1. Introduction
One significant effect of climate change is its adverse impact on human health and performance [
1]. Various scientific reports provide substantial evidence relating climate change-driven temperature variations to heat and cold-related mortalities and morbidities [
2,
3,
4]. Some recent efforts to quantify the effect of extreme temperature variations have reported increases in global temperature-related death ranging between 3% and 12.7% under future projections of greenhouse gas emissions [
5]. Such effects of temperature on human health are often double-sided—extremely low temperatures promote hypothermic reactions. In contrast, extremely high temperatures induce hyperthermic reactions, which are detrimental to well-being, although the projections are seemingly more severe for warmer and poorer localities. Consequently, determining temperature balances that promote bodily homeostasis is crucial to achieving sustainable livelihoods, especially amid the changing climate.
The occurrence of heatwaves (HWs), defined as episodes of prolonged high temperatures and which are partly driven by the changing climate, also contribute significantly to heat-related mortalities and morbidities [
6]. Empirical evidence demonstrating correlations between HWs, and heat-related mortality has been reported in many parts of Europe [
7,
8], the United States [
9], Russia [
10], and Korea [
11]. The impact of HWs on heat-related mortalities is even more worrisome, given a vast number of scientific studies that forecast an increase in the frequency, duration, and severity of HWs in the near future.
Vulnerability to temperature-related mortalities and morbidities is more heightened in urban areas than rural areas. However, this tends to arise from extreme heat conditions than cold heat conditions and is mainly attributed to urban heat islands (UHI). UHIs refer to the often higher surface and atmospheric temperatures in urban environments than their rural, more natural surroundings [
12]. UHIs arise from complex interactions between the urban form, which is primarily modified by urbanization, and urban climates that are substantially influenced by intense anthropogenic activities—such complex interactions significantly modify the urban thermal structure, intensifying extreme heat-related incidences in urban areas [
13,
