
Treatment Effect of Exercise Intervention for Female College Students with Depression: Analysis of Electroencephalogram Microstates and Power Spectrum







Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Exercise Intervention Methods
2.3. EEG Recording
2.4. EEG Data Preprocessing
2.5. EEG Microstate Analysis
2.6. Microstate Parameters Recording
2.7. EEG Power Spectrum Analysis
2.8. Statistics Analysis
- (1)
- A two-way analysis of variance (ANOVA) was carried out for the duration and the occurrence parameters in the microstates with a number of correct items as the dependent variables, groups (HC, DC and EI) as a between-subject variable, and the microstate classes (A, B, C, and D) as within-subject variables. The results were tested post-hoc using independent sample t-tests in the case of a significant main effect. A false discovery rate (FDR) correction was applied to minimize the risk of a type I error. In order to estimate the effect size of these statistical tests, the partial eta-squared (η2) and Cohen’s d were computed for ANOVAs and independent sample t-tests, respectively. p < 0.05 was considered statistically significant.
- (2)
- A one-way ANOVA was performed for the power values in the δ, θ, α, and β frequency bands. p < 0.05 was considered statistically significant.
- (3)
- The spatial correlation of the three groups between the power spectrum values in each band and the temporal parameters of the four categories of microstates were assessed using the Pearson correlation analysis.
3. Results
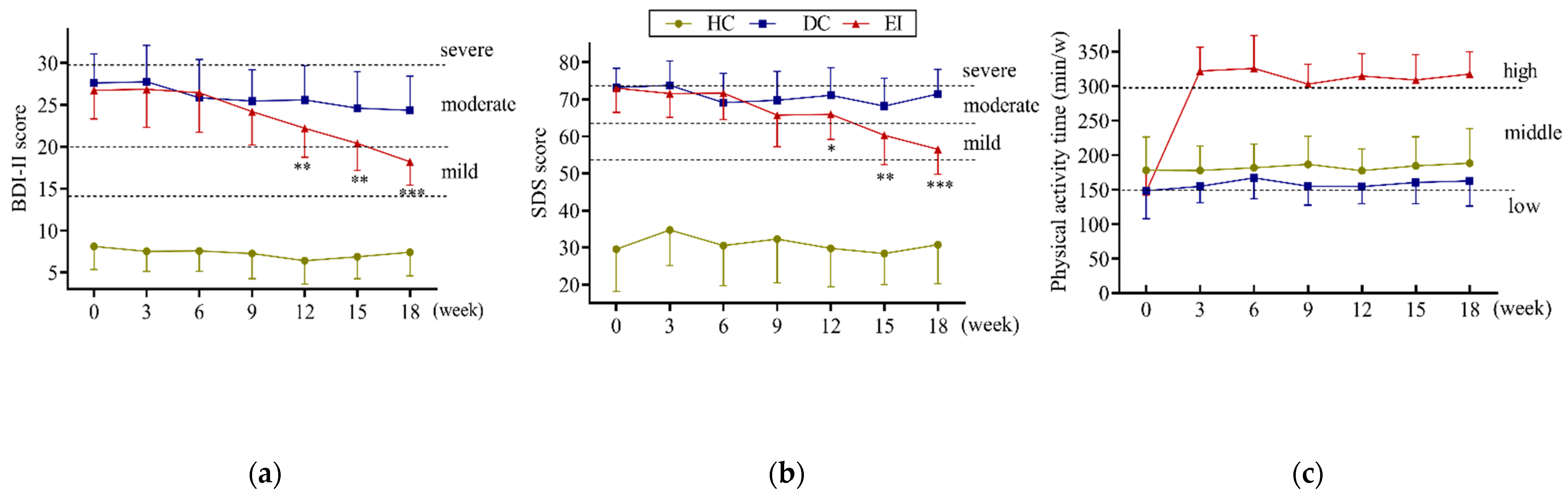
3.1. Total Exercise Level and Depression Symptoms
3.2. Comparison of Microstate Parameters
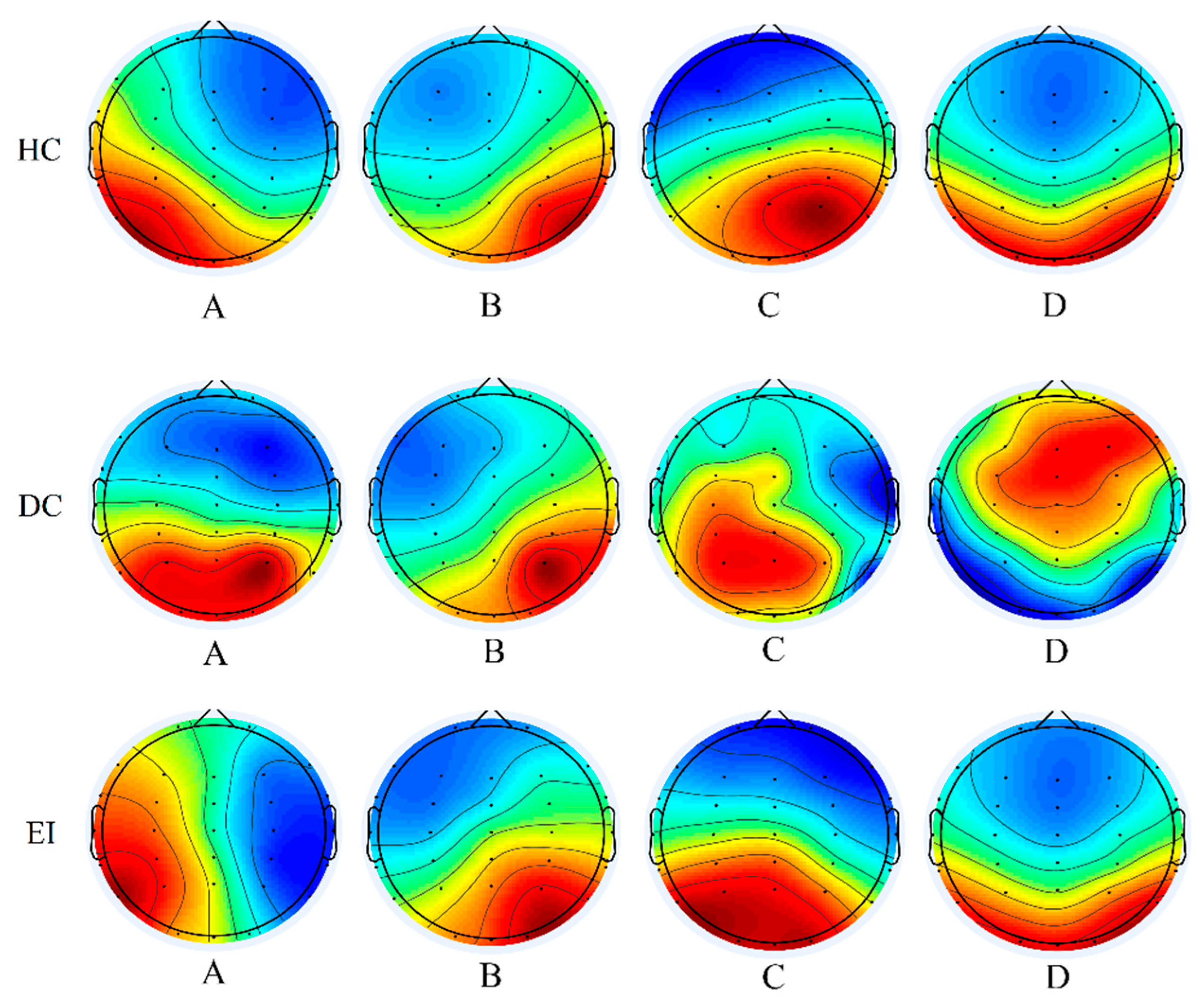
3.2.1. Comparison of Brain Topography in Microstates
3.2.2. Results for EEG Microstate Parameters
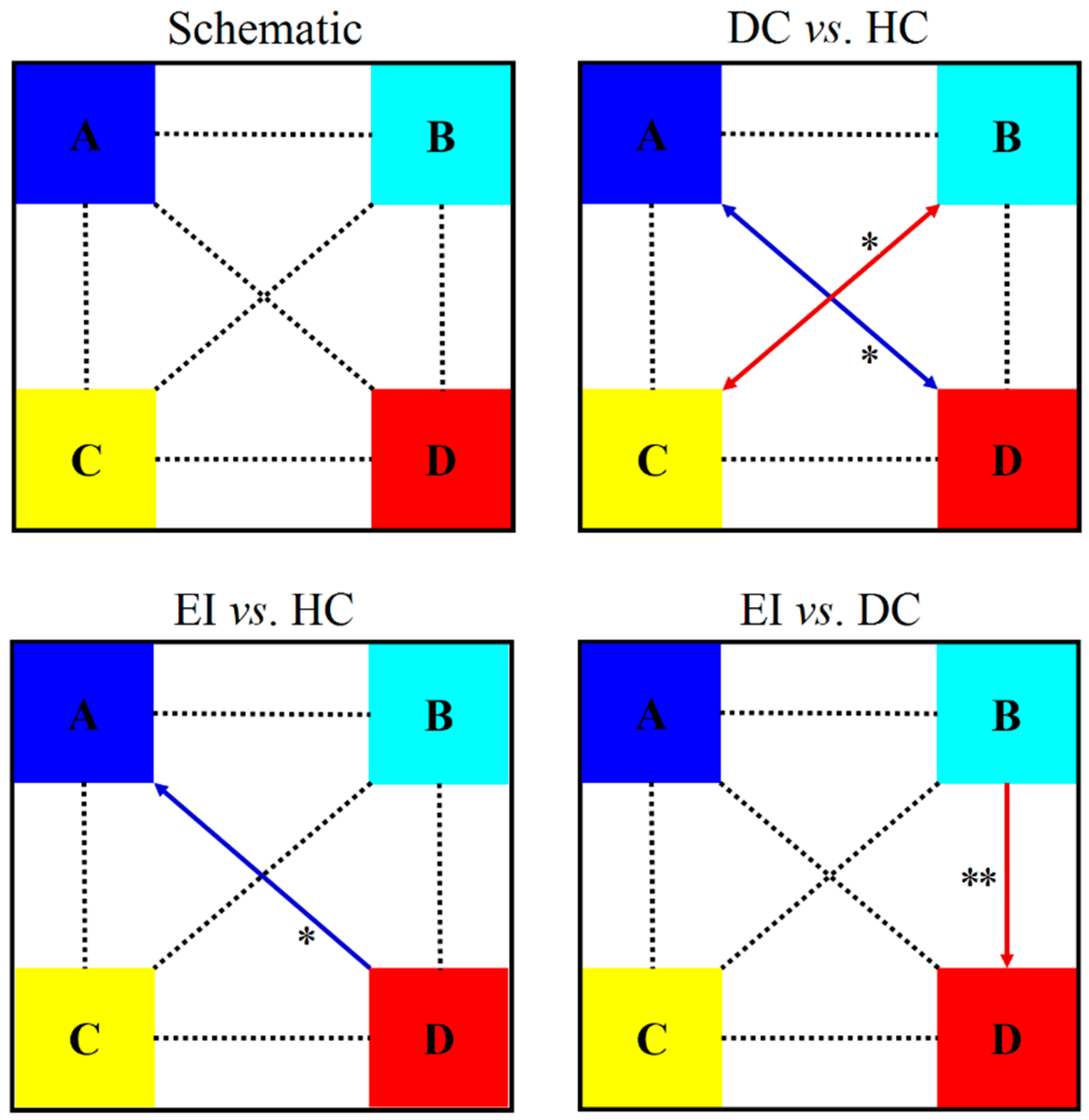
3.2.3. Probabilities of Transition between Microstates
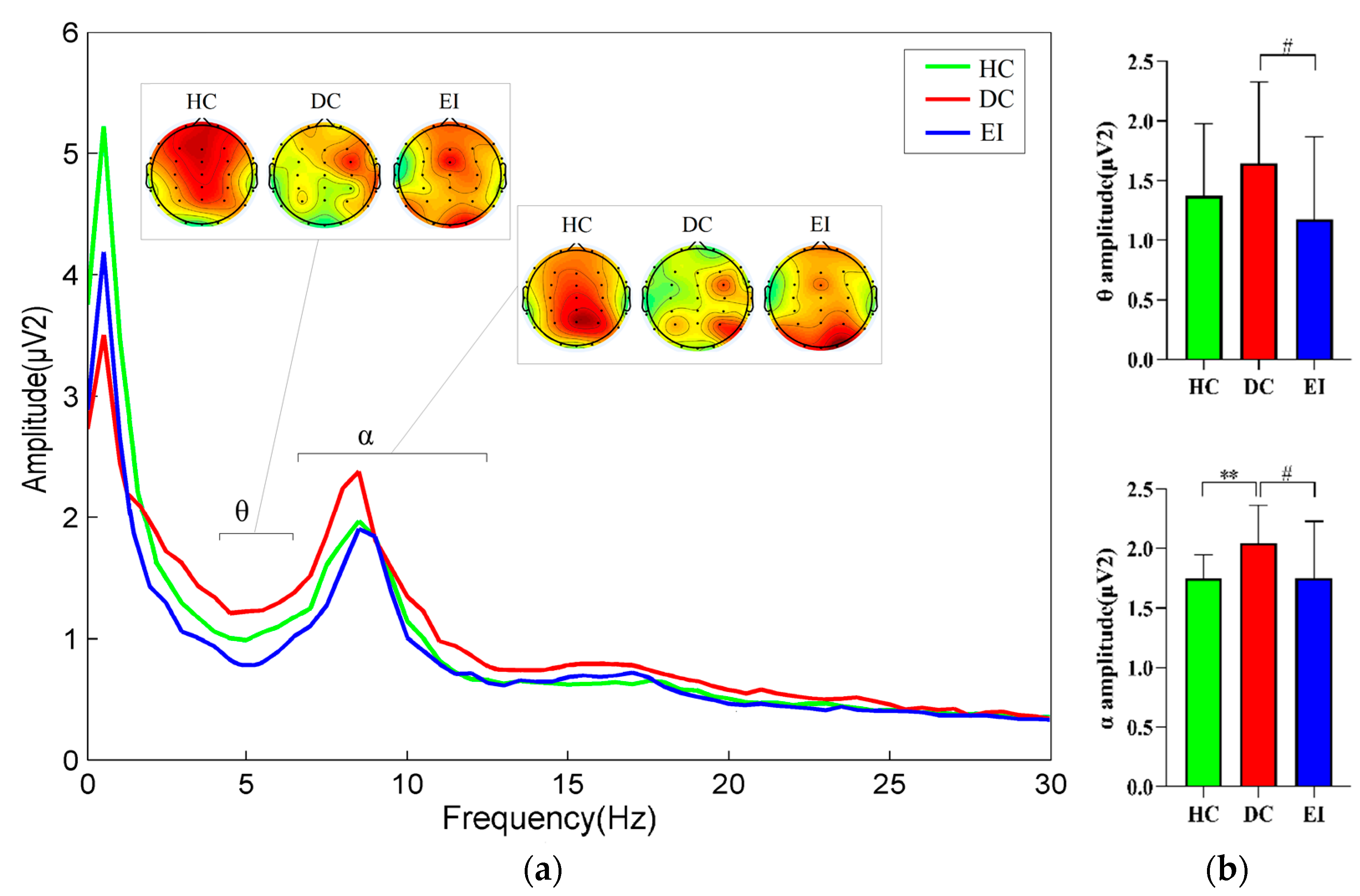
3.3. Comparison between Power Spectrum Values and EEG Energy Maps
