
Hospital Plate Waste Assessment after Modifications in Specific Dishes of Flexible and Inflexible Food Ordering Systems

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
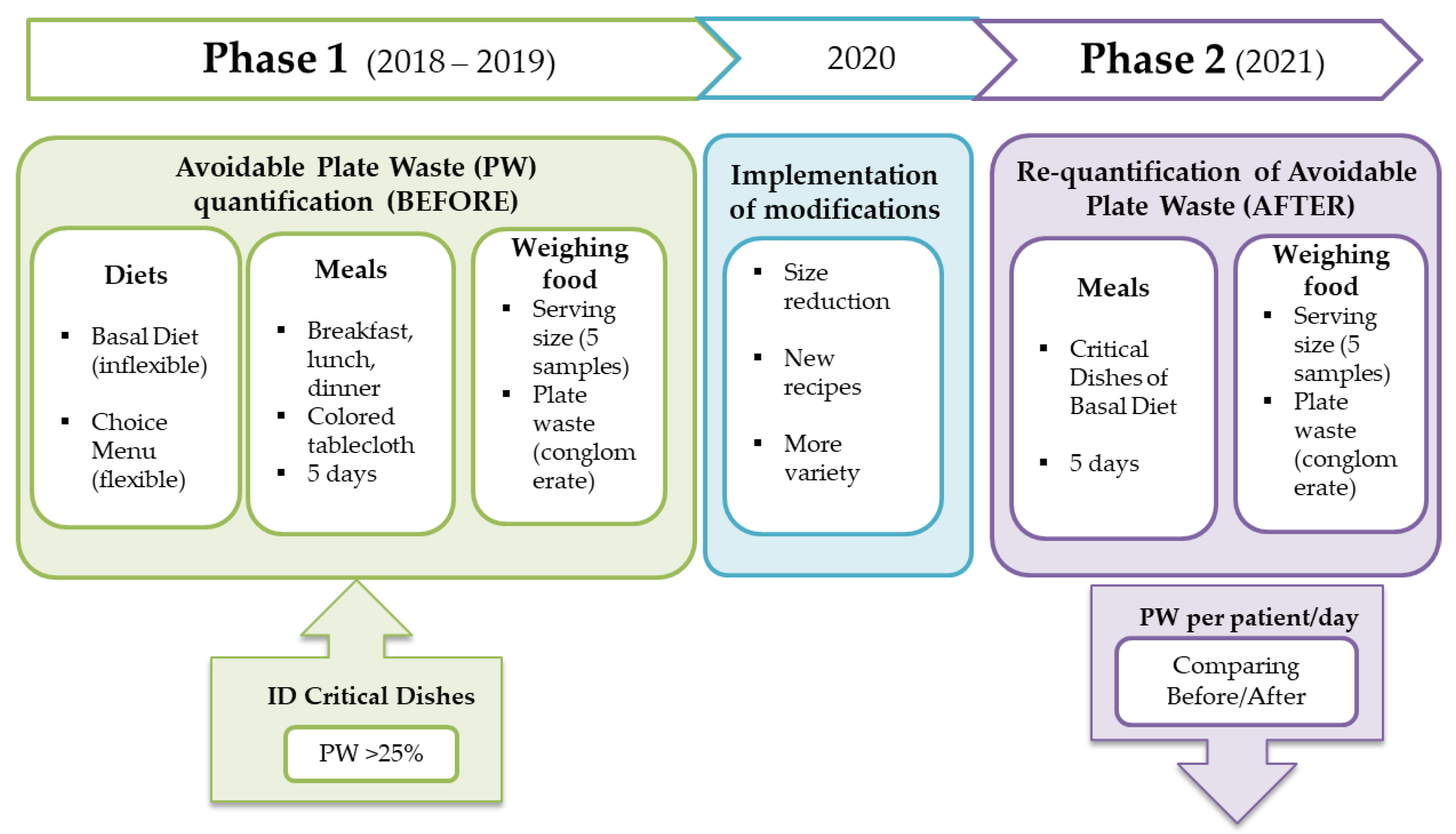
2.1. Case Study Description
2.2. Food Waste Quantification Method
2.3. Statistical Analysis
3. Results