14]. Various scientific studies have demonstrated the effects of UHI on heat-related mortality in many agglomerations. For instance, the extent of UHI impacts on heat-related mortality was reported at 1.1 deaths per million people in American cities [
15]. The effect of UHI on heat-related mortalities has also been demonstrated in Athens [
16], London [
17], and Shanghai [
18]. A more recent study conducted in multiple cities in China has shown that compound heat events are more pronounced in urban areas than their rural counterparts and such observations are potentially fueled by UHI formation [
19]. Such influences of UHI on the well-being of urban populations are forecasted to worsen, considering the increasing rate of urbanization resulting in higher UHI intensities (UHII).
UHI and HWs have also been reported to interact synergistically, substantially amplifying heat-related mortalities. For instance, Founda and Santamouris reported higher UHII, reaching up to 3.5 °C, during HW periods than during normal summer conditions in Athens [
20]. Such heightened UHII during HWs have also been reported in Sydney [
21], Seoul [
22] and multiple cities in China [
23]. While the magnitude of the interdependencies between UHI and HWs is likely to differ from locality to locality given the peculiarity of each location (e.g., space form and configuration, land characteristics, etc.), the consensus in the literature points to the synergistic interactions between the two phenomena and their heightened influence on mortalities and morbidities in urban areas. This is worrisome amid increasing evidence projecting increased UHII and more frequent HWs in the near future [
24].
The effects of climate change, HWs, and UHI on heat-related deaths discussed above are not equally distributed across all populations. Some populations are more affected than others, and this primarily arises from the differences in personal factors, social-economic factors, or a complex combination of the two elements. Epidemiological studies have shown that the physiological and psychological toll of extreme temperatures is higher in specific subgroups than the others [
25]. For instance, the effects of high temperatures differ among age groups; temperature-related mortalities and morbidities are amplified at the extreme ends of the age curve [