3.4. Correlation of EEG Power Spectrum with Microstate Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Del Pozo Cruz, B.; Alfonso-Rosa, R.M.; McGregor, D.; Chastin, S.F.; Palarea-Albaladejo, J.; Del Pozo Cruz, J. Sedentary behaviour is associated with depression symptoms: Compositional data analysis from a representative sample of 3233 US adults and older adults assessed with accelerometers. J. Affect. Disord. 2020, 265, 59–62. [Google Scholar] [CrossRef]
- Abdallah, C.G.; Sanacora, G.; Duman, R.S.; Krystal, J.H. The neurobiology of depression, ketamine and rapid-acting anti-depressants: Is it glutamate inhibition or activation? Pharmacol. Ther. 2018, 190, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Bernaras, E.; Jaureguizar, J.; Garaigordobil, M. Child and Adolescent Depression: A Review of Theories, Evaluation Instruments, Prevention Programs, and Treatments. Front. Psychol. 2019, 10, 543. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Buntrock, C.; Mortier, P.; Auerbach, R.; Weisel, K.K.; Kessler, R.C.; Cuijpers, P.; Green, J.G.; Kiekens, G.; Nock, M.K.; et al. Prediction of major depressive disorder onset in college students. Depress. Anxiety 2019, 36, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Ha, A.S.; Lonsdale, C.; Lubans, D.R.; Ng, J.Y.Y. Increasing Students’ Activity in Physical Education: Results of the Self-determined Exercise and Learning for FITness Trial. Med. Sci. Sports Exerc. 2020, 52, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Asarnow, L.D. Depression and sleep: What has the treatment research revealed and could the HPA axis be a potential mechanism? Curr. Opin. Psychol. 2020, 34, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Zheng, P.; Gao, H.C.; Li, Q.; Shao, W.H.; Zhang, M.L.; Cheng, K.; Yang, D.Y.; Fan, S.H.; Chen, L.; Fang, L.; et al. Plasma metabonomics as a novel diagnostic approach for major depressive disorder. J. Proteome Res. 2012, 11, 1741–1748. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Chi, A.; Yan, J.; Yao, C. Feature of Heart Rate Variability and Metabolic Mechanism in Female College Students with Depression. BioMed Res. Int. