

Digital Health in Schools: A Systematic Review

 ,
, 
 ,
,  ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Screening Strategy and Study Selection
2.4. Data Extraction and Harmonization
2.5. Study Quality and Risk of Bias
3. Results
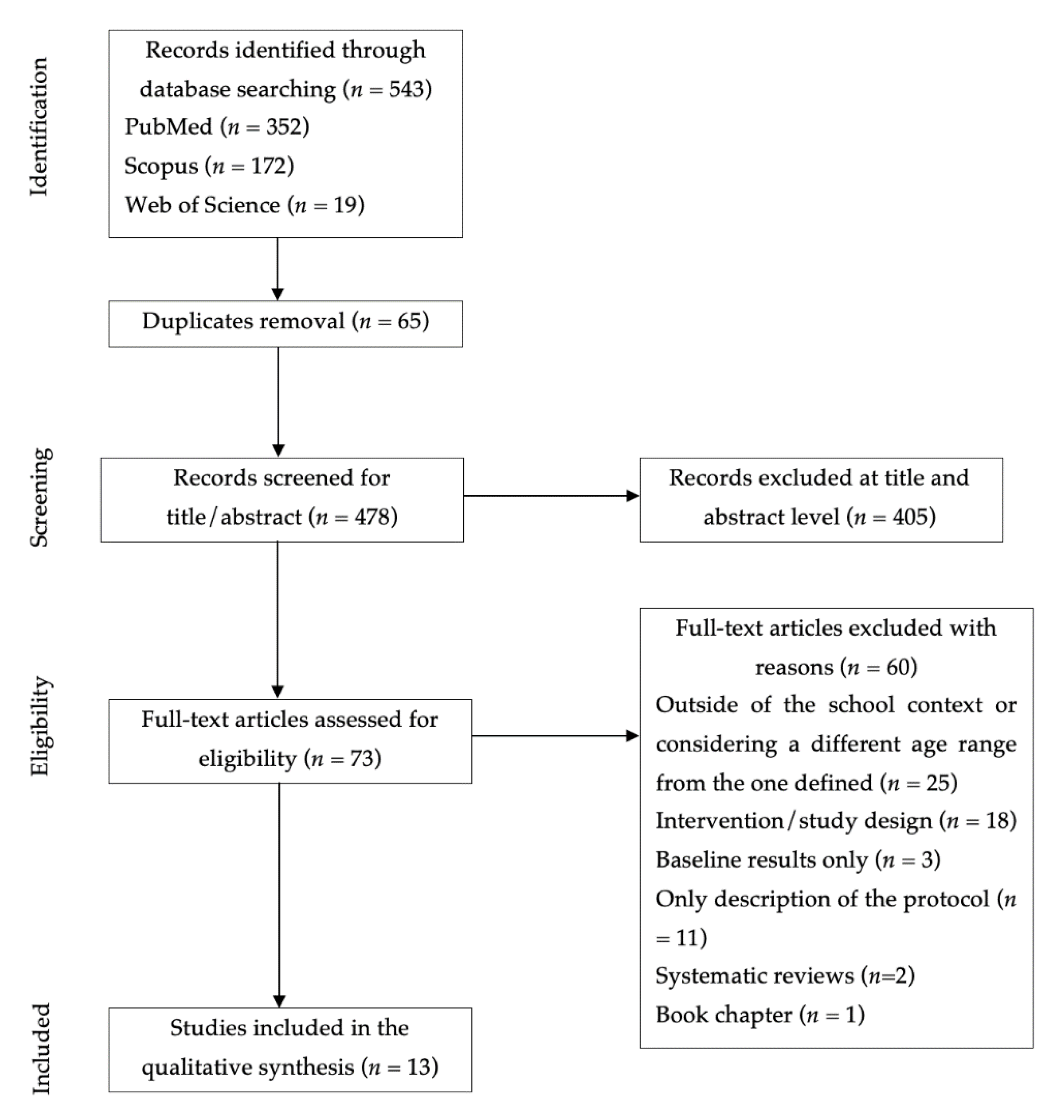
3.1. Study Selection
3.2. Study Quality and Risk of Bias
3.3. Intervention Characteristics
3.4. Main Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marcolino, M.S.; Oliveira, J.A.Q.; D’Agostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The impact of mHealth interventions: Systematic review of systematic reviews. JMIR MHealth UHealth 2018, 6, e8873. [Google Scholar] [CrossRef]
- Blandford, A.; Gibbs, J.; Newhouse, N.; Perski, O.; Singh, A.; Murray, E. Seven lessons for interdisciplinary research on interactive digital health interventions. Digit. Health 2018, 4, 2055207618770325. [Google Scholar] [CrossRef]
- Gurman, T.A.; Rubin, S.E.; Roess, A.A. Effectiveness of mHealth behavior change communication interventions in developing countries: A systematic review of the literature. J. Health Commun. 2012, 17, 82–104. [Google Scholar] [CrossRef] [PubMed]
- Nglazi, M.D.; Bekker, L.-G.; Wood, R.; Hussey, G.D.; Wiysonge, C.S. Mobile phone text messaging for promoting adherence to anti-tuberculosis treatment: A systematic review. BMC Infect. Dis. 2013, 13, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ali, E.E.; Chew, L.; Yap, K.Y.L. Evolution and current status of mhealth research: A systematic review. BMJ Innov. 2016, 2, 33–40. [Google Scholar] [CrossRef]
- Matthew-Maich, N.; Harris, L.; Ploeg, J.; Markle-Reid, M.; Valaitis, R.; Ibrahim, S.; Gafni, A.; Isaacs, S. Designing, implementing, and evaluating mobile health technologies for managing chronic conditions in older adults: A scoping review. JMIR MHealth UHealth 2016, 4, e5127. [Google Scholar] [CrossRef]
- Chiarini, G.; Ray, P.; Akter, S.; Masella, C.; Ganz, A. mHealth technologies for chronic diseases and elders: A systematic review. IEEE J. Sel. Areas Commun. 2013, 31, 6–18. [Google Scholar] [CrossRef]
- Bradway, M.; Carrion, C.; Vallespin, B.; Saadatfard, O.; Puigdomènech, E.; Espallargues, M.; Kotzeva, A. mHealth assessment: Conceptualization of a global framework. JMIR MHealth UHealth 2017, 5, e7291. [Google Scholar] [CrossRef]
- Stark, A.L.; Geukes, C.; Dockweiler, C. Digital Health Promotion and Prevention in Settings: Scoping Review. J. Med. Internet Res. 2022, 24, e21063. [Google Scholar] [CrossRef]
- Bendtsen, M.; Seiterö, A.; Bendtsen, P.; Henriksson, H.; Henriksson, P.; Thomas, K.; Löf, M.; Müssener, U. mHealth intervention for multiple lifestyle behaviour change among high school students in Sweden (LIFE4YOUth): Protocol for a randomised controlled trial. BMC Public Health 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Tryfona, C.; Oatley, G.; Calderon, A.; Thorne, S. M-Health solutions to support the national health service in the diagnosis and monitoring of autism spectrum disorders in young children. In Proceedings of the International Conference on Universal Access in Human-Computer Interaction, Toronto, Canada, 17–22 July 2016; pp. 249–256. [Google Scholar]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Paakkari, L.; Paakkari, O. Health literacy as a learning outcome in schools. Health Educ. 2012, 112, 133–152. [Google Scholar] [CrossRef]
- Peralta, L.; Rowling, L.; Samdal, O.; Hipkins, R.; Dudley, D. Conceptualising a new approach to adolescent health literacy. Health Educ. J. 2017, 76, 787–801. [Google Scholar] [CrossRef]
- Geller, R.J.; Rubin, I.L.; Nodvin, J.T.; Teague, W.G.; Frumkin, H. Safe and healthy school environments. Pediatr. Clin. N. Am. 2007, 54, 351–373. [Google Scholar] [CrossRef] [PubMed]