26]. Gender (used here and throughout the manuscript to refer to the biological differences between individuals of different sexes) has also been reported to modulate the effects of temperature on health and performance—the different responses to temperature changes between genders and age groups have been attributed to the inherent differences in physiology between genders or age groups [
27,
28].
Variations in how certain groups respond to temperature changes have also been attributed to occupational differences. Outdoor workers and occupations involving intense physical activities (e.g., athletes, soldiers) are more prone to temperature-related heat strokes primarily due to large amounts of metabolic heat production and heat gain intrinsic to the nature of certain occupations [
29]. Energy poverty is also an issue that is increasingly having a substantial influence on the resilience of certain groups during extreme temperatures [
30]. Vulnerability to heat-related health issues is highest for populations with less/insufficient access to energy resources or relevant equipment (e.g., heating ventilation and air conditioning systems).
Assessing the effect of local climatic changes on human health and performance is a challenging issue, particularly given the vast range of factors likely to modulate the said effect (i.e., UHI, HWs, personal factors, and social-economic factors) but one of urgency especially considering the changing climate. While the fundamental effects of temperature changes on heat-related mortality are properly understood in the literature, quantification of such effects is likely to vary from locality to locality, mainly due to acclimatization. Heat-related mortalities have been reported to increase substantially when temperatures deviate from the local mean [
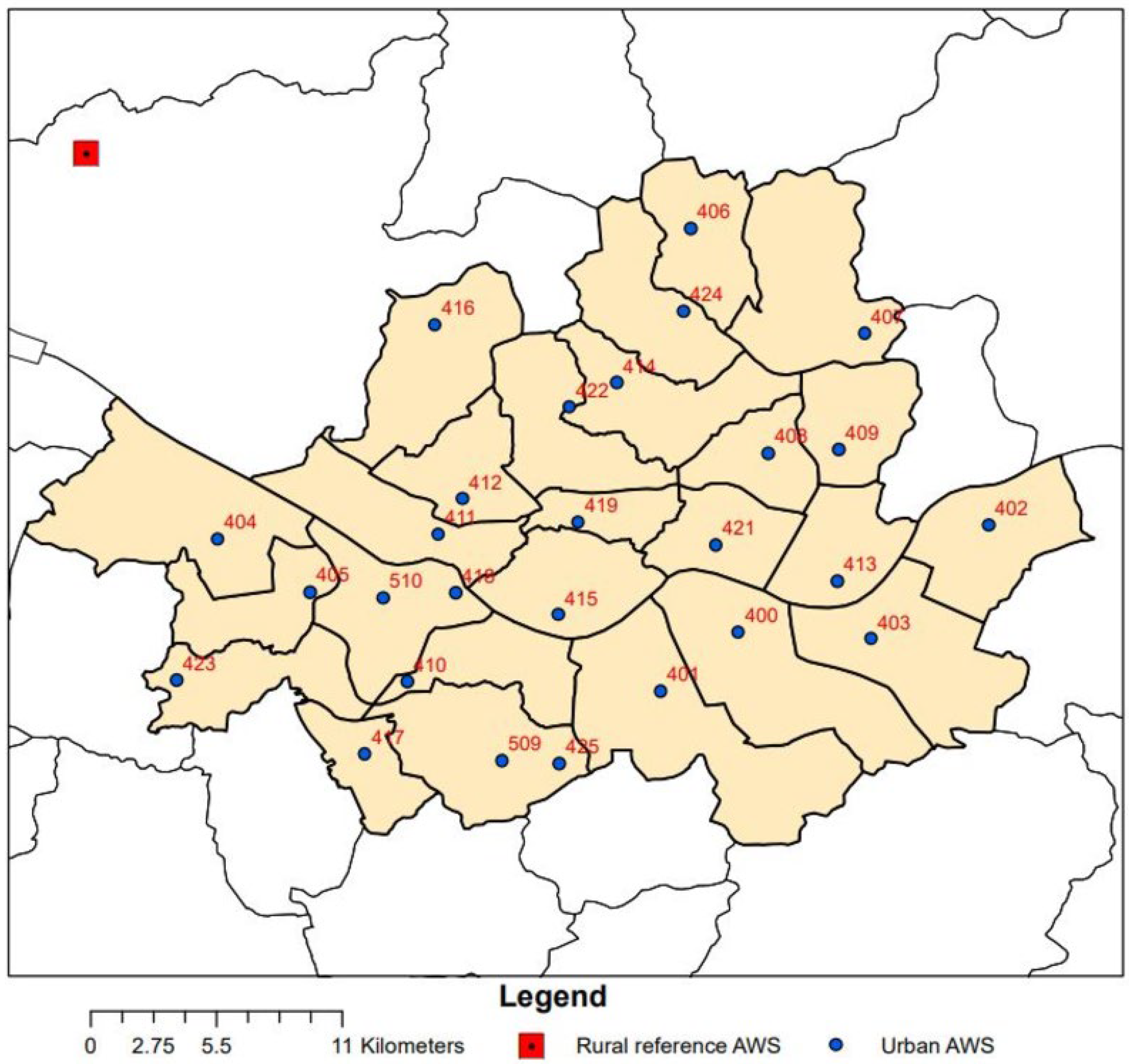
31]. Local mean temperatures vary considerably even across conurbations of similar sizes. To that end, the present study aims to explore variations in heat-related daily mortality counts in Seoul city, a densely populated and highly urbanized conurbation, considering local climatic conditions and personal and social-economic factors. The results shed more light on heat exposure-related vulnerability in Seoul city and form a basis for effective policies to combat heath issues stemming from changes in local climatic conditions.
4. Discussion
