
Identifying Health Care Environment Contradictions in Terms of Infection Control during a Pandemic with a Focus on Health Workers’ Experience


Abstract
:1. Introduction
2. Related Work
2.1. Design Attributes and Infection Control
2.2. Operation Strategies and Infection Control
3. Materials and Methods
4. Identified Problems
4.1. Space Configuration for the Hospitalization of Patients
4.1.1. Poor Isolation of the Infectious Ward
4.1.2. Improper or Absence of Spatial Isolation of Patients with COVID-19 from Others
“Unfortunately, due to limited space and facilities, patients with COVID-19 and non-COVID patients are in the same place, and only some beds for patients with COVID-19 have been isolated by a plastic cover”.
4.1.3. Long Distance between Essential Parts
“The long-distance between some related wards makes us walk a lot every day. This is frustrating. There is a possibility of contaminating different wards of the hospital”.
4.2. Layout and Circulation of the Environment
4.2.1. Problems with the Main Entrance/Shared Entrance for the CT Scan and Lung Screening and the Inadequacy of Facilities
“The medical staff and patients and escorts have to enter the hospital from the same door, and apart from them, the staff has to take off their masks in the crowded entrance during the exit and entrance to be recognized.”
“Unfortunately, there is just one door for patients and health workers. We cannot distinguish the patients from their appearance until the doctor examines them and sees if they are suffering from COVID-19. To go to the doctor’s room, they have to use the entrance used by others and sit beside others, and the only thing that is being practiced is wearing masks.”
“A separate entrance door is allocated to pregnant women.”
“There are several side entrances to the hospital, but the lack of attention to proper signposts results in overcrowding in the main entrance.”
“This hospital is designed for treating cardiovascular patients. Though we treat lung patients, this hospital is not specifically designed for lung patients. The admission of a large number of patients with COVID-19 has posed a serious challenge to the hospital in recent months.”
4.2.2. Problems of the Emergency Department and Waiting Rooms
“Unfortunately, in the emergency section, all the patients are placed together until they are examined and referred to the relevant section. There are patients with COVID-19 and heart disease, etc.”
“Yes, fortunately, we have one special room for COVID patients. The protocols have been followed in this regard, the tests are performed in a special room within the emergency section.”