- Hagell, A.; Rigby, E.; Perrow, F. Promoting health literacy in secondary schools: A review. Br. J. Sch. Nurs. 2015, 10, 82–87. [Google Scholar] [CrossRef]
- Nash, R.; Patterson, K.; Flittner, A.; Elmer, S.; Osborne, R. School-Based Health Literacy Programs for Children (2–16 Years): An International Review. J. Sch. Health 2021, 91, 632–649. [Google Scholar] [CrossRef]
- Middelweerd, A.; Mollee, J.S.; van der Wal, C.N.; Brug, J.; Velde, S.J.T. Apps to promote physical activity among adults: A review and content analysis. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 1–9. [Google Scholar] [CrossRef]
- Conroy, D.E.; Yang, C.-H.; Maher, J.P. Behavior change techniques in top-ranked mobile apps for physical activity. Am. J. Prev. Med. 2014, 46, 649–652. [Google Scholar] [CrossRef]
- Lyons, E.J.; Lewis, Z.H.; Mayrsohn, B.G.; Rowland, J.L. Behavior change techniques implemented in electronic lifestyle activity monitors: A systematic content analysis. J. Med. Internet Res. 2014, 16, e3469. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. Quality Assessment Tool for Quantitative Studies Dictionary: The Effective Public Health Practice Project (EPHPP); McMaster University: Hamilton, Canada, 2008. [Google Scholar]
- Ahmed, T. Effect of mHealth tool on knowledge regarding reproductive health of school going adolescent girls: A before-after quasi-experimental study. BMJ Open 2020, 10, e036656. [Google Scholar] [CrossRef]
- Benítez-Andrades, J.A.; Arias, N.; García-Ordás, M.T.; Martínez-Martínez, M.; García-Rodríguez, I. Feasibility of Social-Network-Based eHealth Intervention on the Improvement of Healthy Habits among Children. Sensors 2020, 20, 1404. [Google Scholar] [CrossRef]
- Bethke, N.; Gellert, P.; Knoll, N.; Weber, N.; Seybold, J. A school-based educational on-site vaccination intervention for adolescents in an urban area in Germany: Feasibility and psychometric properties of instruments in a pilot study. BMC Public Health 2022, 22, 60. [Google Scholar] [CrossRef]
- Brown, J.M.; Savaglio, R.; Watson, G.; Kaplansky, A.; LeSage, A.; Hughes, J.; Kapralos, B.; Arcand, J. Optimizing child nutrition education with the foodbot factory mobile health app: Formative evaluation and analysis. JMIR Form. Res. 2020, 4, e15534. [Google Scholar] [CrossRef]
- Egilsson, E.; Bjarnason, R.; Njardvik, U. Usage and Weekly Attrition in a Smartphone-Based Health Behavior Intervention for Adolescents: Pilot Randomized Controlled Trial. JMIR Form. Res. 2021, 5, e21432. [Google Scholar] [CrossRef] [PubMed]
- Galy, O.; Yacef, K.; Caillaud, C. Improving Pacific Adolescents’ Physical Activity Toward International Recommendations: Exploratory Study of a Digital Education App Coupled With Activity Trackers. JMIR Mhealth Uhealth 2019, 7, e14854. [Google Scholar] [CrossRef] [PubMed]
- Guerra, A.M.; Montes, F.; Useche, A.F.; Jaramillo, A.M.; González, S.A.; Meisel, J.D.; Obando, C.; Cardozo, V.; Hunter, R.F.; Sarmiento, O.L. Effects of a Physical Activity Program Potentiated with ICTs on the Formation and Dissolution of Friendship Networks of Children in a Middle-Income Country. Int. J. Environ. Res. Public Health 2020, 17, 5796. [Google Scholar] [CrossRef]
- Hyman, A.; Stewart, K.; Jamin, A.M.; Lauscher, H.N.; Stacy, E.; Kasten, G.; Ho, K. Testing a school-based program to promote digital health literacy and healthy lifestyle behaviours in intermediate elementary students: The Learning for Life program. Prev. Med. Rep. 2020, 19, 101149. [Google Scholar] [CrossRef]