Climate change, often from the perspective of long-term temporal temperature variability, has been at the forefront of human-centric issues in the 21st century. Epidemiological research, through various methodologies, has shown that extreme temperatures can have diverse physiological strains on a human body, leading to many health issues. For instance, Bobb et al. [
56] reported that risks of hospitalization for fluid and electrolyte disorders, renal failure, and urinary tract infection increase under extreme heat events. Similar epidemiological research [
57,
58,
59] has reported the significance of extreme heat vents on people’s physiological well-being, which could eventually lead to fatal outcomes.
The health vulnerabilities imposed by increasing temperatures are a much more severe concern in urban agglomerations as they often experience escalated thermal conditions, mainly resulting from local climate change [
25]. While the impacts of temperature changes concern the majority population, the sensitivity and adaptive capacity to said temperature changes vary from demographic to demographic. Such variations are primarily a consequence of a complex combination of personal and social-economic elements. Consequently, it is essential to identify groups most vulnerable to heat exposure and subsequently deliver targeted mitigation and adaptive strategies. Moreover, the compounding effects of local/regional climate change vary from locality to locality and are driven mainly by geographical and social-political-economic elements endemic to said localities. Analyses dealing with the impact of regional and global climate change should thus be area-specific to enable locally tailored interventions and planning. To that end, the main objective of the current study was to quantitively evaluate the associations between temperature and respiratory and cardiovascular mortalities in Seoul while simultaneously analyzing how the said associations differ across different demographics characterized by (i) personal factors (i.e., age and gender), (ii) social-economic factors (i.e., education level), and (ii) local climatic episodes (i.e., UHI and HWs).
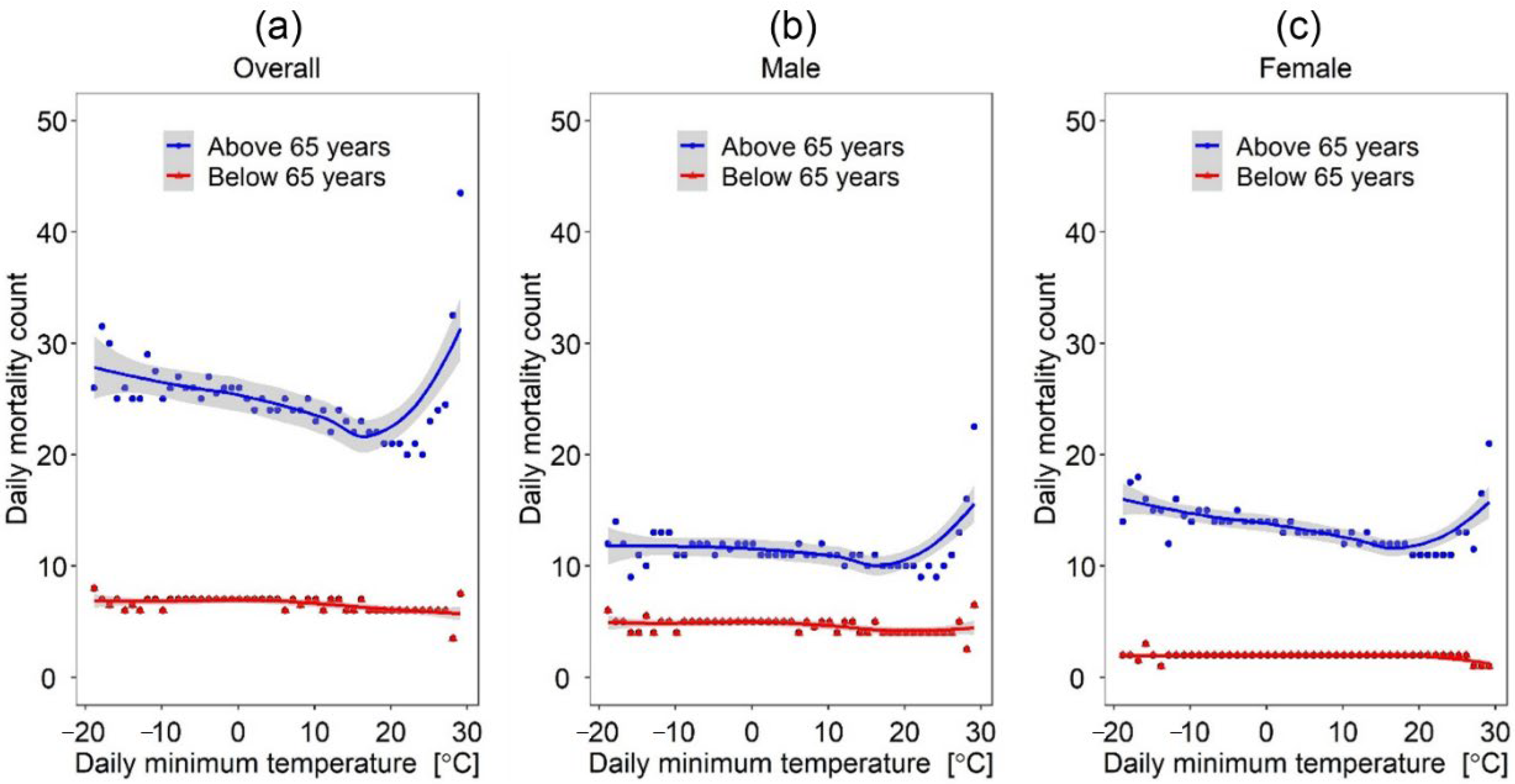
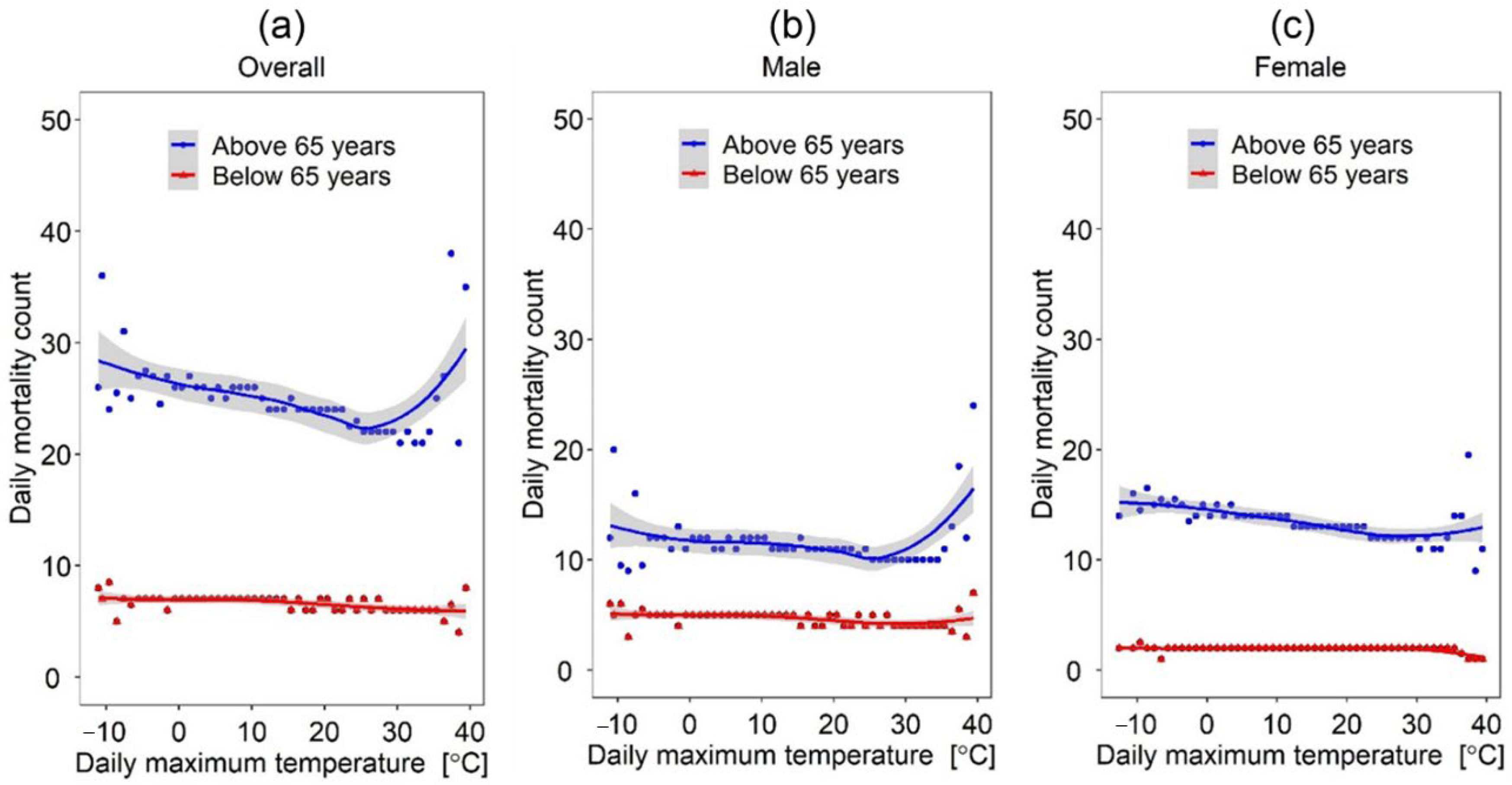
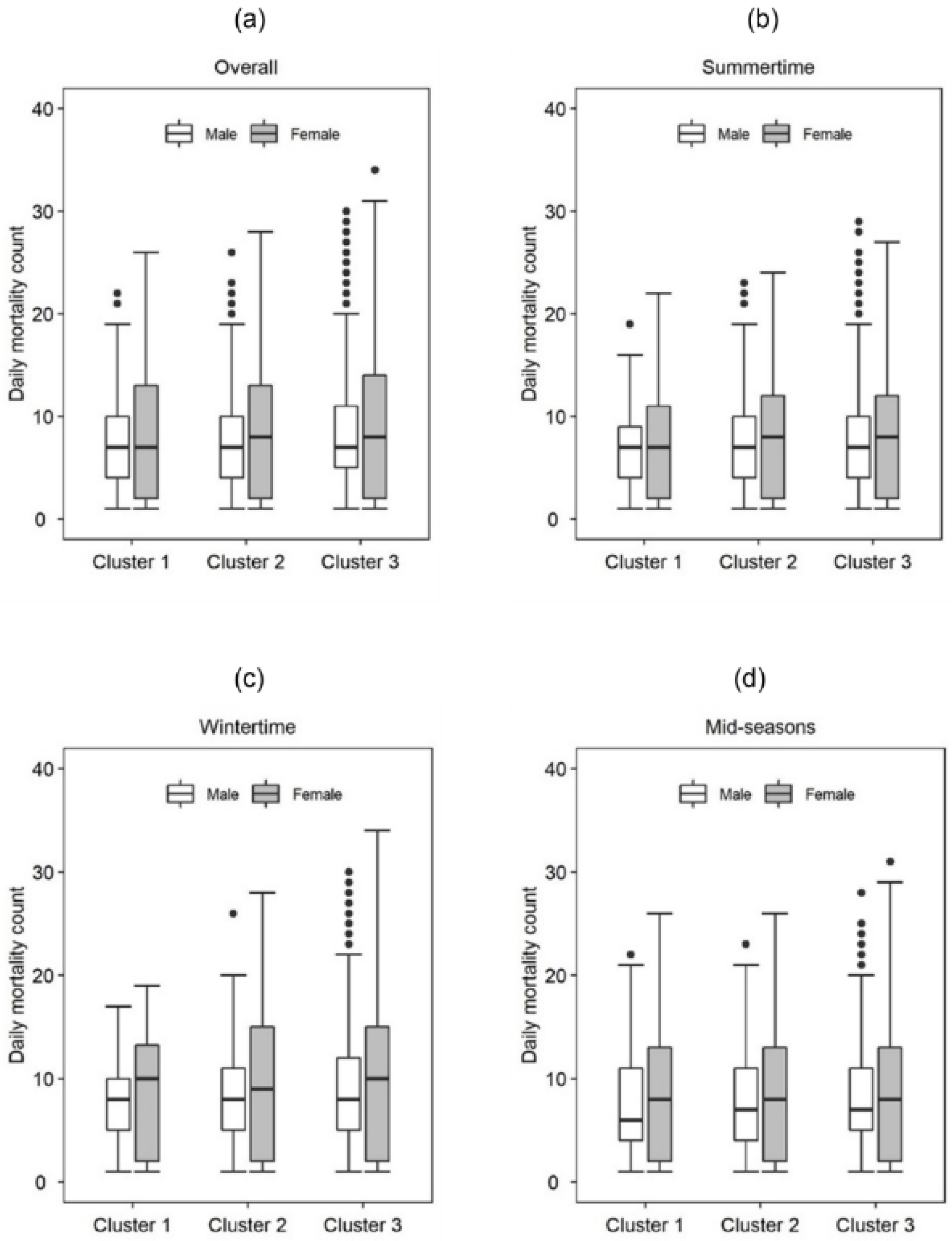
Our results showed that the effect of temperature variants (e.g., minimum daily temperature, average daily temperature, and maximum daily temperature) differ significantly across different age groups (i.e., above 65 years and below 65 years of age) and between males and females. For instance, given the same daily maximum temperature, the number of mortalities was significantly higher for females above 65 years of age than their male counterparts (see
