
Resilient Built Environment: Critical Review of the Strategies Released by the Sustainability Rating Systems in Response to the COVID-19 Pandemic




Abstract
:1. Introduction
- Contact.
- Droplets.
- Aerosols.
2. Aim and Purpose
- Elimination: physical removal of the hazard.
- Substitution: replace the hazard.
- Engineering controls: isolate people from the hazard.
- Administrative controls: change the way people work.
- PPE: protect the workers with personal protective equipment [44].
- Any lack within the strategies developed by the Sustainability Rating Systems specifically to minimize the transmission of infectious diseases.
- The level of sustainability of the above-mentioned strategies addressed in response to the COVID-19 pandemic.
3. Methodology
3.1. Publications
3.2. Scope of Application
- Internationally applicable (not country-specific).
- Voluntary (standards and codes are excluded).
- Focused on buildings in operation with a defined fit-out.
- Referred to mechanical ventilated workspaces.
3.3. Degree of Sustainability
3.4. Extents and Limitations
4. Results
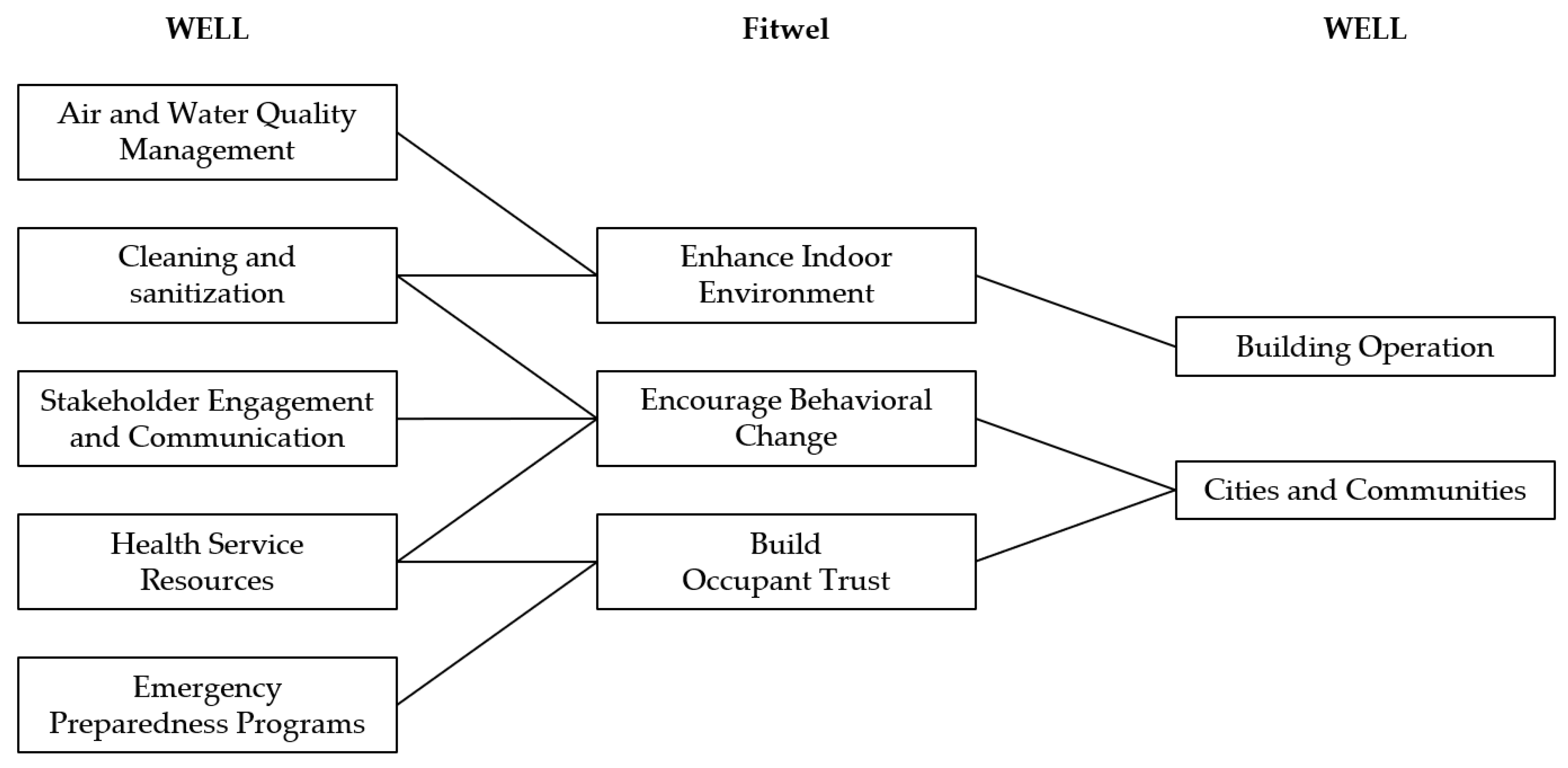
4.1. WELL Health-Safety Rating
- Cleaning and Sanitization Procedures.
