186463 (accessed on 18 May 2023).
- Eurostat. Population on 1st January by Age, Sex and Type of Projection (Data Code: PROJ_19NP) [Data Set]. Available online: https://ec.europa.eu/eurostat/databrowser/view/PROJ_19NP__custom_4540833/default/table?lang=en (accessed on 14 February 2023).
- Grześkowiak, A.; Przybysz, K.; Peternek, P.; Stanimir, A. Pokolenie 65+ Perspektywa Społeczno-Ekonomiczna; Wydawnictwo Uniwersytetu Ekonomicznego we Wrocławiu: Wrocław, Poland, 2021. [Google Scholar]
- Cahill, J.; McLoughlin, S.; O’Connor, M.; Stolberg, M.; Wetherall, S. Addressing Issues of Need, Adaptability, User Acceptability and Ethics in the Participatory Design of New Technology Enabling Wellness, Independence and Dignity for Seniors Living in Residential Homes. In Human Aspects of IT for the Aged Population. Aging, Design and User Experience; Zhou, J., Salvendy, G., Eds.; Springer: Cham, Germany, 2017; pp. 90–109. [Google Scholar] [CrossRef]
- Krawczyk-Suszek, M.; Kleinrok, A. Health-Related Quality of Life (HRQoL) of People over 65 Years of Age. Int. J. Environ. Res. Public Health 2022, 19, 625. [Google Scholar] [CrossRef] [PubMed]
- Special Eurobarometer 378: Active Ageing Report. European Commission, Directorate-General for Communication. 2012. Available online: https://europa.eu/eurobarometer/surveys/detail/1002 (accessed on 14 February 2023).
- Schwanen, T.; Ziegler, F. Wellbeing, independence and mobility: An introduction. Ageing Soc. 2011, 31, 719–733. [Google Scholar] [CrossRef]
- World Health Organization [WHO]. Decade of Healthy Ageing: Baseline Report; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications-detail-redirect/9789240017900 (accessed on 18 May 2023).
- United Nations [UN]. Sustainable Development Goals; United Nations: New York, NY, USA, 2015; Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed on 17 April 2023).
- Almeida-Silva, M.; Monteiro, A.; Carvalho, A.R.; Teixeira, A.M.; Moreira, J.; Tavares, D.; Tomás, M.T.; Coelho, A.; Manteigas, V. Sustainable and Active Program—Development and Application of SAVING Methodology. Int. J. Environ. Res. Public Health 2022, 19, 6803. [Google Scholar] [CrossRef] [PubMed]
- Cox, C. The Sustainable Development Goals and Aging: Implications for Social Work. J. Hum. Rights Soc. Work 2020, 5, 39–47. [Google Scholar] [CrossRef]
- Office of High Commissioner on Human Rights [OHCHR]. Sustainable Development Goals; Office of High Commissioner on Human Rights: Geneva, Switzerland, 2016; Available online: https://www.ohchr.org/Documents/Issues/MDGs/Post2015/Contribution2016HLPF.pdf (accessed on 17 April 2023).
- World Health Organization [WHO]. UN Decade of Healthy Ageing: Plan of Action; World Health Organization: Geneva, Switzerland, 2020; Available online: https://cdn.who.int/media/docs/default-source/decade-of-healthy-ageing/decade-proposal-final-apr2020-en.pdf?sfvrsn=b4b75ebc_28&download=true (accessed on 18 May 2023).
- Bolderdijk, J.; Steg, L.; Geller, E.; Lehman, P.K.; Postmes, T. Comparing the effectiveness of monetary versus moral motives in environmental campaigning. Nat. Clim Change 2013, 3, 413–416. [Google Scholar] [CrossRef]
- Barbaccia, V.; Bravi, L.; Murmura, F.; Savelli, E.; Viganò, E. Mature and Older Adults’ Perception of Active Ageing and the Need for Supporting Services: Insights from a Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 7660. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization [WHO]. Age-Friendly Environments in Europe A Handbook of Domains for Policy Action; WHO Regional Office for Europe: Copenhagen, Denmark, 2017; Available online: https://www.who.int/publications/i/item/9789289052887 (accessed on 14 February 2023).