3.1. Phase 1: Plate Waste Analysis before Modifications
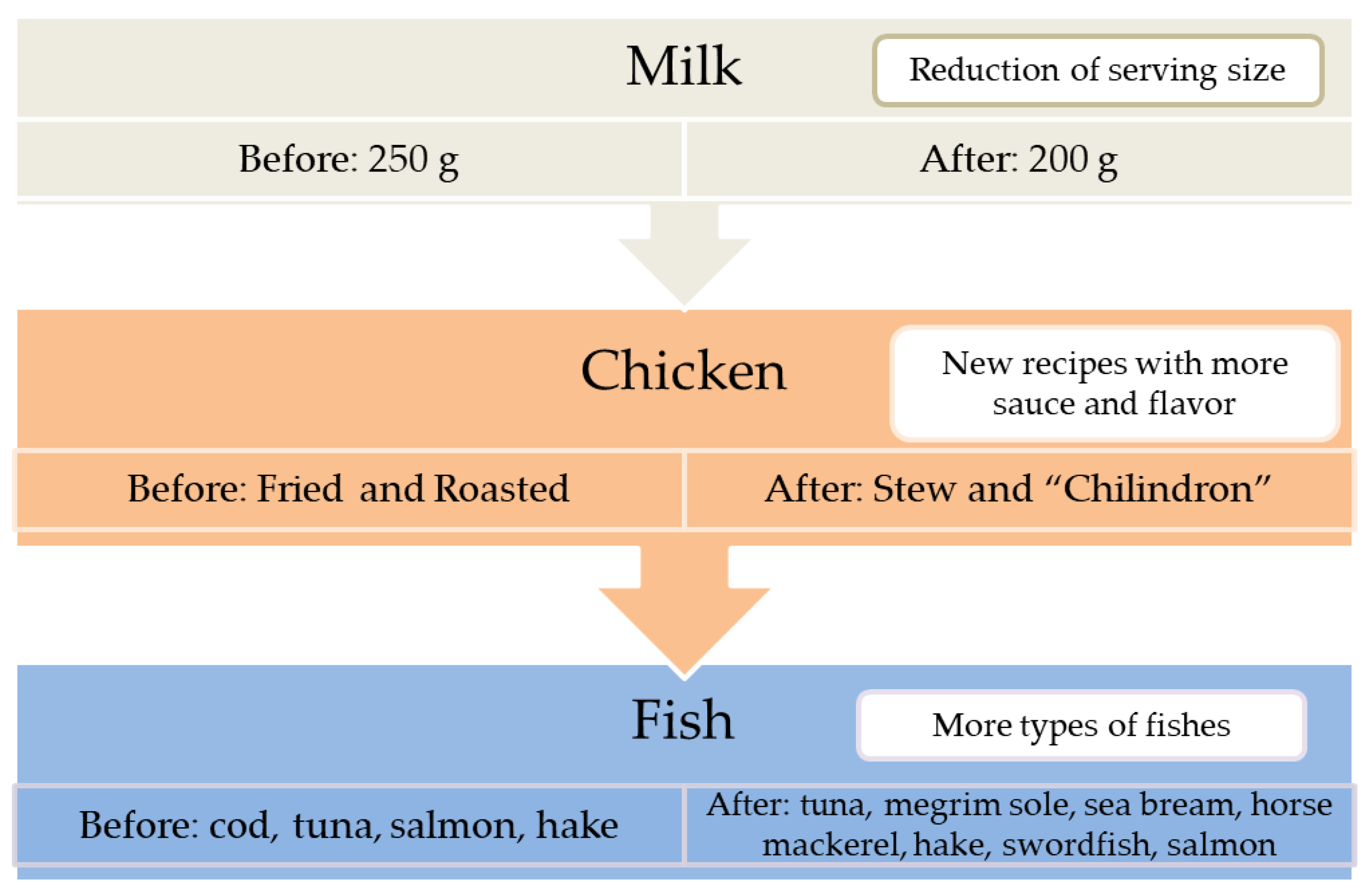
3.2. Phase 2: Plate Waste Analysis after Modifications
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- ONU. 17 SDG History; ONU: New York, NY, USA; Available online: https://sdgs.un.org/goals (accessed on 23 July 2021).
