1. Introduction
Environmental concerns such as global warming and land use, which result from human activities, are often consequences of “larger and complex chains of cause and effect, [that] will shape their future” [
1]. Deforestation and the subsequent use of cleared land for intensified farming, for instance, has many negative environmental impacts, including loss of biodiversity in terms of flora and fauna due to permanent plantations grown in monocultures [
2]. Modern tools and technologies are therefore needed to make it possible to better understand and address different aspects of such complex human–environment interactions [
3]. In this regard, maps can play an important role, forming the basis for these tools and technologies for supporting geospatial human–environment resource management and decision making [
4], among other tasks.
Similarly, maps also play an important role in epidemiology and public health, both of which have, once again, complex chains of cause and effect including environmental factors. In fact, with the advent of geographical information systems (GIS) and advanced information visualisation techniques, interactive maps have become essential tools for the analysis of geographical patterns of disease incidence and prevalence, as well as communication of public health knowledge, as dramatically illustrated by the proliferation of web-based maps and disease surveillance “dashboards” during the COVID-19 pandemic. However, this increased use of interactive maps to present health data goes beyond public health information dissemination, with map-based interfaces being widely used in support of analytical tasks in epidemiology and public health research and practice as well.
Epidemiology can be defined as “the study of the distribution and determinants of health-related states or events in specified populations, and the application of this study to the prevention and control of health problems” [
5]. This definition conveys geographical, temporal, and causal elements which have been the focus of map-based interfaces and systems, in public health, and other domains.
In relation to infectious diseases, particularly those that are vector-borne and occur in areas affected by substantial changes in land use and climate, informatics support for epidemiological work needs to be able to provide effective means of gathering and aggregating information from diverse sources [
6], including land use, climate, human movements and population density, distribution of peri-domestic and sylvatic animals which could act as disease reservoirs, distribution of disease vectors (such as mosquitoes, sandflies, etc.), disease incidence and prevalence, healthcare services and infrastructure, and public health interventions, among others. These complex information requirements create a number of challenges for system design.
The nature of the challenges faced by designers of such systems illustrates fundamental issues in spatio-temporal visualisation. Tackling these issues involves addressing how map-based interfaces can support real-world scenarios and use cases involving collaborating multidisciplinary teams, as well as challenges related to the integration and appropriate granularity of spatial public health data, cluster identification, and statistical modelling, visualisation of change, identification of causal relationships between variables that characterise the evolution of spatio-temporal events, and assessment of the effects of public health interventions.
While GIS have provided a basis on which to build interactive systems to address these requirements and support some of the related tasks, they lack the ability to incorporate the vast amounts of geo-referenced data created everyday on an ad hoc basis by internet users. These data, which by some estimates could comprise as much as 2 exabytes (
bytes) per day, have been regarded as a potentially valuable source of epidemiological information [
7]. At the other end of the spectrum, there is the issue of incorporating individual citizen, researcher, and healthcare professional input specifically related to a particular disease surveillance task into GIS databases. While many systems have been developed that employ both ad hoc and task-specific user-generated data [
8], general issues related to the integration of spatial and temporal data in interactive systems remain an active area of research.
In this paper, we review these issues, and describe approaches to addressing them in interactive systems through the analysis of uses of map-based interfaces for supporting epidemiological research and decision-making in public health in collaborative settings. We start with a brief overview of traditional cartographic maps in general, and then introduce interactive maps and map-based interfaces, followed by their applications in epidemiology, pointing out current developments and existing challenges in this area. Finally, we illustrate these issues by describing a practical application of map-based interfaces in research on health and the environmental and socioeconomic factors affecting the spread of infectious diseases in an Amazonian region, in South America, involving multidisciplinary collaboration.
2. Maps, Interactions and Applications in Epidemiology
While everyone would claim they know what a “map” is, the term
map itself may mean rather different things to different people, and it may vary from person to person and from culture to culture [
9], as a compilation of three hundred and twenty one different definitions of the word “map” by Andrews [
10] would attest.
Similarly, although most people would think of a map as some form of representation of a geographical area, others would argue that maps can be used to represent many other kinds of information, some of which may even have nothing to do with physical reality—for instance representing political, cultural, or historical information [
11].
However, what all maps have in common is that they generalise and simplify the information they represent, rather that trying to fully represent any reality [
12], and by doing so, they may distort or compromise that information [
13]. All maps also project salient and relevant aspects of such information onto a geometry—in the form of bounded objects—with certain topological properties, in a manner similar to geographical projections but not always corresponding to geographical objects. As such, every map is a representation of reality and “not reality itself” [
14]. Despite this, to function well, maps need to maintain a sufficient level of accuracy necessary for the tasks they are designed to support [
13]. In addition, maps that more closely represent reality are more likely to support their intended tasks than those that do not [
15].
In that sense, geographical maps are perhaps the most functional type of maps, because they represent some form of physical reality, projected onto a 2-dimensional (2D) space [
9]. Indeed, the earliest maps are thought to have been created to help people find their way [
16]—what is referred to more commonly as
wayfinding—in some “real” physical or metaphysical world. There are of course many types of such geographical maps, each supporting a particular range of tasks. These include, for instance, cartographic maps [
17], tourist maps [
13,
18], road maps [
9], and public transport maps, such as the well-known London Underground map [
19].
Tyner [
20] focuses on the functionality of geographical maps and divides them into three main categories:
General-purpose maps or reference maps do not emphasise any particular geographical feature over another, but instead show the location of different geographic phenomena, such as cities, roads, rivers, etc.
Special-purpose maps are targeted at specific users and their needs, such as geological maps, soil maps, weather maps, etc.
Thematic maps tend to show a single distribution over a spatial background or framework, to help locating the distribution being mapped, such as population density, land use, family income, rain fall, etc.
In contrast, Lambert and Zanin [
14] focus more on the representational aspect of geographical maps and divide them into two main categories:
Topographic maps represent concrete elements resulting from direct observations of, for instance, roads, waterways, buildings, etc.
