



A Novel Edge-Computing-Based Framework for an Intelligent Smart Healthcare System in Smart Cities


 ,
,  ,
,  ,
,  , and
, and
Abstract
1. Introduction
- (i)
- Cloud computing is a kind of computing dependent on sharing computer assets in place of having local servers to address data packages. Through cloud computing, each type of processing and calculation related to sensitive user data is accomplished in the cloud. Previously for computing frameworks, the computer server or every other server has been in use. However, more advanced computing may now be achieved on the cloud. Figure 1 depicts the functionality of the cloud layer, fog layer, and body sensing layer in a standard design of a healthcare application. Currently, each business organization and venture is transforming towards cloud technology with the added advantage of fog computing.
- (ii)
- Fog computing is a decentralized computing infrastructure or method in which computing resources are located among the data supply and the cloud. Fog computing is a paradigm that provides offerings to user requests at the edge networks. The fog layer gadgets typically perform networking operations along with routers, gateways, bridges, and hubs. Researchers envision these gadgets to act simultaneously on each computational and networking process. However, these gadgets are resource-restricted compared to cloud servers. The geological spread and the decentralized nature help in supplying reliable services with coverage over a vast vicinity. Fog computing is the physical place of the gadgets that are much closer to the customers than the cloud servers. Despite the broad deployment of cloud computing, some systems and services still cannot take advantage of this trendy computing paradigm due to inherent problems of cloud architecture, such as undesirable delay, lack of mobility hold-up, and location awareness. As a result, the fog computing paradigm has developed as a potential infrastructure to provide efficient communiqué and resource consumption.
2. Related Work
3. Advanced Healthcare Using an IoT-Enabled System
3.1. Fog-Assisted Secured Healthcare
3.2. Healthcare Using Artificial Intelligence and Machine Learning Support
3.3. Healthcare Using Deep-Learning Methods
4. Mist-Enabled Smart Health System for a Smart City
4.1. System Architecture
4.2. The Hardware Component of the Mist-Enabled Smart Health Model
- Network of body area sensor devices: This part is made up of three primary sensing devices: health sensors and activity sensors with environmental sensors. Electrocardiogram sensors, electroencephalogram sensors, electromyography sensors, respiratory sensors, thermocouple sensors, and differential pressure sensors with potentiometric sensors are among the medical sensors available. These components are responsible for transferring the data from the patient’s body through associated gateway devices.
- Gateway: Overall, three kinds of gateway gadgets (cell phones, laptops, as well as tablets) operate even as mist nodes, acquiring data from various sensors and forwarding them to broker/worker units for some further assessment.
- Mist–fog bus modules: The below are indeed the components of the mist–fog bus structure:
- The broker node collects the task requests and input data from gateway endpoints. Before sending data, the request input module accepts job requests from gateway devices. To enhance overall trustworthiness and data security, the Security Supervisor module enables protected interactions between two units and prevents this acquired data from unwanted access or harmful alteration. The load statistics among all worker nodes supply into the arbitration module (a component of the resource supervisor on the broker node), which then decides in real time whether this is the same end node or a subset of end nodes to send jobs to.
- Worker node: One module that handles assigned jobs is the broker node’s resource supervisor. Embedded types of equipment, single-board computers (SBCs) such as Raspberry Pis, can be used as worker nodes. Worker nodes in MistBus can also use advanced deep-learning models to analyze and interpret data as well as generate recommendations. Other features such as computerized information, data purification with mining, big data analytics, as well a repository can be added to the worker node. Through the gateway devices, the worker nodes receive input data, produce results, and communicate them with the gateway devices. In this proposed framework, if it requires this, the broker end node can act similarly to the worker node.
- Cloud Data Center: This mist-enabled innovative health utilizes the fog infrastructure or Cloud Data Center resources if this mist framework becomes overcrowded, services are latency tolerant, or the length of incoming data is significantly more prominent than a typical one.
