
COVID-19: Evaluation of Fever Clinic and Fever Sentinel Configuration—A Case Study of Harbin, China

Abstract
:1. Introduction
2. Inequality in Healthcare Services of Fever Clinics and Fever Sentinels
2.1. COVID-19 Exacerbates Inequities in Healthcare Accessibility
2.2. The Spatial Structure of China’s Large Cities Affects the Layout of Healthcare Facilities and the Accessibility of Fever Clinics
2.3. The Dual Rural–Urban System in China and the Construction of COVID-19 Fever Clinics
2.4. The Lag in the Construction of New Urban Areas, Planning Patterns, and Inequalities in Accessibility of COVID-19 Fever Clinics
2.5. The Maintenance and Control Measures of the Emergency Medical Facilities Need to Be Improved
3. Materials and Methods
3.1. Research Scope and Hierarchical Assessment Framework
3.1.1. Study Area
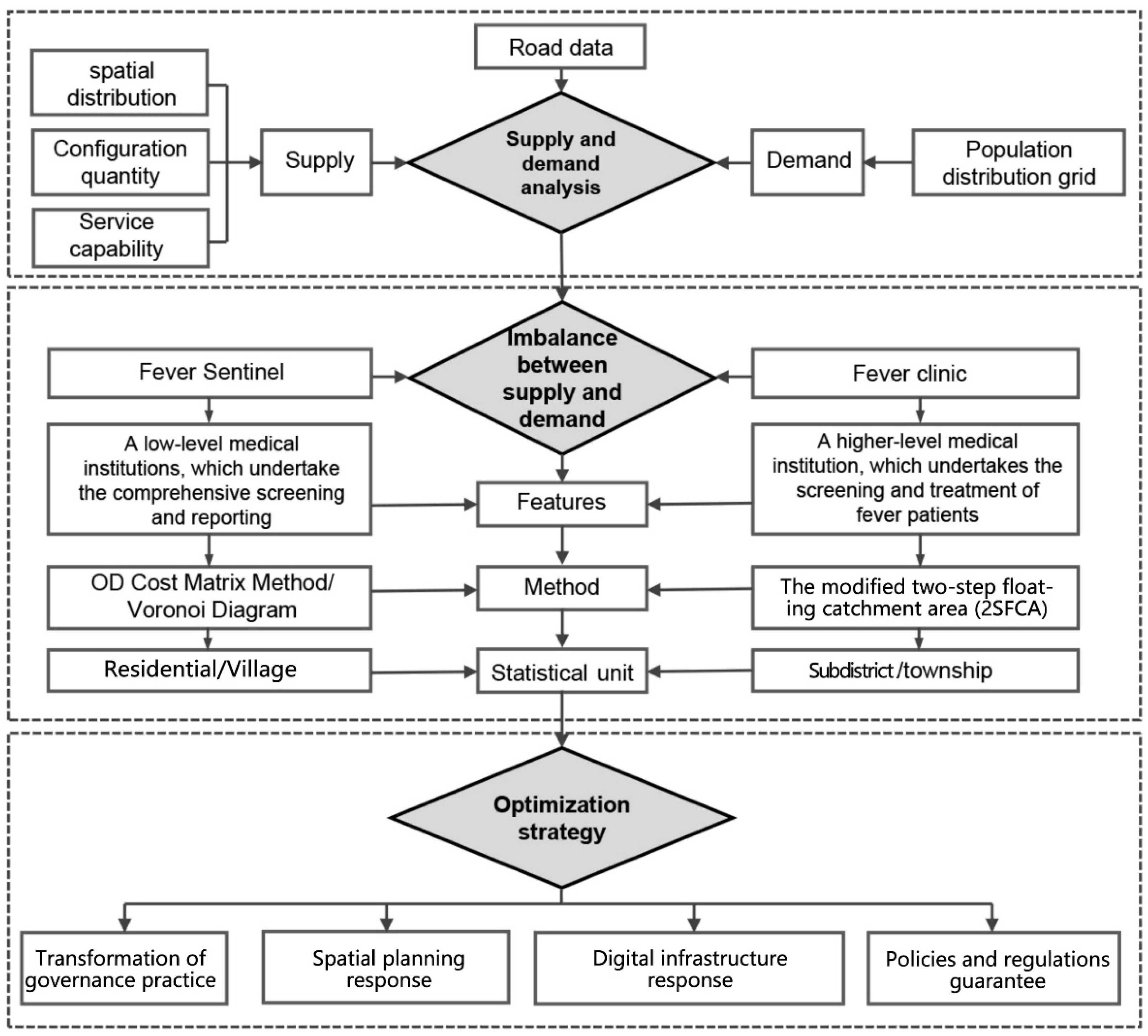
3.1.2. Assessment Framework Construction
3.2. Data
3.3. Methods
3.3.1. Kernel Density Analysis
3.3.2. The Modified Two-Step Floating Catchment Area (2SFCA) Method
3.3.3. OD Cost Matrix Method
3.3.4. Voronoi Diagram Method
4. Results
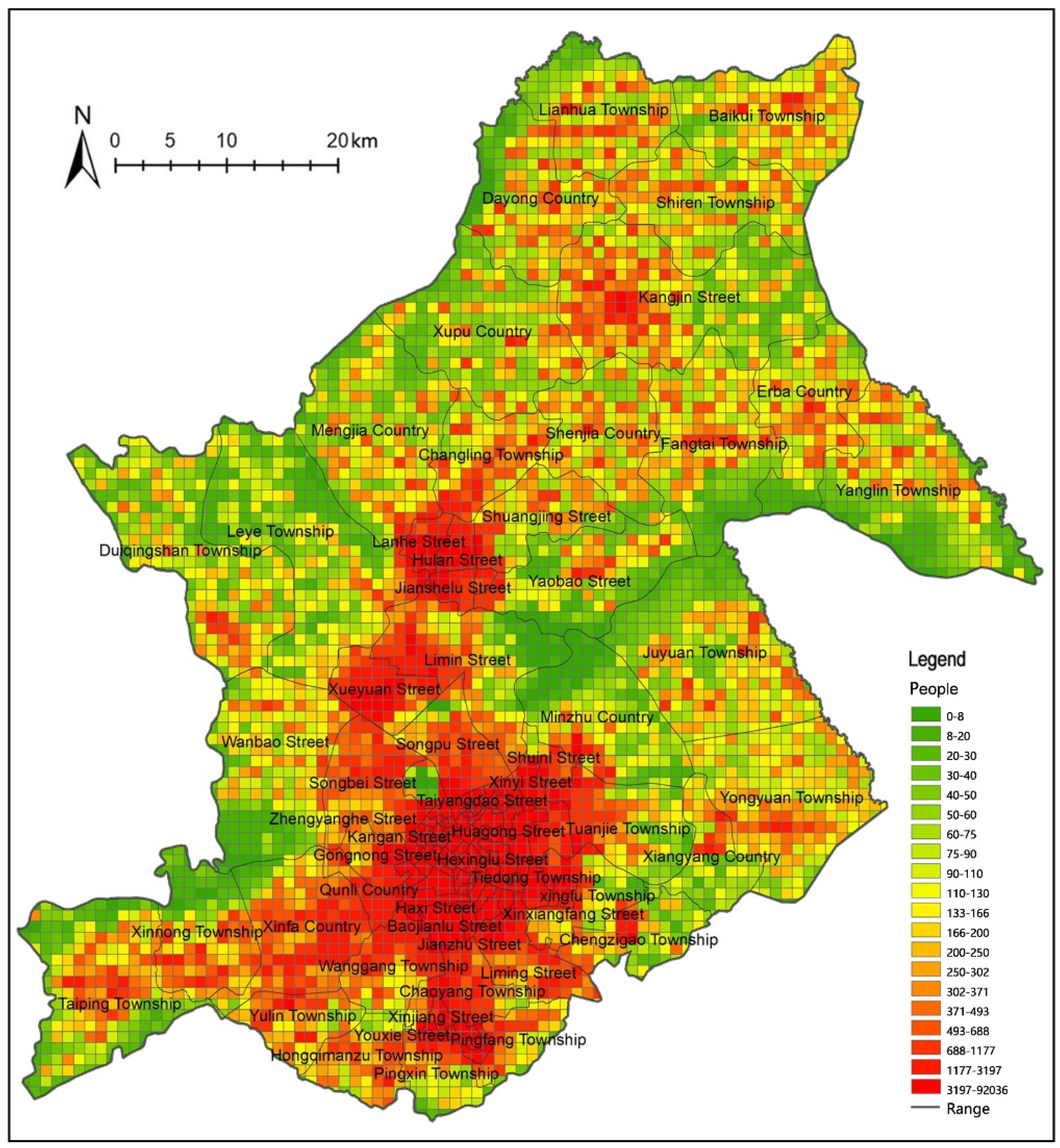
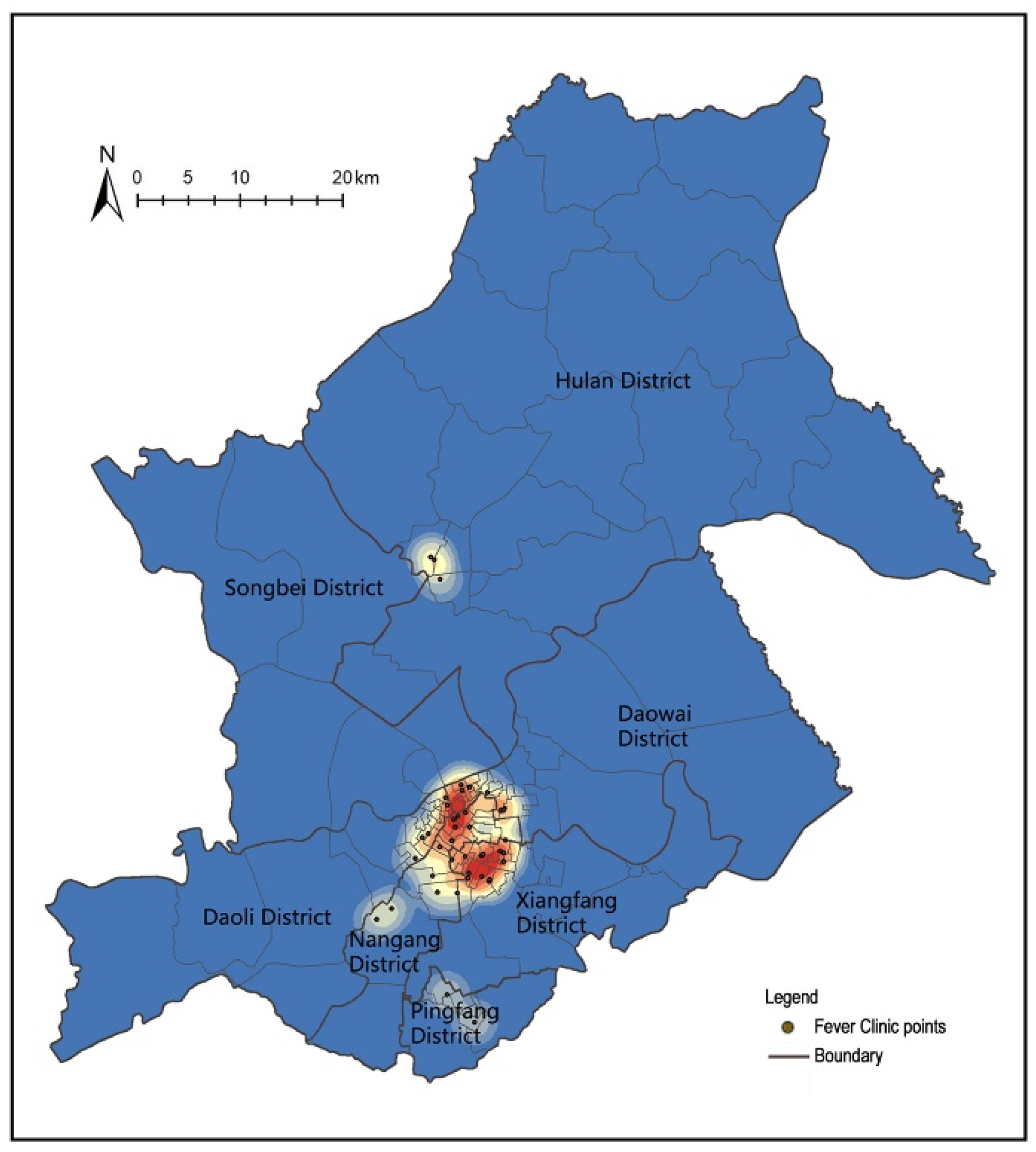
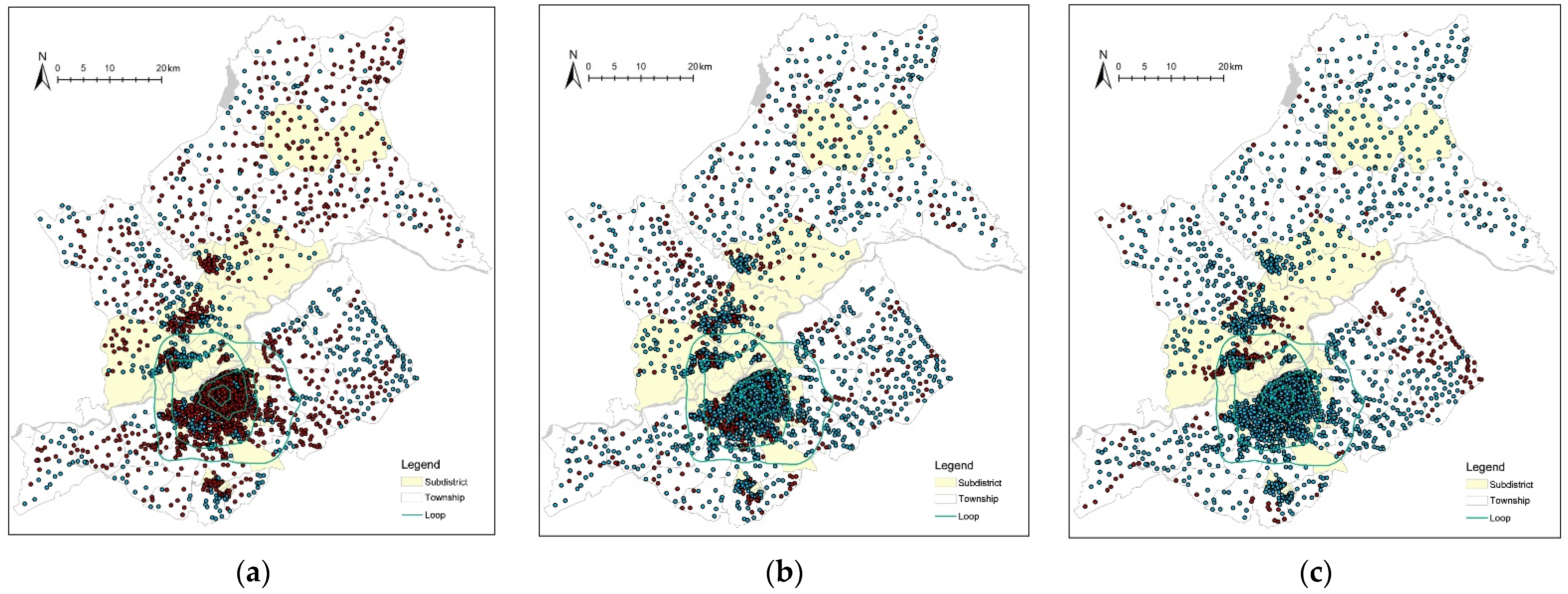
4.1. Spatial Distribution Characteristics of Fever Clinics and Fever Sentinels
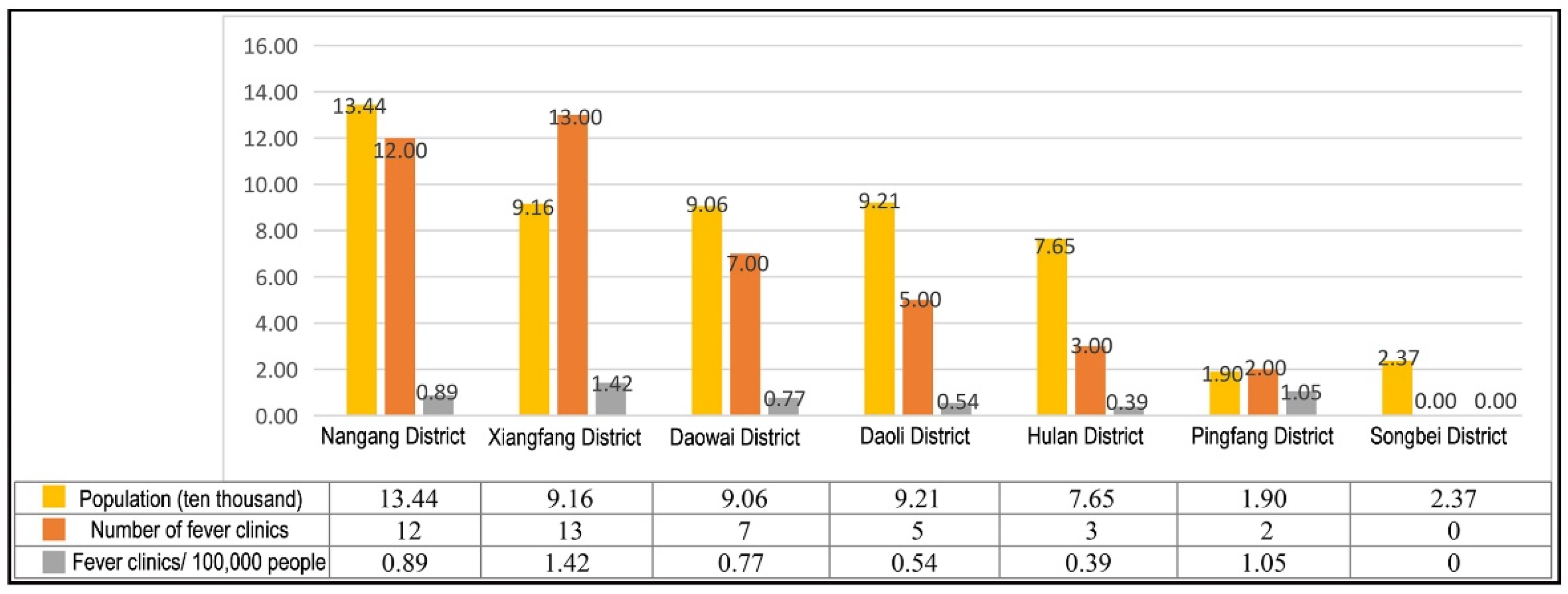
4.2. Characteristics of the Numbers of Fever Clinics and Allocated Fever Sentinel Sites
4.3. Analysis of the Accessibility of Fever Clinics
4.3.1. Choice of Research Methodology
4.3.2. Fever Clinic Accessibility Results
4.4. Fever Sentinel Accessibility and Service Pressure Analysis
4.4.1. The Accessibility of Fever Sentinels
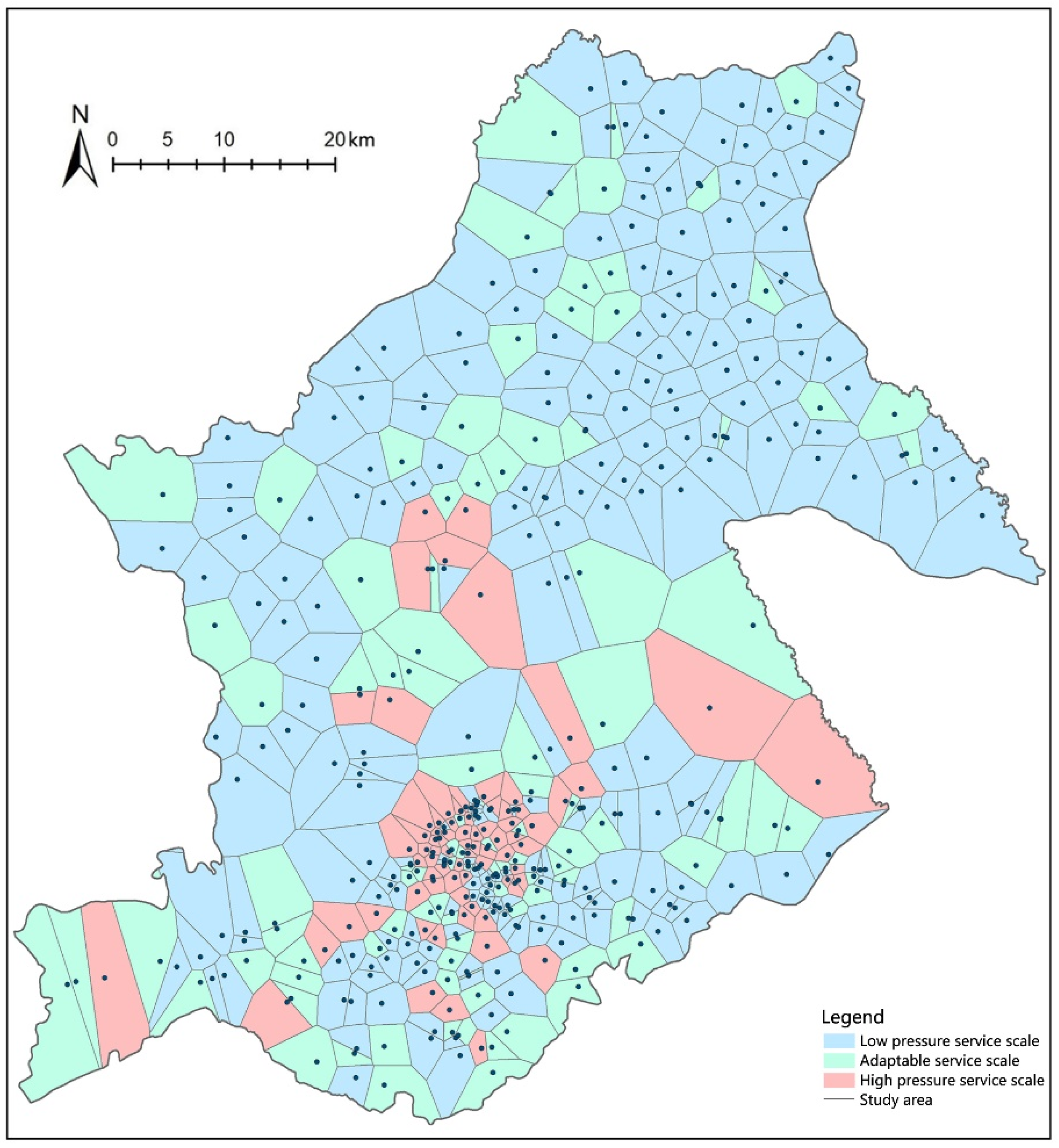
4.4.2. Fever Sentinel Service Pressure Analysis
5. Discussion and Proposals
5.1. The History of Urban–Rural Development and Inequalities in Medical COVID-19 Monitoring Institutions
5.2. Reconstruction of the Spatial Planning and Governance System for Urban Fever Clinics and Fever Sentinels
5.2.1. Transformation of Governance Practice: Response to Public Health Emergencies under the Concept of “Peacetime and Epidemic Combination”
5.2.2. Spatial Planning Response: Layout of Fever Clinics and Fever Sentinels for Health Equity