- Emergency Preparedness Programs.
- Health Service Resources.
- Air and Water Quality Management.
- Stakeholder Engagement and Communication.
- Innovation [65].
4.2. Fitwel Viral Response Module
- Enhance Indoor Environments.
- Encourage Behavioral Change.
- Build Occupant Trust [66].
4.3. LEED Safety First Pilot Credits
4.4. Other Sustainability Rating Systems
4.5. Comparison of the Strategies
5. Discussion
6. Conclusions
- Company policies show a higher environmental and economic sustainability compared to the strategies directly related to the built environment because they are preventive rather than corrective measures.
- The measures addressed by WELL, Fitwel and LEED are similar even though the structure of the SRS is different.
- The SRS promote a weak sustainability approach that accepts that economic development can reduce natural capitals.
- The Criteria of the SRS are only compared with benchmark values whose aggregated level of assessment does not allow to map different choices.
- There is a general lack of analytical strategies that address occupancy rates and physical distancing, whose importance is shown in the latest research where the airborne transmission stands out as the main route of infection.
- Fitwel lacks in considering the implications of food and vaccines.
- WELL does not consistently address Personal Protective Equipment.
- LEED is the less solid with only 6 strategies.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wagner, E.K. Basic Virology; Blackwell Science: Malden, MA, USA, 1999; ISBN 978-0-632-06109-9. [Google Scholar]
- Yin, Y.; Wunderink, R.G. MERS, SARS and Other Coronaviruses as Causes of Pneumonia. Respirology 2017, 23, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Hui, D.S.; Azhar, E.I.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; Mchugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The Continuing 2019-NCoV Epidemic Threat of Novel Coronaviruses to Global Health—The Latest 2019 Novel Coronavirus Outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Nie, J.; Li, Q.; Wu, J.; Zhao, C.; Hao, H.; Liu, H.; Zhang, L.; Nie, L.; Qin, H.; Wang, M.; et al. Establishment and Validation of a Pseudovirus Neutralization Assay for SARS-CoV-2. Emerg. Microbes Infect. 2020, 9, 680–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.-R.; Cao, Q.-D.; Hong, Z.-S.; Tan, Y.-Y.; Chen, S.-D.; Jin, H.-J.; Tan, K.-S.; Wang, D.-Y.; Yan, Y. The Origin, Transmission and Clinical Therapies on Coronavirus Disease 2019 (COVID-19) Outbreak—An Update on the Status. Mil. Med Res. 2020, 7, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilder-Smith, A.; Chiew, C.J.; Lee, V.J. Can We Contain the COVID-19 Outbreak with the Same Measures as for SARS? Lancet Infect. Dis. 2020, 20, e102–e107. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Ni, W.; Wang, Z.; Ma, G.; Pan, B.; Dong, L.; Gao, R.; Jiang, F. The Distribution of SARS-CoV-2 Contamination on the Environmental Surfaces during Incubation Period of COVID-19 Patients. Ecotoxicol. Environ. Saf. 2021, 208, 111438. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Morawska, L. Could Fighting Airborne Transmission Be the next Line of Defence against COVID-19 Spread? City Environ. Interact. 2019, 4, 100033. [Google Scholar] [CrossRef] [PubMed]
- Adam, D. A Guide to R—The Pandemic’s Misunderstood Metric. Nature 2020, 583, 346–348. [Google Scholar] [CrossRef]
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and Influenza Pandemics. Lancet Infect. Dis. 2020, 20, e238–e244. [Google Scholar] [CrossRef]
- Harding, A.; Lanese, N. The 12 Deadliest Viruses on Earth. Available online: https://www.livescience.com/56598-deadliest-viruses-on-earth.html (accessed on 12 December 2020).