4.3. The Mist-Enabled Smart Health Model Software Components
- Data cleaning and pre-processing: Pre-processing data is the first action once submitted. It also involves employing data analytics technologies to filter information. To obtain essential ingredients of data feature vectors that influence patient health conditions, the filtered data are condensed to a smaller size using Principal Component Analysis (PCA) adopting Set Partition [41] and protected using the Singular Value Decomposition (SVD) technique [42]. It immediately concludes the input data, then suggests medicine and appropriate check-ups depending on the continually trained data-related healthcare professionals, and preserves it in a database for re-training as required.
- Resource supervisor: Workload management and arbitration modules [43] are the two elements that define this framework. The workload manager keeps track of job requests and task queues for data processing. It also maintains large amounts of data that must be evaluated. The arbitration component assigns the mist, fog, or cloud resources that have been provided for processing tasks that have been scheduled and handled through this workload supervisor. The arbitration part is embedded with this broker end node and evaluates whether the fog computing node, the fog worker end node, or the Cloud Data Center must give this information to find outcomes [43]. To balance the load and ensure optimal performance, the fundamental purpose is to divide tasks across multiple devices. Users can customize their load balancing and arbitration techniques depending on their application needs with mist-enabled innovative health.
- Deep-learning module: The dataset is used to develop a neural network for identifying data endpoints that will feature vectors created following the pre-processing of this information acquired through this wireless body area network. This anticipates and processes output for this information gained through these intelligent gateway gadgets depending on the task assigned by the resource supervisor.
- Ensembling module: This component takes the results from many models and utilizes polling to measure the output class; that is, whether or not the individual has cardiovascular disease. The feature is located on the task-assigned FogBus node and is responsible for relaying and gathering reliable out-run through various worker end nodes.
4.4. Sequence of Communication
4.5. Proposed Work
4.6. Resource Scheduling Algorithm for Mist Layer
| Algorithm 1 Algorithm for Resource Scheduling in the Mist Layer |
| Input: Output: Initialize: Set the threshold value for the worker load set of tasks to be executed Set of worker load Set of workers if do else end if return exit |
4.7. Q-Reinforcement Learning over Mist (QRLM) Algorithm
| Algorithm 2 QRLM Algorithm |
| function QRLM Input: Output: Initialize: Set of states Set of actions Probability of transitioning the present state Set of rewards Reward discount factor Compute: for do if and do end if end for return exit |
4.8. Experimental Setup
- ▪
- Samsung Galaxy S7 with Android 9 is taken as the gateway device;
- ▪
- Dell XPS 13 with Intel (R) Core (TM) i5-7200 CPU as the broker node;
- ▪
- Worker Node: Raspberry Pi 3B+, ARM Cortex-A53 quad-core SoC CPU @ 1.4 GHz as a worker node;
- ▪
- Microsoft Azure, 1 GB RAM, as a mist node.
4.9. Data Set
- Age: the person’s age in years;
- Sex: a binary value (1 = male, 0 = female);
- Cp: the type of chest pain;
- Resting cardiographic data (0 for normal);
- Cholesterol (in mg/dL);
- Blood sugar (>120 mg/dL);
- Blood pressure at rest (mmHg);
- ST elevation (0.05 mv);
- Maximum heart rate;
- ST depression;
- ST segment slope;
- Colored fluorescence;
- Heart disease target;
- Angiography status (value between 0 and 1).
5. Results and Discussions
5.1. Performance Measurement Characteristics
- Correctness: 30% of the dataset’s data were used for testing, while 70% were used to train the model. To create the corresponding trained deep-learning framework, all the worker/broker nodes received an equal distribution. Since the volume of mist nodes increases, it would be necessary to send the dataset examples to every node to utilize all training resources. This not only cuts down on training time but also improves exam accuracy. The training and test accuracies were examined to see any such impacts. The proportion of all patients for whom this framework correctly predicts whether or not they have heart disease is known as accuracy. With different mist conditions, we changed the number of edge nodes and whether or not the results are assembled to test accuracy levels.