Figure 6). The finding reports that older females are more vulnerable to health issues resulting from elevated temperatures and reiterates reports from studies in South Korea [
60], Spain [
61], England [
62] as well as cities in China [
63]. Such differences in sensitivities to heat exposure between genders are, to an extent, attributed to differences in physiological characteristics inherent of the two genders (e.g., in terms of temperature regulatory mechanisms [
64,
65]. Another possible explanation for such a result pertains to social demographic characteristics that encourage gender differences in elements such as life expectancy and social isolation [
61,
66]. On the contrary, a study conducted in the Tibetan counties in China reported males to be more susceptible to extreme temperature exposure than females [
67]. Similarly, a recent study conducted in multiple cities in China found that males were more affected by high-frequency temperature variations than females [
68] while another study in Taiwan found no differences in susceptibility between the two genders [
69]. Such observations seem to emphasize regional differences in temperature-mortality effects and perhaps warrants more intense discussions on the role of regional climatic conditions on temperature-mortality relationships.
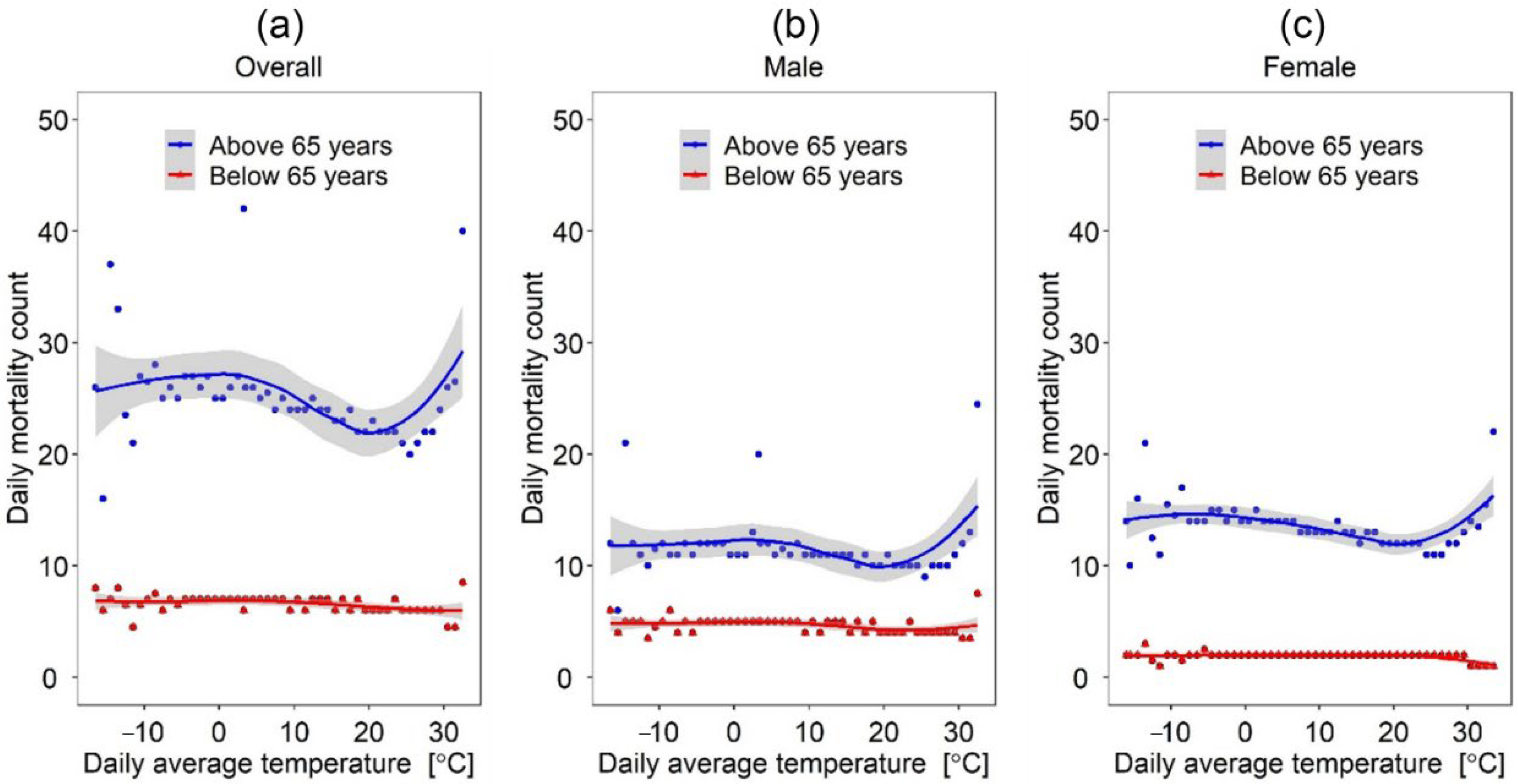
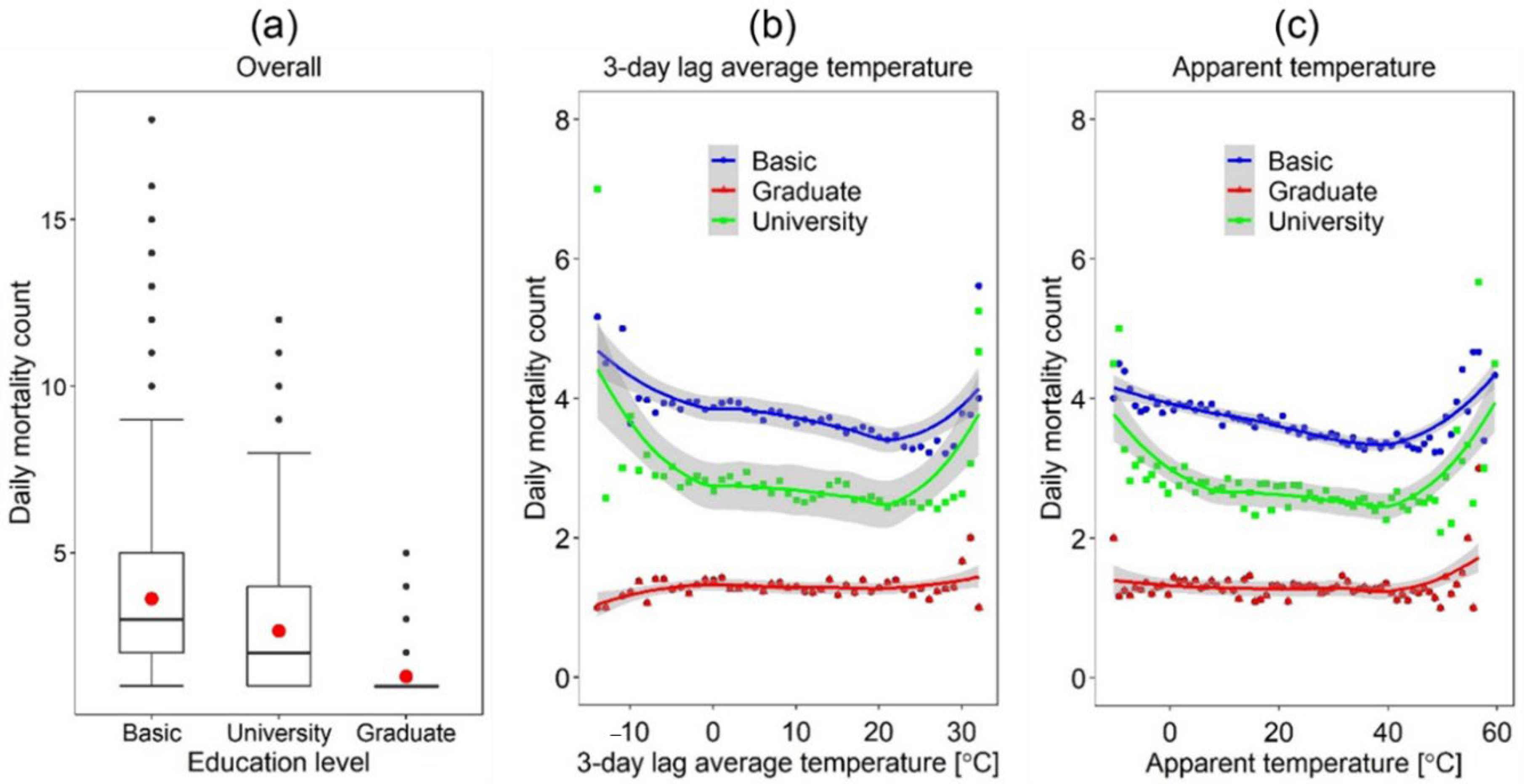
One interesting finding with vast implications for urban planning policies is the inflection temperature point upon which daily mortalities increase between the two genders. This is better observed considering the daily average temperature (see
Figure 5)—the inflection temperature point for males was observed at 20 °C while that for females was 21.5 °C. The finding suggests that the population in Seoul is acclimatized to low temperatures and that this is more the case for males than females. This can also be viewed from the perspective of physiological differences between the two sexes; men have been reported to have larger decreases in core body temperature than women when exposed to cold temperatures [
70], and possibly the reason for the observed lower inflection temperature point in males than females (i.e., 20 °C vs. 21.5 °C).