Thematic maps represent localisable qualitative and quantitative information using rules of graphical semiology [
21].
Maps used in epidemiology and public health work are often of thematic type, regardless of whether their functional or representational aspects are considered first. In fact, maps used for public health–related purposes—in the form of disease maps [
22]—might constitute one of the earliest forms of thematic maps. The use of such thematic maps to monitor, explain, and predict patterns of disease spread as part of epidemiological reasoning dates back at least to the late 18th century [
22]. The best known example of this type of disease mapping is the study of the cholera epidemic in London in 1845, in which John Snow used a map to argue that the majority of cholera deaths occurred near a water pump in the Broad Street neighbourhood of Soho, and therefore proposed that cholera was likely to be a water-borne disease [
22,
23,
24].
2.1. Interactive Maps
Regardless of their type, all maps are visualisations, and as such, they aim to support seeing and exploring their underlying data in different ways [
9]. More specifically, maps are designed to help their readers perform a range of tasks, including for instance identifying locations of interest, getting data related to those locations, identifying any data patterns related to those locations, or making spatial comparison between such patterns at different locations on the same map, or between different maps [
25]. Sometimes it is also necessary to compare data patterns across time, either for the same location—i.e., temporal comparisons—or between different locations—i.e., spatio-temporal comparisons.
Bertin [
21], for instance, discusses how multiple maps juxtaposed on a 2D plane can help viewers identify patterns in geospatial data more readily. Similarly, Carr and Pickle [
26] use the idea of
small multiples, as proposed by Bertin, to suggest
micromaps as a technique for highlighting geographical patterns in data.
While it is possible—as has been the case for centuries—to perform a wide range of tasks using static maps, it is clearly more effective and often more efficient to perform them using interactive maps [
20]. For instance, it has been argued that making side-by-side comparison of maps is not generally very effective for investigating spatial correspondence between them [
15]. It has, therefore, been necessary to develop interactive techniques such as
layering to deal with some of the limitations of static maps [
27]. For example, Andrienko et al. review interactive methods for spatio-temporal visualisations [
28] and identify some of the challenges in this field [
29].
Interactivity can, of course, take place at different levels and does depend on the application area and the context of use. It can refer to any tool, in the form of a standalone application or a webmap [
9], that allows users to set different parameters used to generate, control, and display maps during their use, and by doing so, extend the user’s interaction capabilities far beyond those possible with static maps [
30]. Furthermore, while there are a wide range of interactive map systems, their level of interactivity is always constrained by the number of parameters they allow their users to manipulate, and to what extend and by which means [
30].
Despite these constraints, however, in many modern computer applications, maps go far beyond their traditional functionality of simply presenting data, and can therefore be considered as versatile interfaces to geospatial data [
31] as well as other types of data, including epidemiological and public health data. Such interactive map-based interfaces need to support “information exploration and knowledge construction […] without hypotheses about the data” and through “unencumbered search for structures and trends” [
32].
In more recent years, the availability of powerful API for web-based map systems has made it possible to overlay geospatial data on interactive maps in a wide range of applications [
27]. This is achieved using
layers of data, which can be turned on and off to show or hide different data sets that the users are familiar with [
33]. Maps are also being used increasingly as the underlying framework for a wide range of decision support systems, web-based information systems and computer games targeting environmental issues [
30].
2.2. Interactive Maps in Scientific Research
Maps have gained currency as geographic visualisation tools in scientific research over the past few decades. DiBiase [
34] has, for instance, proposed a framework for map-based scientific visualisation, in an attempt to define the use of maps in scientific research—particularly in earth sciences. In this framework, scientific research is considered as a four-stage process which consists of
private visual thinking—i.e., the exploration and confirmation stages—and
public visual communication—i.e., the synthesis and presentation stages. Maps can be used both at the initial stages of research for private visual thinking, as well as at the later stages for public visual communication of research findings. In this context, cartography can therefore be considered as a research tool for discovery of new scientific knowledge, in addition to communication of what is discovered.