- Time factor: Arbitration time, latency, execution time, and jitter are examples of the time factor. We compared these temporal characteristics for several mist configurations, such as cloud-only computing architecture, up to two edge nodes (with or without ensembling), and no edge nodes.
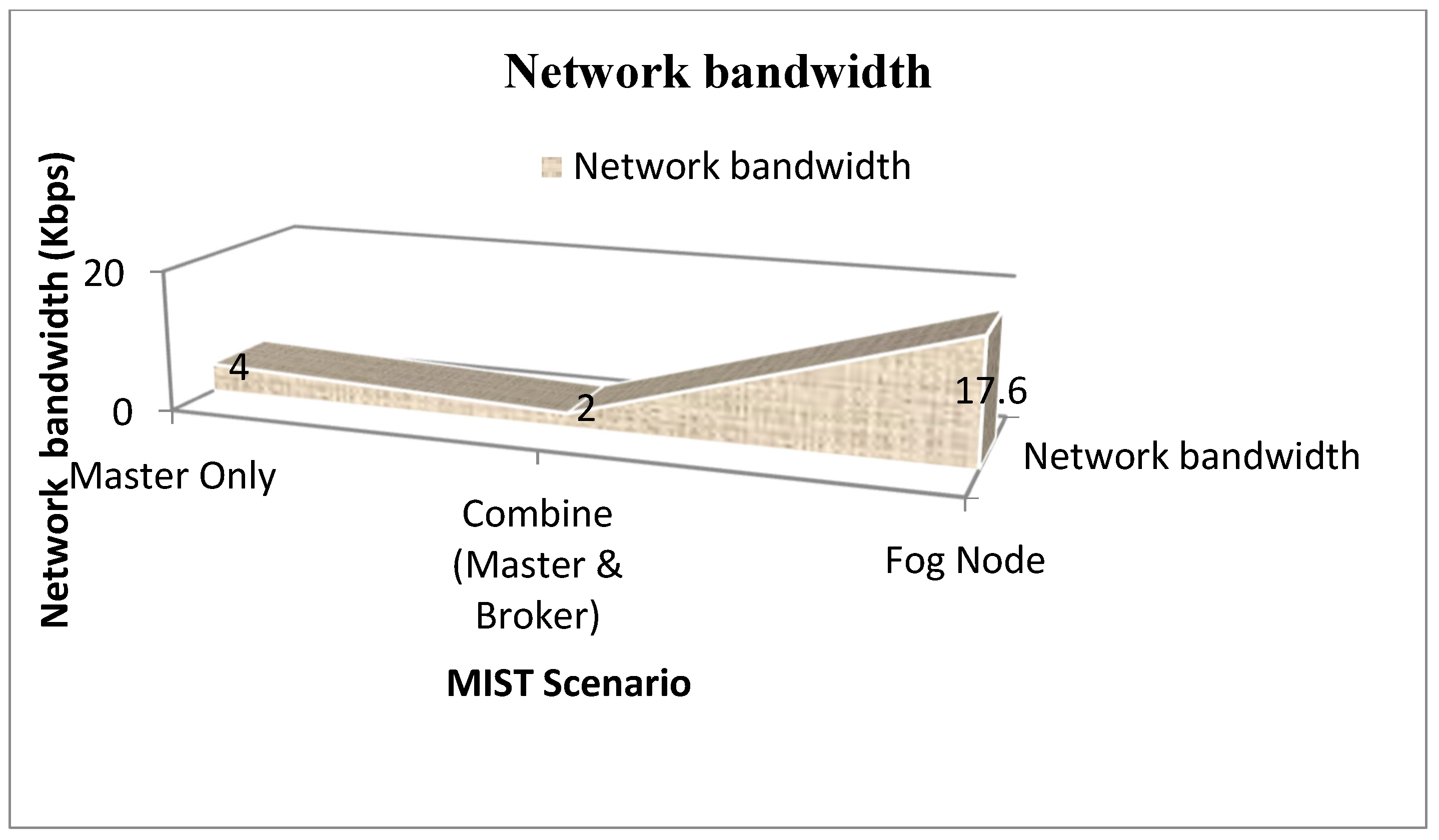
- Utilization of network bandwidth: This was examined to ascertain network use in various scenarios because the scenario (broker alone, workers, or cloud) and the number of worker nodes impact network consumption. Like the testing for time parameters, we compared the network bandwidth used for the various mist scenarios. This was done to ascertain how bandwidth utilization and the different mist configurations that HealthMist offers relate to one another.