5.2.3. Digital Infrastructure Response: Building a Smart COVID-19 Epidemic Prevention Technology System
5.2.4. Policies and Regulations Guarantee: Improving the Medical Prevention and Control Mechanism and Emergency Measures in Public Health
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sara, R.; Morgan, H.; Rebecca, M.; Casoni, M. How the trump administration’s pandemic health care response failed racial health equity: Case studies of structural racism and a call for equity mindfulness in federal health policy making. J. Health Politics Policy Law 2021, 46, 761–783. [Google Scholar] [CrossRef]
- Abedi, V.; Olulana, O.; Avula, V.; Chaudhary, D.; Khan, A.; Shahjouei, S.; Li, J.; Zand, R. Racial, economic, and health inequality and COVID-19 infection in the United States. J. Racial Ethn. Health Disparities 2020, 8, 732–742. [Google Scholar] [CrossRef] [PubMed]
- Azar, K.M.J.; Shen, Z.; Romanelli, R.J.; Lockhart, S.H.; Smits, K.; Robinson, S.; Brown, S.; Pressman, A.R. Disparities in outcomes among COVID-19 patients in a large health care system in California. Health Aff. 2020, 39, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Unmasking and Overcoming Health Inequities in Urban Settings; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Corburn, J. Urban place and health equity: Critical issues and practices. Int. J. Environ. Res. Public Health 2017, 14, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michael, M. Medical care, social determinants of health, and health Equity. World Med. Health Policy 2018, 10, 195–197. [Google Scholar] [CrossRef]
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.A.J.; Taylor, S. Closing the gap in a generation: Health equity through action on the social determinants of health. The Lancet. 2008, 372, 1661–1669. [Google Scholar] [CrossRef]
- Paterson, I.; Judge, K. Equality of Access to Healthcare; Routledge: London, UK, 2002. [Google Scholar]
- Why is the “Shanghai program” of fever clinic recommended for national study. Healthy China Obs. 2020, 6, 59.