MacEachren [
15,
35,
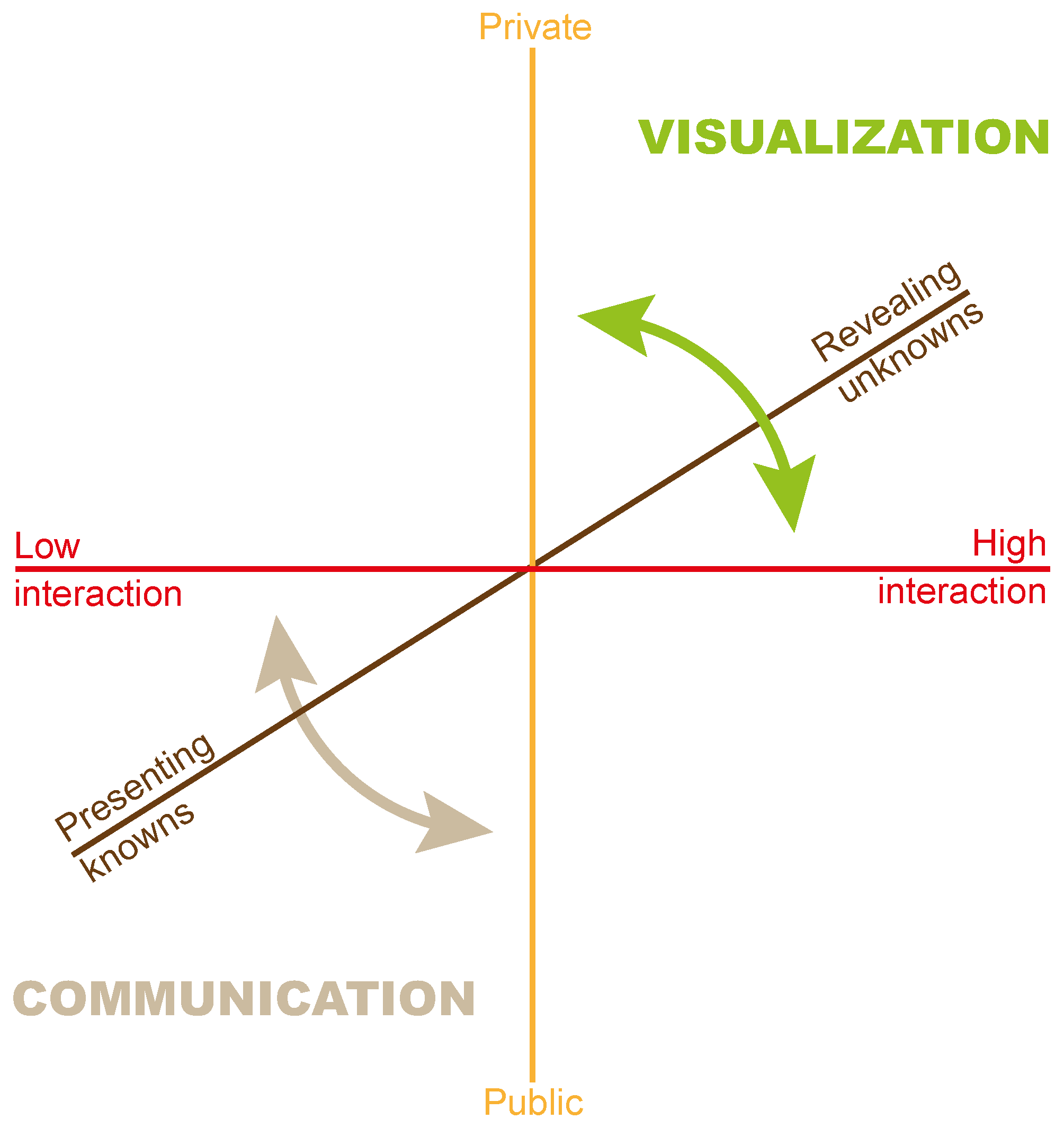
36] expands on the framework proposed by DiBiase, incorporating the work of others to define cartography as a “cube” space based around how maps are used, rather than just how they are made.
Figure 1 provides a representation of this cube space as proposed by MacEachren for defining maps in terms of their use for visualisation of unknown and communication of known information. MacEachren [
35] defines this 3-dimensional (3D) space along three continua:
- 1
Private–public, ranging from generating maps for one’s own private use, to their use by a wider public audience.
- 2
Unknown–known, ranging from the use of maps for revealing unknowns, to their use for presenting knowns.
- 3
High–low interaction, ranging from high “human–map interaction” where users are able to manipulate maps substantially, to low interaction where users have limited ability to change the maps.
MacEachren [
35] notes that while there are no clear boundaries in this map use space, there are identifiable extremes in it. For instance, the uses of maps for geovisualisation type tasks are more towards the private, revealing unknowns, and high human–map interaction space. The communication type uses of maps, on the other hand, are more towards the public, presenting knowns, and low human–map interaction space. An example of interactive mapping used in a geovisualisation task that combines environmental and climatic factors is presented by Walker et al. [
37]. This application, while primarily aimed at private exploration (by experts) also provides support for public visualisation, illustrating a trend which has gained traction with the advent of web-based visualisation applications.
However, it is also important to note that, as MacEachren [
35] points out, no map use is possible without some level of interaction, and a high level of interaction does not necessarily mean the use of computer technology, “‘Interactive’ computer tools, however, expand the possibilities for ‘interaction’ with maps and thus the possibilities to facilitate visual thinking, perhaps in qualitative as well as quantitative ways” [
35]. It is this potential of maps as interactive tools for scientific research which is of particular interest to us in the context of this article.
Furthermore, it is equally important to note here that while interactive maps can be considered as powerful tools in scientific research, maps are by their nature designed artifacts, and as such, they only represent some form of reality, as discussed earlier. Therefore, the use of maps as tools in scientific research must take into account the inherent shortcoming of maps as partly subjective, rather than entirely objective, representations.
In this regard, one should keep in mind that maps, as visual representations, are essentially collection of signs, as well as being signs themselves. As such, maps aim to provide meaning to the signs they represent. MacEachren [
15] identifies three categories of meanings represented by maps, those about
space,
time, and
attributes in space–time. MacEachren further points out that “[b]eyond this basic taxonomy of meaning are questions about the specificity of sign relations, directness of references and associated literality of interpretants, differences in the concreteness of references given meaning through signs, and the etymology of specific signs or groups of sign relations” [
15]. These issues make maps highly interpretive visual tools—perhaps far more than other forms of visualisations—and such issues need to be taken into account when maps are used in scientific research. (A full discussion of all issues noted here is beyond the scope of this article. Interested readers are referred to [
15]).
In addition to the issues related to meaning in maps, there are also other limitations which should be considered when using maps. Tyner [
9] provides a summary of map limitations by dividing them into six categories:
The nature of maps: these relate to the fact that maps are always drawn to scale, usually using some kind of projection onto a 2D surface, by generalising details.
Data: these related to data accuracy, positional accuracy, lack of data, gaps in data, or the currency of data used in maps.
Technology: these relate to different hardware or software technologies, or the methods used for drawing/creation, delivery, or printing of maps.
Cartographer: these relate to the mapmakers’ skills, their knowledge of the subject, or their inherent biases as human beings.
Agency or client: these relate to the fact that maps are hardly ever neutral, and they are created to cater for the objectives or biases of those for whom they are created.
User: these relate to the limitations of map users/readers in terms of their lack of skills, or projecting their own stereotypes onto maps they are using, or indeed in using the wrong map for the task they need to perform.
These limitations are, however, not necessarily bad in themselves, but they may not always be obvious or deliberate [
9]. As such, it is important to be aware of their possible negative impact, without considering them as reasons for not using maps in scientific research.