- Lee, J.E.; Song, S.; Ahn, J.S.; Kim, Y.; Lee, J.E. Use of a Mobile Application for Self-Monitoring Dietary Intake: Feasibility Test and an Intervention Study. Nutrients 2017, 9, 748. [Google Scholar] [CrossRef] [PubMed]
- Lyles, A.A.; Amresh, A.; Huberty, J.; Todd, M.; Lee, R.E. A Mobile, Avatar-Based App for Improving Body Perceptions Among Adolescents: A Pilot Test. JMIR Serious Games 2017, 5, e4. [Google Scholar] [CrossRef] [PubMed]
- Nuijten, R.C.Y.; Gorp, P.V.; Borghouts, T.; Blanc, P.L.; den Berg, P.V.; Kemperman, A.; Hadian, E.; Simons, M. Preadolescent Students’ Engagement With an mHealth Intervention Fostering Social Comparison for Health Behavior Change: Crossover Experimental Study. J. Med. Internet Res. 2021, 23, e21202. [Google Scholar] [CrossRef] [PubMed]
- Pope, L.; Garnett, B.; Dibble, M. Lessons Learned Through the Implementation of an eHealth Physical Activity Gaming Intervention with High School Youth. Games Health J. 2018, 7, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Sousa, P.; Martinho, R.; Reis, C.I.; Dias, S.S.; Gaspar, P.J.S.; Dixe, M.D.A.; Luis, L.S.; Ferreira, R. Controlled trial of an mHealth intervention to promote healthy behaviours in adolescence (TeenPower): Effectiveness analysis. J. Adv. Nurs. 2020, 76, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- Verjans-Janssen, S.R.; van de Kolk, I.; Kann, D.H.V.; Kremers, S.P.; Gerards, S.M. Effectiveness of school-based physical activity and nutrition interventions with direct parental involvement on children’s BMI and energy balance-related behaviors–A systematic review. PLoS ONE 2018, 13, e0204560. [Google Scholar] [CrossRef] [PubMed]
- Kerner, C.; Goodyear, V.A. The motivational impact of wearable healthy lifestyle technologies: A self-determination perspective on Fitbits with adolescents. Am. J. Health Educ. 2017, 48, 287–297. [Google Scholar] [CrossRef]
- la Haye, K.D.; Robins, G.; Mohr, P.; Wilson, C. Obesity-related behaviors in adolescent friendship networks. Soc. Netw. 2010, 32, 161–167. [Google Scholar] [CrossRef]
- Macdonald-Wallis, K.; Jago, R.; Page, A.S.; Brockman, R.; Thompson, J.L. School-based friendship networks and children’s physical activity: A spatial analytical approach. Soc. Sci. Med. 2011, 73, 6–12. [Google Scholar] [CrossRef]
- Garcia, J.M.; Agaronov, A.; Sirard, J.R.; Whaley, D.; Rice, D.J.; Weltman, A. Psychosocial and Friend Influences on Objective Sedentary Behavior and Screen Time: A Mixed Methods Analysis. J. Phys. Act. Health 2017, 14, 213–221. [Google Scholar] [CrossRef]
- Draper, C.; Grobler, L.; Micklesfield, L.; Norris, S. Impact of social norms and social support on diet, physical activity and sedentary behaviour of adolescents: A scoping review. Child. Care Health Dev. 2015, 41, 654–667. [Google Scholar] [CrossRef]
- Fitzgerald, A.; Fitzgerald, N.; Aherne, C. Do peers matter? A review of peer and/or friends’ influence on physical activity among American adolescents. J. Adolesc. 2012, 35, 941–958. [Google Scholar] [CrossRef]
- Vu, T.; Lin, F.; Alshurafa, N.; Xu, W. Wearable food intake monitoring technologies: A comprehensive review. Computers 2017, 6, 4. [Google Scholar] [CrossRef]
- Khamzina, M.; Parab, K.V.; An, R.; Bullard, T.; Grigsby-Toussaint, D.S. Impact of Pokémon Go on physical activity: A systematic review and meta-analysis. Am. J. Prev. Med. 2020, 58, 270–282. [Google Scholar] [CrossRef] [PubMed]
- Sardi, L.; Idri, A.; Fernández-Alemán, J.L. A systematic review of gamification in e-Health. J. Biomed. Inform. 2017, 71, 31–48. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Key Search Terms | Related Search Terms |
|---|---|
| Children and Adolescents | Children OR Adolescent OR youth |