- Nayan, N.; Kumar, M.K.; Nair, R.K.; Manral, I.; Kapoor, R. Clinical triaging in cough clinic alleviates COVID-19 overload in emergency department in India. SN Compr. Clin. Med. 2021, 3, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; He, Q.; Shen, T.; Wu, Z.; Tan, M.; Chen, Y.; Weng, Q.; Nie, L.; Zhang, H.; Zheng, B. “An integrated system, three separated responsibilities”, a new fever clinic management model, in prevention and control of novel coronavirus pneumonia. World J. Clin. Cases 2021, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, L.; Liu, Y.; Wu, L.; Lu, C.; Wang, W.; Zheng, X.; Wan, J.; Jin, Y.; Yu, W. Establishing quality evaluation system of nursing management in fever clinics: A delphi method. J. Nurs. Manag. 2021, 29, 2542–2556. [Google Scholar] [CrossRef]
- Jiang, H.; Liu, J.; Ren, N.; He, R.; Li, M.; Dong, Q. Emergency management in fever clinic during the outbreak of COVID-19: An experience from Zhuhai. Epidemiol. Infect. 2020, 148, e174. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.; Chen, Y.; Gao, Y.; Sun, P.; Chang, R.; Zhou, B.; Qiu, H.; Cheng, F. Mobile isolation wards in a fever clinic: A novel operation model during the COVID-19 pandemic. Epidemiol. Infect. 2021, 149, e61. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhou, H.; Wu, X.; Huang, W.; Jia, B. Strategies for qualified triage stations and fever clinics during the outbreak of COVID-2019 in the county hospitals of western Chongqing. J. Hosp. Infect. 2020, 105, 128–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfson, J.A.; Leung, C.W. An opportunity to emphasize equity, social determinants, and prevention in primary Care. Ann. Fam. Med. 2020, 18, 290–291. [Google Scholar] [CrossRef] [PubMed]
- Zafri, N.M.; Nurullah, M.; Neema, M.N.; Waliullah, M. Spatial accessibility to healthcare facilities in coastal region of Bangladesh. Int. J. Health Plan. Manag. 2021, 36, 643–655. [Google Scholar] [CrossRef]
- Brodar, K.E.; Hong, N.; Liddle, M.; Hernandez, L.; Waks, J.; Sanchez, J.; Delamater, A.; Davis, E. Transitioning to telehealth services in a pediatric diabetes clinic during COVID-19: An interdisciplinary quality improvement initiative. J. Clin. Psychol. Med. Settings 2021, 10, 1–12. [Google Scholar] [CrossRef]
- Wang, D.; Tian, Y.; Qian, Z.; Tang, Y. An analysis on spatial accessibility of fever clinics and designated hospitals in response to epidemic events of infectious diseases:A case study of Hunan province. Chin. J. Health Policy 2021, 14, 74–79. [Google Scholar] [CrossRef]