2.3. Interactive Maps in Epidemiology
Static maps often function as
coordinative artifacts [
38,
39] in enabling the
articulation work [
40] of multidisciplinary teams engaged in disease surveillance and epidemiological tasks. In such cases, maps have been used to plan interventions, to divide and coordinate the work of medical professionals and researchers, to track the progression of epidemics, and to focus discussion and analysis task in co-located meetings. This kind of use of shared artefacts is characteristic of cooperative work in multidisciplinary settings, including multidisciplinary medical team meetings, where it serves to structure team communication [
41]. Effective coordination mechanisms can in fact be employed on shared physical maps with the help of physical actions (e.g., placement of push pins, annotation, etc.) and careful design [
42].
The advent of interactive maps has, however, enabled vastly enhanced support for collaboration in epidemiology, as well as in other areas of public health. Interactive web-based “dashboards”, for instance, have contributed to geovisualisation tasks and made it possible for researchers, public health officials, and policy makers to share up-to-date information on disease spread [
43]. In this regard, interactive maps offer a powerful tool for the visualisation of variations in disease burden in populations across places and time—in what is known as
spatial epidemiology—helping to characterise geographically global and local determinants of population health heterogeneity [
44,
45].
As noted above, spatial elements have been an integral part of epidemiological work since the establishment of the discipline in its current form, by supporting the key analytical tasks of discovering disease clusters, predicting disease spread, monitoring exposures, analysing location-related social determinants of health (such as environmental changes, neighbourhood infrastructure, and socioeconomic demographics), and assessing the effects of public health interventions. Lately, technologies that enable large-scale data collection (including but not limited to crowd-sourcing, social media analysis, citizen science) and mobile collaborative tools have also started to provide more widespread use in spatial epidemiology [
46]. While these tools have enjoyed popularity in the visualisation and data science community, and their potential has been acknowledged in spatial epidemiology, concerns still remain about incompleteness, inconsistency, and bias issues that often affect data acquired through such tools [
44].
Therefore, the need for more robust methods for aggregation of diverse data sources for analysis and visualisation through interactive maps is well established [
47]. In response to this need, conventional epidemiological models have been supplemented—and in some cases replaced by—new methods such as agent-based modelling [
48] to facilitate the incorporation of molecular epidemiological [
47] and social network data into map representations [
6].
In addition to the challenges related to the incorporation of new technologies and data sources to epidemiological maps, other more fundamental issues also remain, some of which are exacerbated by the greater availability of data that has followed the introduction of web and mobile communications technology, and by the nature of interactive visualisations in general. These issues can be classified into two main groups: (1) inherent constraints of spatial representation, and (2) issues representing temporal information. These issues are, therefore, further discussed in the following sections.
2.3.1. Spatial Representation
As regards spatial representation, challenges include: the risk of cognitively overloading or misleading users [
47], the granularity of geo-referenced data [
44], security and privacy issues, and the need to integrate map visualisations within different public health tasks [
49,
50] and epidemiological processes and patterns [
51].
Map representations of disease spread may mislead users by suggesting the presence of visual patterns or clusters which turn out to be spurious products of spatial autocorrelation—such as the fact that values for one geographic location naturally tend to be similar to those of nearby locations—or conversely, by obscuring the presence of actual clusters due to arbitrary boundaries (e.g., municipality, region or country borders). Fortunately, statistical methods for analysis of autocorrelation have been proposed, which help users assess potential distortions due to spatial proximity [
44]. Similarly, kernel methods have been used to overcome issues relating to the impact of geographical boundaries (e.g., see [
52]).
The issues of geographical granularity and privacy are inter-related. While geo-referenced epidemiological data are usually available in aggregated form, there is arguably a need for more granular data—at the level of individual position and mobility—such as the information that can be derived from GPS devices which are now ubiquitous, thanks to the widespread penetration of smartphone technology. Such information could be used, for instance, to determine individual exposure to diseases and predict their outbreaks. However, reconciling the needs of public health and individual rights can be a delicate balancing act, as illustrated by experiences of some countries during the COVID-19 pandemic [
53,
54].
Finally, there are many different uses for static and interactive maps, and users of spatial epidemiological data have likewise diverse tasks to perform, often involving different sets of requirements. We review an example of such diversity in more detail in
Section 5.
2.3.2. Temporal Representation
Integrating temporal aspects to essentially spatial artefacts such as maps poses challenges that go beyond those faced in epidemiological contexts [
28,
29]. Time is of vital importance to epidemiology, as the discipline seeks to identify and test causal relationships between exposures and outcomes, and time is intrinsic to causal analysis.
Visualisation of spatio-temporal data can be accomplished in static maps through multiple snapshots depicting cross-sections of the temporal evolution of events of interest—e.g., successive depictions of infection rates over a geographical area—or location changes [
55,
56]. However, interactive maps can also utilise animation—e.g., in the form of snapshots in time, movement histories and time windows [
28]—to reveal change patterns that might not otherwise be apparent in static snapshots. Such designs can be conceptualised as treating time as a cartographic variable—similar to Bertin’s visual variables [
21]—as suggested by cartographic research [
15,
42].
As with spatial epidemiology, temporal epidemiological maps face a need for underlying disease and process models that can be better integrated to spatio-temporal analysis [
45]. In this regard, and as we have previously pointed out, agent-based models [
48] which can better account for complex boundary conditions and the spatio-temporal dynamics of disease spread, offer a promising alternative to traditional differential equation models [
6].
Finally, temporal map-based visualisations need better support for causal inference, to enable the user to relate spatio-temporal changes to statistical data, and make assumptions about causal relationships [
57]. This is a complex issue that will likely provide fertile ground for research for many years to come.
3. Tasks and Requirements
In conducting a field investigation, epidemiologists are faced with several tasks that require the use of maps and GIS tools. These tasks are well documented in epidemiology practice and in books such as the
CDC Field Epidemiology Manual [
58]. Implicit in these practices is the fact that field investigations are usually carried out by research teams encompassing investigators of different disciplinary backgrounds and expertise. Therefore, although the tasks and requirements for GIS and interactive visual tools are often described in relation to a relatively uniform set of functions, different aspects of field work will dictate specific uses of software tools and visualisation methods.