- Howse, K.; Sidorenko, A. Europe: An Age-inclusive Society? Popul. Ageing 2022, 15, 301–305. [Google Scholar] [CrossRef]
- Foster, L.; Walker, A. Active and successful aging: A European policy perspective. Gerontologist 2015, 55, 83–90. [Google Scholar] [CrossRef]
- Rybaczewska, M.; Sparks, L. Ageing consumers and e-commerce activities. Ageing Soc. 2022, 42, 1879–1898. [Google Scholar] [CrossRef]
- Walker, A. A strategy for active ageing. Int. Soc. Secur. Rev. 2002, 55, 121–139. [Google Scholar] [CrossRef]
- Boerio, P.; Garavaglia, E.; Gaia, A. Active ageing in Europe: Are changes in social capital associated with engagement, initiation and maintenance of activity in later life? Ageing Soc. 2021, 43, 122–1140. [Google Scholar] [CrossRef]
- Zirves, M.; Demirer, I.; Pfaff, H. Everyday Life and Social Contacts of Dementia and Non-Dementia Residents over 80 Years in Long-Term Inpatient Care: A Multi-Level Analysis on the Effect of Staffing. Int. J. Environ. Res. Public Health 2021, 18, 11300. [Google Scholar] [CrossRef]
- Rowe, J.W.; Kahn, R.L. Successful aging 2.0: Conceptual expansions for the 21st century. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2015, 70, 593–596. [Google Scholar] [CrossRef]
- Principi, A.; Di Rosa, M.; Domínguez-Rodríguez, A.; Varlamova, M.; Barbabella, F.; Lamura, G.; Socci, M. The Active Ageing Index and policy making in Italy. Ageing Soc. 2021, 1–26. [Google Scholar] [CrossRef]
- Minghetti, A.; Donath, L.; Hanssen, H.; Roth, R.; Lichtenstein, E.; Zahner, L.; Faude, O. Physical Performance, Cardiovascular Health and Psychosocial Wellbeing in Older Adults Compared to Oldest-Old Residential Seniors. Int. J. Environ. Res. Public Health 2022, 19, 1451. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Niu, H.; Zhou, D. Analysis and Study on the Furniture Used by the Aging Population Based on the Quality of Sleep. In Human Aspects of IT for the Aged Population. Aging, Design and User Experience; Zhou, J., Salvendy, G., Eds.; Springer: Cham, Germany, 2017; pp. 244–254. [Google Scholar] [CrossRef]
- Pastor, D.; Ballester-Ferrer, J.A.; Carbonell-Hernández, L.; Baladzhaeva, S.; Cervello, E. Physical Exercise and Cognitive Function. Int. J. Environ. Res. Public Health 2022, 19, 9564. [Google Scholar] [CrossRef]
- Gluchowski, A.; Bilsborough, H.; Mcdermott, J.; Hawley-Hague, H.; Todd, C. ‘A Lot of People Just Go forWalks, and Don’t Do Anything Else’: Older Adults in the UK Are Not Aware of the Strength Component Embedded in the Chief Medical Officers’ Physical Activity Guidelines—A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 10002. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.; Stanton, D. Active Ageing Index 2014: Analytical Report; co-funded by European Commission’s Directorate General for Employment, Social Affairs and Inclusion, Brussels, United Nations Economic Commission for Europe: Geneva, Switzerland, 2015. [Google Scholar]
- Sprod, J.; Olds, T.; Brown, W.; Burton, N.; van Uffelen, J.; Ferrar, K.; Maher, C. Changes in use of time across retirement: A longitudinal study. Maturitas 2017, 100, 70–76. [Google Scholar] [CrossRef] [PubMed]
- de Sousa, B.A.; da Silva, F.C.; Ribeiro, Í.L.; de Lima, D.B.B.; da Silva, R. Sociodemographic, Anthropometric, Functional and Psychosocial Factors Associated with Physical Activity in Older Adults. Ageing Int. 2022, 47, 617–629. [Google Scholar] [CrossRef]
- Lassen, A.J.; Moreira, T. Unmaking old age: Political and cognitive formats of active ageing. J. Aging Stud. 2014, 30, 33–46. [Google Scholar] [CrossRef]
- Garrido, J.F.; Conde, M.D.; Vázquez, M.V.; Rodríguez, L.V. Are Older Adults’ Leisure Patterns Consistent with the Active Ageing Model? The Influence of the Ageist Stereotypes. Soc. Policy Soc. 2022, 21, 575–596. [Google Scholar] [CrossRef]
- Ogg, J. Lifelong Learning in Ageing Societies: Lessons from Europe. In UNESCO—2021 UIL Report Embracing a Culture of Lifelong Learning; UNESCO Institute for Lifelong Learning: Hamburg, Germany, 2021. [Google Scholar]
- Zaidi, A. Active ageing index: A legacy of the European year 2012 for active ageing and solidarity between generations. Policy Brief 2015. Available online: http://envejecimiento.csic.es/documentos/documentos/EuropeanCenter-04-2015.pdf (accessed on 19 May 2023).