- Zhang, J.; Han, P.; Yang, L. Spatial accessibility of fever clinics for multi-tiered prevention and control on COVID-19 in Beijing. J. Peking Univ. Health Sci. 2021, 53, 543–548. [Google Scholar] [CrossRef]
- Yong, Q.; Liu, D.; Li, G.; Wu, W.; Sun, W.; Liu, S. Reducing exposure to COVID-19 by improving access to fever clinics: An empirical research of the Shenzhen area of China. BMC Health Serv. Res. 2021, 21, 959. [Google Scholar] [CrossRef]
- Song, Y.; Wu, Y. Research on the allocation of community health-care facilities in Shenzhen under the background of COVID-19 normalized prevention and control. Spec. Zone Econ. 2021, 3, 51–53. [Google Scholar]
- Kwan, M.P. Space-time and integral measures of individual accessibility: A comparative analysis using a point-based framework. Geogr. Anal. 1998, 30, 191–216. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, M.P.; Weber, J. Scale and accessibility: Implications for the analysis of land use-travel interaction. Appl. Geogr. 2008, 28, 110–123. [Google Scholar] [CrossRef]
- Zhan, Q.; Xi, W.; Sliuzas, R. A GIS-based method to assess the shortage areas of community health service—Case study in Wuhan, China. In Proceedings of the 2011 International Conference on Remote Sensing, Environment and Transportation Engineering, Nanjing, China, 24–26 June 2011; IEEE: Atlanta, GA, USA, 2011. [Google Scholar] [CrossRef]
- Haesen, S.; Rauch, A.; Elger, B.; Rost, M. Equivalence of care? Accessibility and availability of dialysis services for older prisoners in Switzerland. Int. J. Prison. Health 2021. ahead-of-print. [Google Scholar] [CrossRef]
- Hulland, E.N.; Wiens, K.E.; Shirude, S.; Morgan, J.D.; Pigott, D.M. Travel time to health facilities in areas of outbreak potential: Maps for guiding local preparedness and response. BMC Med. 2019, 17, 232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naghawi, H. Using geographic information system in analyzing hospital accessibility: A case study in New Orleans. Jordan J. Civ. Eng. 2012, 6, 353–360. [Google Scholar]
- Yang, Q.; Xu, J. An analysis model of public service facilities based on attraction accessibility. Planners 2015, 7, 96–101. [Google Scholar] [CrossRef]