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Hua, L.; Jiang, H.; Dai, Z.; Han, Y.; Lin, P.; Wang, H.; Lu, Q.; Yao, Z. Autonomic Nervous System Is Related to Inhibitory and Control Function Through Functional Inter-Region Connectivities of OFC in Major Depression. Neuropsychiatr. Dis. Treat. 2020, 16, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Carek, P.J.; Laibstain, S.E.; Carek, S.M. Exercise for the Treatment of Depression and Anxiety. Int. J. Psychiatry Med. 2011, 41, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Kvam, S.; Kleppe, C.L.; Nordhus, I.H.; Hovland, A. Exercise as a treatment for depression: A meta-analysis. J. Affect. Disord. 2016, 202, 67–86. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Knapen, J.; Vancampfort, D.; Moriën, Y.; Marchal, Y. Exercise therapy improves both mental and physical health in patients with major depression. Disabil. Rehabil. 2014, 37, 1490–1495. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Mental Health Physical Activity. Available online: https://www.who.int/mental_health/mhgap/evidence/resource/depression_q6.pdf (accessed on 25 May 2015).
- National Institute for Health and Clinical Excellence (UK). Depression: Evidence Update April 2012: A Summary of Selected New Evidence Relevant to NICE Clinical Guideline 90 ‘The Treatment and Management of Depression in Adults’ (2009); National Institute for Health and Clinical Excellence: London, UK, 2012.
- Ströhle, A. Physical activity, exercise, depression and anxiety disorders. J. Neural Transm. 2008, 116, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.T.; Vorup, J.; Nistrup, A.; Wikman, J.M.; Alstrøm, J.M.; Melcher, P.G.S.; Pfister, G.U.; Bangsbo, J. Effect of team sports and resistance training on physical function, quality of life, and motivation in older adults. Scand. J. Med. Sci. Sports 2017, 27, 852–864. [Google Scholar] [CrossRef] [PubMed]
- Sabiston, C.M.; Jewett, R.; Ashdown-Franks, G.; Bélanger, M.; Brunet, J.; O’Loughlin, E.; O’Loughlin, J. Number of Years of Team and Individual Sport Participation During Adolescence and Depressive Symptoms in Early Adulthood. J. Sport Exerc. Psychol. 2016, 38, 105–110. [Google Scholar] [CrossRef]