“The waiting room is not suitable for hospitalization and admission of patients with COVID-19 because the waiting room is small, there is no natural ventilation, and the necessary distance cannot be observed at all.”
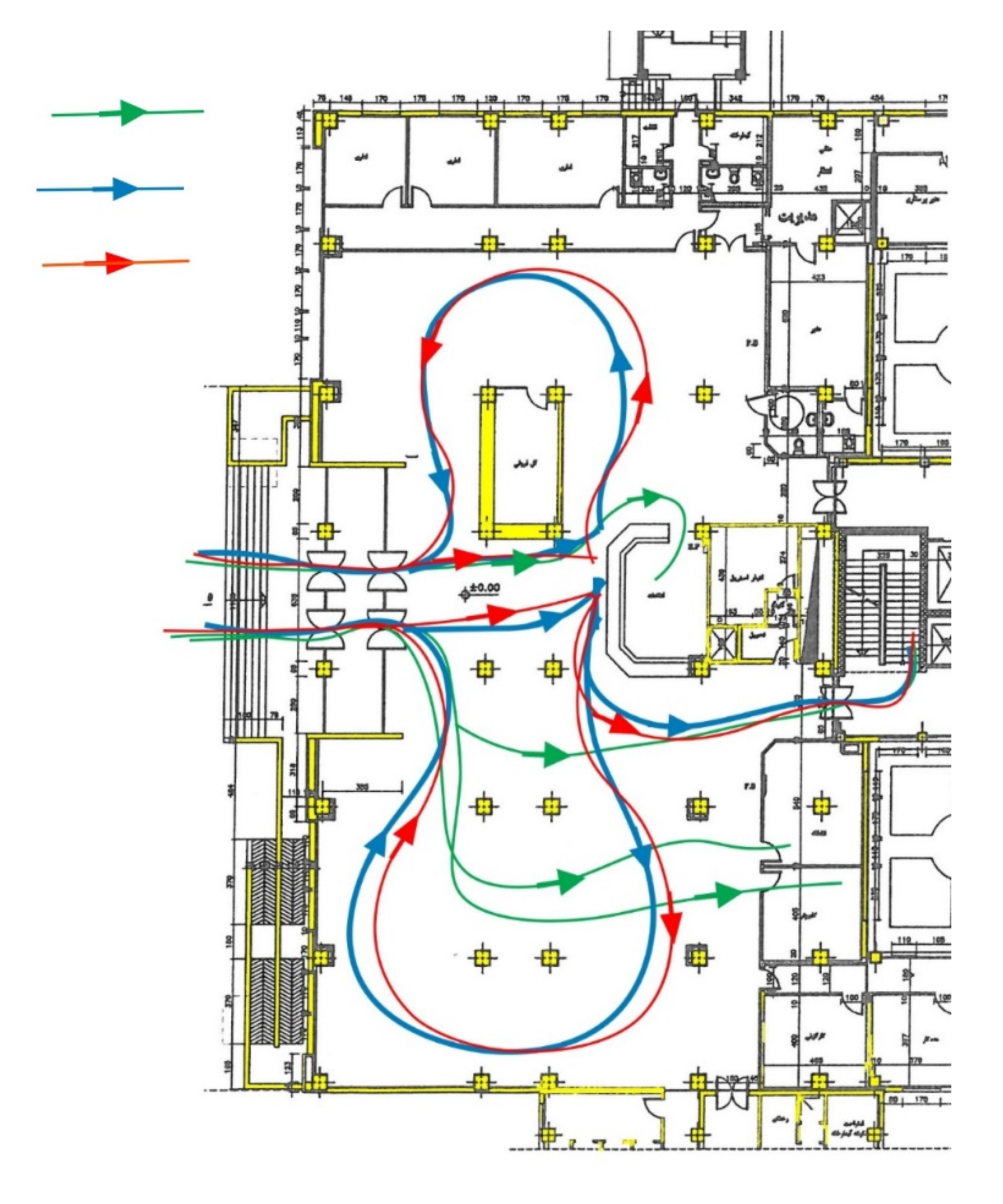
4.2.3. Improper or Absence of Spatial Isolation of Communication Spaces and Transporting Patient Tested Positive
“If the test is positive, a CT scan of the lungs should be done immediately in the infectious ward of the hospital. For a CT scan, patients and their escorts have to go to different parts. The doctor often asks the acute cases to be hospitalized. This cohort of patients is admitted to the third floor. Unfortunately, the location of this ward on the third floor has created problems because the patients need to use different corridors and communal spaces, and this expands the disease cycle.”
4.2.4. Lack of Sufficient Elevators
“There are six elevators for ordinary people and three elevators for transporting patients in this hospital, of which one is supposed to be used for the patients with COVID-19. Overcrowding at the visiting time makes the patients’ supporters (who have spent several hours directly with the sick person) use other elevators in this complex”.
“There are three elevators for transporting regular patients, but since the time of breakout, we are facing a shortage of elevators. To reach the elevators, we have to go through the common corridors.”
4.3. Operation Services
4.3.1. Non-Segregation of Hospital Admission and Lack of Social Distancing Measures
“The problem with all hospitals is that the admission ward for COVID-19 has not been isolated from the other wards.”
“The treatment staff can’t move tables and partitions, and they have to be very close to each other and work in a small space.”
4.3.2. Improper Clothing Isolation and Disinfection of Equipment for Non-COVID-19 Patients
“This hospital has a central laundry, and it is not possible to separate and allocate a separate place for the stuff of patients with COVID-19, and all washing is done inside this place.”
“All hospital equipment and supplies for the patients with COVID-19 and non-COVID-19 patients need to be disinfected. The disinfection is carried out in a sterile room.”
4.3.3. Lack of Indoor Environmental Conditions/Improper Lighting
“There is not enough light in the rooms, and the height of the rooms is very low. I do not like to stay in hospital rooms for a long time. These spaces are too depressing.”