- Wei, C.; Wheeler, K.K.; Huang, Y.; Lin, S.M.; Sui, D.Z.; Xiang, H. Evaluation of spatial accessibility to ohio trauma centers using a GIS-Based Gravity Model. Br. J. Med. Med. Res. 2015, 10, 1–10. [Google Scholar] [CrossRef]
- Tao, Z.; Yao, Z.; Kong, H.; Duan, F.; Li, G. Spatial accessibility to healthcare services in Shenzhen, China: Improving the multi-modal two-step floating catchment area method by estimating travel time via online map APIs. BMC Health Serv. Res. 2018, 18, 345. [Google Scholar] [CrossRef] [Green Version]
- Jin, M.; Liu, L.; Tong, D.; Gong, Y.; Liu, Y. Evaluating the Spatial accessibility and distribution balance of multi-level medical service facilities. Int. J. Environ. Res. Public Health 2019, 16, 1150. [Google Scholar] [CrossRef] [Green Version]
- Neng, W.; Bin, Z.; Troy, S. A three-step floating catchment area method for analyzing spatial access to health services. Int. J. Geogr. Inf. Sci. 2012, 26, 1073–1089. [Google Scholar] [CrossRef]
- Wei, L.; Yi, Q. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef]
- Liang, X.; Ma, R.; Cheng, Y.; Gong, Q.; Li, J.; Zhu, B. The Right to Accessible COVID-19 Testing in the Post-Epidemic Period under the Urban–Rural Integration: Haishu District, Ningbo City, China. Sustainability 2022, 14, 1636. [Google Scholar] [CrossRef]
- Kanuganti, S.; Sarkar, A.K.; Singh, A.P. Quantifying accessibility to health care using two-step floating catchment area method (2SFCA): A case study in rajasthan. Transp. Res. Procedia 2016, 17, 391–399. [Google Scholar] [CrossRef]
- Henning-Smith, C.; Hernandez, A.; Lahr, M.; Kozhimannil, K. Rural-Urban Differences in Access to, Attitudes Toward, and Satisfaction with Care Among Medicare Beneficiaries. Health Serv. Res. 2020, 55, 20–21. [Google Scholar] [CrossRef]
- Booysen, F.; Gordon, T. Trends and socio-economic inequality in public perceptions of healthcare delivery in South Africa. Int. J. Qual. Health Care 2020, 32, 135–139. [Google Scholar] [CrossRef]
- Strauss, P.; Winter, S.; Waters, Z.; Toussaint, D.W.; Watson, V.; Lin, A. Perspectives of trans and gender diverse young people accessing primary care and gender-affirming medical services: Findings from Trans Pathways. Int. J. Transgender Health 2022, 23, 295–307. [Google Scholar] [CrossRef]