- Clarke, A.; Warren, L. Hopes, fears and expectations about the future: What do older people’s stories tell us about active ageing? Ageing Soc. 2007, 27, 465–488. [Google Scholar] [CrossRef]
- Molesztak, A. Nordic walking jako współczesna forma aktywności seniorów (Nordic walking as a contemporary activity form of seniors). J. Educ. Health Sport 2016, 6, 365–375. [Google Scholar] [CrossRef]
- Przybysz, K.; Stanimir, A. Tourism-Related Needs in the Context of Seniors’ Living and Social Conditions. Int. J. Environ. Res. Public Health 2022, 19, 15325. [Google Scholar] [CrossRef]
- Yang, Y.; Dolega, L.; Darlington-Pollock, F. Ageing in Place Classification: Creating a geodemographic classification for the ageing population in England. Appl. Spat. Anal. 2022, 16, 583–623. [Google Scholar] [CrossRef] [PubMed]
- Baeriswyl, M.; Oris, M. Social participation and life satisfaction among older adults: Diversity of practices and social inequality in Switzerland. Ageing Soc. 2021, 43, 1259–1283. [Google Scholar] [CrossRef]
- Vilhelmson, B.; Thulin, E.; Elldér, E. Is ageing becoming more active? Exploring cohort-wise changes in everyday time use among the older population in Sweden. Eur. J. Ageing 2022, 19, 447–461. [Google Scholar] [CrossRef] [PubMed]
- Sawińska, A. Problemy konsumpcji w turystyce i rekreacji. In Ekonomika Turystyki i Rekreacji; Panasiuk, A., Ed.; Wydawnictwo Naukowe PWN: Warszawa, Poland, 2011; pp. 176–201. [Google Scholar]
- Butler, R.N. Age-Ism: Another Form of Bigotry. Gerontologist 1969, 9, 243–246. [Google Scholar] [CrossRef]
- Vauclair, C.M.; Lima, M.L.; Abrams, D.; Swift, H.J.; Bratt, C. What do older people think that others think of them, and does it matter? The role of meta-perceptions and social norms in the prediction of perceived age discrimination. Psychol. Aging 2016, 31, 699–710. [Google Scholar] [CrossRef]
- Chan, C.M.A.; Liang, J.S.E. Active Aging: Policy Framework and Applications to Promote Older Adult Participation in Hong Kong. Ageing Int. 2013, 38, 28–42. [Google Scholar] [CrossRef]
- Zielińska-Szczepkowska, J. What Are the Needs of Senior Tourists? Evidence from Remote Regions of Europe. Economies 2021, 9, 148. [Google Scholar] [CrossRef]
- Baraković, S.; Baraković Husić, J.; van Hoof, J.; Krejcar, O.; Maresova, P.; Akhtar, Z.; Melero, F.J. Quality of Life Framework for Personalised Ageing: A Systematic Review of ICT Solutions. Int. J. Environ. Res. Public Health 2020, 17, 2940. [Google Scholar] [CrossRef] [PubMed]
- Giustini, M.; Longo, E.; Beggiato, M.; Cozzolino, M., for working group CHANGE (Eds.) Ageing today: A new challenge for tomor—773 ow. State of the art of the European Project CHANGE (Care of Health Advertising New Goals for Elderly people); Rapporti ISTISAN 774 09/49; Istituto Superiore di Sanità: Rome, Italy, 2009.