Foster et al. [
59] summarise the tasks and steps of epidemiological field investigations. These involve: (1) preparatory steps, (2) confirmation of diagnosis, (3) assessment of epidemics, (4) case counting, (5) descriptive epidemiology, (6) interventions, (7) hypothesis identification and testing, and (8) communication of findings.
In preparing for field work, maps can be used from the start for creating situational awareness, that is, for establishing the geographical areas of interest. While publicly available online maps such as OpenStreetMap [
60] are valuable for preparation work, their coverage of remote geographical areas may lack sufficient detail [
49], or may even be inaccurate sometimes. In such cases, if available, local map resources such as printed maps may be used for this purpose. Preparation also includes surveying existing data resources and developing a strategy for data collection, as well as selecting or developing the necessary software tools to be used. Foster et al. [
59] recommend engaging the services of a GIS subject matter expert to assist with these tasks.
Following the planning stage, and confirmation and geo-referencing of diagnoses, maps and GIS can be employed to assist in determining whether an epidemic is taking place. In this task, interactive maps being used should enable the researcher to collate detailed population data to estimate risk of infection. Such interactive maps should also be flexible enough to provide views of different boundaries that might affect disease spread, including national or state borders—which might affect disease spread due to different public health policies and resources across the boundaries. Interactive maps should also support consideration for environmental and climatic factors that affect the spread of diseases—e.g., the ability of a vector to migrate between forest and urban regions may be affected by changing patterns of human activity, such as road building. As mentioned earlier, in epidemiology, being able to monitor infection rates in space and time is crucial for the estimation of such risks.
Once the necessary background data and software tool and resources have been assembled, the tasks of keeping track of disease case incidence, and recording individual case data in relation to their specific location, time, and descriptive population attributes need to be carried out. Interactive maps can be instrumental in supporting these tasks as well, from the perspective of data collection and spatio-temporal visualisation—as will be illustrated in
Section 5.
Visualisation tools and interactive maps can also support the generation of hypotheses concerning future patterns of epidemics—for instance, in estimating the impact of climate change on disease spread [
61] —as well as supporting the design of studies to investigate those hypotheses. Similarly, these tools can assist in the implementation and evaluation of interventions and prevention policies by enabling researchers and healthcare authorities to assess the efficacy of different measures, as well as identifying any possible long-term trends.
A final step in the epidemiological investigation process described by Foster et al. [
59] is the task of communicating findings, which includes dissemination of situation awareness, as seen for instance in the use of web-based maps during the COVID-19 pandemic [
62,
63]. While this is certainly an opportune use for interactive maps, there are a variety of other scenarios in which interactive maps can act as effective communication tools. As mentioned before, maps can act as coordination artefacts in support of communication among multidisciplinary team members, extending beyond epidemiological investigations and filed work—an example of this is described in
Section 5.2. Another use of interactive maps as communication tools is in health promotion and communication with the wider public in support of behaviour change for risk reduction. An interactive stylised map has been used, for instance, in a multi-user
serious game designed to promote behaviour change towards elimination of environments favourable to sandfly breeding (e.g., areas of accumulation of leaves, rubbish, and stagnant water near residences) in rural areas [
64].
4. Enabling Technology, Resources, and Standards
Geographical information systems as tools for integrating and analysing spatial data have played a vital role in the wider area of environmental health since the 1980s and of epidemiology since the 1990s [
65]. The primary role of GIS in these contexts is that of assisting the process of surveillance. Cromley and McLafferty [
65,
66] define three types of surveillance for which GIS could be used: (1) hazard surveillance for monitoring air pollutants, disease vectors, soil chemicals, etc., (2) exposure surveillance for monitoring how people have been exposed to hazards, and (3) outcomes surveillance from monitoring the health impact of exposures. Other visualisation tools and analysis methods can then utilise GIS to help researchers answer their underlying fundamental question of “How are health outcomes related to environmental hazards and exposures?” [
66].
However, although the importance of these types of analysis tools and visualisations in epidemiology and public health has become increasingly acknowledged, there are yet to be widely adopted and used in practice. A major hurdle in adopting them is their availability and associated cost, particularly in under-resourced regions where they are in fact often most needed. Since most such tools and visualisations are largely dependent on geographical information systems, which in turn utilise data from trusted, but also expensive, sources such as government or ordnance surveys, this makes them unavailable or sparsely updated in developing countries [
67].
In contrast to GIS, Volunteered Geographic Information (VGI) “represent a paradigmatic shift in how geographic information is created and shared and by whom, as well as its content and characteristics” [
68]. Defined broadly, VGI refers to geo-referenced data created by citizen volunteers [
69]. Using this definition, Fast and Rinner [
70] describe VGI systems as the environments for creating crowdsourced VGI information products. They also define the three components of a VGI system to be: (1) the project and its initiators, (2) the participants volunteering their geographic information, and (3) the technical infrastructure required to implement the system [
70]. The technical infrastructure in turn needs to provide the necessary functions for the input, management, analysis, and presentation of VGI. Fast and Rinner propose that when a VGI system is being considered for development, all these components need to be defined clearly. However, despite their increasing popularity, there are still barriers to the adoption of VGI [
71] systems, among which are those related to concerns about their data quality and incomplete representation [
72].
Perhaps one of the most successful VGI projects is the OpenStreetMap [
73] participatory mapping application. OpenStreetMap (OSM) provides the technical infrastructure to allow its worldwide contributors to collaboratively edit the OSM world map and create its open source cartographical outputs [
60]. OSM can be considered as a valuable tool for developing interactive map-based visualisation systems and analysis tools to support epidemiology and public health research and collaboration work. Yet, like most other VGI systems, OSM is rarely used for tasks such as epidemiology and exposure assessment studies [
67]. This is often due to concerns about its data quality. Senaratne et al. [
74] note that the reason for this varying quality is because OSM data is being generated by heterogeneous contributors, using a range of different tool and technologies, with different levels of detail and precision, serving heterogeneous purposes, and without any gatekeepers to ensure data quality and accuracy.