- Energy consumption: Because energy is such an essential factor in the transition from cloud to mist layer, we looked into energy usage in various environments. We looked at the different HealthMist setups used for diverse individuals.
5.2. Parameter Comparison and Discussion
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Venkatesh, J.; Aksanli, B.; Chan, C.S.; Akyurek, A.S.; Rosing, T.S. Modular and Personalized Smart Health Application Design in a Smart City Environment. IEEE Internet Things J. 2018, 5, 614–623. [Google Scholar] [CrossRef]
- Rani, S.; Ahmed, S.H.; Shah, S.C. Smart Health: A Novel Paradigm to Control the Chikungunya Virus. IEEE Internet Things J. 2019, 6, 1306–1311. [Google Scholar] [CrossRef]
- Islam, S.M.R.; Kwak, D.; Kabir, M.H.; Hossain, M.; Kwak, K.-S. The Internet of Things for Health Care: A Comprehensive Survey. IEEE Access 2015, 3, 678–708. [Google Scholar] [CrossRef]
- Sengupta, S.; Bhunia, S.S. Secure Data Management in Cloudlet Assisted IoT Enabled e-Health Framework in Smart City. IEEE Sens. J. 2020, 20, 9581–9588. [Google Scholar] [CrossRef]
- Pathinarupothi, R.K.; Durga, P.; Rangan, E.S. IoT-Based Smart Edge for Global Health: Remote Monitoring With Severity Detection and Alerts Transmission. IEEE Internet Things J. 2019, 6, 2449–2462. [Google Scholar] [CrossRef]
- Zhou, Z.; Yu, H.; Shi, H. Human Activity Recognition Based on Improved Bayesian Convolution Network to Analyze Health Care Data Using Wearable IoT Device. IEEE Access 2020, 8, 86411–86418. [Google Scholar] [CrossRef]
- Liu, L.; Xu, J.; Huan, Y.; Zou, Z.; Yeh, S.-C.; Zheng, L.-R. A Smart Dental Health-IoT Platform Based on Intelligent Hardware, Deep Learning, and Mobile Terminal. IEEE J. Biomed. Health Inform. 2020, 24, 898–906. [Google Scholar] [CrossRef]
- Verma, P.; Sood, S.K. Fog Assisted-IoT Enabled Patient Health Monitoring in Smart Homes. IEEE Internet Things J. 2018, 5, 1789–1796. [Google Scholar] [CrossRef]
- Alshehri, F.; Muhammad, G. A Comprehensive Survey of the Internet of Things (IoT) and AI-Based Smart Healthcare. IEEE Access 2021, 9, 3660–3678. [Google Scholar] [CrossRef]
- Ray, P.P.; Thapa, N.; Dash, D. Implementation and Performance Analysis of Interoperable and Heterogeneous IoT-Edge Gateway for Pervasive Wellness Care. IEEE Trans. Consum. Electron. 2019, 65, 464–473. [Google Scholar] [CrossRef]
- Krall, A.; Finke, D.; Yang, H. Mosaic Privacy-Preserving Mechanisms for Healthcare Analytics. IEEE J. Biomed. Health Inform. 2021, 25, 2184–2192. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, W.; Helal, S.; Khaled, A.; Hutchinson, W. IoTility: Architectural Requirements for Enabling Health IoT Ecosystems. IEEE Trans. Emerg. Top. Comput. 2021, 9, 1206–1218. [Google Scholar] [CrossRef]
- Vedaei, S.S.; Fotovvat, A.; Mohebbian, M.R.; Rahman, G.M.E.; Wahid, K.A.; Babyn, P.; Marateb, H.R.; Mansourian, M.; Sami, R. COVID-SAFE: An IoT-Based System for Automated Health Monitoring and Surveillance in Post-Pandemic Life. IEEE Access 2020, 8, 188538–188551. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Xiong, H.; Liu, X.; Zhang, Y.; Nie, X.; Deng, R.H. Lightweight and Privacy-Aware Fine-Grained Access Control for IoT-Oriented Smart Health. IEEE Internet Things J. 2020, 7, 6566–6575. [Google Scholar] [CrossRef]