- Kijak, R.I.; Szarota, Z. Starość. Między Diagnozą a Działaniem. In Starość. Między Diagnozą a Działaniem; Centrum Rozwoju Zasobów Ludzkich: Warszawa, Poland, 2013. [Google Scholar]
- Reyes, M.-F.; Satorres, E.; Delhom, I.; Bueno-Pacheco, A.; Meléndez, J.C. Coping and Life Satisfaction in Colombian Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 10584. [Google Scholar] [CrossRef]
- Król-Zielińska, M.; Osiński, W.; Zieliński, J.; Kusy, K. Physical fitness of elderly people in Poland in comparison with the population of the United States. Stud. Phys. Cult. Tour. 2006, 13 (Suppl.), 53–55. [Google Scholar]
- Sala, E.; Cerati, G.; Gaia, A. Are social media users more satisfied with their life than non-users? A study on older Italians. Ageing Soc. 2023, 43, 76–88. [Google Scholar] [CrossRef]
- Li, J.; Shao, W. Influence of Sports Activities on Prosocial Behavior of Children and Adolescents: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 6484. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Qiu, L.; Zuo, M. Gamification on Senior Citizen’s Information Technology Learning: The Mediator Role of Intrinsic Motivation. In Human Aspects of IT for the Aged Population. Aging, Design and User Experience; Zhou, J., Salvendy, G., Eds.; Springer: Cham, Germany, 2017; pp. 461–476. [Google Scholar] [CrossRef]
- Walker, A. Commentary: The Emergence and Application of Active Aging in Europe. J. Aging Amp Soc. Policy 2008, 21, 75–93. [Google Scholar] [CrossRef]
- Heinonen, T.; Valokivi, H.; Luo, H. Active Aging and Well-being of Older Northern Women in Finland. Ageing Int. 2022. [Google Scholar] [CrossRef]
- Infante, P.; Jacinto, G.; Afonso, A.; Conde, J.; Engana, T.; Vicente, J.; Silva, P.; Coelho, A.C.; Costa, P. Evaluation of Some Physical and Health Parameters in a Local Physical Activity Program for Seniors. Port. J. Public Health 2019, 37, 10–18. [Google Scholar] [CrossRef]
- Weeks, L.E.; Profit, S.; Campbell, B.; Graham, H.; Chircop, A.; Sheppard-LeMoine, D. Participation in physical activity: Influences reported by seniors in the community and in long-term care facilities. J. Gerontol. Nurs. 2008, 34, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Kashtanova, D.A.; Taraskina, A.N.; Erema, V.V.; Akopyan, A.A.; Ivanov, M.V.; Strazhesko, I.D.; Akinshina, A.I.; Yudin, V.S.; Makarov, V.V.; Kraevoy, S.A.; et al. Analyzing Successful Aging and Longevity: Risk Factors and Health Promoters in 2020 Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 8178. [Google Scholar] [CrossRef]
- Gallardo-Peralta, L.P.; Sanchez-Moreno, E.; Herrera, S. Aging and Family Relationships among Aymara, Mapuche and Non-Indigenous People: Exploring How Social Support, Family Functioning, and Self-Perceived Health Are Related to Quality of Life. Int. J. Environ. Res. Public Health 2022, 19, 9247. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Jiménez, C.; Dumitrache, C.; Rubio, L.; Ruiz-Montero, P. Self-perceptions of ageing and perceived health status: The mediating role of cognitive functioning and physical activity. Ageing Soc. 2022, 1–20. [Google Scholar] [CrossRef]
- Walker, A.; Zaidi, A. New Evidence on Active Ageing in Europe. Intereconomics 2016, 51, 139–144. [Google Scholar] [CrossRef]
- Hernández, N.; Refugio, C.; Tentori, M.; Favela, J.; Ochoa, S. Mobile and Context-Aware Grocery Shopping to Promote Active Aging. In Ambient Assisted Living and Active Aging; Nugent, C., Coronato, A., Bravo, J., Eds.; IWAAL 2013. Lecture Notes in Computer Science; Springer: Cham, Germany, 2013; Volume 8277, pp. 71–79. [Google Scholar] [CrossRef]
- Gallistl, V.; Richter, L.; Heidinger, T.; Schütz, T.; Rohner, R.; Hengl, L.; Kolland, F. Precarious ageing in a global pandemic—Older adults’ experiences of being at risk due to COVID-19. Ageing Soc. 2022, 1–19. [Google Scholar] [CrossRef]
