1. Introduction
Understanding factors influencing healthy ageing among older people from ethnic minority groups is very timely within the context of migration and ageing in most European countries. There is vast literature focused on the social determinants of health and inequities in labour and social outcomes among ethnic minority populations that propagate into old age. However, there is little attention to the role of ageing perceptions and expectations within different communities and individuals and the implications of the uptake of healthy ageing behaviour. Maintaining a healthy ageing behaviour and propagating health education are essential to a sustainable healthcare system. This paper argues for the need to recognise the risk factors linked to potentially outdated views of ageing among earlier cohorts of migrants in Europe to develop innovative approaches to reduce health inequalities in old age. Realising the importance of individual and community-held views about ageing can inform interventions to support younger cohorts of migrants to adopt healthier habits and plan better for the later stages of life. Patient empowerment and early planning can contribute to a more sustainable healthcare system. This paper takes the United Kingdom (UK) as a case example and focuses on people who migrated from Pakistan, India and Turkey during the 1960s and 1970s and are likely to be in their 70s in 2020.
Until recently, in the UK, the standard definition of belonging to an ethnic minority was proxied by those born outside the UK [
1]. This definition, however, is being challenged, as it does not capture second and third generations ethnic minorities born in the UK, nor does it consider the ethnic diversity of the country of origin. Ethnic minorities in the older age group are usually referred to as migrants, even though they may hold residency or British nationality. In this paper, the term ‘older migrants’ [
2,
3,
4] refers to older people from a minority ethnic group, regardless of their current residency/nationality or country of birth.
Few studies focus on ethnic minorities in the UK [
5,
6], and fewer are available for older ethnic minorities to the extent of being excluded from research [
7]. Overall, current evidence indicates significant health inequalities and adverse health outcomes among older migrants [
8,
9,
10]. These differentials are the product of many systematic [
11] and individual factors. However, there is also evidence of some effects linked to individuals’ and groups’ perceptions of ageing in shaping the uptake of healthy ageing behaviour [
12]. For example, some studies point out the presence of more pessimistic views of ageing, less preparation for older age, and limited expectations among older migrants in the UK and Europe [
13,
14,
15]. Such perspectives are partly associated with and attributed to several factors that occur across the life course, such as the loss of social capital due to the migration process and earlier trauma [
8,
16]. However, the formation and effect of what we may term ‘outdated views on ageing’ is not explicitly addressed in the literature. This study aims to find a possible explanation for the outdated views and attempt to explain, where possible, differentials in the uptake of innovations and how this might be linked to adopting healthy ageing behaviour. It is essential to consider why migrants’ view of ageing could be outdated and how a lesser diffusion of innovations might further impact these views to consider possible ways to mitigate their effects when planning public health interventions. The Diffusion of Innovation Theory can help understand whether older migrants have the same rate of uptake of healthy ageing innovation compared to the average older population while controlling for other factors.
The Diffusion of Innovation theory originated in the 1960s explains how innovation can spread in a social system [
17]. Innovation can be new information, an idea, a healthy habit, a practice, or similar. In this context, the social system consists of individuals and their social networks. Information can be transmitted within the social system using communication channels. The process and the speed of adaptation depend on the size of the population, the communication channel and time. In the diffusion of innovation theory [
17], innovators who can accept new ideas quickly first adopt innovation and then spread it to members of the social system who are open to new ideas. Those members are early adopters. As more individuals adopt the innovation, more individuals become comfortable in forming most of the adaptors. As time passes, the number of adaptors reaches a threshold upon which no more social system members are willing to adopt. According to this theory, those members of the social system who are not ready to adopt are referred to as the laggards. Applying this theory has resulted in a large body of research and models to quantify and study the diffusion process of innovations. One known model is the fundamental diffusion model [
17], which is implemented in the study presented in this paper.
1.1. Health Inequalities of Migrants and Ethnic Minorities
Evidence from North America [
18,
19,
20] indicates that newly arriving migrants are likely to be healthier than their counterparts in their host countries, even amongst older age groups, in what is usually referred to as migrant health advantage. Moreover, this advantage appears to deteriorate with increasing duration of residence [
21]. Furthermore, research from the United States of America (USA) indicates that compared to USA-born whites, white migrants are likely to keep their health advantage. In contrast, non-white migrants tend to lose such an advantage over time as they continue to live in the US, with a steeper decline attributed to racialized migrant incorporation processes [
22].
In Europe, similar evidence indicates that older migrants are likely to have started their migration journey healthier than their counterparts in the host countries [
8,
23]. However, after staying in their host countries, migrants tend to suffer from adverse health outcomes and chronic diseases similar to the general host populations at an earlier age. Similar findings have been reported in a recent quantitative study [
24] examining the health outcomes of migrants (defined as those born outside the UK). The study relied on the Labour Force Survey (LFS) quarterly data from 2019, the Annual Population Survey (APS) from 2019, and Understanding Society: COVID-19 Study, 2020 (First wave, April 2020). Amongst the findings was that in 2019, recent migrants across all age groups were healthier than the general population who were born in the UK. Overall, around 27% of newly arriving migrants reported long-lasting health problems compared to 42% of the UK born. However, migrants who lived longer in the UK were likely to have more health problems than the newly arrived, even when compared to those in the same age groups. The migration selection process could explain why younger migrant groups are likely to be healthier than UK-born at similar ages; those who are capable of migrating tend to be the healthiest among their group, reflecting the ‘migrants’ health advantage’ [
18,
19]. It is, however, harder to explain why those who arrived at older ages tend to have better health outcomes than migrants who lived longer in the UK and who are in the same age group. These health differentials for the older age group of migrants could be related to disadvantaging factors associated with living in the UK, where structural inequalities persist. This might worsen their health compared to their peers still living in their home countries.