- Yu, H.; Zhou, Z. Optimization of IoT-Based Artificial Intelligence Assisted Telemedicine Health Analysis System. IEEE Access 2021, 9, 85034–85048. [Google Scholar] [CrossRef]
- Zhang, H.; Li, J.; Wen, B.; Xun, Y.; Liu, J. Connecting Intelligent Things in Smart Hospitals Using NB-IoT. IEEE Internet Things J. 2018, 5, 1550–1560. [Google Scholar] [CrossRef]
- Wu, T.; Wu, F.; Qiu, C.; Redouté, J.-M.; Yuce, M.R. A Rigid-Flex Wearable Health Monitoring Sensor Patch for IoT-Connected Healthcare Applications. IEEE Internet Things J. 2020, 7, 6932–6945. [Google Scholar] [CrossRef]
- Zhou, R.; Zhang, X.; Wang, X.; Yang, G.; Guizani, N.; Du, X. Efficient and Traceable Patient Health Data Search System for Hospital Management in Smart Cities. IEEE Internet Things J. 2021, 8, 6425–6436. [Google Scholar] [CrossRef]
- Mercuri, M.; Sacco, G.; Hornung, R.; Zhang, P.; Visser, H.J.; Hijdra, M.; Liu, Y.-H.; Pisa, S.; Van Liempd, B.; Torfs, T. 2-D Localization, Angular Separation and Vital Signs Monitoring Using a SISO FMCW Radar for Smart Long-Term Health Monitoring Environments. IEEE Internet Things J. 2021, 8, 11065–11077. [Google Scholar] [CrossRef]
- Kumar, A.; Krishnamurthi, R.; Nayyar, A.; Sharma, K.; Grover, V.; Hossain, E. A Novel Smart Healthcare Design, Simulation, and Implementation Using Healthcare 4.0 Processes. IEEE Access 2020, 8, 118433–118471. [Google Scholar] [CrossRef]
- Khansari, S.M.; Arbabi, F.; Moazen Jamshidi, M.H.; Soleimani, M.; Ebrahimi, P. Health Services and Patient Satisfaction in IRAN during the COVID-19 Pandemic: A Methodology Based on Analytic Hierarchy Process and Artificial Neural Network. J. Risk Financ. Manag. 2022, 15, 288. [Google Scholar] [CrossRef]
- Alabdulatif, A.; Khalil, I.; Saidur Rahman, M. Security of Blockchain and AI-Empowered Smart Healthcare: ApplicationBasedAnalysis. Appl. Sci. 2022, 12, 11039. [Google Scholar] [CrossRef]
- Firouzi, F.; Farahani, B.; Daneshmand, M.; Grise, K.; Song, J.; Saracco, R.; Wang, L.L.; Lo, K.; Angelov, P.; Soares, E.; et al. Harnessing the Power of Smart and Connected Health to Tackle COVID-19: IoT, AI, Robotics, and Blockchain for a Better World. IEEE Internet Things J. 2021, 8, 12826–12846. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.; Zafar, K.; Baig, A.R. Fog-Centric IoT Based Framework for Healthcare Monitoring, Management and Early Warning System. IEEE Access 2021, 9, 74168–74179. [Google Scholar] [CrossRef]
- Mclennan, S.; Kahrass, H.; Wieschowski, S.; Strech, D.; Langhof, H. The spectrum of ethical issues in a Learning Health Care System: A systematic qualitative review. Int. J. Qual. Health Care 2018, 30, 161–168. [Google Scholar] [CrossRef]
- Panesar, S.; Cagle, Y.; Chander, D.; Morey, J.; Fernandez-Miranda, J.; Kliot, M. Artificial Intelligence and the Future of Surgical Robotics. Ann. Surg. 2019, 270, 223–226. [Google Scholar] [CrossRef]
- Rozario, M.; Zainuddin, A.A.; Gamage, S.A. Artificial Intelligence and Machine learning in the Healthcare Sector: A Review. Malays. J. Sci. Adv. Technol. 2021, 3, 89–96. [Google Scholar] [CrossRef]
- Firyulina, M.A.; Kashirina, I.L. Using of machine learning methods in cardiology. J. Phys. Conf. Ser. 2021, 1902, 012135. [Google Scholar] [CrossRef]
- Secinaro, S.; Calandra, D.; Secinaro, A.; Muthurangu, V.; Biancone, P. The role of artificial intelligence in healthcare: A structured literature review. BMC Med. Inform. Decis. Mak. 2021, 21, 1–23. [Google Scholar] [CrossRef]