4.4. Organizational Support for Staff
4.4.1. Inadequate Resting Places for Medical Staff
“The medical interns’ and residents’ resting area has few facilities, and there are 3-4 beds in each room. Since each one needs to be on call during the break, the ringing tone is of annoyance to others. It would be better for each person to have a separate room.”
“There are six or eight people in a small room. Though each one needs to have his mask on, social distancing is not observed.”
“The resting room is not separated from the ward. The nurses’ resting room is inside the COVID-19 ward. The room is very crowded, and there are almost 10 beds in a small room.”
4.4.2. Inappropriate Eating Conditions of Treatment Staff
“Since the time of the outbreak, we have not been to the self-service restaurant in the hospital. I think each section should have a separate restaurant, and this area should have access to the terrace and special open space.”
“The pantry is not close to the resting room and is near the place where there are lots of patients, and the risk of contamination is anxiety-provoking.”
4.4.3. Improper Separation of Sanitation Services
“In surgery, intensive care, and infectious wards, the sanitation services of the medical staff and patients are separated from each other, but in the other wards, they are commonly used by patients. This makes the medical staff feel anxious.”
5. Discussion
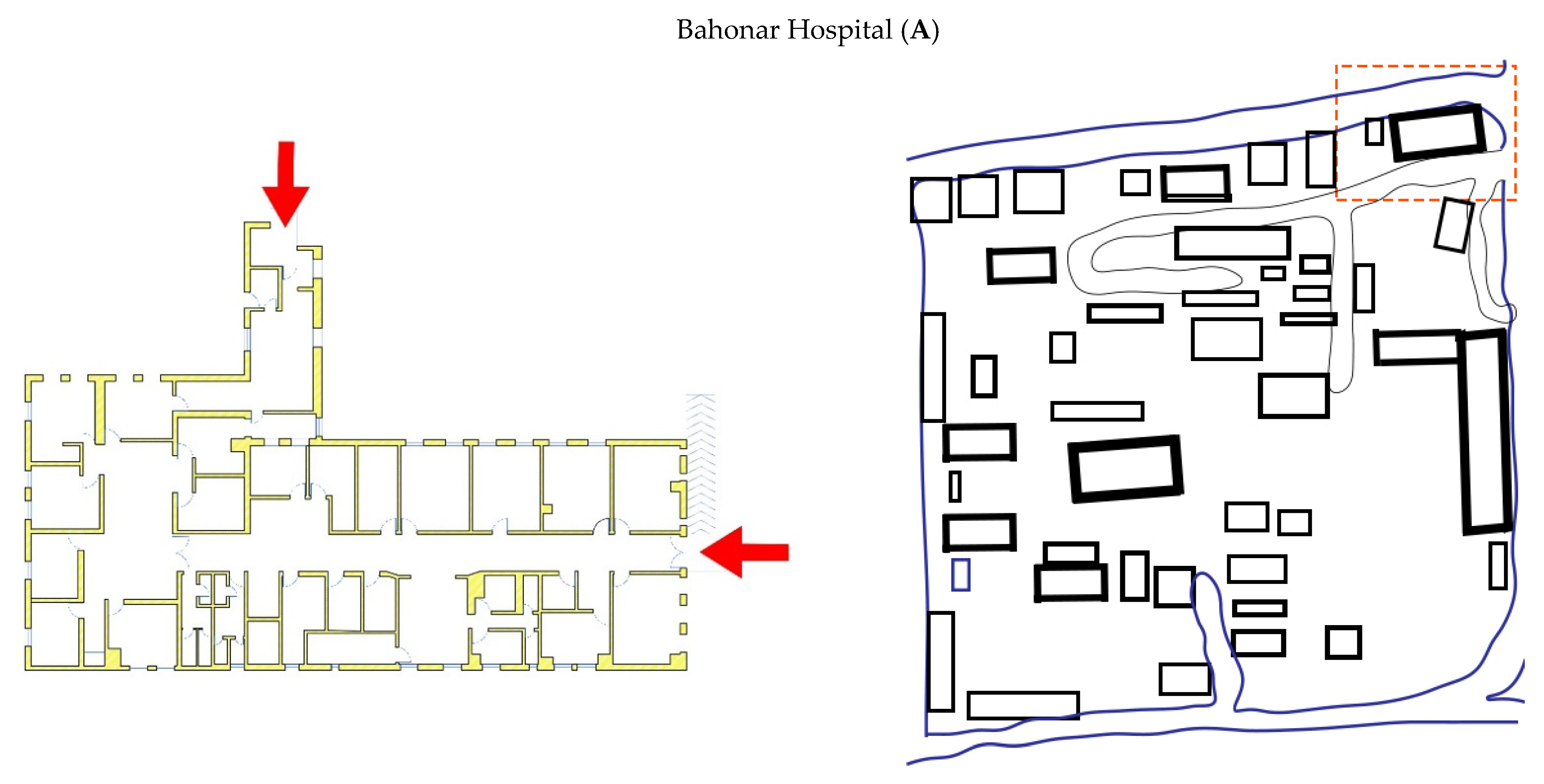
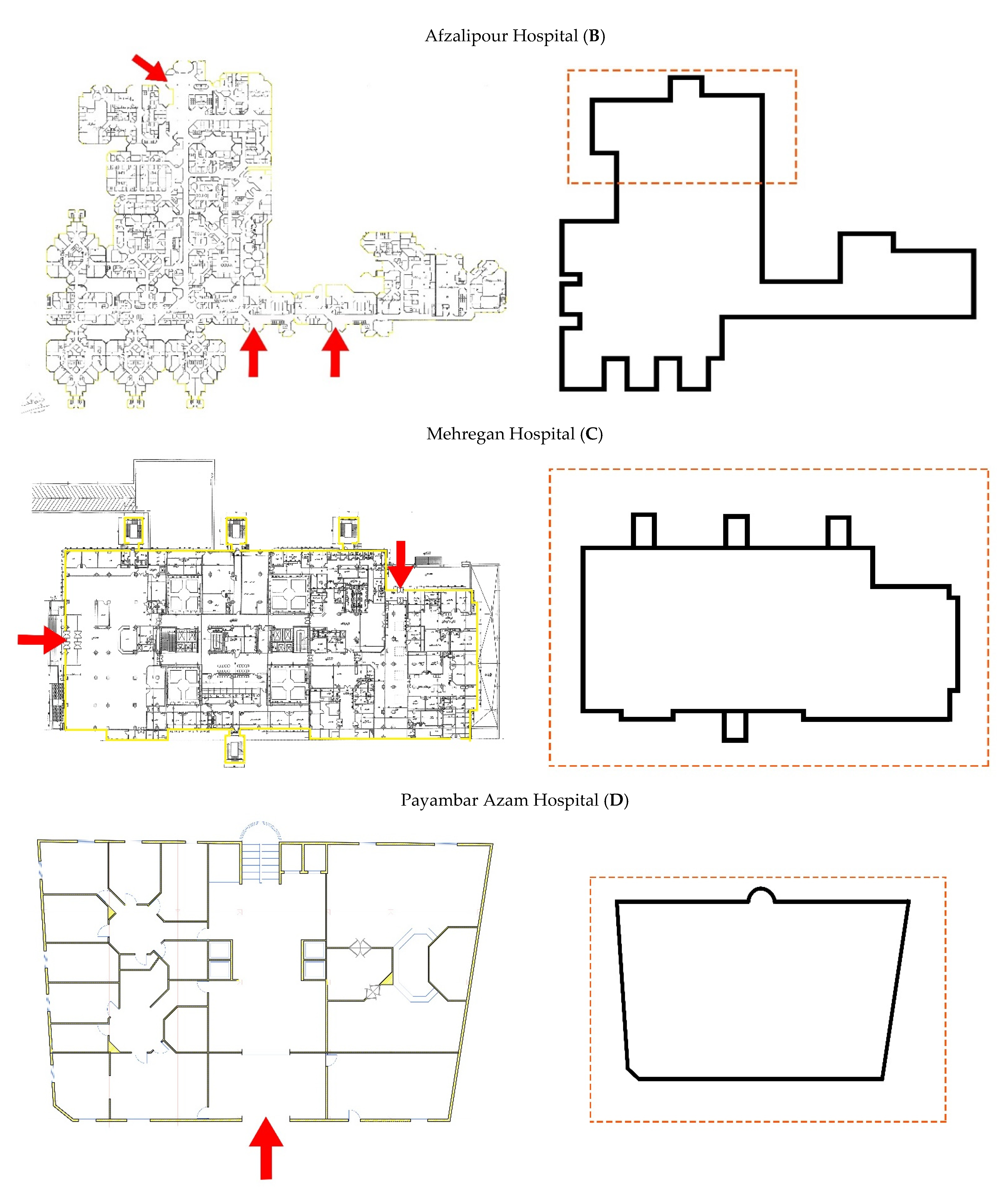
- Several single and double-story linear scattered buildings in the hospital yard.