| Infectious Disease | COVID-19 OR Infectious OR Disease * |
| Intervention | Intervention * OR Program * OR Protocol * OR RCT OR “Randomized controlled trial” OR “Experimental” |
| mHealth | mHealth OR “Mobile health” OR eHealth |
| School | School |
| Authors | Selection Bias | Design | Confounders | Blinding | Data Collection Methods | Withdrawals and Dropouts | Overall |
|---|---|---|---|---|---|---|---|
| [23] | Strong | Moderate | NA | Weak | Strong | Strong | Moderate |
| [24] | Weak | Moderate | Strong | Weak | Strong | Strong | Weak |
| [25] | Moderate | Moderate | Strong | Weak | Strong | Strong | Moderate |
| [26] | Weak | Moderate | NA | Weak | Strong | Strong | Weak |
| [27] | Moderate | Strong | Strong | Strong | Strong | Weak | Moderate |
| [28] | Weak | Moderate | NA | Weak | Strong | Strong | Weak |
| [29] | Moderate | Strong | Strong | Weak | Strong | Moderate | Moderate |
| [30] | Moderate | Moderate | Strong | Weak | Strong | Strong | Moderate |
| [31] | Weak | Moderate | NA | Weak | Strong | Strong | Weak |
| [32] | Weak | Moderate | NA | Weak | Strong | NA | Weak |
| [33] | Weak | Strong | Strong | Weak | Strong | Weak | Weak |
| [34] | Moderate | Strong | Weak | Weak | Strong | Weak | Weak |
| [35] | Moderate | Strong | Strong | Weak | Strong | Weak | Weak |
| Author (Year) | Sample | Purpose | Health Area | Intervention | Instruments and Measures | Main Results |
|---|---|---|---|---|---|---|
| [23] | 400 female students aged between 14 and 19 years | To examine the effect of the mHealth tool on knowledge regarding reproductive health, and to determine the use of the mHealth tool among schoolgirls. | Reproductive health | Short message service (SMS) delivered through a mobile phone for 8 weeks. Each user received three SMS every week. The first one contained a multiple-choice quiz question on reproductive health. The users answered the quiz by replying to the SMS. Then, two SMS with the correct answer and additional information on the quiz topic were sent sequentially. | Reproductive health knowledge (mobile health tool, SMS). | Post-intervention knowledge scores on reproductive health were significantly higher compared to baseline scores. The SMS approach was an easy and effective way to improve reproductive health knowledge for adolescent girls. |
| [24] | 230 students aged between 11 and 15 years (IG = 139; CG = 91) | To assess the feasibility of an eHealth solution to address eating habits and PA in adolescents. | Physical activity and nutrition | Use of an eHealth application (“SanoyFeliz”) for 14 weeks. Through the platform, students could connect and interact with other users, post comments and photos, receive notifications and information about nutrition and PA daily, and get virtual rewards for improving their habits. | Eating habits and PA were assessed through the KIDMED (nutrition) and PAQ-A questionnaires. Body measurements (body mass and height) were used to obtain the children’s BMI. | A significant statistical decrease in the BMI was observed in the IG for individuals with an initial percentile greater than 50%. KIDMED scores were significantly better in the IG after 14 weeks compared with the CG. However, PA levels have slightly decreased after the intervention, particularly in the CG. |