- Zhang, M.Q.; Wang, X.H.; Chen, Y.L.; Zhao, K.L.; Cai, Y.Q.; An, C.L.; Lin, M.G.; Mu, X.D. Clinical features of 2019 novel coronavirus pneumonia in the early stage from a fever clinic in Beijing. Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, E013. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Cannizzaro, E.; Ramaci, T.; Cirrincione, L.; Plescia, F. Work-Related Stress, Physio-Pathological Mechanisms, and the Influence of Environmental Genetic Factors. Int. J. Environ. Res. Public Health 2019, 16, 4031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannizzaro, E.; Plescia, F.; Cirrincione, L.; Lo Pinto, E.; Plescia, F. Sport for Job. Differences in Cortisol Levels in a Water Polo Team at Different Times of Workout. EuroMediterr. Biomed. J. 2018, 13, 181–184. [Google Scholar] [CrossRef]
- Cannizzaro, E.; Cirrincione, L.; Mazzucco, W.; Scorciapino, A.; Catalano, C.; Ramaci, T.; Ledda, C.; Plescia, F. Night-Time Shift Work and Related Stress Responses: A Study on Security Guards. Int. J. Environ. Res. Public Health 2020, 17, 562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singhal, T. A Review of Coronavirus Disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Novel Coronavirus (2019-NCoV): Situation Report; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Rastogi, P.; Sobek, O.N.; Jephson, G.; Allison, J. A Data-Driven Indoor Air Quality Framework for Post-COVID-19 Workplace Re-Entry: Summary for Policymakers; arbnco Ltd.: Glasgow, UK, 2020. [Google Scholar]
- The Society of Heating, Air-Conditioning and Sanitary Engineers of Japan (SHASE); Architectural Institute of Japan (AIJ). Role of Ventilation in the Control of the COVID-19 Infection: Emergency Presidential Discourse; AIJ: Tokyo, Japan, 2020. [Google Scholar]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission Routes of 2019-NCoV and Controls in Dental Practice. Int. J. Oral Sci. 2020, 12, 1–6. [Google Scholar] [CrossRef]
- Bennett, D.H.; McKone, T.E.; Evans, J.S.; Nazaroff, W.W.; Margni, M.D.; Jolliet, O.; Smith, K.R. Defining Intake Fraction. Environ. Sci. Technol. 2002, 36, 207A–211A. [Google Scholar] [CrossRef] [Green Version]
- Tellier, R.; Li, Y.; Cowling, B.J.; Tang, J.W. Recognition of Aerosol Transmission of Infectious Agents: A Commentary. BMC Infect. Dis. 2019, 19, 101. [Google Scholar] [CrossRef]
- Baron, P. Generation and Behavior of Airborne Particles (Aerosols); Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA, 2020.
- Sun, C.; Zhai, Z. The Efficacy of Social Distance and Ventilation Effectiveness in Preventing COVID-19 Transmission. Sustain. Cities Soc. 2020, 62, 102390. [Google Scholar] [CrossRef] [PubMed]
- Coleman, K.K.; Nguyen, T.T.; Yadana, S.; Hansen-Estruch, C.; Lindsley, W.G.; Gray, G.C. Bioaerosol Sampling for Respiratory Viruses in Singapore’s Mass Rapid Transit Network. Sci. Rep. 2018, 8, 17476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishiura, H.; Oshitani, H.; Kobayashi, T.; Saito, T.; Sunagawa, T.; Matsui, T.; Wakita, T.; MHLW COVID-19 Response Team; Suzuki, M. Closed Environments Facilitate Secondary Transmission of Coronavirus Disease 2019 (COVID-19). medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, M.D.; Luís, N.C. COVID-19 Could Leverage a Sustainable Built Environment. Sustainability 2020, 12, 5863. [Google Scholar] [CrossRef]
- BRE Global Limited. Encouraging Resilient Assets Using BREEAM. BREEAM Resources. Watford, UK, 2020, 10. Available online: https://files.bregroup.com/breeam/BREEAM_Resilience_BRE_115440.pdf (accessed on 4 October 2021).