- Kar, U.K.; Dash, R. The Future of Health and Healthcare in a World of Artificial Intelligence. Arch. Biotechnol. Biomed. 2018, 1. [Google Scholar] [CrossRef]
- Rodriguez-Romero, V.; Bergstrom, R.F.; Decker, B.S.; Lahu, G.; Vakilynejad, M.; Bies, R.R. Prediction of Nephropathy in Type 2 Diabetes: An Analysis of the ACCORD Trial Applying Machine Learning Techniques. Clin. Transl. Sci. 2019, 12, 519–528. [Google Scholar] [CrossRef]
- Kwak, G.H.; Hui, P. DeepHealth: Review and Challenges of Artificial Intelligence in Health Informatics, No. Ml. arXiv 2019, arXiv:arXiv: 1909.00384. [Google Scholar]
- Hu, Y.; Wang, B.; Sun, Y.; An, J.; Wang, Z. Graph-Based Semi-Supervised Learning for Activity Labeling in Health Smart Home. IEEE Access 2020, 8, 193655–193664. [Google Scholar] [CrossRef]
- Yang, S.; Zhu, F.; Ling, X.; Liu, Q.; Zhao, P. Intelligent Health Care: Applications of Deep Learning in Computational Medicine. Front. Genet. 2021, 12, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Kaul, D.; Raju, H.; Tripathy, B.K. Deep Learning in Healthcare. In Study in Big Data; Springer: Berlin/Heidelberg, Germany; Volume 91, pp. 97–115. [CrossRef]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Toh, C.; Brody, J.P. Applications of Machine Learning in Healthcare. In Smart Manufacturing—When Artificial Intelligence Meets the Internet of Things; IntechOpen: London, UK, 2021; pp. 1–25. [Google Scholar] [CrossRef]
- Garcia, P.S.R.; Kleinschmidt, J.H. Sharing Health and Wellness Data with Blockchain and Smart Contracts. IEEE Lat. Am. Trans. 2020, 18, 1026–1033. [Google Scholar] [CrossRef]
- Meneghello, F.; Calore, M.; Zucchetto, D.; Polese, M.; Zanella, A. IoT: Internet of Threats? A Survey of Practical Security Vulnerabilities in Real IoT Devices. IEEE Internet Things J. 2019, 6, 8182–8201. [Google Scholar] [CrossRef]
- Vecchiola, C.; Chu, X.; Buyya, R. Aneka: A software platform for NET-based cloud computing. High Speed Large Scale Sci. Comput. 2009, 18, 267–295. [Google Scholar]
- Hsieh, J.H.; Lee, R.C.; Hung, K.C.; Shih, M.J. Rapid and coding-efficient SPIHT algorithm for wavelet-based ECG data compression. Integr. VLSI J. 2018, 60, 248–256. [Google Scholar] [CrossRef]
- Liu, T.Y.; Lin, K.Y.; Wu, H.C. ECG Data Encryption Then Compression Using Singular Value Decomposition. IEEE J. Biomed. Health Inform. 2017, 22, 707–713. [Google Scholar] [CrossRef]
- Tuli, S.; Mahmud, R.; Tuli, S.; Buyya, R. FogBus: A Blockchain-based Lightweight Framework for Edge and Fog Computing. J. Syst. Softw. 2019, 154, 22–36. [Google Scholar] [CrossRef]
- Dua, D.; Graff, C. UCI Machine Learning Repository; University of California, School of Information and Computer Science: Irvine, CA, USA, 2019; Available online: http://archive.ics.uci.edu/ml (accessed on 7 October 2022).
- Kato, N.; Loh, M.; Takeuchi, F.; Verweij, N.; Wang, X.; Zhang, W.; Tanika, N.; Kelly, T.; Saleheen, D.; Lehne, B.; et al. Trans-ancestry genomewide association study identifies 12 genetic loci influencing blood pressure and implicates a role for DNA methylation. Nat. Genet. 2015, 47, 1282–1293. [Google Scholar] [CrossRef]