- Smith, J.A. Reflections on the framing of ‘health equity’ in the Nationa l Primary Health Care Strategic Framework: A cause for celebration or concern? Health Promot. J. Aust. 2014, 25, 42–45. [Google Scholar] [CrossRef]
- Okonkwo, N.E.; Aguwa, U.T.; Jang, M.; Barré, I.A.; Page, K.R.; Sullivan, P.S.; Beyrer, C.; Baral, S. COVID-19 and the US response: Accelerating health inequities. BMJ Evid. Based Med. 2020, 26, 176–179. [Google Scholar] [CrossRef]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef]
- Solnica, A.; Barski, L.; Jotkowitz, A. Allocation of scarce resources during the COVID-19 pandemic: A Jewish ethical perspective. J. Med. Ethics 2020, 46, 444–446. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Liu, Y.; Zhao, J.; Li, G. Urban total factor productivity: Does urban spatial structure matter in China? Sustainability 2019, 12, 214. [Google Scholar] [CrossRef] [Green Version]
- Cavallo, R.; Komossa, S.; Marzot, N.; Pont, M.B.; Kuijper, J. (Eds.) The Inevitable Spatial Blend: Infrastructures and City: Between New and Old Urban Configurations; IOS Press: Amsterdam, The Netherlands, 2014; pp. 387–392. [Google Scholar] [CrossRef]
- Si, Z.; Ying, Z. Research on the spatial layout of medical facilities in Beijing from the perspective of international comparative. City Plan. Rev. 2020, 44, 47–54, 89. [Google Scholar] [CrossRef]
- Luo, B.; Xia, W.; Wei, Q.; Zhang, Q. Rethink Profoundly on the Special Planning of Urban Medical and Health Facilities Under the Background of COVID-19: An Empirical Analysis of Wuhan. Mod. Urban Res. 2020, 10, 2–11. [Google Scholar] [CrossRef]
- Chen, Y.; Song, J.; Lin, X. Nanjing Urban-rural Medical Facilities Planning. Planners 2013, 29, 83–88. [Google Scholar] [CrossRef]
- Ma, C.; Song, Z.; Zong, Q. Urban-rural inequality of opportunity in health care: Evidence from China. Int. J. Environ. Res. Public Health 2021, 18, 7792. [Google Scholar] [CrossRef]
- Liu, P.; Guo, W.; Liu, H.; Hua, W.; Xiong, L. The integration of urban and rural medical insurance to reduce the rural medical burden in China: A case study of a county in Baoji City. BMC Health Serv. Res. 2018, 18, 796. [Google Scholar] [CrossRef] [Green Version]