- Ay, B.; Yildirim, O.; Talo, M.; Baloglu, U.B.; Aydin, G.; Puthankattil, S.D.; Acharya, U.R. Automated Depression Detection Using Deep Representation and Sequence Learning with EEG Signals. J. Med. Syst. 2019, 43, 205. [Google Scholar] [CrossRef]
- De Aguiar Neto, F.S.; Rosa, J.L.G. Depression biomarkers using non-invasive EEG: A review. Neurosci. Biobehav. Rev. 2019, 105, 83–93. [Google Scholar] [CrossRef]
- Lehmann, D.; Ozaki, H.; Pal, I. EEG alpha map series: Brain micro-states by space-oriented adaptive segmentation. Electroencephalogr. Clin. Neurophysiol. 1987, 67, 271–288. [Google Scholar] [CrossRef]
- Michel, C.M.; Koenig, T. EEG microstates as a tool for studying the temporal dynamics of whole-brain neuronal networks: A review. NeuroImage 2018, 180, 577–593. [Google Scholar] [CrossRef]
- Cai, Y.; Chen, S.; Chen, Y.; Li, J.; Wang, C.D.; Zhao, F.; Dang, C.P.; Liang, J.; He, N.; Liang, M.; et al. Altered Resting-State EEG Microstate in Idiopathic Sudden Sensorineural Hearing Loss Patients with Tinnitus. Front. Neurosci. 2019, 13, 443. [Google Scholar] [CrossRef]
- Koenig, T.; Lehmann, D.; Merlo, M.C.; Kochi, K.; Hell, D.; Koukkou, M. A deviant EEG brain microstate in acute, neuroleptic-naive schizophrenics at rest. Eur. Arch. Psychiatry Clin. Neurosci. 1999, 249, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Britz, J.; Van De Ville, D.; Michel, C.M. BOLD correlates of EEG topography reveal rapid resting-state network dynamics. NeuroImage 2010, 52, 1162–1170. [Google Scholar] [CrossRef]
- Milz, P.; Faber, P.L.; Lehmann, D.; Koenig, T.; Kochi, K.; Pascual-Marqui, R.D. The functional significance of EEG microstates-—Associations with modalities of thinking. Neuroimage 2016, 125, 643–656. [Google Scholar] [CrossRef]
- Thilakavathi, B.; Devi, S.S.; Malaiappan, M.; Bhanu, K. EEG power spectrum analysis for schizophrenia during mental activity. Australas. Phys. Eng. Sci. Med. 2019, 42, 887–897. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, T.; Tandon, S.D. Prevention of Depression in Childhood and Adolescence. Child Adolesc. Psychiatr. Clin. N. Am. 2016, 25, 201–218. [Google Scholar] [CrossRef] [PubMed]