| [25] | 863 students aged between 14 and 17 years | To improve vaccination rates and knowledge and self-efficacy in a school context. | Vaccination | For 1 week, educational units (about 45 m) were taught by a physician in the classrooms. Information was distributed using a PowerPoint presentation with interactive elements, and social media elements such as newspaper articles and videos were included. All four participating schools received a visit from the Prevention Bus, which contained a medical team, two physicians, two nurses, and a bus driver. | Seven indicators and measures were assessed: school recruitment log, vaccination documents, vaccinations delivered, rating of the educational unit, semistructured interviews on the education unit, vaccination-related knowledge scale, and vaccination-related perceived self-efficacy scale. | From the whole sample, 437 students (50.9%) brought their vaccination cards to a school, and 79 received vaccinations. Students improved their scores in six of the knowledge questions in the post-intervention. The teaching methods (interactive and social media components) were perceived as very good by the participants. |
| [26] | 102 students (39 females and 63 males) aged 9 and 12 years | To describe the development and user testing of a nutrition education gamified app designed for children. | Nutrition | Testing a gamified mHealth app (“Foodbot Factory”) designed to improve food and nutrition knowledge among children. Five interactive user testing sessions were conducted for approximately 20 to 30 min using an Apple iPad (iOS 12) or a Lenovo tablet (Android 8.1.0). | Qualitative interviews and questionnaires to assess users’ satisfaction, engagement, usability, and knowledge gained. | In the final user test, most users still found the app was fun, had clear goals, and was easy to use (71–94%). A total of 71% of students have shown interest in still using the Footbot Factory after the intervention. |
| [27] | 41 students aged 15.6 ± 0.25 years (IG = 20; CG = 21) | To describe the usage and feasibility of an mHealth intervention concerning self-efficacy levels, and emotional and physical health. | Physical activity, nutrition, and mental health | The IG had access to the app for 6 weeks, and measurements were compared between this time point and the baseline. Multiple focus group studies were performed among adolescents and advisors for app development. Based on the results, the app was built as a social health game. Through gamification, the app functionality aims to help users set goals and develop health-related missions in three main categories: nutrition, PA, and mental health. | The app’s acceptability and functionality were assessed with the Systematic Usability Scale. Further, the amount, frequency, ad time of daily PA was measured through in-app activity. The stress levels, quality of sleep, and energy levels were evaluated by completing in-app health tasks. The anthropometric assessment included height and weight. | The reported daily PA increased by nearly 20% in the IG, dropping by almost 26% in the CG. Self-efficacy levels increased by 8% in the IG and decreased by 3% among the CG. |
| [28] | 24 students aged between 12 and 14 years | To investigate whether a technology-based educational program that combines education, PA, and self-assessment of goal achievement, would contribute to changing PA behaviors toward the international PA recommendations. | Physical activity and nutrition | The iEngage educational program was implemented through an app for 4 weeks. The app targeted health literacy, PA-related skills, and sugar-focused nutrition guidelines. Learning activities, goal setting, self-assessment tasks, and brief 2- to 5-min PA sessions (focused on particular movements such as sprints, squats, jumping, etc.) were developed in two modules of 1 h per week. | Anthropometric and physical fitness data (aerobic capacity, speed, and agility) were assessed three weeks before the program. The baseline PA behavior was measured using research-grade activity sensors (GENEActiv) five consecutive days before the program. PA during the program was measured using Misfit activity trackers. | On average, participants achieved 11197 ± 1376 steps per day during the 4-week intervention. PA showed an overall increase, particularly in the less active individuals (an increase of nearly 15% in the daily steps). The satisfaction with the modules was 95% across the program |