- Poore, J.; Nemecek, T. Reducing Food’s Environmental Impacts through Producers and Consumers. Science 2018, 360, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Crippa, M.; Solazzo, E.; Guizzardi, D.; Monforti-Ferrario, F.; Tubiello, F.N.; Leip, A. Food Systems Are Responsible for a Third of Global Anthropogenic GHG Emissions. Nat. Food 2021, 2, 198–209. [Google Scholar] [CrossRef]
- Mestre Montserrat, M.; Martínez Sánchez, V. Desperdicio Alimentario, Análisis de Una Problemática Poliédrica. Pap. Relac. Ecosociales Cambio Glob. 2013, 139, 93–103. [Google Scholar] [CrossRef]
- FAO; IFAD; UNICEF; WFP; WHO. Brief to The State of Food Security and Nutrition in the World 2020; FAO: Rome, Italy; IFAD: Rome, Italy; WFP: Rome, Italy; UNICEF: New York, NY, USA, 2020. [Google Scholar] [CrossRef]
- Stenmarck, A.; Jensen, C.; Quested, T.; Moates, G.; Buksti, M.; Cseh, B.; Juul, S.; Parry, A.; Politano, A.; Redlingshofer, B.; et al. Estimates of European Food Waste Levels; FUSION EU: Oxfordshire, UK, 2016. [Google Scholar]
- UNEP. Food Waste Index Report 2021; UNEP: Nairobi, Kenya, 2021. [Google Scholar]
- Carino, S.; Porter, J.; Malekpour, S.; Collins, J. Environmental Sustainability of Hospital Foodservices across the Food Supply Chain: A Systematic Review. J. Acad. Nutr. Diet. 2020, 120, 825–873. [Google Scholar] [CrossRef] [PubMed]
- Van Bokhorst-De Van Der Schueren, M.A.E.; Roosemalen, M.M.; Weijs, P.J.M.; Langius, J.A.E. High Waste Contributes to Low Food Intake in Hospitalized Patients. Nutr. Clin. Pract. 2012, 27, 274–280. [Google Scholar] [CrossRef]
- ONU. Goal 12: Responsible Consumption and Production; ONU: Ada, OH, USA; Available online: https://www.un.org/sustainabledevelopment/sustainable-consumption-production (accessed on 23 July 2021).
- HCWH Europe. Fresh, Healthy, and Sustainable Food. Best Practices in European Healthcare; HCWH Europe: Brussels, Belgium; Berlin, Germany, 2016; Volume 57. [Google Scholar]
- HCWH Europe. El Proyecto MECAHF; HCWH Europe: Brussels, Belgium, 2020. [Google Scholar]
- Antasouras, G.; Vasios, G.K.; Kontogiorgis, C.; Ioannou, Z.; Poulios, E.; Deligiannidou, G.-E.; Troumbis, A.Y.; Giaginis, C. How to improve food waste management in hospitals through focussing on the four most common measures for reducing plate waste. Int. J. Health Plann. Mgmt. 2022, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Strotmann, C.; Göbel, C.; Friedrich, S.; Kreyenschmidt, J.; Ritter, G.; Teitscheid, P. A Participatory Approach to Minimizing Food Waste in the Food Industry-A Manual for Managers. Sustainability 2017, 9, 66. [Google Scholar] [CrossRef]
- BEDCA. Base de Datos española de Composición de Alimentos. Available online: https://www.bedca.net/bdpub/index.php (accessed on 30 June 2021).
- Strotmann, C.; Friedrich, S.; Kreyenschmidt, J.; Teitscheid, P.; Ritter, G. Comparing Food Provided and Wasted before and after Implementing Measures against Food Waste in Three Healthcare Food Service Facilities. Sustainability 2017, 9, 1409. [Google Scholar] [CrossRef]
- Alharbi, N.S.; Qattan, M.Y.; Alhaji, J.H. Towards Sustainable Food Services in Hospitals: Expanding the Concept of “plate Waste” to “Tray Waste”. Sustainability 2020, 12, 6872. [Google Scholar] [CrossRef]
- Aminuddin, N.F.; Kumari Vijayakumaran, R.; Abdul Razak, S. Patient Satisfaction With Hospital Food Service and Its Impact on Plate Waste in Public Hospitals in East Malaysia. Hosp. Pract. Res. 2018, 3, 90–97. [Google Scholar] [CrossRef]