- Fuentes-García, J.P.; Villafaina, S.; Collado-Mateo, D.; Cano-Plasencia, R.; Gusi, N. Chess Players Increase the Theta Power Spectrum When the Difficulty of the Opponent Increases: An EEG Study. Int. J. Environ. Res. Public Health 2019, 17, 46. [Google Scholar] [CrossRef]
- Roepke, A.M.; Seligman, M.E.P. Depression and prospection. Br. J. Clin. Psychol. 2015, 55, 23–48. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; Fletcher, K.; Hyett, M.; Hadzi-Pavlovic, D.; Barrett, M.; Synnott, H. Measuring melancholia: The utility of a prototypic symptom approach. Psychol. Med. 2008, 39, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Zung, W.W.K. A Self-Rating Depression Scale. Arch. Gen. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef]
- Gellish, R.L.; Goslin, B.R.; Olson, R.E.; McDONALD, A.; Russi, G.D.; Moudgil, V.K. Longitudinal Modeling of the Relationship between Age and Maximal Heart Rate. Med. Sci. Sports Exerc. 2007, 39, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Von Wegner, F.; Knaut, P.; Laufs, H. EEG Microstate Sequences from Different Clustering Algorithms Are Information-Theoretically Invariant. Front. Comput. Neurosci. 2018, 12, 70. [Google Scholar] [CrossRef] [PubMed]
- Brunet, D.; Murray, M.M.; Michel, C.M. Spatiotemporal Analysis of Multichannel EEG: Cartool. Comput. Intell. Neurosci. 2011, 2011, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Koenig, T.; Studer, D.; Hubl, D.; Melie, L.; Strik, W.K. Brain connectivity at different time-scales measured with EEG. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2005, 360, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Drissi, N.M.; Szakács, A.; Witt, S.T.; Wretman, A.; Ulander, M.; Ståhlbrandt, H.; Darin, N.; Hallböök, T.; Landtblom, A.M.; Engström, M. Altered Brain Microstate Dynamics in Adolescents with Narcolepsy. Front. Hum. Neurosci. 2016, 10, 369. [Google Scholar] [CrossRef] [PubMed]