| [29] | 125 students aged between 9 and 13 years (IG1: MARA = 2 classes; IG2: MARA + SMS = 2 classes; CG: 3 classes) | Assess the potential cohesion effect of a PA school-based intervention by analyzing longitudinally the friendship network structure and the mechanisms of friendship formation/dissolution. | Physical activity and social interaction | The interventions were implemented for 10 weeks. The IG1 (MARA group) was intervened three times per week during the school recess of 30 min. In total, 30 sessions of PA combined with supervised games with ties, balls, hoops, stairs, and dancing were carried out. The IG2 (MARA + SMS group), in addition to the intervention made in IG1, was also targeted with SMS each weekday. The SMS was focused on promoting the students’ participation, engagement, motivation, and empowerment, in extracurricular PA and healthy behaviors among their classmates and family members. The CG did not receive any intervention. | Socioeconomic status was assessed using the demographic and family health questionnaire. The health-related assessment included anthropometry (body mass and height) and accelerometry (GT3X+ accelerometer) to provide BMI. The network structure and cohesion information were collected using an interview. Users’ satisfaction levels were evaluated using the PA class satisfaction questionnaire). | The intervention influenced the mechanisms of friendship formation and dissolution. On average, the MARA + SMS group showed more social cohesion and 3.8 more friendships than the program alone. PA levels and BMI began to affect friendship homophily and the formation/dissolution of friendships in the intervened networks over time. Children became more likely to stop being friends with their peers with different BMIs (network 1 of MARA + SMS). Besides, children became less likely to become friends with their peers with varying levels of PA (network 2 of MARA + SMS and network 3 of MARA) |
| [30] | 126 students aged between 9 and 13 years | To test the effectiveness of an intervention to increase students’ digital health literacy and health knowledge. | Health literacy, physical activity, nutrition, and social interaction | Teachers delivered a classroom-based education program (Learning for Life) over 6 weeks in three schools. Teachers were provided with an educator’s toolkit, student workbook, and online interactive graphics for students focused on health literacy PA, sedentary behavior, and social connectedness. | Technology usage was assessed by self-reported past and current internet usage and which devices they use. Digital health literacy was evaluated using the eHealth Literacy Scale. The interview collected PA levels and sedentary behavior, including the amount of time spent doing sedentary activities. Health knowledge and behavior change included a 10-item questionnaire. | From pre- to post-intervention, students’ digital health literacy improved. However, there was a significant decrease in digital health literacy from post-intervention to follow-up (2 months after the intervention). In the post-intervention assessment, most students could identify at least one healthy behavior (e.g., exercising one hour per day) and reported making at least one healthy change in their lives (e.g., eating more fruits or vegetables). |