- Cazzolla Gatti, R. Coronavirus Outbreak Is a Symptom of Gaia’s Sickness. Ecol. Model. 2020, 426, 109075. [Google Scholar] [CrossRef]
- M’ikanatha, N.M. The Pandemic Century: One Hundred Years of Panic, Hysteria and Hubris. Emerg. Infect. Dis. J. 2020, 26, 450. [Google Scholar] [CrossRef]
- Bruun, C. The Water Supply of Ancient Rome. A Study of Roman Imperial Administration. Soc. Sci. Fenn. 1991, 10, 456. [Google Scholar]
- Lilley, K.D. Urban Planning after the Black Death: Townscape Transformation in Later Medieval England (1350–1530). Urban Hist. 2015, 42, 22–42. [Google Scholar] [CrossRef]
- Jordan, D.P. Transforming Paris: The Life and Labors of Baron Haussmann; University of Chicago Press: Chicago, IL, USA, 1996; ISBN 978-0-226-41038-8. [Google Scholar]
- Kirkland, S. Paris Reborn: Napoléon III, Baron Haussmann, and the Quest to Build a Modern City; St. Martin’s Press: New York, NY, USA, 2013; ISBN 978-0-312-62689-1. [Google Scholar]
- Adams, A.; Schwartzman, K.; Theodore, D. Collapse and Expand: Architecture and Tuberculosis Therapy in Montreal, 1909, 1933, 1954. Technol. Cult. 2010, 49, 908–942. [Google Scholar] [CrossRef]
- Campbell, M. What Tuberculosis Did for Modernism: The Influence of a Curative Environment on Modernist Design and Architecture. Med. Hist. 2005, 49, 463–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Megahed, N.A.; Ghoneim, E.M. Antivirus-Built Environment: Lessons Learned from Covid-19 Pandemic. Sustain. Cities Soc. 2020, 61, 102350. [Google Scholar] [CrossRef]
- Reyes, R.; Ahn, R.; Thurber, K.; Burke, T.F. Urbanization and Infectious Diseases: General Principles, Historical Perspectives, and Contemporary Challenges. In Challenges in Infectious Diseases; Fong, I.W., Ed.; Emerging Infectious Diseases of the 21st Century; Springer: New York, NY, USA, 2013; pp. 123–146. ISBN 978-1-4614-4496-1. [Google Scholar]
- Ott, M.; Shaw, S.F.; Danila, R.N.; Lynfield, R. Lessons Learned from the 1918-1919 Influenza Pandemic in Minneapolis and St. Paul, Minnesota. Public Health Rep. 2007, 122, 803–810. [Google Scholar] [CrossRef]
- Baldwin, A.N. Sars and the Built Environment in Hong Kong. In Proceedings of the Institution of Civil Engineers—Municipal Engineer; Thomas Telford Ltd.: London, UK, 2006; Volume 159, pp. 37–42. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, (CDC). Hierarchy of Controls | NIOSH | CDC. Available online: https://www.cdc.gov/niosh/topics/hierarchy/default.html (accessed on 12 December 2020).