- Melvin, S.C.; Wiggins, C.; Burse, N.; Thompson, E.; Monger, M. The role of public health in COVID-19 emergency response efforts from a rural health perspective. Prev. Chronic Dis. 2020, 17, E70. [Google Scholar] [CrossRef]
- Wagner, T.; Ramirez, C.; Godoy, B. Covid-19 rural health inequities: Insights from a real-world scenario. J. Commun. Healthc. 2022, 15, 22–26. [Google Scholar] [CrossRef]
- Silver, A. Could rural China’s healthcare deal with COVID-19? BMJ 2021, 375, n2759. [Google Scholar] [CrossRef]
- Yang, Z.; Zhu, X.; Moodie, D. Optimization of land use in a new urban district. J. Urban Plan. Dev. 2014, 141, 05014010. [Google Scholar] [CrossRef]
- Zhuang, L.; Ye, C. Disorder or reorder? The spatial production of state-level new areas in China. Sustainability 2018, 10, 3628. [Google Scholar] [CrossRef] [Green Version]
- He, Y. Reflections on the COVID-19 pandemic: A perspective from China. Aust. Soc. Work. 2021, 74, 519–520. [Google Scholar] [CrossRef]
- Wei, Y.; Sha, F.; Zhao, Y.; Jiang, Q.; Hao, Y.; Chen, F. Better modelling of infectious diseases: Lessons from COVID-19 in China. BMJ 2021, 375, n2365. [Google Scholar] [CrossRef]
- People’s Government of Heilongjiang Province. Harbin Announced 72 Fever Clinics. Available online: https://www.hlj.gov.cn/n200/2020/0123/c43-10918604.html (accessed on 28 January 2020).
- Boots, B.N. Weighting Thiessen Polygons. In Economic Geography; Taylor & Francis, Ltd.: Abingdon, UK, 2016; Volume 56, pp. 248–259. [Google Scholar] [CrossRef]
- Liu, L.; Wang, L. A study on spatial distribution of fever clinics in Shanghai during the epidemic of COVID-19 pneumonia. Shanghai Urban Plan. Rev. 2020, 2, 87–93, 98. [Google Scholar]
- Liu, J.; Zhu, Q. Research of equalizing layout of public service facilities: Take health facilities of central six districts of Beijing for example. Urban Dev. Stud. 2016, 23, 6–11. [Google Scholar] [CrossRef]
- Health Commission of Anhui Province. Anhui: Redrawing the “Runway” for Township Health Centers. Available online: http://wjw.ah.gov.cn/public/7001/56213701.html (accessed on 13 July 2021).
- Department of Planning, Development and Information Technology. Statistical Bulletin of China’s Health Development in 2020. Available online: http://www.nhc.gov.cn/guihuaxxs/s10743/202107/af8a9c98453c4d9593e07895ae0493c8.shtml (accessed on 13 July 2021).