These health differentials could be attributed to the challenges migrants likely face with their daily living while living in host countries, including competing demands and prioritising work over health due to the need to remit and reduced social capital [
25]. They are also more likely to provide and rely on informal care to and from family members due to a combination of preferences, limited information and structural barriers to accessing formal care [
15]. In the process, they are less likely to undergo regular health checks and may even delay treatments, with potential adverse health implications [
8].
Furthermore, Migrants tend to be concentrated in specific income clusters with barriers to the labour market and are likely disadvantaged by socioeconomic factors, although the effect varies across ethnic groups [
26]. Several studies report structural discrimination and racism where migrants of colour and visible social markers are likely economically and socially disadvantaged [
27]. According to Public Health England, in 2017, over 50% of people from Bangladeshi and Pakistani ethnic groups lived in the most deprived 20% of areas in England [
28]. To highlight the magnitude of these figures, in England, life expectancy is lowest in the most deprived areas, with around nine years and seven years shorter for males and females compared to the least deprived areas [
28].
1.2. Ethnic Minorities and COVID-19
There is evidence that COVID-19 had a disproportional effect on ethnic minorities in the UK [
29,
30,
31], with the highest age-standardised diagnosis rates reported among people from ethnic minority groups [
32,
33]. When controlling for the effects of sex, age, deprivation and region, people of Bangladeshi ethnicity had around twice the risk of death when compared to people of White British ethnicity. Furthermore, people from other ethnic minority groups had between 10% and 50% higher risk of death when compared to White British. These were reflected in ethnic differentials in COVID-19-related mortality rates, ranging between 1.6 to 4 times higher than White British groups depending on ethnicity and gender [
32,
33].
The disproportional COVID-19 impact is likely to reflect migrants’ socio-economic vulnerability in their host countries and the lack of ability to avoid infection and access healthcare systems among people from ethnic minority groups [
11,
31]. For example, a study by [
34] reported that healthcare workers from minority ethnic groups have higher levels of either re-use or inadequate access to personal protective equipment (PPE). A review of employment inequalities among British minority ethnic workers in health and social care at the time of COVID-19 highlights the impact of institutional racism and the lack of empowerment amongst minority healthcare workers resulting in the inability of ethnic minority workers to challenge the authority of their employers [
35].
There are other risk factors related to vaccination access and uptake among ethnic minorities, not just COVID-19 vaccination. Evidence suggests divergent approaches in vaccinating recently arrived migrants to Europe, with some European countries excluding them from initiatives to promote catch-up vaccination on arrival [
36].
The uptake of vaccination and other health promotions can improve by directly addressing the role of diffusion of innovation among ethnic minorities. This could be through tailored vaccination messages, community outreach [
37] and ensuring vaccination information is tailored to different beliefs among ethnic minorities [
38]. The diffusion model used in this paper aims to provide a tangible explanation of how targeted messages can significantly impact the uptake rate among older people from ethnic minority groups.
Other unidentified risk factors. A few other European studies suggest unidentified risk factors contributing to health declines among older ethnic minority populations driven by their views on ageing. These suggestions arise in different studies [
13,
15] and align with the social determinants of health framework that perceives personal and cultural characteristics as the core of social health determinants [
39,
40]. For example, older Turkish migrants, one of Europe’s most significant ethnic minorities, are among the most vulnerable group of older people in Europe [
41]. A quantitative study based on survey data that examined differences in ageing perception between Turkish migrants and native Dutch residing in Rotterdam [
14] has found that older Turkish groups are more likely to report more negative views of ageing than their Dutch counterparts. Part of their negative perception can be attributed to fewer resources and challenges related to language barriers, lower income and educational attainment than their Dutch counterparts. However, according to the same study, the most significant part of the variation in perception remains unexplained.
Another large UK qualitative study [
13] adds another dimension to the perception of ageing among older Turkish migrants; it refers to a ‘solid outdated view on ageing’. The study is based on analysing life history interviews with 66 older Turkish migrants aged 65+ years and an additional 30 community or care workers who supported Turkish migrants in London. The analysis is based on Nancy Fraser’s trilogy of interrelated factors of social justice: resources, recognition, and representation [
42], focusing on social networks as a critical resource. One of the key findings is that many participants held a solid perception of ageing that was shaped when they were young in Turkey. This perception had most likely related to views on ageing shared with their grandparents’ generation and did not represent Turkey’s current view of ageing. The study does not explain the reason for this old view. However, the findings suggest a level of detachment from the host country’s perceptions of ageing while holding a view of ageing that can be related to their native country, Turkey. However, the views related to their earlier experience with their own grandparents, as children and young adults, pre-migration; hence, such ageing views were outdated and did not acknowledge the enhancement in the more recent experiences of older people and the broader society in Turkey.