In addition to these limitations, both GIS and VGI systems require a high level of technical skills to develop and use for epidemiology and public health research purposes. Maantay and McLafferty [
65] identify some of the challenges involved in using GIS for environmental health cases, all of which also apply to the use of VGI systems for epidemiology and public health research as well. Apart from requiring technical skills and knowledge of statistical and quantitative analysis methods, this type of research requires for instance access to correct data sets in suitable formats, the ability to manipulate and prepare the data sets for analysis, as well as having sufficient expertise in working with large data sets [
65].
To address the issues of geographical health data quality and accessibility, major public bodies, such as the World Health Organisation (WHO), the US’s Centers for Disease Control and Prevention (CDC), and the European Centre for Disease Prevention and Control (ECDC), have undertaken efforts to create publicly available data sets and resources which can be used by researchers in creating disease maps and interactive applications for various purposes. Other efforts along these lines are also being made at national level in countries such as China [
75].
Along the same lines, the WHO is also launching its own GIS Centre for Health [
76], which aims to bring the benefits of GIS to many countries that currently lack access to this technology, in order to strengthen their health information systems. This centre will provide map standards and services, satellite imagery support, geospatial data sets, mobile data collection tools, health databases, and a GIS software hub, as well as training for their use.
Similarly, the CDC maintains a collection of GIS resources [
77], in addition to distributing the widely used
Epi Info tool to facilitate the use of statistics, maps, and graphs for public health professionals for outbreak investigations, and building of small-scale disease surveillance systems [
78]. Another comprehensive source of health and geographical data is provided by the ECDC, which provides tools such as interactive dashboards, databases and maps, in addition to raw data sets [
79].
There are also many attempts at making the integration and sharing of GIS data more effective by, for instance, proposing specialised ontologies that would provide description of geospatial data in a more unified manner [
80]. Such efforts are in support of attempts at creating more structured data representations, in a manner similar to XML-based markup languages. An example of these is GML (Geography Markup Language), developed by the Open Geospatial Consortium (OGC), as an XML-based grammar for expressing geographical features [
81]. Another related XML-based markup language, also adopted and developed further by OGC, is KML (formerly known as Keyhole Markup Language), which can be used for developing geographic visualisations, and allows annotation of maps and images using text, icons, etc. [
82].
5. Applications of Interactive Maps in Disease Surveillance Research
In this section we present an example case study, based on our own experience of developing interactive map-based tools for disease surveillance research, which relies on combining and visualising environmental factors together with disease data, using a range of technologies for data collection, monitoring, and collaboration. The aim here is to demonstrate how some of the concepts discussed so far in this article can be applied in practice in a real-world project.
A few years ago, we participated in a multidisciplinary research project aimed at studying the determining factors in the spread of neglected infectious diseases in the Peru–Bolivia–Brazil “tri-national” borders [
83]. This study encompassed complex, inter-related environmental, geographical, and socioeconomic factors, including global climate change, the dynamics of land use and cover in tropical forests, migration patterns, population dispersion, and access to healthcare. To support the research, computational, and analytical requirements of this team, we approached health management from a multidisciplinary perspective that combined the environment, human ecology, disease surveillance, and patient care.
As the team comprised researchers (epidemiologists, human ecologists) and healthcare professionals (clinicians and public health managers), we adopted a broad perspective of information exchange, whereby support for collaboration needs could be provided at different levels, in aid of different but inter-related activities, covering support for nurses and community healthcare workers working in remote locations, tools for collection and maintenance of patient records, and provision of exposure and disease data to epidemiological surveillance bodies.
To this end, we developed a set of tools that combined mobile devices for patient care and epidemiology research in the field, centralised databases for modelling and generation of alerts, and support for both synchronous and asynchronous communication. These tools were tied together through map-based interactive visualisations and interfaces which served as the team’s basic coordination mechanisms [
39], while retaining the ability to support a range of tasks performed by specific groups.