- Khanna, A.; Pascual-Leone, A.; Michel, C.M.; Farzan, F. Microstates in resting-state EEG: Current status and future directions. Neurosci. Biobehav. Rev. 2015, 49, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Jia, H.; Wu, X.; Yu, D.; Feng, Y. Altered Resting-State EEG Microstate Parameters and Enhanced Spatial Complexity in Male Adolescent Patients with Mild Spastic Diplegia. Brain Topogr. 2016, 30, 233–244. [Google Scholar] [CrossRef]
- Akin, M. Comparison of Wavelet Transform and FFT Methods in the Analysis of EEG Signals. J. Med. Syst. 2002, 26, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Dressler, O.; Schneider, G.; Stockmanns, G.; Kochs, E.F. Awareness and the EEG power spectrum: Analysis of frequencies. Br. J. Anaesth. 2004, 93, 806–809. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Liu, F.; Shen, J.; Wei, M.; Yang, Y. Comparative efficacy of seven exercise interventions for symptoms of depression in college students: A network of meta-analysis. Medicine 2020, 99, e23058. [Google Scholar] [CrossRef]
- Andreou, C.; Faber, P.L.; Leicht, G.; Schoettle, D.; Polomac, N.; Hanganu-Opatz, I.L.; Lehmann, D.; Mulert, C. Resting-state connectivity in the prodromal phase of schizophrenia: Insights from EEG microstates. Schizophr. Res. 2014, 152, 513–520. [Google Scholar] [CrossRef]
- Strik, W.K.; Dierks, T.; Becker, T.; Lehmann, D. Larger topographical variance and decreased duration of brain electric mi-crostates in depression. J. Neural Transm./Gen. Sect. JNT 1995, 99, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Damborská, A.; Piguet, C.; Aubry, J.-M.; Dayer, A.G.; Michel, C.M.; Berchio, C. Altered Electroencephalographic Resting-State Large-Scale Brain Network Dynamics in Euthymic Bipolar Disorder Patients. Front. Psychiatry 2019, 10, 826. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.; Whitton, A.E.; Deccy, S.; Ironside, M.L.; Rutherford, A.; Beltzer, M.; Sacchet, M.; Pizzagalli, D.A. Abnormalities in electroencephalographic microstates are state and trait markers of major depressive disorder. Neuropsychopharmacology 2020, 45, 2030–2037. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, D.; Levitin, D.J.; Menon, V. A critical role for the right fronto-insular cortex in switching between central-executive and default-mode networks. Proc. Natl. Acad. Sci. USA 2008, 105, 12569–12574. [Google Scholar] [CrossRef] [PubMed]