- Berardi, U. Sustainability Assessment of Urban Communities through Rating Systems. Environ. Dev. Sustain. 2013, 15, 1573–1591. [Google Scholar] [CrossRef]
- Wen, B.; Musa, N.; Onn, C.C.; Ramesh, S.; Liang, L.; Wang, W. Evolution of Sustainability in Global Green Building Rating Tools. J. Clean. Prod. 2020, 259, 120912. [Google Scholar] [CrossRef]
- McArthur, J.J.; Powell, C. Health and Wellness in Commercial Buildings: Systematic Review of Sustainable Building Rating Systems and Alignment with Contemporary Research. Build. Environ. 2020, 171, 106635. [Google Scholar] [CrossRef]
- International WELL Building Institute. Strategies from the WELL Building Standard to Support in the Fight against COVID-19; IWBI: New York, NY, USA, 2020. [Google Scholar]
- Devuyst, D. Linking Impact Assessment and Sustainable Development at the Local Level: The Introduction of Sustainability Assessment Systems. Sustain. Dev. 2000, 8, 67–78. [Google Scholar] [CrossRef]
- Building Research Establishment. Building Back Better with BREEAM: Supporting the Green Recovery; BRE Global Limited: Watford, UK, 2020. [Google Scholar]
- RESET Standard. RESET Indexes for Airborne Viral Transmission. Available online: https://www.reset.build/resources/indexes (accessed on 31 January 2021).
- International WELL Building Institute. WELL Building Standard. Available online: https://www.wellcertified.com/ (accessed on 2 January 2021).
- U.S. Green Building Council USGBC. Releases New LEED Guidance to Address COVID-19 and Support Buildings with Reopening Strategies. Available online: https://www.usgbc.org/articles/usgbc-releases-new-leed-guidance-address-covid-19-and-support-buildings-reopening (accessed on 28 August 2021).
- Center for Active Design Fitwel. Available online: https://www.fitwel.org/ (accessed on 6 January 2021).
- Qian, H.; Miao, T.; Liu, L.; Zheng, X.; Luo, D.; Li, Y. Indoor Transmission of SARS-CoV-2. Indoor Air 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.; De Smet, A.; Langstaff, M.; Ravid, D. What Employees Are Saying about the Future of Remote Work; McKinsey & Company: Houston, TX, USA, 2021. [Google Scholar]
- D’Alessandro, D.; Gola, M.; Appolloni, L.; Dettori, M.; Fara, G.M.; Rebecchi, A.; Settimo, G.; Capolongo, S. COVID-19 and Living Space Challenge. Well-Being and Public Health Recommendations for a Healthy, Safe, and Sustainable Housing. Acta Bio Med. 2020, 91, 61–75. [Google Scholar] [CrossRef]
- Tokazhanov, G.; Tleuken, A.; Guney, M.; Turkyilmaz, A.; Karaca, F. How Is COVID-19 Experience Transforming Sustainability Requirements of Residential Buildings? A Review. Sustainability 2020, 12, 8732. [Google Scholar] [CrossRef]
- Spennemann, D. Residential Architecture in a Post-Pandemic World: Implications of COVID-19 for New Construction and for Adapting Heritage Buildings. J. Green Build. 2021, 16, 199–215. [Google Scholar] [CrossRef]
- Kaklauskas, A.; Lepkova, N.; Raslanas, S.; Vetloviene, I.; Milevicius, V.; Sepliakov, J. COVID-19 and Green Housing: A Review of Relevant Literature. Energies 2021, 14, 2072. [Google Scholar] [CrossRef]
- World Commission on Environment and Development. Our Common Future; Oxford University Press: Oxford, UK; New York, NY, USA, 1987; ISBN 978-0-19-282080-8. [Google Scholar]
- Nilsen, H.R. The Joint Discourse ‘Reflexive Sustainable Development’—From Weak towards Strong Sustainable Development. Ecol. Econ. 2010, 69, 495–501. [Google Scholar] [CrossRef]
- Pelenc, J.; Ballet, J. Strong Sustainability, Critical Natural Capital and the Capability Approach. Ecol. Econ. 2015, 112, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Zugravu-Soilita, N.; Kafrouni, R.; Bouard, S.; Apithy, L. Do Cultural Capital and Social Capital Matter for Economic Performance? An Empirical Investigation of Tribal Agriculture in New Caledonia. Ecol. Econ. 2021, 182, 106933. [Google Scholar] [CrossRef]
- International WELL Building Institute. WELL Health-Safety Rating for Facility Operations and Maintenance; IWBI: New York, NY, USA, 2020. [Google Scholar]
- Center for Active Design. Fitwel Viral Response Module: Reference Guide; Center for Active Design: New York, NY, USA, 2020. [Google Scholar]
- U.S. Green Building Council. LEED Reference Guide for Building Operations and Maintenance, v4 ed.; U.S. Green Building Council: Washington, DC, USA, 2013; ISBN 978-1-932444-20-9. [Google Scholar]
- U.S. Green Building Council. COVID-19 Resources. Available online: https://www.usgbc.org/about/covid-19-resources (accessed on 10 January 2021).