Here, we will examine the uses of interactive maps for supporting two specific types of tasks in that project to illustrate this approach. These tasks were: (1) mobile support for fieldworkers in collecting and monitoring of disease data [
49], in the context of surveillance of Bartonellosis and Leishmaniasis, two neglected tropical diseases, and (2) collaborative analysis of spatial epidemiological data by researchers and public health managers [
50], in the context of epidemiological research on Leishmaniasis incidence in the Brazilian state of Acre. Our aim here is not to fully describe the implementation details of the interactive tools and visualisations developed for either of these two tasks—or any of the other tools developed as part of the bigger project (e.g., for diagnosis [
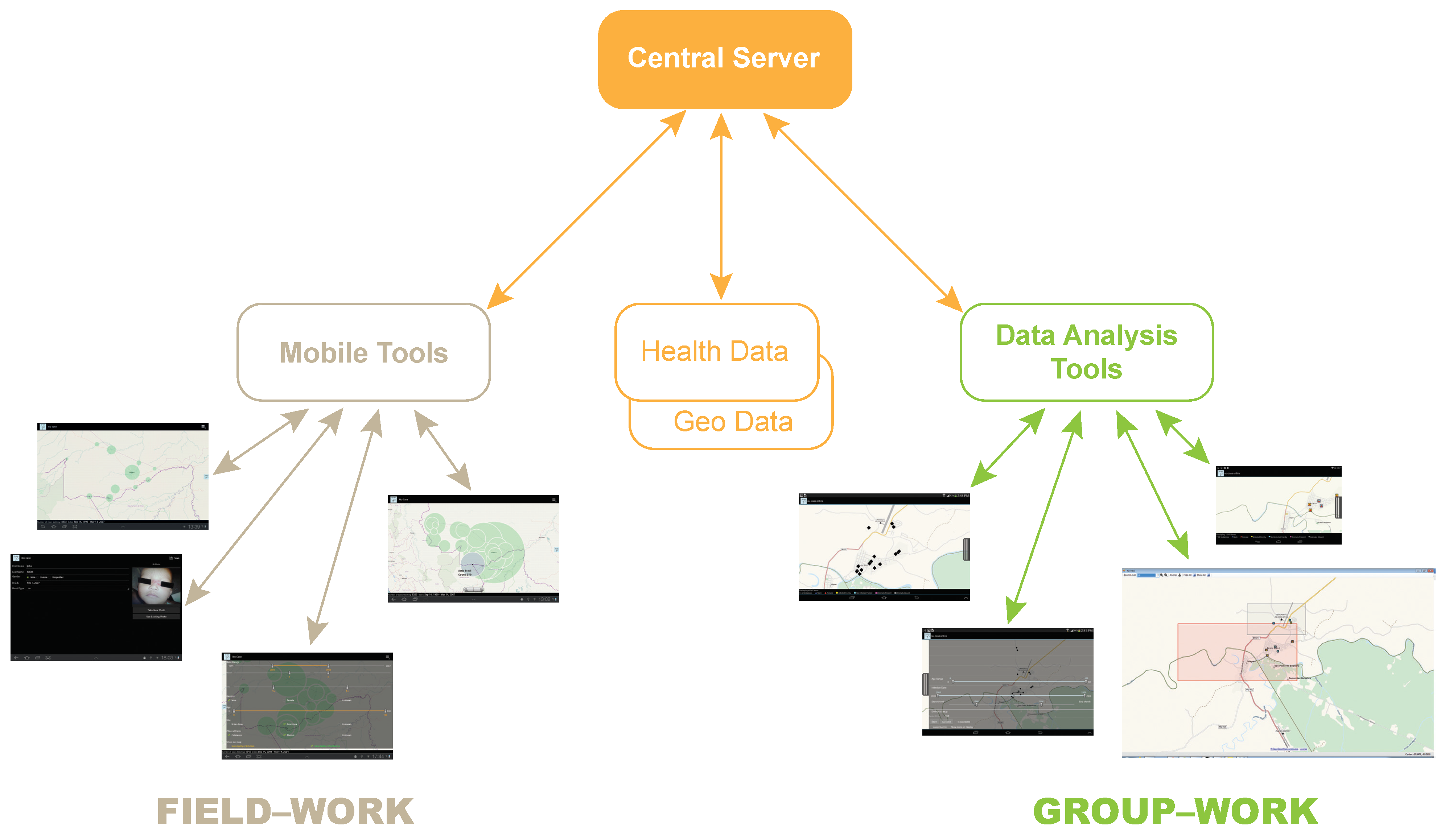
84])—but rather to focus on the role of interactive maps as the underlying framework for supporting the multidisciplinary team’s needs in relation to these tasks.
Figure 2 shows diagrammatic representation of this framework, depicting the relationships between its various components. The tools used for in-field data gathering and in-meeting data analysis all utilise interactive maps as part of their underlying framework.
5.1. Mobile Support for Fieldworkers
To support data collection by health fieldworkers, we developed a prototype designed for tablet devices which integrated collection of patient data, assistance for detection of Leishmaniasis and other infectious diseases, communication with medical specialists, and spatio-temporal visualisation of case reporting [
49]. The health fieldworkers for whom these tools were designed are local healthcare workers, mostly nurses and primary care doctors, but also community health agents. The latter are members of the local community who provide basic health services and play an important role in health promotion. They have limited training in healthcare, and this fact needed to be taken into account in the design of e-health support tools.
Collection of data was done through speech or touch input modalities, depending on the task. Support for the recording of GPS coordinates was also available, so that case incidence could be collected in a central server and later visualised in terms of temporal and spatial dimensions (see
Section 5.2, for instance). Patient data were initially stored on the device and then transferred to a server when the user came within range of internet connectivity. The system displayed case occurrence and distribution on a map of the region.
Figure 3 depicts the map-based interface of this interactive visualisation tool.
On this interactive map, the user could select to see clusters of Leishmaniasis cases by place of infection or notification, to help identify possible disparities between the project’s and official data collection and notification processes. Clusters of disease incidence are represented on the map by transparent circles whose diameters are proportional to the number of cases. The information presented on the map can be interactively explored through selection by the user of different date ranges as well as different combinations of health record variables, as shown in
Figure 4. Animation was employed to display case number progression over time—for different spatial parameters settings—to enable analysis of incidence and prevalence trends, and identification of disease spread patterns.
This interactive map-based data collection and visualisation tool was evaluated positively by different user groups involved in the project [
49]. A questionnaire administered to 47 participants (15 local doctors, 15 epidemiologists, 13 nurses, and 4 public health administrators) found that users were very positive in rating the system’s functionality on a 7-point Likert scale, specially in relation to recording geographical GPS data (mean 6.4, sd = 1.1), accessing patient record cases (6.3, sd = 1.1), and visualising geographical distribution of case data (6.6, sd = 0.8). Disease monitoring was ranked as the most important task supported by the interactive map-based system, followed by support for scientific research, and the recording and notification of cases.
As our user group consisted of health professionals with diverse profiles (nurses, primary care doctors, and community health agents), we gathered their opinions regarding the interactive system’s support for their tasks in different groups through a survey study. This study revealed scientific research and epidemiological surveillance to be closely related tasks that involve a number of sub-tasks. These encompassed data collection and access through networked mobile devices deployed in the region under investigation or surveillance. A map-based system in this case allowed effective coordination and integration of these sub-tasks.
5.2. Support for Collaborative Data Analysis
To support collaborative data analysis by researchers, we implemented a system that enabled map-based visualisation of epidemiological data on a large display with which users could interact through their personal mobile tablet devices, so as to be able to share specific data and their own analyses with the group [
50].