- Chen, J. Research on the layout and development direction of medical institutions in Beijing core area and Tongzhou District. Beijing Plan. Rev. 2019, 6, 95–98. [Google Scholar]
- Chen, Q.; Qi, Y. Discussion on spatial strategy of medical institutions in Guangzhou. In Space Governance for High-Quality Development—Proceedings of the 2020 China Urban Planning Annual Conference (17 Detailed Planning); Urban Planning Society of China: Beijing, China, 2021; pp. 277–282. [Google Scholar] [CrossRef]
- An, P.; Xu, Z.; Li, L. Exploration of the development of the medical system under the guidance of resilient cities—Take the state-level new area of Tianfu new area in Sichuan province as an example. In Space Governance for High Quality Development 2021 China Urban Planning Annual Conference (01 Urban Safety and Disaster Prevention Planning); Urban Planning Society of China: Beijing, China, 2021; pp. 434–445. [Google Scholar] [CrossRef]
- Pal, D.; Ghosh, D.; Santra, P.K.; Mahapatra, G.S. Mathematical analysis of a COVID-19 epidemic model by using data driven epidemiological parameters of diseases spread in India. Biophysics 2022, 67, 231–244. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nangang | Xiangfang | Daowai | Daoli | Hulan | Pingfang | Songbei | |||
|---|---|---|---|---|---|---|---|---|---|
| Subdistrict/township | Number of subdistrict | 18 | 20 | 23 | 19 | 8 | 6 | 5 | |
| Number of township | 2 | 4 | 4 | 4 | 11 | 2 | 2 | ||
| Residential/village | Number of residential | 587 | 388 | 250 | 349 | 188 | 66 | 149 | |
| Number of village | 31 | 101 | 217 | 97 | 463 | 21 | 169 | ||
| Fever clinic | Total number | 12 | 13 | 7 | 5 | 3 | 2 | 0 | |
| Bed | 24710 | 9940 | 4693 | 4118 | 1900 | 1360 | 0 | ||
| Fever Sentinel | City Sentinel | Community Health Service Center | 19 | 20 | 17 | 20 | 8 | 6 | 4 |
| Community Health Service Stations | 16 | 21 | 9 | 4 | 5 | 1 | 3 | ||
| Rural Sentinel | Township Hospital | 2 | 3 | 5 | 3 | 11 | 1 | 4 | |
| Village Clinic | 17 | 39 | 19 | 21 | 120 | 2 | 18 | ||
| Nangang | Xiangfang | Daowai | Daoli | Hulan | Pingfang | Songbei | |||
|---|---|---|---|---|---|---|---|---|---|
| The average number of fever sentinel points | Subdistrict sentinel | Average number of community health service centers | 1.06 | 1.00 | 0.74 | 1.05 | 1.00 | 1.00 | 0.80 |
| Average number of community health service stations | 0.89 | 1.05 | 0.39 | 0.21 | 0.63 | 0.17 | 0.60 | ||
| Township Sentinel | Average number of township hospitals | 1.00 | 0.75 | 1.25 | 0.75 | 1.00 | 0.50 | 2.00 | |
| Average number of village clinics (statistics by administrative village) | 0.65 | 0.40 | 0.09 | 0.21 | 0.25 | 0.09 | 0.11 | ||
| Road Level | Highway | Main Road | Secondary Road | Branch Road |
|---|---|---|---|---|
| Speed (km/h) | 60 | 40 | 30 | 20 |
| Reachable Level | Class I | Class II | Class III | Class IV | Class V |
|---|---|---|---|---|---|
| Reachability value (sheets per 100 people) | 0.0000–0.1245 | 0.1246–0.3649 | 0.3650–0.6093 | 0.6094–0.8571 | 0.8572–1.0951 |
| Class of Accessiblity Area | Accessiblity Value Per 100 People | Total Number and Percentage of Accessibility at All Levels in the Study Area | The Number of Accessible Levels in the Seven Districts | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total Number | Percentage (%) | Pingfang | Nangang | Xiangfang | Daowai | Daoli | Hulan | Songbei | ||
| Level I | 0.00–0.12 | 17 | 13.28 | 0 | 0 | 0 | 2 | 2 | 10 | 2 |
| Level II | 0.12–0.36 | 9 | 7.03 | 0 | 1 | 1 | 1 | 1 | 4 | 2 |
| Level III | 0.36–0.61 | 9 | 7.03 | 2 | 0 | 1 | 0 | 1 | 5 | 0 |
| Level IV | 0.61–0.86 | 15 | 11.72 | 6 | 1 | 4 | 2 | 0 | 0 | 3 |
| Level V | 0.86–1.10 | 78 | 60.94 | 0 | 18 | 18 | 22 | 19 | 0 | 0 |
| Best Travel Distance | Acceptable Travel Distance | More than Expected Distance | |
|---|---|---|---|
| Subdistrict sentinel | 0–1500 m | 1500–3000 m | >3000 m |
| Township sentinel | 0–3000 m | 3000–5000 m | >5000 m |
| Administrative District | Community Health Service Center | Community Health Service Stations | Township Hospital | Village Clinic |
|---|---|---|---|---|
| Low pressure service scale | <25,000 people | <12,500 people | <25,000 people | <5000 people |
| Adaptable service scale | 25,000–30,000 people | 12,500–25,000 people | 25,000–30,000 people | 5000–10,000 people |
| High pressure service scale | >30,000 people | >25,000 people | >30,000 people | >10,000 people |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, D.; Wu, Q.; Feng, Y.; Wu, S. COVID-19: Evaluation of Fever Clinic and Fever Sentinel Configuration—A Case Study of Harbin, China. Sustainability 2022, 14, 9117. https://doi.org/10.3390/su14159117
Xu D, Wu Q, Feng Y, Wu S. COVID-19: Evaluation of Fever Clinic and Fever Sentinel Configuration—A Case Study of Harbin, China. Sustainability. 2022; 14(15):9117. https://doi.org/10.3390/su14159117
Chicago/Turabian StyleXu, Daming, Qian Wu, Yingkun Feng, and Songtao Wu. 2022. "COVID-19: Evaluation of Fever Clinic and Fever Sentinel Configuration—A Case Study of Harbin, China" Sustainability 14, no. 15: 9117. https://doi.org/10.3390/su14159117
APA StyleXu, D., Wu, Q., Feng, Y., & Wu, S. (2022). COVID-19: Evaluation of Fever Clinic and Fever Sentinel Configuration—A Case Study of Harbin, China. Sustainability, 14(15), 9117. https://doi.org/10.3390/su14159117