The literature agrees on differentials in health outcomes among older migrants and native host populations across Europe and that it can be linked to economic and social resources. However, there appears to be a factor related to how some older migrants view ageing, which could be addressed and mitigated. Part of changing individuals’ views requires enhancing the diffusion of innovation among migrants, which depends on social contacts and targeted and culturally sensitive messages. There seem to be common assumptions that migrants are well-connected, communicate well across generations, and care for each other [
43,
44]. However, others argue that older migrants are isolated and have limited access to formal care services [
15,
45]. However, no studies investigated or quantified the differentials of communications within the migrant communities compared to the host populations. This study attempts to fill this specific knowledge gap. It aims to (1) conceptualise the role of outdated or negative ageing views among older migrants as a risk health factor, (2) utilise the concept of the diffusion of innovations and available information in explaining what may prevent updating these views, and (3) explore what should be considered when planning public health campaigns to narrow the gap between the level of uptake among migrants and the majority population.
This paper thus attempts to provide an explanation that relies on the wider assumptions that (a) ageing views are shaped at an earlier stage of life [
46] before the migration events, (b) migrants have fewer social contacts than the native population [
47,
48], and (c) the lack of social contact between migrants and the partial detachment from the host population [
49] maintain such views. These assumptions are likely to result in ageing perceptions that are, at best, old and pessimistic and likely to lead to adverse decisions when planning toward ageing and adversely impact the uptake of health innovations and public health interventions. However, these views can be targeted and updated as part of a more holistic and sustainable healthcare system that acknowledges the growing diversity of the population.
2. Conceptual Framework
In this study, an outdated view of ageing is defined by two main themes: the first is how people perceive their life expectancy, both healthy and unhealthy years. Evidence suggests genetics and environment are among the factors that determine longevity [
50].
The second theme is the misguided health-related information and habits that can be impeded at a young age. For example, in the Middle East, where most of the care given is informal, trying to help older people as much as possible is customary. For example, it attempts to care for older people by relieving them from shopping, cooking and other daily activities [
51]. We now know that maintaining daily life activities, when possible, positively affects physical and cognitive health outcomes [
52]. Another old habit is to treat joint pain by resting, leading to a cycle of weakened muscle and more joint problems ending up with impaired mobility and rapid ageing [
53].
These and other habits are associated with outdated views of ageing because awareness improves over time. Based on that observed during childhood in home countries, an outdated view of ageing is generally more negative than today’s view of ageing, both in migrant’s home countries and the UK. This is due to many factors, including the rapid demographic shifts and increased average life expectancy trends over the past decades in many ageing populations.
The conceptual framing of this study and the depiction of the old view of age formation,
Figure 1, is informed by several sources. First, the Dahlgren and Whitehead model of health determinants, adopted by the British government [
39,
40], describes the interaction between determinants of health with personal characteristics, such as ethnicity in its core. Second, the Decade of Healthy ageing 2020–2030 [
46] is the WHO’s second action plan of its global strategy on ageing. The strategy builds on the United Nations Madrid International Plan of Action on Ageing MIPPA, which is currently undergoing its fourth review. The action plan states, “great inequity in longevity according to social and economic grouping”. It also provides an updated vision of what constitutes healthy ageing. Of its most relevant actions to this discussion is the need to change how people think, feel and act toward ageing. Third, the Multidimensional, Ecological, and Comparative Approach (MECA) for understanding migrants’ life cycle [
54,
55,
56,
57]. MECA seeks to explain how migration impacts the life cycle stages of a family and examines benefits, challenges and contextual stressors that impact immigrants. Although the framework was developed within the context of Latino immigrants to the USA, there are common patterns associated with migration that can affect migrants’ life cycles. However, it may vary depending on the host country and the migrants themselves.
Figure 1 illustrates how migrants may be prone to adopt an outdated ageing view. It assumes they had developed their perception of ageing in childhood, and young adulthood [
46], mostly before the migration event took place. After migration, they are assumed to encounter two different paths. A proportion,
, may follow Path-1, where they are adversely affected by structural factors combined with isolation, which results in them not being able to relate to the host population [
57]. This group is more likely to maintain a view on ageing linked to the experience of their parents and grandparents in their home countries and would willingly accept the old view of ageing that has been shaped before their migration. This may lead to self-ageism [
46], where they (sub)consciously adopt negative views and have fewer expectations or planning towards ageing. That outdated and negative view would reduce their chances of healthy ageing. The other proportion of migrants
take Path-2, where they encounter more positive experiences in the host countries. Such experiences help migrants relate to their new home, update their view of ageing, and increase their chances of healthy ageing. Individual personal characteristics are at the core of health determinants [
39], and the view of ageing is likely to affect migrants’ uptake of healthy ageing behaviour and their health outcomes as they age.