- Sanghera, D.K.; Been, L.; Ortega, L.; Wander, G.S.; Mehra, K.N.; Aston, C.E.; Mulvihill, J.J.; Ralhan, S. Testing the association of novel meta-analysis-derived diabetes risk genes with type II diabetes and related metabolic traits in Asian Indian Sikhs. J. Hum. Genet. 2009, 54, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Malik, R.; Chauhan, G.; Traylor, M.; Sargurupremraj, M.; Okada, Y.; Mishra, A.; Rutten-Jacobs, L.; Giese, A.-K.; Van der Lann, S.W.; Gretarsdottir, S.; et al. Multiancestry genome-wide association study of 520,000 subjects identifies 32 loci associated with stroke and stroke subtypes. Nat. Genet. 2018, 50, 524. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref | Artificial Intelligence/Machine Learning Technique | Focus/Contribution | Limitations |
|---|---|---|---|
| [25] | Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement as far as applicable to qualitative evidence syntheses. | This study provides a thorough summary of the ethical concerns raised by LHCS and emphasizes the significance of striking a balance between the social goal of bettering healthcare and the need to safeguard and respect individual participants. | Discussion of challenges with interpretations is limited. This process should ensure as much as possible the reliability and validity of the findings. |
| [26] | Smart Tissue Autonomous Robot (STAR) against conventional surgical techniques. | The study investigated the augmentation of surgical capabilities to improve outcomes and broadened access to care that may be made possible by the combination of AI and surgical robotics. | The study fails to extensively explain early designs, which are likely to be expensive and have a limited number. Adoption of new technologies where underserved medical contexts provided their clinical efficacy is established and their technology is continuously improved. |
| [27] | Qualitative research method. It is a method of research that relies on non-numerical and unstructured data; the research is based on secondary data. Support vector machine (SVM), 3D convolution neural networks. | The growing usage of technology in the industry makes information systems project management in healthcare relevant. The Internet of Things, artificial intelligence, augmented reality, and big data are just a few of the technologies that are being deployed. | The pandemic situation is discussed, but no primary data were used, which may have produced better findings. |
| [28] | Classification trees (decision trees) are visual and easily interpretable models for solving regression and classification problems. | The tasks completed in the project “Development and research of machine learning methods in the issues of diagnosis and assistance of patients with illnesses of the cardiovascular system” are summarized in this article. | Precision is insufficient for machine-learning models to work properly. One field where the results’ interpretability is crucial is medicine. Understanding why the model anticipated a certain result is crucial for clinicians to use the system effectively. |
| [29] | Qualitative and quantitative factors. Additionally, the Bibliometrix R software package was helpful for the paper. | The study revealed that there is a growing body of literature in this area. It focuses on clinical decision-making, patient data and diagnostics, health services management, and predictive medicine. | There are currently some limitations that will affect future research potential, especially in ethics, data governance, and the competencies of the health workforce. |