- A multi-story clustered plan.
- A linear multi-story plan.
- A square multi-story plan.
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- La Rosa, G.; Fratini, M.; Della Libera, S.; Iaconelli, M.; Muscillo, M. Viral infections acquired indoors through airborne, droplet or contact transmission. Ann. Ist. Super Sanita 2013, 49, 124–132. [Google Scholar] [CrossRef]
- WHO. How Is Covid 19 Transmitted? World Health Organization, 2020. Available online: https://www.who.int/vietnam/news/detail/14-07-2020-q-a-how-is-covid-19-transmitted (accessed on 21 March 2021).
- CDC. Scientific Brief: SARS-COv-2 and Potential Airborne Transmission. Centers for Disease Control and Prevention. Available online: http://en.sbmu.ac.ir/uploads/201007_-_Scientific_Brief__SARS-CoV-2_and_Potential_Airborne_Transmission___CDC.pdf (accessed on 21 March 2021).
- Reason, J. Human error: Models and management. BMJ 2000, 320, 768–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulrich, R.S.; Wilson, P. Evidence-based design for reducing infection. Public Serv. Rev. Health 2006, 8, 24–25. [Google Scholar]
- Haq, S.; Luo, Y. Space syntax in healthcare facilities research: A review. HERD 2012, 5, 98–117. [Google Scholar] [CrossRef]
- Joseph, A.; Rashid, M. The architecture of safety: Hospital design. Curr. Opin. Crit. Care 2007, 13, 714–719. [Google Scholar] [CrossRef]
- Raoofi, A.; Takian, A.; Akbari Sari, A.; Olyaeemanesh, A.; Haghighi, H.; Aarabi, M. COVID-19 pandemic and comparative health policy learning in Iran. Arch. Iran. Med. 2020, 23, 220–234. [Google Scholar] [CrossRef] [Green Version]
- Vindrola-Padros, C.; Andrews, L.; Dowrick, A.; Nehla Djellouli, H.F.; Bautista Gonzalez, E.; Javadi, D.; Lewis-Jackson, S.; Manby, L.; MItchinson, L.; Mulcahy Simmons, S.; et al. Perceptions and experiences of healthcare workers during the COVID-19 pandemic in the UK. BMJ Open 2020, 10, e040503. [Google Scholar] [CrossRef]
- Abbas, S.; Al-Abrrow, H.; Abdullah, H.O.; Alnoor, A.; Khattak, Z.Z.; Khaw, K.W. Encountering Covid-19 and perceived stress and the role of a health climate among medical workers. Curr. Psychol. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y.; et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control 2020, 48, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of healthcare providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e808. [Google Scholar] [CrossRef]
- Song, X.; Fu, W.; Liu, X.; Luo, Z.; Wang, R.; Zhou, N.; Yan, S.; Lv, C. Mental health status of medical staff in emergency departments during the coronavirus disease 2019 epidemic in China. Brain Behav. Immun. 2020, 88, 60–65. [Google Scholar] [CrossRef]
- Kieft, R.A.; de Brouwer, B.B.; Francke, A.L.; Delnoij, D.M. How nurses and their work environment affect patient experiences of the quality of care: A qualitative study. BMC Health Serv. Res. 2014, 14, 249. [Google Scholar] [CrossRef] [Green Version]
- Aiken, L.H.; Sermeus, W.; Van den Heede, K.; Sloane, D.M.; Busse, R.; McKee, M.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P.; Moreno-Casbas, M.T.; et al. Patient safety, satisfaction, and quality of hospital care: Cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ 2012, 344, e1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutney-Lee, A.; McHugh, M.D.; Sloane, D.M.; Cimiotti, J.P.; Flynn, L.; Neff, D.F.; Aiken, L.H. Nursing: A key to patient satisfaction. Health Aff. 2009, 28, w669–w677. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.D.; Kutney-Lee, A.; Cimiotti, J.P.; Sloane, D.M.; Aiken, L.H. Nurses’ widespread job dissatisfaction, burnout, and frustration with health benefits signal problems for patient care. Health Aff. 2011, 30, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Al Thobaity, A.; Alshammari, F. Nurses on the Frontline against the COVID-19 Pandemic: An Integrative Review. Dubai Med. J. 2020, 3, 87–92. [Google Scholar] [CrossRef]