3. Data and Methods
For the UK Social contact matrix, this study uses the publicly available data from the POLYMOD project [
47], the first large-scale quantitative approach to contact patterns. Although the project aimed to inform the parametrisation of mathematical modelling of infectious diseases that depend on population mixing patterns, the results can inform the diffusion of the innovation process; here, we assume that innovation can spread through similar routes to infectious diseases. Data on social contacts is based on a population-based prospective survey of mixing patterns conducted in eight European countries (The UK, Germany, Italy, Belgium, Finland, Luxembourg, The Netherlands, and Poland). The survey employed 7290 participants using a standard paper diary to record the characteristics of contacts for one day. Among the key findings, one of the data’s highlights is that mixing patterns and social contact characteristics across the eight European countries are very similar, where people tend to mix with those within the same age group. This similarity may suggest that what is discussed in the context of the UK concerning contact rates may draw similar conclusions with other European countries.
For the three other countries, India, Pakistan and Turkey, the social contact matrices data come from a different study that estimated social contacts for countries not yet included in the POLYMOD project. The publicly available projections result from a Bayesian hierarchical model using data from various sources. The latter include the POLYMOD project’s mixing patterns, demographic and health surveys from lower-income countries, the World Bank, the UN statistics, and the Demographic Household Surveys Program (DHS). A complete list of data sources and methodology used for estimation is explained in [
48]. Social contact Data for each of the four countries is aggregated [
58] into the age groups of 0–20, 20–30,30–50,50–65,65–80. Data regrouping and matrices visualisation is carried out using the R lattice package [
59,
60].
Other demographic factors data obtained from the World Bank [
61] and the United Nations data [
62] were used to prepare demographic statistics on Life expectancy at birth and the mean age at first marriage for both males and females for the UK, India, Pakistan and Turkey. The aim of utilising this data is to seek further explanations for the differences in average contact rates at older ages across the four countries.
The diffusion model [
17] employed in this paper examines the adoption of innovation within a population over time. The model assumes a closed population, where no changes to the population size due to births or deaths and individuals are categorized as either adaptors or not. It describes the progression of the cumulative number or proportion of individuals who become adapters, starting from an initial state of few adopters and approaching a predetermined ceiling as the diffusion process unfolds. This deterministic model provides insights into the dynamics of innovation adoption, capturing the pattern of gradual uptake, reaching a peak, and eventually stabilizing. These assumptions are based on findings of various research specific to the diffusion of innovation processes in different fields [
63,
64,
65,
66,
67,
68]. The model formation can be illustrated as follows: if we assume that within a closed social system of size
. At time-point
, during the adoption, the number of adopters could be represented as
. And the number of potential adopters is
. However, it is usually assumed that 100% uptake of innovation is not feasible, and an upper threshold
is only attainable. During the diffusion phase, we assume the size of that social system’s population is fixed, with no birth or mortality.
It follows that from the interaction between those who adopted and the potential adopters, the number of adapters will increase with an instantaneous rate of change proportional to
, which is usually termed internal influence. Similarly, we can assume an additional increase in the number of adopters from an external influence such as media, for example, public health awareness advertisements in the media such as the radio and television. That will be an addition to the instantaneous rate of change proportional to
. This mixed influence diffusion model can be written as follows:
where
are constants coefficients of diffusion. A representation of the instantaneous rate of change for the fraction of adopters,
, can be achieved by setting
, and followed by an algebraic manipulation resulting in:
where (
is an upper threshold, beyond which there are no more adopters within the social system, and
represents the fraction of laggards.
In its most basic form, this fundamental diffusion model is usually referred to as the mixed influence diffusion model [
69]. It can be seen from all the above that the external effect is an additive component. Furthermore, when considering the comparative nature of the discussion within this paper and the neutralising of the size of the closed population by using the fraction form of the model, Equation (2), we can remove the external influence diffusion component to focus the comparison on the internal influence resulting from the contact rate. This formation is referred to as the internal influence diffusion model, which confines the social interaction between members of the social system as the channel for spreading ideas and innovations [
63,
70]. The model integration is carried out using the C++ Boost library [
71] to produce the comparative results of the uptake of innovation.
4. Results
Figure 2 shows the social contact rates for the four countries included in this study. The average daily contact rate is considerably higher in Pakistan, India and Turkey (21.2, 14.1 and 12.1) within the age groups younger than 20 years old compared to 7.88 for the UK. However, the average daily contact rate drops considerably within the older group of 65–80 with averages of (0.2, 0.3 and 0.7) in each of these countries compared to an average of 1.71 in the UK. Contact rates are also higher in the UK for the age group 50–65, with an average of 2.31 daily contract rate compared to (1.2, 1.4, 1.4) for the three other countries, Pakistan, India and Turkey.
Figure 2 shows that the highest contact rates among minority groups are found in the younger age groups (<20 and 20–30 years) with daily contact rates of (6.9, 5.6, 6.1) for India, Pakistan and Turkey, considerably higher than the 3.6 observed for the UK general population in the same age groups. However, the pattern converges for the age groups of 30 to 50, followed by a reverse starting in the older groups. For the age group 50–65, the daily contact rates for the three countries drop to (1.4, 1.2, 1.4) compared to 2.31 for the UK general population. These results contradict the common assumption found in the literature that migrants communicate well between themselves, and they have strong social networks and hence might not need tailored public health interventions, especially when it comes to social care [
43,
44].