- Eriksson, M.; Malefors, C.; Bergström, P.; Eriksson, E.; Osowski, C.P. Quantities and Quantification Methodologies of Food Waste in Swedish Hospitals. Sustainability 2020, 12, 3116. [Google Scholar] [CrossRef]
- Gomes, A.; Saraiva, C.; Esteves, A.; Gonçalves, C. Evaluation of Hospital Food Waste-A Case Study in Portugal. Sustainability 2020, 12, 6157. [Google Scholar] [CrossRef]
- Navarro, D.A.; Boaz, M.; Krause, I.; Elis, A.; Chernov, K.; Giabra, M.; Levy, M.; Giboreau, A.; Kosak, S.; Mouhieddine, M.; et al. Improved Meal Presentation Increases Food Intake and Decreases Readmission Rate in Hospitalized Patients. Clin. Nutr. 2016, 35, 1153–1158. [Google Scholar] [CrossRef]
- Schiavone, S.; Pelullo, C.P.; Attena, F. Patient Evaluation of Food Waste in Three Hospitals in Southern Italy. Int. J. Environ. Res. Public Health 2019, 16, 4330. [Google Scholar] [CrossRef] [PubMed]
- Sonnino, R.; McWilliam, S. Food Waste, Catering Practices and Public Procurement: A Case Study of Hospital Food Systems in Wales. Food Policy. 2011, 36, 823–829. [Google Scholar] [CrossRef]
- Dias-Ferreira, C.; Santos, T.; Oliveira, V. Hospital Food Waste and Environmental and Economic Indicators—A Portuguese Case Study. Waste Manag. 2015, 46, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Freil, M.; Nielsen, M.A.; Biltz, C.; Gut, R.; Mikkelsen, B.E.; Almdal, T. Reorganization of a Hospital Catering System Increases Food Intake in Patients with Inadequate Intake. Scand. J. Food Nutr. 2006, 50, 83–88. [Google Scholar] [CrossRef][Green Version]
- Maunder, K.; Lazarus, C.; Walton, K.; Williams, P.; Ferguson, M.; Beck, E. Energy and Protein Intake Increases with an Electronic Bedside Spoken Meal Ordering System Compared to a Paper Menu in Hospital Patients. Clin. Nutr. ESPEN 2015, 10, e134–e139. [Google Scholar] [CrossRef]
- McCray, S.; Maunder, K.; Krikowa, R.; MacKenzie-Shalders, K. Room Service Improves Nutritional Intake and Increases Patient Satisfaction While Decreasing Food Waste and Cost. J. Acad. Nutr. Diet. 2018, 118, 284–293. [Google Scholar] [CrossRef]
- Williams, P.; Walton, K. Plate Waste in Hospitals and Strategies for Change. e-SPEN Eur. e-J. Clin. Nutr. Metab. 2011, 6, 235–241. [Google Scholar] [CrossRef]
- Green Healthcare EPA. Food Waste Reduction Programme Case Study St.Michael’s Hospital-Dun Laoighaire; Green Healthcare Programme; Green Healthcare EPA: Washington, DC, USA, 2013. [Google Scholar]
- Monteiro, D.M.S.; Brockbank, C.; Heron, G. Food Waste in Event Catering: A Case Study in Higher Education. J. Food Prod. Marke. 2020, 26, 262–278. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Meal | Item | Dish | Dish Characteristics |
|---|---|---|---|
| Breakfast | Drink | Milk | Only milk |
| Dessert | Pastry | Homemade pastry | |
| Complementary | Olive oil, jam and sugar | Individual packet | |
| Lunch | First course | Vegetables | Without sauce |
| Legumes | Without sauce | ||
| Main course | Fish | Cod, tuna. Without bones, fat, skin or sauce | |
| Chicken | Fried, roasted. Without bone, fat, skin or sauce | ||
| Red meat | Grilled, baked. Without fat or sauce | ||
| Side dish | Warm side dish | Vegetables (baked, grilled) or fried potatoes | |
| Dinner | First course | Soup | With pasta, vegetables or semolina |
| Purée | Vegetable purée | ||
| Main course | Egg | Omelette with vegetables or potato | |
| Fish | Salmon, hake. Without bones, fat, skin or sauce |
| Dish | Diet | n | SS Patient/Day (g) Mean (sd) | PW Patient/Day (g) Mean (sd) | PW Patient/Day (%) Mean (sd) | p Value 1 |