Visual communication and interaction at meetings through sharing of data on large displays is typical of multidisciplinary medical teamwork. In this particular setting, the team consisted of epidemiologists, health service researchers, and ecologists conducting research on Leishmaniasis and Bartonellosis. Leishmaniasis is endemic in the Brazilian state of Acre. While Bartonellosis is not known to occur in this region, it is endemic to the neighbouring regions in Peru and Bolivia. The research team had expertise in both of these diseases and were interested in finding out whether climatic, demographic, and land-use changes undergone by the region would favour the spread of Bartonellosis to these new areas. Teamwork in such settings typically involves presentation and discussion of evidence from several sources by members of the team. A shared display usually helps focus the presentations, establish common ground, and record the information under discussion [
41]. Thus, while our first use case focused on map-based interaction for data collection and epidemiological modelling in a distributed setting where communication was mostly asynchronous, this second use case focused on synchronous, co-located collaboration within a multidisciplinary team [
50].
The system supported coupled and decoupled modes of interaction across an ensemble consisting of a large shared display and several individual mobile device screens. Coupled interactions—involving networked use of large and small displays at the same time—took place around group visualisations, while decoupled interactions took place on private small device displays. Map views displayed on the mobile devices could be shared on the large display for visualisation by the whole team. Thus, the system allowed shifting between visual analysis by individual team members on their personal interactive maps and shared activities carried out together on a group visualisation display. The use of interactive maps as the common basis for both the shared and personal visualisations aimed to facilitate a seamless transition between these coupled and decoupled modes of interaction.
Figure 5 shows examples of these coupled group (top) and decoupled individual (bottom) modes of interaction, simultaneously on a tablet device and a large computer display. Individual analysts were able to share map-based information—such as information resulting from their visual analysis in decoupled interaction mode—on the shared large display in support of coupled group interactions. The screenshots on the left (top and bottom) show a single variable (presence of peri-domestic animals in the vicinity of patients’ dwellings) represented as black square icons. The images on the right (top and bottom) show combinations of several variables specifying details of records which are displayed on another area of the shared visualisation. Each variable (e.g., sex, whether family members have been infected, etc.) is represented by a different icon, which are combined and placed on the map. Records outwith the areas selected or being viewed by individual analysts remain invisible on the group visualisation. Visualisations shared with the group by individual collaborators appear on the shared map as individual overlays, displaying their personal view ports, records select for sharing, different levels of detail, and other configuration parameters. Personal views are identified on the large screen as semi-transparent rectangular regions, with their geometries varying according to the screen size, resolution, and magnification of the mobile devices connected to the large shared screen.
Our observations of multidisciplinary meetings prior to the development of the system revealed that most disciplines made use of maps to explain data presented during their meetings. This pattern was most prominent for epidemiologists, who presented statistical data—through a wall projector and presentation software—and made frequent references to maps by alternating between slides. Although analyses of patient records were often presented, these presentations were not adequately supported by maps. Adequate support would have required preparation of the maps ahead of the meetings. Lack of proper support for this task forced the presenters to rely on textual tables and verbal references to geographical regions under discussion, confining geographic information exchanges to verbal explanations. Different data sets were shared in the meetings, including statistics for disease incidence and prevalence, geographical distribution of cases, data on the utilisation of local health services, health policy documents shown for purposes of strategic planning, assessment of interventions and identification of candidate areas for future interventions.
Following the initial experience of interacting with our prototype system, users suggested many possible enhancements. These suggestions included using the large screen for collaborative creation of tables, sharing of geo-referenced photographs, support for integration of overlays and data from external sources (e.g., demographic details for visible or selected geographical regions), and support for annotating the visualisation shown on the large display by individual team members using their mobile devices for the purpose of recording meeting decisions and outcomes. While there were many such valuable suggestions for improvements, it is interesting to note that the existing map-based interactive visualisation would still remain the basis for supporting almost all of these other tasks as well.
6. Conclusions
In this article, we have reviewed the application of interactive maps to support complex analytical tasks in epidemiology and public health, as well as emerging technology, resources, and standards that have enabled interactive map-based applications to be built and deployed in large scale by major public health bodies.
We have highlighted some of the challenges that application developers face in this area and illustrated ways in which we have tackled some of these challenges in practice by describing two example cases for which we have previously designed map-based interactive visualisation tools. These tools have been deployed as part of a project aimed at supporting the work of a multidisciplinary team conducting research on disease surveillance in remote regions and investigating environmental, sociogeographic, and health factors that affect the spread of infectious diseases. Furthermore, we have reported the feedback received from a multidisciplinary group of researchers, healthcare professionals, and public health managers who regularly make use of maps in their work, elucidating the roles interactive maps might play in supporting their diverse range of activities. By linking theoretical and practical perspectives on interactive maps—in particular the challenges of integrating temporal and spatial aspects of geovisualisation—to concrete cases of epidemiology research work, this article contributes towards establishing an analytical framework for geographical and environmental factors affecting the spread of infectious diseases.
Based on our extensive review, as well as our own in-field experience reported here, we would argue that interactive maps can play a crucial role as an underlying basis for development of tools and technologies that could be used for the analysis of environmental and geographical factors affecting the spread of infectious diseases. In fact, our work suggests that emerging epidemiological modelling paradigms such as agent-based modelling can benefit from interactive maps by allowing tighter integration between data collection in the field and epidemiological surveillance, providing novel tools which could contribute to the early detection of outbreaks and ultimately to the prevention of pandemics.
However, we would also note that while much progress has been made towards integrating spatial and temporal aspects of epidemiological work into effective map-based interfaces, research is still much needed on issues relating to a range of challenges faced by multidisciplinary teams working in this area. These challenges include, for instance, spatial data granularity, temporal consistency, privacy, integration of data from diverse sources, adequacy of the underlying epidemiological models used to provide predictions, and improved support for causal inference using interactive maps.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}