Some demographical statistics concerning old age were considered to investigate potential reasons for the observed differentials in the average daily social contact rates among the older populations in the four countries. Specifically, both male and female life expectancy and mean age at first marriage could be used to understand the likely number of lonely years among married couples by gender, assuming a continued partnership (no separation) and no remarriage following widowhood (see
Table 1). For example, in the UK, in 1971, a female was expected to live 6.3 years more than a male and marry at age 21.3, 2.9 years younger. That might have resulted in her being widowed for 9.2 years with a reduced contact rate with someone in the same age group (absence of partner/spouse). On the other hand, the negative sign for India’s difference in life expectancy in 1971 resulted from females living shorter than males on average during that year. That resulted in likely lonely years of 3.9 for females at that time. This is, however, changed to 7 years by 2016. Although the differences in likely lonely years due to the demographic statistics of life expectancy and the mean age of first marriage appear to favour the UK when compared to Turkey and India, this is not the case in comparison to Pakistan. As such, these demographic factors alone cannot explain the differences in contact rates between the four countries in this study.
The results presented in
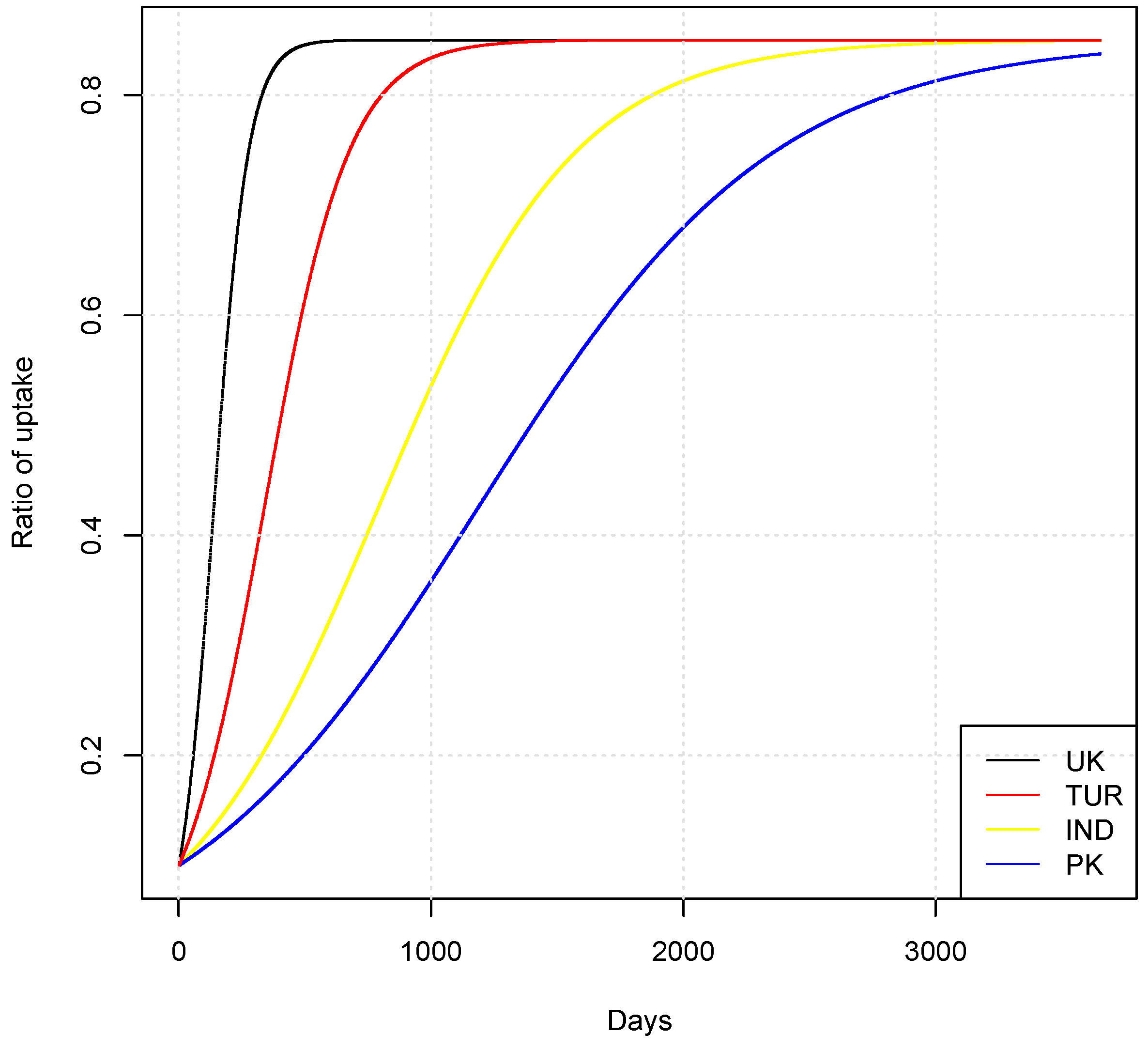
Table 2 show considerable differences in the time-to-adaption of innovations for the three older ethnic minority groups compared to those of the UK general population. For example, for the Turkish group, it would take 2.4 times the amount of time needed for a similar proportion of the UK to reach the same level of adaption (whether 85% or 100% uptake). The same can be noted for the other two groups of India and Pakistan, with multiples of 5.7 and 8.5, respectively.