- Aygün, G.; Demirkiran, O.; Utku, T.; Mete, B.; Urkmez, S.; Yilmaz, M.; Yaşar, H.; Dikmen, Y.; Oztürk, R. Environmental contamination during a carbapenem-resistant Acinetobacter baumannii outbreak in an intensive care unit. J. Hosp. Infect. 2002, 52, 259–262. [Google Scholar] [CrossRef]
- Boyce, J.M.; Potter-Bynoe, G.; Chenevert, C.; King, T. Environmental contamination due to methicillin-resistant Staphylococcus aureus possible infection control implications. Infect. Control Hosp. Epidemiol. 1997, 18, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Huisman, E.R.C.M.; Morales, E.; van Hoof, J.; Kort, H.S.M. Healing environment: A review of the impact of physical environmental factors on users. Build. Environ. 2012, 58, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Pangrazio, J.R. Planning Public Spaces for Health Care Facilities. Health Facilities Management. Available online: http://www.hfmmagazine.com/display/HFM-newsarticle.dhtml?dcrPath/templatedata/HF_Common/NewsArticle/data/HFM/Magazine/2013/Mar/313HFM_FEA_design (accessed on 13 January 2013).
- Jiang, S.; Verderber, S. On the Planning and Design of Hospital Circulation Zones. HERD 2017, 10, 124–146. [Google Scholar] [CrossRef]
- Brambilla, A.; Rebecchi, A.; Capolongo, S. Evidence based hospital design. A literature review of the recent publications about the EBD impact of built environment on hospital ’occupants’ and organizational outcomes. Ann. Ig. 2019, 31, 165–180. [Google Scholar]
- Capolongo, S.; Gola, M.; Brambilla, A.; Morganti, A.; Mosca, E.I.; Barach, P. COVID-19 and Healthcare facilities: A decalogue of design strategies for resilient hospitals. Acta Bio. Med. 2020, 91, 50–60. [Google Scholar]
- Ulrich, R.S. View Through a Window May Influence Recovery from Surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [Green Version]
- Nejati, A.; Shepley, M.; Rodiek, S.; Lee, C.; Varni, J. Restorative Design Features for Hospital Staff Break Areas: A Multi-Method Study. HERD 2016, 9, 16–35. [Google Scholar] [CrossRef] [PubMed]
- Debajyoti, P.; Harvey, T.; Barach, P. The impact of exterior views on nurse stress: An Exploratory Study. Health Environ. Res. Des. J. 2008, 2, 27–38. [Google Scholar]
- Bedon, C.; Mattei, S. Facial Expression-Based Experimental Analysis of Human Reactions and Psychological Comfort on Glass Structures in Buildings. Buildings 2021, 11, 204. [Google Scholar] [CrossRef]
- Lateef, F. Hospital design for better infection control. J. Emergencies Trauma Shock 2009, 2, 175. [Google Scholar] [CrossRef]
- Urlich, R.; Zimring, C.; Quan, X.; Joseph, A.; Choudhary, R. The Role of the Physical Environment in the Hospital of the 21st Century; The Center for Health Design: Concord, CA, USA, 2004. [Google Scholar]
- Menzies, D.; Fanning, A.; Yuan, L.; FitzGerald, J.M. Hospital ventilation and risk for tuberculous infection in Canadian health care workers. Ann. Intern. Med. 2000, 133, 779–789. [Google Scholar] [CrossRef]