| [31] | 33 students aged between 16 and 18 years (24 females and 9 males) | Test the feasibility of a mobile application and examine whether it could be used to monitor dietary intake among adolescents. | Nutrition | Three-month intervention study. Participants answered pre- and post-intervention dietary habit questionnaires. Participants were asked to record all foods and beverages consumed using voice or text input. Nutrient intake was measured using 24 h recalls pre- pre-and-intervention. | Monitor Dietary intake (Moblie App, “Diet-A”). | There was a significant decrease in sodium and calcium intake between pre-and post-intervention. Nearly 61.9% of the participants reported being satisfied with the app’s usage to monitor their food intake, and 47.7% liked getting personal information about their dietary intake. However, more than 70% answered that using the app was burdensome or had trouble remembering to record their food intake. |
| [32] | 42 students aged between 15 and 18 years | Develop and assess the acceptability of an avatar-based mobile app (Monitor Your Avatar, MYA). | Self-perception | Cross-sectional study. First, the research team measured height, weight, body fat percentage, and adolescents’ body parts. Then, it was divided into three phases: (i) Perceived Avatar—adolescents designed the avatar to represent how they currently perceive their bodies to look; (ii) Target Avatar—adolescents take the first avatar and transform it as they want their bodies to look within realistic, healthy parameters; (iii) Actual Avatar—adolescents enter their body part measurements into the app and generate an actual avatar of themselves. | Interactive and designed mobile health app (MYA). Open-ended reaction questions to assess participants’ acceptability to MYA. | Avatar-based mobile apps provide immediate feedback and allow users to engage with personalized images to represent their perceptions and actual body images. The participants reacted positively to the avatar app and could view avatars that represented them. |
| [33] | 313 participants (290 students aged between 11 and 13 years, and 23 teachers) | Evaluate how social comparison drives preadolescents’ engagement with an mHealth app. | Physical activity, nutrition, and social interaction | Students and teachers used an mHealth tool (“GameBus”) for 12 weeks that rewarded healthy activities. Three different social comparative settings as treatments, test whether an intergroup competition would be more effective in promoting healthy habits. A crossover study design was adopted to ensure that all the participants were exposed twice to every treatment. Each treatment simulated a different implementation of the social comparison technique: (i) intragroup competition, (ii) intergroup competition, and (iii) intergroup competition, increasing teachers as potential role models for students. | Use an mHealth tool for health promotion (mobile app, “GameBus”). Post-intervention survey (individual factor proposed by the social comparison model of competition; students’ perception of closeness to their peers, similarity to their teachers and/or peers, the relevance of the prescribed activities, and personality). | An intergroup competition can increase preadolescents’ passive engagement with mHealth apps. However, an intergroup competition does not necessarily result in preadolescents performing more unique activities on average. The active involvement of a role model (e.g., a teacher) can influence the average number of activities performed by preadolescents in an intergroup setting. |