Table 2 shows that the number of days to reach a target level of adaptation differs based on the upper threshold of adaptation (U). However, the time different migrant groups take to reach the upper threshold relative to the UK general population remains unchanged, regardless of the upper threshold. This conclusion can be reached directly from the model. Simple mathematical manipulation can show that, relative to the population size, the rate of adaptation is directly proportional to the contact rate. Moreover, when U, the threshold for potential possible adapters, gets smaller, the adaptation process gets slower. For example, when U = 0.85, for the UK, it would take 164 days to reach the level of adaptation of 50%, compared to 130 days for U = 1.0.
Figure 3 visualises the time series of the cumulative uptake ratio for innovation with an upper threshold of 0.85 among a closed population for each of the four countries of the UK, TUR, IND and PK. The summary statistics of this figure are presented in the first half of
Table 2. It can be seen from the visualisation how the diffusion process starts with an exponential increase before slowing down gradually as it approaches the upper threshold of 0.85 and ceases to increase above this limit.
5. Discussion
This study attempts to quantify the effect of social contacts on the uptake of innovations among three older migrant groups compared to the UK population. In doing so, this paper aims to fill an apparent gap in the literature and support the development of a more inclusive and sustainable healthcare system. The main findings of this study could be summarised as follows: older migrants likely have outdated views of ageing, and their social contacts are much lower than expected. As a result, older migrants are expected to take much longer to adopt healthy ageing innovations and are at higher risk of social isolation than their native host counterparts. The assumption that older migrants are more susceptible to social isolation due to migration-related challenges is widely studied [
72,
73]. However, research on non-migrant adults in the UK consistently shows a prevalent risk of social isolation and loneliness in later life, stemming from factors such as loss of significant others, diminished social networks, and reduced social participation [
74,
75]. Social isolation is a multidimensional issue, and both populations may experience deficits in these dimensions due to different circumstances.
Increasing the uptake of health innovation requires culturally specific public health interventions. Targeting younger cohorts of migrants (less than 30) will likely result in significant uptake of healthy ageing behaviour in the long term.
Definitions of healthy ageing are debatable as they tend to overemphasise functional dependencies and result in a public and policy discourse that treats all older adults generically without consideration for heterogeneity, hence, excluding their own perception of healthy ageing [
76,
77]. Research shows that maintaining physical functioning is subject to external socioeconomic status and environmental factors over the life course [
55,
76]. Recently, the WHO updated its definition of healthy ageing as the process of developing and maintaining the functional ability that enables wellbeing in older age [
46]. Moreover, that functional ability includes, among other components, the ability to build and maintain relationships and contribute to society. These functional abilities are shaped by the interaction between the intrinsic capacity of the individual and environmental characteristics. This universal view of ageing is characterised by both inequity and diversity. The new definition is shifting from regarding healthy ageing as disease-free and physical independence to enabling older people to do what they value. It acknowledges the link between the 2030 sustainable development goals and healthy ageing and that older people face the same barriers as others but with a higher magnitude. It also emphasises that part of achieving healthy ageing is changing perceptions towards ageing [
46].
The discussion of the old view of the ageing formation and its effect within the suggested framework in
Figure 1 can be streamlined by trying to answer a few questions. First, (1) Why would some older migrants have an outdated view of ageing? The answer will likely be twofold: limited communication with their home country and detachment from the host country. Considering the first fold (a) limited communications with the home country, those who migrated in 1970 at the age of 20 are now in their 70s (
Figure 1). When they left their home countries, India, Pakistan and Turkey, the average life expectancy at birth was 48, 53 and 51 years, respectively. Reflecting how migrants’ parents and possibly their grandparents aged. However, life expectancy in the four countries increased over time to 70, 67 and 70 in 2019. Part of the increase in average life expectancy can be attributed to reduced child mortality. However, it also reflects reduced mortality in the older age groups and overall enhancement of the general population’s health outcomes. Even if the latter assumption does not hold, it should still be reasonable to assume that the peer cohort of those who migrated and are still living in their home countries gradually updated their view of ageing, realising that people live longer.
Some of those who migrated in 1970 are likely to have lost this transitional view of ageing (Path-1 in
Figure 2). In the 1970s and up to the late 1990s, methods of international communications with their home countries were either limited or expensive. The widespread use of the internet started in the mid-1990s [
78]. Internet-based voice and video communication became widely available to the public in subsequent years. Moreover, the proliferation of smartphones and various applications, such as WhatsApp, further enhanced the accessibility of cross-country communications. The difficulty of maintaining communications with their home country may have resulted in maintaining some outdated views about the home country’s health and ageing development.