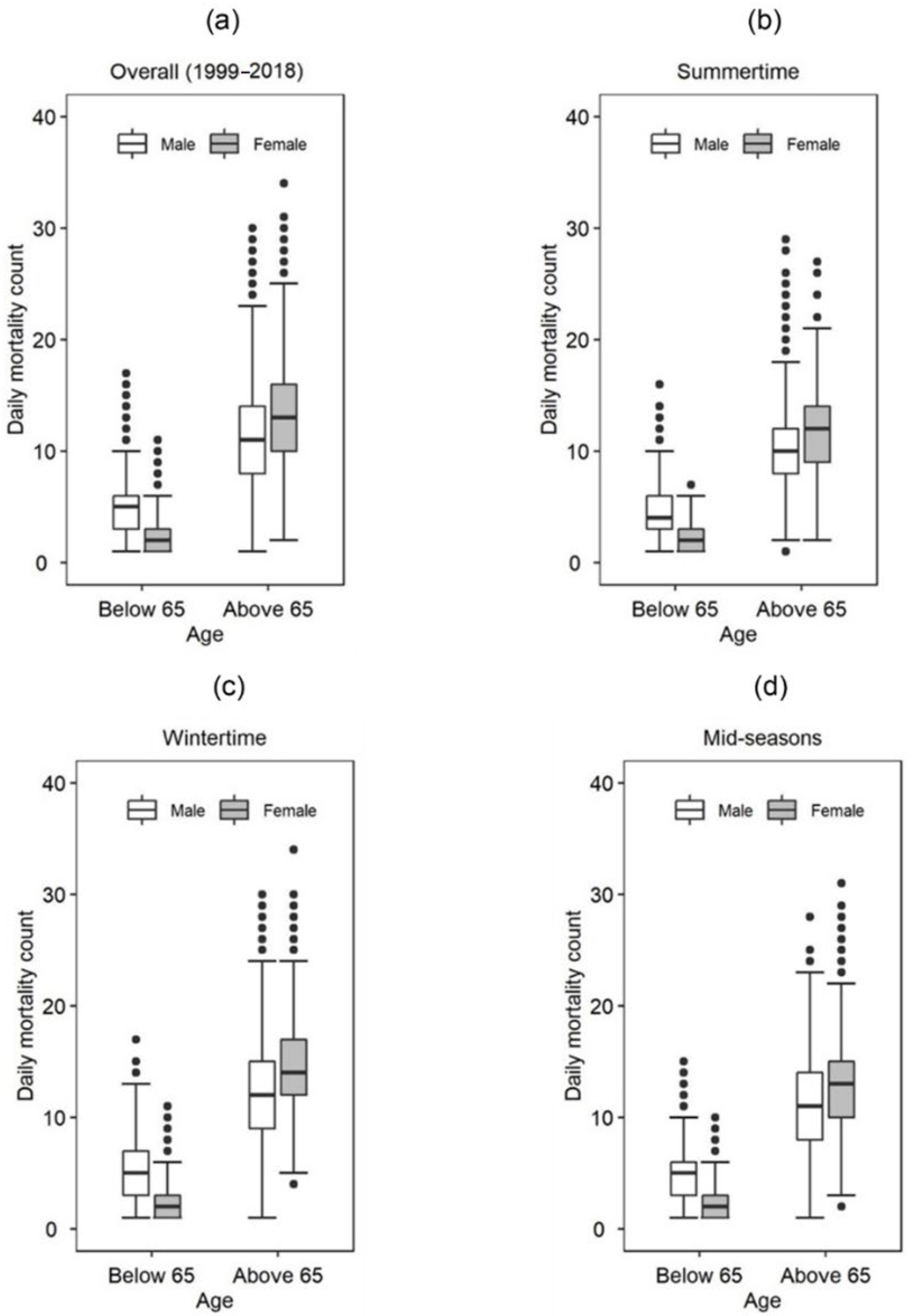
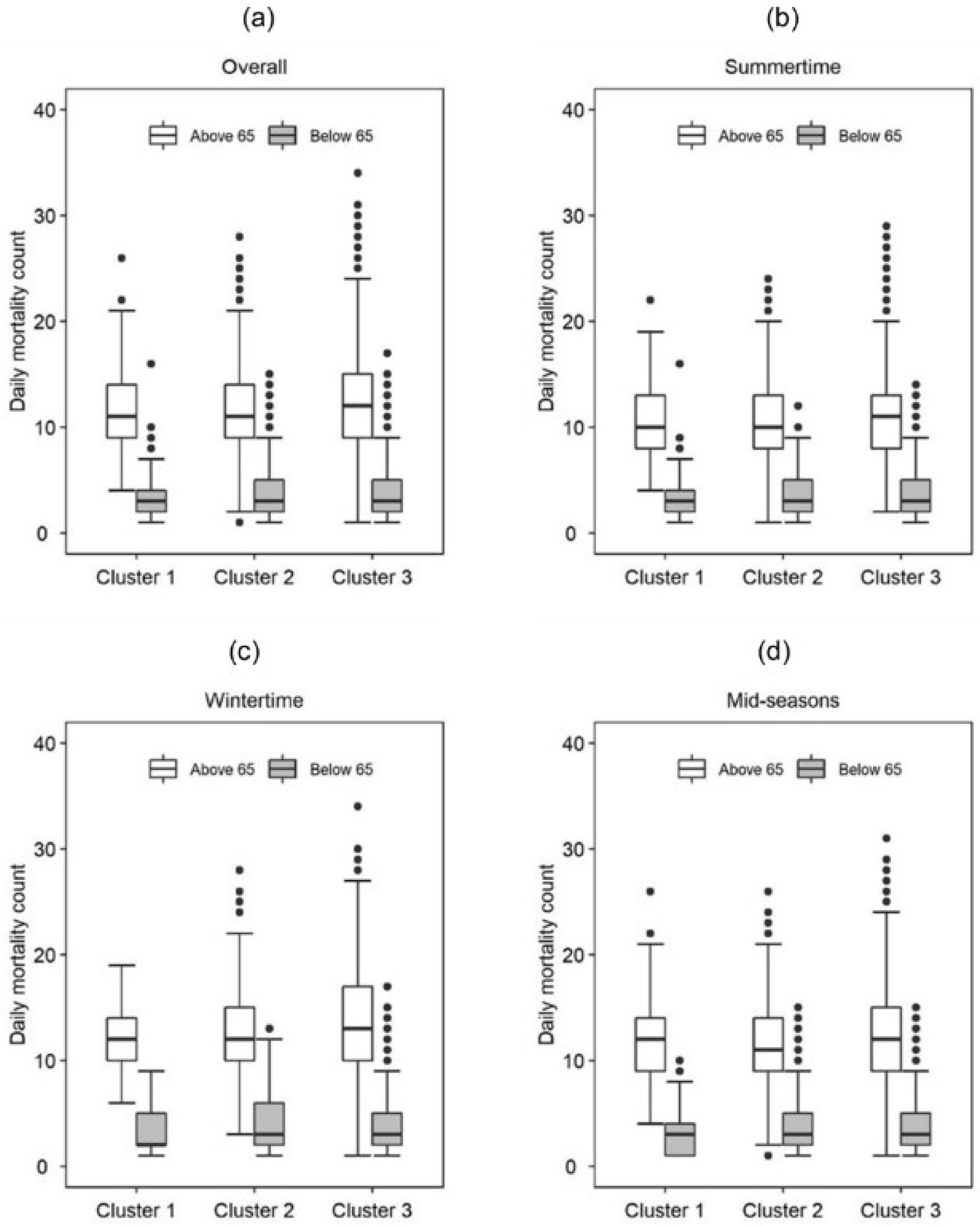
Furthermore, age was indicated as a significant factor contributing to heat-related mortalities. For instance, given the same outdoor temperature conditions, the number of mortalities was significantly higher for the “above 65 years” age group than the “below 65 years” age group. This finding also corroborates reports from previous studies [
52] and is potentially explained by the age-related differences in physiological mechanisms that influence thermoregulatory pathways. For instance, during elevated heat exposure, older individuals are reported to respond with reduced blood flow from the skin and minimized redistribution of blood from the splanchnic and renal circulations relative to younger individuals—as a result, core body temperatures increase, potentially leading to hypothermia [
71].