| [34] | 105 students aged between 16 and 18 years (IG = N/S; CG = N/S) | Encourage high school students to meet PA goals using a newly developed game. | Physical activity | Twelve-week pilot test. Students were randomly assigned to a Game Condition or Control Condition. The difference was that the Game Condition received access to the Camp Conquer game, and the number of steps and active minutes was translated into coins and gems. | The number of steps and the amount of time spent in activity per day were collected using the Fitbit devices. Additional data included the number of logins into the gaming platform and a baseline questionnaire focused on PA, sleep, gaming, and dietary patterns. | The intervention was not successful in increasing PA in high school students. Nearly 50% of the participants did not consistently wear their FitBit or engage in the gaming intervention. Logistical factors, such as needing to charge the FitBit and take it off for sports/sleep, and game glitches, were some of the reasons. |
| [35] | 353 students aged between 12 and 16 years (IG = 140; CG = 213). | Evaluate the effectiveness of lifestyle change of an mHealth intervention to promote healthy behaviors in adolescence (TeenPower). | Health literacy | For 6 months, the IG was invited to engage in the mHealth intervention (TeenPower) in addition to school-based intervention. The CG followed the school-based intervention (face-to-face psycho-educative sessions with nutritional, behavioral, and PA counseling). The IG was access to the TeenPower mobile software application: created for adolescents to provide them with educational resources, social support, self-monitoring features, interactive training modules, and motivational tools. | A questionnaire assessed the Adolescent Lifestyle Profile, which included information on health responsibility, PA level, nutrition, positive life perspective, interpersonal relationship, stress management, and spiritual health. Body image dissatisfaction. The eHealth literacy was evaluated using the eHealth Literacy Scale tool. The Body Image perception was measured using a sequence of seven silhouettes and the presently estimated body dissatisfaction minus the desired body shape. | The post-intervention assessment dropped significantly (IG = 53 and CG = 151 students). Although the considerable dropout rate, mHealth intervention (TeenPower) significantly affects nutrition, positive life perspective, and global lifestyle outcomes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
França, C.; Santos, F.; Martins, F.; Lopes, H.; Gouveia, B.; Gonçalves, F.; Campos, P.; Marques, A.; Ihle, A.; Gonçalves, T.; et al. Digital Health in Schools: A Systematic Review. Sustainability 2022, 14, 13848. https://doi.org/10.3390/su142113848
França C, Santos F, Martins F, Lopes H, Gouveia B, Gonçalves F, Campos P, Marques A, Ihle A, Gonçalves T, et al. Digital Health in Schools: A Systematic Review. Sustainability. 2022; 14(21):13848. https://doi.org/10.3390/su142113848
Chicago/Turabian StyleFrança, Cíntia, Francisco Santos, Francisco Martins, Helder Lopes, Bruna Gouveia, Frederica Gonçalves, Pedro Campos, Adilson Marques, Andreas Ihle, Tatiana Gonçalves, and et al. 2022. "Digital Health in Schools: A Systematic Review" Sustainability 14, no. 21: 13848. https://doi.org/10.3390/su142113848
APA StyleFrança, C., Santos, F., Martins, F., Lopes, H., Gouveia, B., Gonçalves, F., Campos, P., Marques, A., Ihle, A., Gonçalves, T., & Gouveia, É. R. (2022). Digital Health in Schools: A Systematic Review. Sustainability, 14(21), 13848. https://doi.org/10.3390/su142113848