- Lakomý, M. The effect of roles prescribed by active ageing on quality of life across European regions. Ageing Soc. 2021, 43, 664–688. [Google Scholar] [CrossRef]
- de Wit, A.; Qu, H.; Bekkers, R. The health advantage of volunteering is larger for older and less healthy volunteers in Europe: A mega-analysis. Eur. J. Ageing 2022, 19, 1189–1200. [Google Scholar] [CrossRef]
- Tanskanen, A.; Hämäläinen, H.; Arpino, B.; Danielsbacka, M. Prosocial activity in later life: Are informal help and care associated with volunteering and charity? Ageing Soc. 2022, 1–36. [Google Scholar] [CrossRef]
- Olivera, J. Ageing unequally in Europe. Socio-Econ. Rev. 2022, 20, 401–422. [Google Scholar] [CrossRef]
- Chacur, K.; Serrat, R.; Villar, F. Older adults’ participation in artistic activities: A scoping review. Eur. J. Ageing 2022, 19, 931–944. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J. Playful Method for Seniors to Embrace Information Technology. In Human Aspects of IT for the Aged Population. Aging, Design and User Experience; Zhou, J., Salvendy, G., Eds.; Springer: Cham, Germany, 2017; pp. 429–446. [Google Scholar] [CrossRef]
- Siltanen, S.; Portegijs, E.; Saajanaho, M.; Pynnönen, K.; Kokko, K.; Rantanen, T. Self-rated resilience and mobility limitations as predictors of change in active aging during COVID-19 restrictions in Finland: A longitudinal study. Eur. J. Ageing 2022, 19, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Øye, C.; Norvoll, R.; Vabø, M. ‘Keeping up appearances’—Negotiating identities of being fit in older age: A multi-site ethnographic study of daily life in contemporary day centres. Ageing Soc. 2021, 1–18. [Google Scholar] [CrossRef]
- Battersby, L.; Fang, M.L.; Canham, S.L.; Sixsmith, J.; Moreno, S.; Sixsmith, A. Co-creation Methods: Informing Technology Solutions for Older Adults. In Human Aspects of IT for the Aged Population. Aging, Design and User Experience; Zhou, J., Salvendy, G., Eds.; Springer: Cham, Germany, 2017; pp. 77–89. [Google Scholar] [CrossRef]
- Brox, E.; Luque, L.F.; Evertsen, G.J.; Hernandez, J.E.G. Exergames for elderly: Social exergames to persuade seniors to increase physical activity. In Proceedings of the 5th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth) and Workshops, Dublin, Ireland, 23–26 May 2011; pp. 546–549. [Google Scholar] [CrossRef]
- Principi, A.; Santini, S.; Socci, M.; Smeaton, D.; Cahill, K.; Vegeris, S.; Barnes, H. Retirement plans and active ageing: Perspectives in three countries. Ageing Soc. 2018, 38, 56–82. [Google Scholar] [CrossRef]
- Commission of the European Communities [CEC]. Europe’s Response to World Ageing, Promoting Economic and Social Progress in an Ageing World: A Contribution of the European Commission to the Second World Assembly on Ageing, Communication from the Commission to the Council and the European Parliament, COM (2002) 143 Final; Commission of the European Communities: Geneva, Switzerland, 2002.
- Boudiny, K. ‘Active ageing’: From empty rhetoric to effective policy tool. Ageing Soc. 2013, 33, 1077–1098. [Google Scholar] [CrossRef]
- ESS 2018 European Social Survey European Research Infrastructure (ESS ERIC). In ESS9-Integrated File, 3.1st ed.; [Data set]; Sikt-Norwegian Agency for Shared Services in Education and Research: Bergen, Norway, 2021. [CrossRef]
- ESS 2020 European Social Survey European Research Infrastructure (ESS ERIC). In ESS10-Integrated File, 2.1st ed.; [Data set]; Sikt-Norwegian Agency for Shared Services in Education and Research: Bergen, Norway, 2022. [CrossRef]
- ESS. Sampling. Available online: https://www.europeansocialsurvey.org/methodology/ess_methodology/sampling.html (accessed on 31 January 2023).