- GIGA: Performance-Driven ESG Data for Real-Estate. Certification for Health & Regeneration Focused on Indoor Air Quality. RESET Standard. Québec, Canada 2017. Available online: https://reset.build/download/RESET_Standard_v2_0_prerelease_170312.pdf (accessed on 4 October 2021).
- Bourdic, L.; Salat, S. Building Energy Models and Assessment Systems at the District and City Scales: A Review. Build. Res. Inf. 2012, 40, 518–526. [Google Scholar] [CrossRef]
- Mori, K.; Christodoulou, A. Review of Sustainability Indices and Indicators: Towards a New City Sustainability Index (CSI). Environ. Impact Assess. Rev. 2012, 32, 94–106. [Google Scholar] [CrossRef]
- U.S. Green Building Council. LEED Project Profiles. Available online: https://www.usgbc.org/projects (accessed on 29 August 2021).
- Filippini, T.; Rothman, K.J.; Cocchio, S.; Narne, E.; Mantoan, D.; Saia, M.; Goffi, A.; Ferrari, F.; Maffeis, G.; Orsini, N.; et al. Associations between Mortality from COVID-19 in Two Italian Regions and Outdoor Air Pollution as Assessed through Tropospheric Nitrogen Dioxide. Sci. Total Environ. 2020, 760, 143355. [Google Scholar] [CrossRef]
- Huang, G.; Brown, P.E. Population-Weighted Exposure to Air Pollution and COVID-19 Incidence in Germany. Spat. Stat. 2021, 41, 100480. [Google Scholar] [CrossRef] [PubMed]
- Liang, D.; Shi, L.; Zhao, J.; Liu, P.; Sarnat, J.A.; Gao, S.; Schwartz, J.; Liu, Y.; Ebelt, S.T.; Scovronick, N.; et al. Urban Air Pollution May Enhance COVID-19 Case-Fatality and Mortality Rates in the United States. Innovation 2020, 1, 100047. [Google Scholar] [CrossRef]
- Razzaq, A.; Sharif, A.; Aziz, N.; Irfan, M.; Jermsittiparsert, K. Asymmetric Link between Environmental Pollution and COVID-19 in the Top Ten Affected States of US: A Novel Estimations from Quantile-on-Quantile Approach. Environ. Res. 2020, 191, 110189. [Google Scholar] [CrossRef]
- Travaglio, M.; Yu, Y.; Popovic, R.; Selley, L.; Leal, N.S.; Martins, L.M. Links between Air Pollution and COVID-19 in England. Environ. Pollut. 2021, 268, 115859. [Google Scholar] [CrossRef] [PubMed]
- Konstantinoudis, G.; Padellini, T.; Bennett, J.; Davies, B.; Ezzati, M.; Blangiardo, M. Long-Term Exposure to Air-Pollution and COVID-19 Mortality in England: A Hierarchical Spatial Analysis. Environ. Int. 2021, 146, 106316. [Google Scholar] [CrossRef] [PubMed]
- López-Feldman, A.; Heres, D.; Marquez-Padilla, F. Air Pollution Exposure and COVID-19: A Look at Mortality in Mexico City Using Individual-Level Data. Sci. Total Environ. 2021, 756, 143929. [Google Scholar] [CrossRef] [PubMed]
- Stewart, E.J.; Schoen, L.J.; Mead, K.; Olmsted, R.N.; Sekhar, C.; Vernon, W.; Pantelic, J.; Li, Y.; Sultan, Z.M.; Conlan, W. ASHRAE Position Document on Infectious Aerosols; ASHRAE: Atlanta, GA, USA, 2020. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Epidemiological Disease | Period | Measures on the Built Environment |
|---|---|---|
| Infectious diseases | 2nd century | Aqueducts, water and sanitation systems [34]. |
| Black Death/ Bubonic Plague | 14th century | Larger public spaces with more organized layouts [35]. |
| Cholera | 19th century | Sanitation of sewage systems to stop fecal–oral transmission route [36,37]. |
| Tuberculosis/ White Plague | 19th century | Modern minimal design with terraces, balconies and flat roofs to capture sunlight and air [38,39] and reject dust, pollution and diseases [40]. |
| Spanish Flu | 20th century | Social distancing and gauze masks [41,42]. |
| SARS-CoV-1 | 21st century | Taking people’s temperatures [8] and improved ventilation and drainage systems [43]. |