- Anderson, R.L.; Mackel, D.C.; Stoler, B.S.; Mallison, G.F. Carpeting in hospitals: An epidemiological evaluation. J. Clin. Microbiol. 1982, 15, 408–415. [Google Scholar] [CrossRef] [Green Version]
- Noskin, G.A.; Bednarz, P.; Suriano, T.; Reiner, S.; Peterson, L.R. Persistent contamination of fabric-covered furniture by vancomycin-resistant enterococci: Implications for upholstery selection in hospitals. Am. J. Infect. Control 2000, 28, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, R.S.; Zimring, C.; Zhu, X.; DuBose, J.; Seo, H.-B.; Choi, Y.-S.; Quan, X.; Joseph, A. A review of the research literature on evidence-based healthcare design. HERD 2008, 1, 61–125. [Google Scholar] [CrossRef]
- Alfonsi, E.; Capolongo, S.; Buffoli, M. Evidence Based Design and healthcare: An unconventional approach to hospital design. Ann Ig. 2014, 26, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Marberry, S.O. Improving Healthcare with better Building Design; Health Administration Press: Chicago, IL, USA, 2006. [Google Scholar]
- Emmanuel, U.; Osondu, E.D.; Kalu, K.C. Architectural design strategies for infection prevention and control (IPC) in health-care facilities: Towards curbing the spread of Covid-19. J. Environ. Health Sci. Eng. 2020, 18, 1699–1707. [Google Scholar] [CrossRef] [PubMed]
- Hockberger, P. The damaging effects of sunlight on bacteria. J. Photochem. Photobiol. 2000, 58, 155–191. [Google Scholar] [CrossRef]
- Strong, P. Daylight Benefit in Healthcare Buildings. Designing Buildings-BR Group. 2020. Available online: https://www.designingbuildings.co.uk/w/images/2/22/David_Strong_(2of2)Daylight_Benefits_in_Healthcare_buildgs-BRGroup (accessed on 23 April 2021).
- Hamilton, D.K. The four levels of evidence-based practice. Healthc. Des. 2003, 11, 19–26. [Google Scholar]
- Elf, M.; Anåker, A.; Marcheschi, E.; Sigurjónsson, Á.; Ulrich, R.S. The built environment and its impact on health outcomes and experiences of patients, significant others and staffs’ protocol for a systematic review. Nurs. Open 2020, 7, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Strauss, A.L.; Corbin, J.M. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 2nd ed.; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Ulrich, R.S.; Berry, L.L.; Quan, X.; Parish, J.T. A conceptual framework for the domain of evidence-based design. HERD 2010, 4, 95–114. [Google Scholar] [CrossRef]
- Shepley, M.M. Predesign and post occupancy analysis of staff behavior in a neonatal intensive care unit. Child. Health Care 2002, 31, 237–253. [Google Scholar] [CrossRef]
- Shepley, M.M.; Davies, K. Nursing unit configuration and its relationship to noise and nurse walking behavior: An AIDS/HIV unit case study. AIA Acad. J. 2003, 6, 12–14. [Google Scholar]
- Setola, N.; Borgianni, S. Designing Public Spaces in Hospitals; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Dickerman, K.N.; Barach, P. Designing the Built Environment for A Culture and System of Patient Safety—A Conceptual, New Design Process. In Advances in Patient Safety: New Directions and Alternative Approaches; Henriksen, K., Battles, J.B., Keyes, M.A., Grady, M.L., Eds.; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008; Volume 2. [Google Scholar]
- Maarefvand, M.; Hosseinzadeh, S.; Farmani, O.; Safarabadi Farahani, A.; Khubchandani, J. Coronavirus outbreak and stress in Iranians. Int. J. Environ. Res. Public Health 2020, 17, 4441. [Google Scholar] [CrossRef]
- Hamshahrionline. Available online: https://www.hamshahrionline.ir/news/531134/ (accessed on 1 March 2021).