| [30] | They used two machine-learning models, i.e., Support Vector Machines (SVM) and Random Forest (RF) and their results showed a staggering agreement with related works. | The technological advancement in mobile computing, artificial neural networks, robotics, the storage of huge data on the internet, cloud-based machine learning, information processing algorithms, etc., has propelled the use of AI in modern healthcare. | The study needs to address technical difficulties during a surgical procedure. Moreover, complicated surgical interventions need cognitive as well as decision-making skills. |
| [31] | Random Forest and Simple Logistic Regression methods | Age, urine albumin excretion, low-density lipoprotein, triglycerides, cholesterol, and glomerular filtration rate (GFR) have all been identified as risk factors for DN.Additionally, fasting plasma glucose (FPG), potassium, and changes in FPG and GFR after year 1 were identified as early and late biomarkers of DN, respectively, using ML approaches. | |
| [32] | The work reviewed various deep-learning architectures, such as the convolutional neural network (CNN), recurrent neural network (RNN), graph neural network (GNN), autoencoder (AE), Boltzmann machine (RBM), and deep belief network (DBN), as well as their variations that incorporate transfer learning, attention learning, and reinforcement learning. | A thorough analysis of the previous seven years’ worth of work in the domains of genetics, sensing, internet communication health, electronic health records, medical imaging, and artificial intelligence in health informatics. | The fact that current research is reliant on retrospective data from hospitals that are easily shareable datasets raises the possibility of data contradiction and bias. We see missing value issues due to patient transfers, poor chart maintenance, and procedural tendencies. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tripathy, S.S.; Imoize, A.L.; Rath, M.; Tripathy, N.; Bebortta, S.; Lee, C.-C.; Chen, T.-Y.; Ojo, S.; Isabona, J.; Pani, S.K. A Novel Edge-Computing-Based Framework for an Intelligent Smart Healthcare System in Smart Cities. Sustainability 2023, 15, 735. https://doi.org/10.3390/su15010735
Tripathy SS, Imoize AL, Rath M, Tripathy N, Bebortta S, Lee C-C, Chen T-Y, Ojo S, Isabona J, Pani SK. A Novel Edge-Computing-Based Framework for an Intelligent Smart Healthcare System in Smart Cities. Sustainability. 2023; 15(1):735. https://doi.org/10.3390/su15010735
Chicago/Turabian StyleTripathy, Subhranshu Sekhar, Agbotiname Lucky Imoize, Mamata Rath, Niva Tripathy, Sujit Bebortta, Cheng-Chi Lee, Te-Yu Chen, Stephen Ojo, Joseph Isabona, and Subhendu Kumar Pani. 2023. "A Novel Edge-Computing-Based Framework for an Intelligent Smart Healthcare System in Smart Cities" Sustainability 15, no. 1: 735. https://doi.org/10.3390/su15010735
APA StyleTripathy, S. S., Imoize, A. L., Rath, M., Tripathy, N., Bebortta, S., Lee, C.-C., Chen, T.-Y., Ojo, S., Isabona, J., & Pani, S. K. (2023). A Novel Edge-Computing-Based Framework for an Intelligent Smart Healthcare System in Smart Cities. Sustainability, 15(1), 735. https://doi.org/10.3390/su15010735