For the second fold, (b) not being able to relate their view of ageing to that of the host population. Even when accompanied by preparation, migration is an unexpected live transition event [
57]. It imposes stressors on the average life cycle, altering how migrants live the expected and unexpected life events. It makes it challenging to share life experiences and events with own extended family members who remain in their home countries, imposing a stressor on the normal family life cycle where people expect to share these events. Migrants endure that and other life transition events over time within a changing social and physical landscape. In an ordinary life course, individuals are expected to draw on their social capital represented in their families, culture and language. However, migration pulls the individual away from most of their social capital, causing continuous stress. The magnitude of how migrants can overcome and compensate for these adverse effects of migration depends on their ability to adapt to the new host environment.
Furthermore, this adaptation depends also on external effects. Racism and discrimination may reduce migrants’ access to social and economic resources and alter their abilities to utilise available resources to reach their potential [
57]. Within the EMCA model [
55,
57], the stressor of racism is detrimental to health outcomes and overall behaviour across all life cycle stages, with isolation and depression as common symptoms in all migrants’ life cycle stages. All these other stressors combined with the dislocation away from social capital add complexity to the developmental course, including migrants’ views of later life [
57]. Older migrants may change their original wish of migration and think of a return to their home countries. The pile-up of stressors throughout their life following migration may lead some to more confusion about how they should view their ageing and whether they relate to the host population or their peers in their home countries [
55]. However, their view of ageing in their home countries is likely to be lagged back in time, and they may end up with an outdated view of ageing and “They are not here nor there” [
13].
Second question, (2) How outdated would that ageing view be for those who migrated in the early 1970s? For those who follow Path_1, their views are likely to be decades old, depending on their age at the time of migration. Such views are likely to be outdated enough to disrupt planning for ageing and later life and to encounter self-ageism earlier in life. This outdated view of ageing is not limited to the four countries in this study. Ageing transition is increasing rapidly, mainly in developing countries [
79]. For example, if we look at the Middle East and North Africa (MENA) region, in a country like Algeria, between 1960 to 2000, life expectancy at birth increased by 31 years [
61,
80] and similar increasing trends are observed in Tunisia, Iran, Lebanon, Bahrain and the United Arab Emirates. Average life expectancy at birth is the popular measure for what to expect to live on average, and earlier groups in the 1960 and 1970 did not have time to adjust or plan their lives accordingly. A similar argument can be drawn based on the average life expectancy at age 60, which increased during the same period from 14 to 22 years, resulting in 8 extra years above what was expected.
Globally, a person aged 60 in 2020 could expect to live, on average, an additional 22 years than in the 1960s; however, with great inequity in longevity and little evidence that older people today are in better health than previous generations [
79]. These rapid increases in life expectancy, in the absence of planning and awareness to change attitudes towards ageing, have adverse consequences. Most of these unexpected extra years are accompanied by ill health, negatively impacting the whole society [
79]. The fast-ageing transition is likely to be confusing at the individual level for people still living in their own countries [
51]. Hence, it is reasonable to assume more confusion for migrants from these countries who only witnessed the earlier time of the 1960s and 70s and did not witness that improvement in life expectancy and other health outcomes. Older migrants’ views of ageing are likely to be decades old, with a perception that is, by construction, more negative.
Following the migration event, migrants are expected to be pulled by various demands, including pressures to remit [
57]; hence they are unlikely to plan for ageing. Furthermore, reduced interactions with their older family members in their home countries make them unlikely to update their view of ageing. By the time they reach old age, they have little social interaction within their host communities. They will likely revert to the old perceptions they recall from their parents or grandparents before the migration event. Even though research shows socio-economic factors significantly impact health in later life, an outdated view of ageing can compound that effect.
It is logical to assume that when there is public trust in health research, including how participants and data are treated, then the public is likely to follow the recommendations based on such research. However, evidence shows that trust in health research is not shared among people from different ethnic groups in the UK. A recent public attitude survey towards health research in the UK reported that only 35% of ethnic minority respondents believed they would be treated with dignity and respect in research compared to 52% of white respondents [
49]. Furthermore, only 26% of ethnic minority respondents were very confident about their data security compared to 37% of white respondents. These results could be translated to the probability of an individual from each group accepting a public health innovation. It shows reduced trust, which is linked to earlier negative experiences and may lead to more separation from the surrounding environment [
26,
27]. This would also hinder the possibility of altering their views of ageing when compared to the majority population. Such detachment is likely to entrench the old views of ageing as facts. The results in
Table 2 can be thought of as based on an equal probability of accepting a public health innovation across the four groups. However, if we consider these public attitude figures, the actual results should reflect a broader gap that disadvantages ethnic minorities.
Third question, (3) What is the impact of the outdated ageing views on migrants’ health outcomes and healthy ageing in general? The answer is that it is likely to have negative impacts and confounding effects on achieving healthy ageing. Those who are pessimistic about their ageing are not likely to take advantage of health-promoting behaviour and habits. They are likely to prioritise many of the daily life demands over health monitoring, seeking early diagnosis and treatment. They are less likely to invest in planning or considering material resources for later life. The particulars of such effects are likely to be further associated with the individual culture and personality.