- Sajadi, H.; Hartley, K. COVID-19 pandemic response in Iran: A dynamic perspective on policy capacity. J. Asian Public Policy 2021. [Google Scholar] [CrossRef]
- Rassouli, M.; Ashrafizadeh, H.; Shirinabadi Farahani, A.; Akbari, M.E. COVID-19 Management in Iran as One of the Most Affected Countries in the World: Advantages and Weaknesses. Front. Public Health 2020, 8, 510. [Google Scholar] [CrossRef] [PubMed]
- Myatt, T.A.; Johnston, S.L.; Zuo, Z.; Wand, M.; Kebadze, T.; Rudnick, S.; Milton, D.K. Detection of airborne rhinovirus and its relation to outdoor air supply in office environments. Am. J. Respir. Crit. Care Med. 2004, 169, 1187–1190. [Google Scholar] [CrossRef]
- Roshanzadeh, M.; Jamalinik, M.; Hasheminik, M.; Tajabadi, A. Stigma of Covid-19: The Basic Challenge in Health Economics. Iran Occup. Health 2020, 17 (Suppl. 1), 137–141. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Built Environment and Its Impact on Health Outcomes and Experiences of Staff during COVID-19 | Built Environment Design Variables | Main Problems |
|---|---|---|
| Lack of supportive environmental factors to minimize hospital-acquired infections | Layouts and circulations | Problems with COVID-19 patients and others sharing the main entrance |
| Problems with the emergency department and waiting rooms | ||
| Improper spatial isolation of communal spaces and transporting patients who have tested positive through horizontal and vertical circulation | ||
| Space configuration | Poor isolation of the infectious ward | |
| Improper or absence of spatial isolation of patients with COVID-19 from others | ||
| Long distance between essential parts of the hospital | ||
| Lack of operation strategies | Shared Facilities between COVID-19 and other patients | Improper clothing isolation and disinfection of equipment for non-COVID-19 patients |
| Visual comfort measures | Lack of improper lighting/ lack of windows | |
| Lack of organization support | Staff resting rooms | Inadequate resting places |
| Staff dining spaces | Inappropriate eating conditions of treatment staff | |
| Social Distancing | Lack of social distancing in staff rooms and fixed furniture | |
| Sanitation facilities | Improper separation of sanitation services |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lesan, M.; Khozaei, F.; Kim, M.J.; Shahidi Nejad, M. Identifying Health Care Environment Contradictions in Terms of Infection Control during a Pandemic with a Focus on Health Workers’ Experience. Sustainability 2021, 13, 9964. https://doi.org/10.3390/su13179964
Lesan M, Khozaei F, Kim MJ, Shahidi Nejad M. Identifying Health Care Environment Contradictions in Terms of Infection Control during a Pandemic with a Focus on Health Workers’ Experience. Sustainability. 2021; 13(17):9964. https://doi.org/10.3390/su13179964
Chicago/Turabian StyleLesan, Maryam, Fatemeh Khozaei, Mi Jeong Kim, and Marziyeh Shahidi Nejad. 2021. "Identifying Health Care Environment Contradictions in Terms of Infection Control during a Pandemic with a Focus on Health Workers’ Experience" Sustainability 13, no. 17: 9964. https://doi.org/10.3390/su13179964
APA StyleLesan, M., Khozaei, F., Kim, M. J., & Shahidi Nejad, M. (2021). Identifying Health Care Environment Contradictions in Terms of Infection Control during a Pandemic with a Focus on Health Workers’ Experience. Sustainability, 13(17), 9964. https://doi.org/10.3390/su13179964