Low-educated groups showed higher mortalities than high-educated groups. We hypothesize that the primary reasons for the seen differences in heat-related mortalities among groups with different education levels are closely linked to occupational job differences and long-term differences in financial capabilities. For instance, individuals in the high education clusters are likely involved in professions often conducted in well-ventilated/heated indoor spaces, significantly reducing the toll of temperature extremes on their health; the opposite is likely true for individuals in low education clusters. Additionally, other lifestyle differences that arise from the variability in economic status between highly educated and low-educated individuals (e.g., quality of their homes, access to a nutritious diet, access to medical facilities) and that lead to accumulated health issues in the low-education group—these pre-existing issues could exacerbate the influence of extreme temperature deviations on low educated individuals leading to increased rates of mortality.
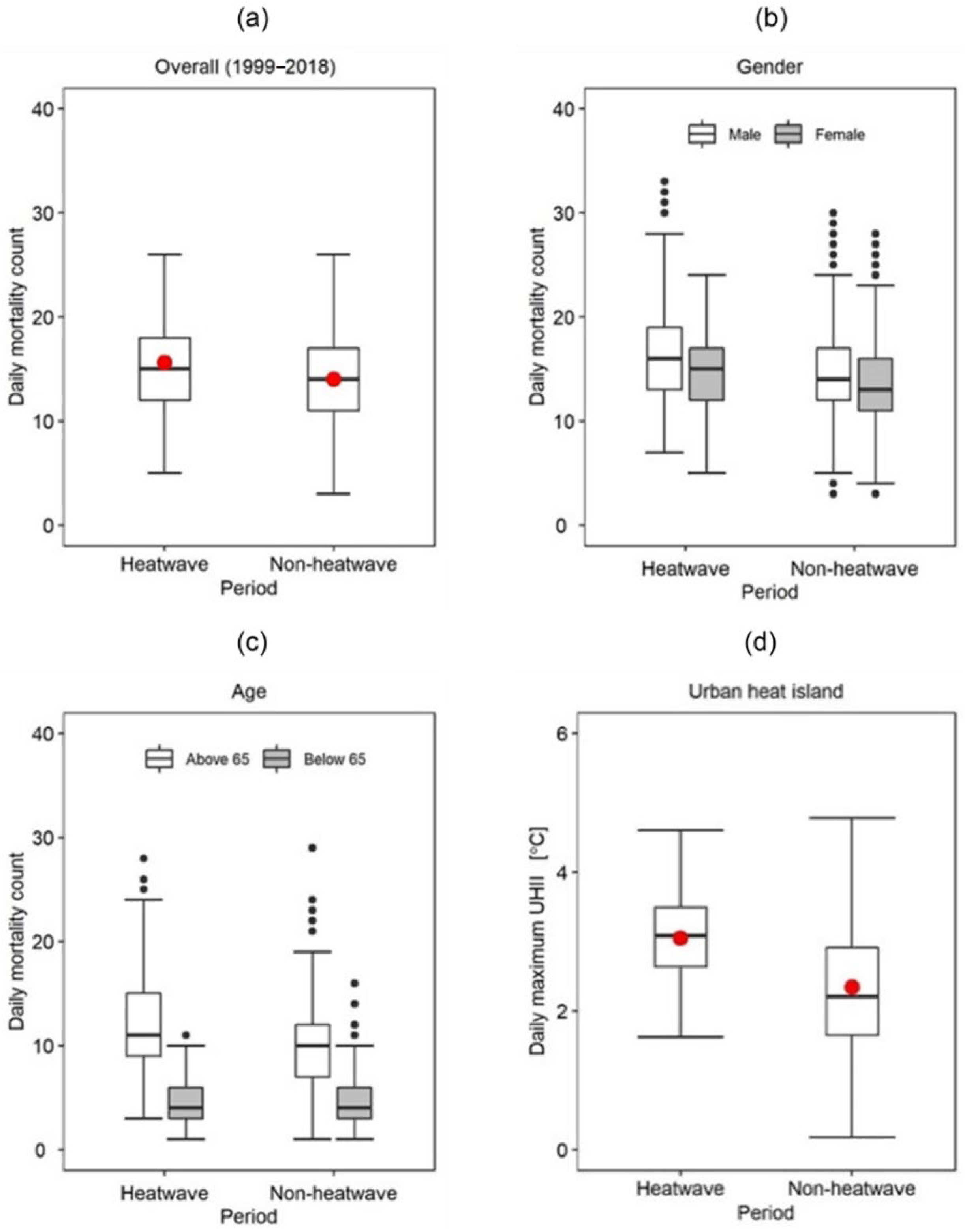
Our analysis also showed that, generally, heat-related daily mortalities were on average 1 death higher during HW than NHW periods. Such findings are commensurate with reports from previous studies; For example, a study on non-accidental deaths during HWs in European cities reported increases in HW-induced mortalities of up to 33.6% in Milan and 7.6% in Munich [
72]. The effect of HWs on heat-related mortalities is fundamentally explained by the earlier discussed severe pressure that heat exposure exerts on the thermoregulatory mechanisms of the human body. One specifically interesting observation relates to how gender modulates the influence of HWs on heat-related mortality. For example, we found that the number of heat-related deaths during HW was, on average, two deaths higher in males than females (see
Table 4). This finding corroborates recent observations in Seoul that report a slightly higher risk of male mortality than female mortality during HW episodes [
73]. However, numerous other studies have reported contradictory observations. For example, Fouillet et al., [
74], reported a higher percentage (i.e., 64%) of female deaths than male deaths during the 2003 HW in France. Similar reports have been observed in Chinese cities [
75] and more recently in Senegal [
76]. One potential reason for the contradictions in the literature is perhaps because a vast number of previous research have seldom considered other demographic characteristics likely to expose men more to heat risks, particularly during HW episodes. For instance, outdoor workers who consist mainly of a higher proportion of men than women are particularly vulnerable to exertional heat strokes stemming from elevated temperatures during HW episodes. Consequently, it is essential to analyze the effects of gender on heat-related mortalities during HW episodes for specific subgroups. Additionally, assessing the role of public health interventions and the implementation of early warning systems for extreme heat events on reducing heat-related mortalities would provide deeper insights on the real effect of HWs on temperature-related deaths. This would be particularly interesting as recent studies in South Korea [
77] have reported a relatively higher number of HW-related deaths in rural areas than urban areas. While such observations contradict existing theoretical evidence, they also point to the lack of in-depth analysis on the impact of HW on temperature-related mortalities that considers other overlooked social-economic characteristics such as the prevalence of HVAC usage and availability in the much-developed sub-regions of Seoul city. The observed effect of HWs on mortality is also potentially amplified by the additional influence of UHI. Previous studies [
20,
22,
78] have drawn linkages between HW and UHI, illustrating synergetic interactions between the two elements. These interactions are also found in the present study (See
Figure 9) and further point to the usefulness of UHI mitigative measures in reducing mortalities during HWs.