| Degree of Sustainability | Environmental Sustainability | Economic Sustainability |
|---|---|---|
| Low | The impact on the environment is consistent as regards the use of natural resources (materials, water, energy, etc.) | The capex needed to implement the strategy is consistent and characterized by a payback longer than the lifecycle of the building |
| Medium | The impact on the environment is comparable to similar buildings | The return on investment (ROI) of the strategy implemented is typically less than a decade |
| High | The impact of the strategy on the environment is negligible | The cost needed to implement the strategy can be easily put in the operating budget of the building in use (opex) |
| Rating System | Strategy | Scope | Category | Sustainability | |
|---|---|---|---|---|---|
| Environment | Economic | ||||
| WELL | Support Handwashing | Cleaning and sanitization | Built Environment | High | High |
| WELL | Reduce Surface Contact | Cleaning and sanitization | Built Environment | High | Medium |
| WELL | Improve Cleaning Practices | Cleaning and sanitization | Built Environment | High | High |
| WELL | Select Preferred Cleaning Products | Cleaning and sanitization | Built Environment | High | Medium |
| WELL | Reduce Respiratory Particle Exposure | Cleaning and sanitization | Built Environment | High | Medium |
| WELL | Develop Emergency Preparedness Plan | Emergency Preparedness Programs | Built Environment | High | High |
| WELL | Create Business Continuity Plan | Emergency Preparedness Programs | Company Policy | High | High |
| WELL | Plan for Healthy Re-Entry | Emergency Preparedness Programs | Company Policy | High | High |
| WELL | Provide Emergency Resources | Emergency Preparedness Programs | Company Policy | High | High |
| WELL | Bolster Emergency Resilience | Emergency Preparedness Programs | Company Policy | High | High |
| WELL | Provide Sick Leave | Health Service Resources | Company Policy | High | Medium |
| WELL | Provide Health Benefits | Health Service Resources | Company Policy | High | Medium |
| WELL | Support Mental Health Recovery | Health Service Resources | Company Policy | High | Medium |
| WELL | Promote Flu Vaccines | Health Service Resources | Company Policy | High | Medium |
| WELL | Promote a Smoke-Free Environment | Health Service Resources | Company Policy | High | High |
| WELL | Assess Ventilation | Air and Water Quality Management | Built Environment | Medium | Low |
| WELL | Assess and Maintain Air Treatment Systems | Air and Water Quality Management | Built Environment | High | Low |
| WELL | Develop Legionella Management Plan | Air and Water Quality Management | Built Environment | High | Medium |
| WELL | Monitor Air and Water Quality | Air and Water Quality Management | Built Environment | High | High |
| WELL | Manage Mold and Moisture | Air and Water Quality Management | Built Environment | High | High |
| WELL | Promote Health and Wellness | Stakeholder Engagement and Communication | Company Policy | High | High |
| WELL | Share Food Inspection Information | Stakeholder Engagement and Communication | Company Policy | High | High |
| Fitwel | Enhanced Indoor Air Quality Policy | Enhance Indoor Environment | Built Environment | Medium | Low |
| Fitwel | Humidity Control Policy | Enhance Indoor Environment | Built Environment | Medium | Medium |
| Fitwel | Enhanced Indoor Air Quality Testing and Monitoring Protocol | Enhance Indoor Environment | Built Environment | High | Low |
| Fitwel | Legionella Water Management Plan | Enhance Indoor Environment | Built Environment | High | Medium |