|---|---|---|---|---|---|---|
| Breakfast | ||||||
| Milk | BD and CM | 530 | 240.3 (9.2) | 71.0 (9.88) | 29.5 (4.1) | |
| Olive oil | BD | 355 | 10.0 (0.0) | 2.4 (0.5) | 24.3 (4.5) | |
| Jam | BD | 331 | 25.0 (0.0) | 3.4 (1.3) | 13.6 (5.1) | |
| Sugar | BD | 392 | 10.0 (0.0) | 2.3 (0.1) | 22.9 (1.2) | |
| Pastry | BD | 320 | 61.2 (2.9) | 7.9 (0.7) | 12.9 (1.3) | |
| Lunch | ||||||
| Vegetables | BD | 188 | 228.1 (38.2) | 33.6 (7.6) | 14.7 (1.7) | 0.49 |
| CM | 47 | 267.1 (7.0) | 49.1 (31.1) | 18.4 (11.5) | ||
| Legumes | BD | 195 | 266.4 (54.3) | 48.0 (17.4) | 17.7 (2.8) | nd |
| CM | 16 | 271.6 (18.7) | 44.3 2 | 16.3 2 | ||
| Fish | BD | 218 | 151.9 (27.7) | 42.7 (14.9) | 29.5 (14.6) | 0.11 |
| CM | 51 | 130.2 (33.0) | 14.6 (13.1) | 12.1 (13.4) | ||
| Chicken | BD | 199 | 166.7 (28.3) | 61.0 (41.9) | 35.7 (20.3) | nd |
| CM | 9 | 132.8 (10.9) | 64.9 2 | 63.1 2 | ||
| Read meat | BD | 203 | 102.3 (15.9) | 24.4 (17.8) | 24.0 (18.6) | 0.59 |
| CM | 62 | 113.4 (55.6) | 23.4 (21.7) | 19.4 (11.1) | ||
| Warm side dish | BD | 188 | 55.2 (23.6) | 13.8 (11.0) | 21.9 (11.5) | 0.90 |
| CM | 51 | 142.8 (42.9) | 20.6 (16.0) | 20.2 (24.8) | ||
| Dinner | ||||||
| Soup | BD | 214 | 258.3 (10.4) | 153.1 (16.7) | 20.5 (6.2) | 0.95 |
| CM | 85 | 235.7 (18.8) | 48.7 (21.0) | 20.8 (9.1) | ||
| Purée | BD | 313 | 229.5 (22.0) | 34.3 (9.2) | 14.9 (3.5) | 0.56 |
| CM | 37 | 230.7 (24.7) | 41.1 (23.8) | 18.0 (10.8) | ||
| Egg | BD | 295 | 148.5 (16.2) | 17.3 (9.8) | 11.5 (5.9) | 0.81 |
| CM | 62 | 170.2 (36.6) | 16.7 (12.2) | 10.5 (7.7) | ||
| Fish | BD | 211 | 144.9 (10.1) | 31.5 (7.3) | 22.1 (6.7) | 0.41 |
| CM | 69 | 111.7 (54.1) | 9.4 (12.4) | 13.5 (18.6) | ||
| Critical Dish | n | SS Patient/Day (g) Mean (sd) | PW Patient/Day (g) Mean (sd) | PW Patient/Day (%) Mean (sd) | p Value 1 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | Before | After | ||
| Milk | 530 | 446 | 240.3 | 205.6 | 71.0 (9.9) | 63.5 (21.4) | 29.5 (4.1) | 30.9 (10.4) | 0.81 |
| Chicken | 199 | 114 | 166.7 (28.3) | 228.9 (1.0) | 61.0 (41.9) | 16.4 (9.3) | 35.7 (20.3) | 7.2 (4.0) | 0.06 |
| Fish (lunch) | 218 | 135 | 151.9 (27.7) | 126.0 (27.5) | 42.7 (14.9) | 17.3 (11.0) | 29.5 (14.6) | 12.8 (7.4) | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paiva, L.; Hernández, C.; Santos, D.; Garayoa, R.; García, L.; Urdangarín, C.; Vitas, A.I. Hospital Plate Waste Assessment after Modifications in Specific Dishes of Flexible and Inflexible Food Ordering Systems. Sustainability 2022, 14, 15616. https://doi.org/10.3390/su142315616
Paiva L, Hernández C, Santos D, Garayoa R, García L, Urdangarín C, Vitas AI. Hospital Plate Waste Assessment after Modifications in Specific Dishes of Flexible and Inflexible Food Ordering Systems. Sustainability. 2022; 14(23):15616. https://doi.org/10.3390/su142315616
Chicago/Turabian StylePaiva, Lourdes, Carla Hernández, Diana Santos, Roncesvalles Garayoa, Laura García, Claudia Urdangarín, and Ana Isabel Vitas. 2022. "Hospital Plate Waste Assessment after Modifications in Specific Dishes of Flexible and Inflexible Food Ordering Systems" Sustainability 14, no. 23: 15616. https://doi.org/10.3390/su142315616
APA StylePaiva, L., Hernández, C., Santos, D., Garayoa, R., García, L., Urdangarín, C., & Vitas, A. I. (2022). Hospital Plate Waste Assessment after Modifications in Specific Dishes of Flexible and Inflexible Food Ordering Systems. Sustainability, 14(23), 15616. https://doi.org/10.3390/su142315616