We also assessed the potential effect of UHI on heat-related mortalities across sexes and age groups. Our results showed that the number of heat-related mortalities was significantly higher in high UHII clusters than low UHII clusters, particularly for the “above 65” age group and the females, further pointing to the attenuated sensitivity to heat exposure by females and the elderly. It is worth noting that the direct influences of UHI on heat-related mortality have been somewhat neglected in the literature despite its obvious significance for climate-resilient environments [
79] and adaptive potential that can be achieved through implementing UHI mitigative strategies [
80]. Studies that precisely assess the effect of UHI on heat-related mortality are warranted and critical in the development of robust urban health policies. Furthermore, it is worth noting that although the models relating UHII to seasonal mortality explain relatively low mortality variations (see
Table 7), the models are still statistically significant at a
p-value < 0.05, indicating a good fit of the model to the data. Perhaps increasing the amount of data could better establish the inferred relationship between UHI intensity and mortality in Seoul—this is one issue that can be looked into as large datasets covering long periods become available.
Our results also reiterate previous reports on the impact of seasonality on temperature-related mortalities [
81]. The mortality risk is substantially lower during the summer months than in winter, which points to a more serious concern for cold-related mortalities than heat-related mortalities in Seoul, especially for females and the elderly (e.g., >65 years of age). One potential reason for the higher mortalities during cold periods is linked to bronchoconstriction likely to develop during exposure to extreme cold conditions. Cold exposure also weakens mucociliary defenses, which cause respiratory infections and potential inflammation [
82]. These conditions are likely to persist longer than those caused by heat exposure. They have been reported as the potential reason for the higher mortalities during colder periods than hotter ones [
83]. This observation has wide implications, particularly regarding the current research trends in the field. Most of the research in the field seems to focus more on the consequences of heat-related mortalities, yet cold exposure claims higher mortality counts. Our findings agree with those by Gasparrini et al. [
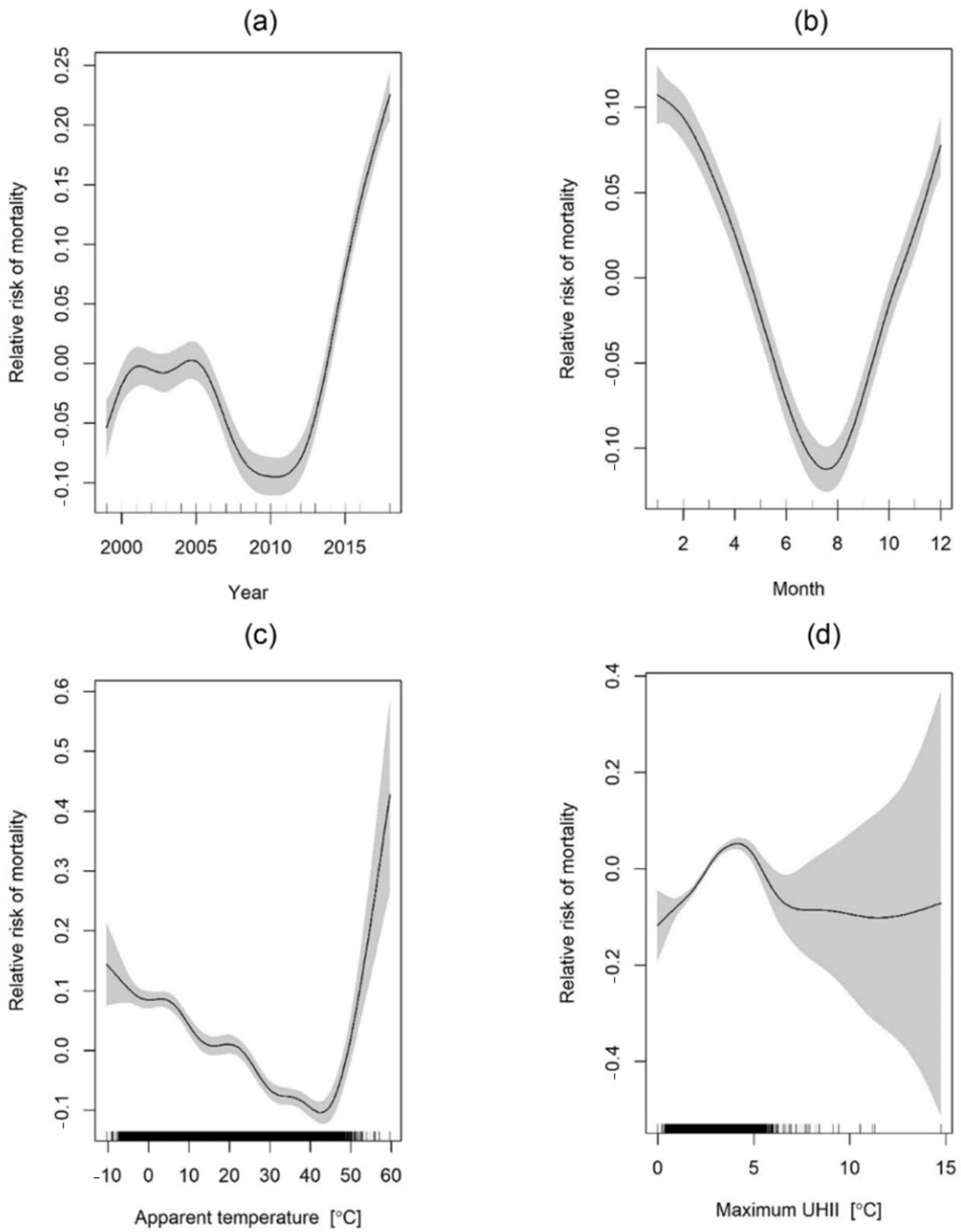
84], who critically reviewed existing epidemiological studies and found higher mortalities associated with cold exposure than heat exposure. This observation is useful for public health policies, particularly for Seoul city, as it evidences the mortality risk associated with cold exposure and provides a platform for discussing relevant policies and mitigation strategies. Moreover, while our results show a decline in the risk of temperature-related mortalities over the years for the “below 65 age group” (see
Figure 16a), the risk increased substantially for the “above 65 age group” (see
Figure 15a). This finding partly contradicts previous observations [
85] reporting a temporal decline in heat-related mortalities during summers in South Korea and cold-related mortalities in London [
86]. The contradictions are, potentially, because studies in the field have often concentrated on different demographics with no agreed-upon categorization scheme. For instance, the definition for elderly individuals seems to lack consistency across studies in the literature. Moreover, the role of improved infrastructure, technology, and public health interventions is seldom incorporated into the analysis. With such uncertainties, understanding the effect of temperature on human health becomes even more challenging. There is thus abundant space for analyzing temporal trends in temperature-related mortality in Seoul, particularly considering other social-economic elements (e.g., prevalence and use of aiding mechanical equipment) and newly implemented urban policies.
























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}