| Fitwel | Enhanced Cleaning, Disinfecting, and Maintenance Protocol | Enhance Indoor Environment | Built Environment | High | High |
| Fitwel | Enhanced Green Purchasing Policy | Enhance Indoor Environment | Built Environment | High | Medium |
| Fitwel | Surface Hygiene Stations | Encourage Behavioral Change | Built Environment | High | Medium |
| Fitwel | Personal Protective Equipment (PPE) Guidelines | Encourage Behavioral Change | Company Policy | High | High |
| Fitwel | Personal Protective Equipment (PPE) Provision Plan | Encourage Behavioral Change | Company Policy | High | Medium |
| Fitwel | Hand Hygiene | Encourage Behavioral Change | Company Policy | High | Medium |
| Fitwel | Health Promotion Signage | Encourage Behavioral Change | Company Policy | High | High |
| Fitwel | Specialized Health Programming and Services Plan | Encourage Behavioral Change | Company Policy | High | Medium |
| Fitwel | Social Support Groups | Encourage Behavioral Change | Company Policy | High | High |
| Fitwel | Contagious Disease Outbreak Preparedness Plan | Build Occupant Trust | Company Policy | High | High |
| Fitwel | Business Continuity | Build Occupant Trust | Company Policy | High | High |
| Fitwel | Mental Health First Aid | Build Occupant Trust | Company Policy | High | High |
| Fitwel | Viral Response Design Guidelines | Build Occupant Trust | Company Policy | High | High |
| Fitwel | Enhanced Stakeholder Collaboration Plan | Build Occupant Trust | Company Policy | High | High |
| Fitwel | Communication Plan | Build Occupant Trust | Company Policy | High | High |
| Fitwel | Paid Sick Leave Policy | Build Occupant Trust | Company Policy | High | High |
| Fitwel | Family Support Policy | Build Occupant Trust | Company Policy | High | High |
| LEED | Re-Enter Your Workspace | Building Operation | Built Environment | High | Medium |
| LEED | Cleaning and Disinfecting Your Space | Building Operation | Built Environment | High | Medium |
| LEED | Managing Indoor Air Quality during COVID-19 | Building Operation | Built Environment | Medium | Low |
| LEED | Building Water System Recommissioning | Building Operation | Built Environment | High | Medium |
| LEED | Pandemic Planning | Cities and Communities | Company Policy | High | High |
| LEED | Social Equity in Pandemic Planning | Cities and Communities | Company Policy | High | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marotta, A.; Porras-Amores, C.; Rodríguez Sánchez, A. Resilient Built Environment: Critical Review of the Strategies Released by the Sustainability Rating Systems in Response to the COVID-19 Pandemic. Sustainability 2021, 13, 11164. https://doi.org/10.3390/su132011164
Marotta A, Porras-Amores C, Rodríguez Sánchez A. Resilient Built Environment: Critical Review of the Strategies Released by the Sustainability Rating Systems in Response to the COVID-19 Pandemic. Sustainability. 2021; 13(20):11164. https://doi.org/10.3390/su132011164
Chicago/Turabian StyleMarotta, Antonio, César Porras-Amores, and Antonio Rodríguez Sánchez. 2021. "Resilient Built Environment: Critical Review of the Strategies Released by the Sustainability Rating Systems in Response to the COVID-19 Pandemic" Sustainability 13, no. 20: 11164. https://doi.org/10.3390/su132011164
APA StyleMarotta, A., Porras-Amores, C., & Rodríguez Sánchez, A. (2021). Resilient Built Environment: Critical Review of the Strategies Released by the Sustainability Rating Systems in Response to the COVID-19 Pandemic. Sustainability, 13(20), 11164. https://doi.org/10.3390/su132011164