Figure 2 highlights a window of opportunity to target those younger migrants, aged 30 or less, with targeted innovation and information about healthy ageing and planning resources for later stages of life. Migrants appear to suffer from lesser social contact in older age than the UK host population, which should be considered when planning public health interventions.
The World Health Organisation WHO “Decades of healthy ageing” report [
46] emphasises changing perceptions towards ageing, which is directly linked to the diffusion of information. For example, the report calls for developing and implementing activities to reduce self-directed ageism and health promotion throughout life-course to build and maintain physical and mental health. These recommendations can be translated as targeting older groups to eliminate or reduce self-ageism. However, in this study, these groups are of low contact rate (1.4,1.2,1.4) for the age group of 50–65 (India, Pakistan, Turkey) and consequently low diffusion of innovation rates. Therefore, based on the diffusion model presented here, Equation (2) and the contact matrices,
Figure 1, a long-term strategy should target the younger age groups of 00–20 and 20–30. These groups have the highest daily rate of contact (14.1, 21.2,12.1) for the youngest age group (India, Pakistan, Turkey) and, consequently, the highest diffusion of innovations compared to other groups for the same countries.
The same report [
46] also calls for enabling people to continue to do what they value, even if they lose capacity. It also states that building and maintaining intrinsic capacity can be achieved by encouraging healthy ageing behaviour. However, the nature and types of encouragement and health behaviour should be culturally specific. For example, the report [
46] mentions reducing excessive alcohol intake. While this might be a clear health risk in some cultures, it will not be in others. Another call for action is reducing loneliness and social isolation by providing information and leisure and social activities opportunities. A practical approach for the propagation of interventions linked to reducing social isolation will require more understanding of the diffusion of innovation within a specific culture.
The Validity of the Internal-Influence Model for the Current Discussion and Its Limitation
The results presented in this paper are based on applying a mathematical model (Equation (2)) for a contagion paradigm of transmission of information via interpersonal contacts only. Furthermore, it uses the contact rates within the three countries are proxies for similar ethnic groups within the UK. These assumptions should be considered when planning public health interventions, for example, by either increasing the ratio of early adaptors within ethnic minority groups, designing interventions with more time to adapt the innovation or both. When the UK government started rolling out vaccinations for COVID-19, it was reported that vaccination uptake was slower among ethnic minority groups [
81]. The UK government responded by targeting the messages to local communities, effectively increasing the number of early adaptors and accelerating the diffusion of the innovation process allowing for better vaccination uptake rates.
The diffusion results presented in
Table 2 do not consider the transmission of information via external channels such as the media. However, including the mainstream media effect while changing the model to a mixed-influence model is unlikely to narrow the relative differentials in the diffusion speed but likely to widen the gap even further. Adding an external communication channel will likely lead to faster diffusion rates for all groups, but with different magnitudes, disadvantaging ethnic minorities even further. A coefficient of diffusion relating to the external channel,
, could be considered as a function of both the access to media channels and the trust in those channels.
The accessibility to different media channels could be assumed to be the same for all groups. However, the language and content complexities may favour the native population more, as they likely have rooted cultural aspects. With regards to trust, according to a survey by Runnymede Trust in 2014 [
82], 94% of Pakistanis in the UK thought the media portrayals of BME groups promote racism and that over two-thirds of Indians (68%) and Black Africans (67%) agree with that statement. Given these findings, it is reasonable to assume these figures reflect a lower level of trust in the media among ethnic minority groups compared to the white population. Based on accessibility and trust, adding an external influence for media is likely to benefit the host population with a faster adaptation of innovations, more than the ethnic minority groups. Based on these findings, the external diffusion was left out in the current study as it does not alter the discussion and focuses only on the internal-influence diffusion of innovation.
There are, however, other potential improvements for the internal influence model, such as employing the whole contact matrices to account for the effect of the cumulative interactions across all different age groups. As applied in this paper, social contact matrices have been well-established in epidemiological studies for examining the transmission dynamics of diverse infectious diseases [
83,
84,
85]. These matrices, derived from reputable sources [
47,
48], serve as valuable tools for understanding the patterns of social interactions and their implications for disease spread. Furthermore, the model could be extended to allow for a latent state. Within such an improved model, the potential adopter interacts with the earlier adopter taking some time to consider before either committing to adopt the innovation or decide not. Furthermore, within such a model, we can allow the individuals within the social system to grow older while exposed to innovation. However, such a flexible model, which employs a realistic age structure and multi-stage transitions, is more complex, and those flexibilities come with the cost of more parameters, with many unavailable or challenging to measure accurately. Additionally, while such an improved model could be beneficial for long-term policy planning, that kind of model is not particularly helpful for the specific focus of the current study. The use of modelling in this paper aims to contextualise the considerable differences in the diffusion of innovation between older ethnic minority groups compared to the general UK older population. However, the suitability of a diffusion model for a public health intervention will be specific to its context and should consider other factors [
86,
87,
88,
89,
90].







{kind=link}
{kind=link}
{kind=link}