- Pesonen, J.; Komppula, R.; Riihinen, A. Typology of Senior Travellers as Users of Tourism Information Technology. Inf. Technol. Tour. 2015, 15, 233–252. [Google Scholar] [CrossRef]
- European Commission. Assessment of the Europe 2020 Strategy Joint Report of the Employment Committee (EMCO) and Social Protection Committee (SPC); Publications office of the European Union: Luxembourg, 2019. Available online: https://ec.europa.eu/social/main.jsp?langId=en&catId=1063&furtherNews=yes&newsId=9487 (accessed on 5 August 2022).
- Begg, I.; Bongardt, A.; Torres, F. Europe 2020 and employment. In Europe 2020—A Promising Strategy? Intereconomics 2010, 45, 146–151. [Google Scholar]
- European Commission. Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions. In The European Platform Against Poverty and Social Exclusion: A European Framework for Social and Territorial Cohesion. COM(2010), 758 Final; European Commission: Brussels, Belgium, 2010. Available online: https://op.europa.eu/en/publication-detail/-/publication/16456b4c-211e-434f-9884-a11b6d6a7f79/language-en/format-PDF/source-search (accessed on 5 August 2022).
- Alén, E.; Domínguez, T.; Losada, N. New Opportunities for the Tourism Market: Senior Tourism and Accessible Tourism. In Visions for Global Tourism Industry–Creating and Sustaining Competitive Strategies; Kasimoglu, M., Ed.; IntechOpen: London, UK, 2012; pp. 139–166. [Google Scholar]
- Przybysz, K.; Stanimir, A.; Wasiak, M. Subjective Assessment of Seniors on the Phenomenon of Discrimination: Analysis Against the Background of the Europe 2020 Strategy Implementation. Eur. Res. Stud. J. 2021, 24, 810–835. [Google Scholar] [CrossRef]
- Kaufman, L.; Rousseeuw, P.J. Finding Groups in Data: An Introduction to Cluster Analysis; Wiley: New York, NY, USA, 1990. [Google Scholar]
- Walesiak, M. Strategie postępowania w badaniach statystycznych w przypadku zbioru zmiennych mierzonych na skalach różnego typu. Bad. Oper. I Decyz. 1993, 1, 71–77. [Google Scholar]
- Mirkin, B. Mathematical Classification and Clustering; Kluwer Academic Publishers: Dordrecht, The Netherland, 1996. [Google Scholar]
- Handl, A. Multivariate Analysemethoden. In Theorie und Praxis Multivariater Verfahren unter Besonderer Berücksichtigung von S-PlUS; Springer-Verlag: Berlin/Heidelberg, Germany, 2002. [Google Scholar]
- Timm, N.H. Applied Multivariate Analysis; Springer-Verlag: New York, NY, USA, 2002. [Google Scholar]
- Backhaus, K.; Erichson, B.; Plinke, W.; Weiber, R. Multivariate Analyzemethoden; Springer: Berlin, Germany, 2003. [Google Scholar]
- Härdle, W.; Simar, L. AppliedMultivariate StatisticalAnalysis; Springer-Verlag: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Han, J.; Kamber, M.; Pain, J. Data Mining Concepts and Techniques, 3rd ed.; Elsevier Inc.: Waltham, MA, USA, 2012. [Google Scholar]
- Rand, W.M. Objective Criteria for the Evaluation of Clustering Methods. J. Am. Stat. Assoc. 1971, 66, 846–850. [Google Scholar] [CrossRef]
- Hubert, L.; Arabie, P. Comparing Partitions. J. Classif. 1985, 2, 193–218. [Google Scholar] [CrossRef]
- Rivera-Ochoa, F.S.; González-Herrera, I.V.; Zacarías-Flores, M.; Correa-Muñoz, E.; Mendoza-Núñez, V.M.; Sánchez-Rodríguez, M.A. Relationship between Self-Perception of Aging and Quality of Life in the Different Stages of Reproductive Aging in MexicanWomen. Int. J. Environ. Res. Public Health 2022, 19, 6839. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).