- Coste, C.P.; Kleinschmidt, A. Cingulo-opercular network activity maintains alertness. NeuroImage 2016, 128, 264–272. [Google Scholar] [CrossRef]
- Atluri, S.; Wong, W.; Moreno, S.; Blumberger, D.M.; Daskalakis, Z.J.; Farzan, F. Selective modulation of brain network dy-namics by seizure therapy in treatment-resistant depression. NeuroImage Clin. 2018, 20, 1176–1190. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.A.; Gandevia, S.C.; Macefield, V.G. Somatotopic organization of the processing of muscle and cutaneous pain in the left and right insula cortex: A single-trial fMRI study. Pain 2007, 128, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Serrano, J.I.; Del Castillo, M.D.; Cortés, V.; Mendes, N.; Arroyo, A.; Andreo, J.; Rocon, E.; Del Valle, M.; Herreros, J.; Romero, J.P. EEG Microstates Change in Response to Increase in Dopaminergic Stimulation in Typical Parkinson’s Disease Patients. Front. Neurosci. 2018, 12, 714. [Google Scholar] [CrossRef]
- Tomescu, M.; Rihs, T.; Rochas, V.; Hardmeier, M.; Britz, J.; Allali, G.; Fuhr, P.; Eliez, S.; Michel, C. From swing to cane: Sex differences of EEG resting-state temporal patterns during maturation and aging. Dev. Cogn. Neurosci. 2018, 31, 58–66. [Google Scholar] [CrossRef]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable intrinsic connectivity networks for salience processing and executive control. J. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef]
- Gujral, S.; Aizenstein, H.; Reynolds, C.F., III; Butters, M.A.; Erickson, K.I. Exercise effects on depression: Possible neural mechanisms. Gen. Hosp. Psychiatry 2017, 49, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Laird, A.R.; Fox, P.; Eickhoff, S.B.; Turner, J.; Ray, K.L.; McKay, D.R.; Glahn, D.C.; Beckmann, C.F.; Smith, S.M.; Fox, P.T. Behavioral Interpretations of Intrinsic Connectivity Networks. J. Cogn. Neurosci. 2011, 23, 4022–4037. [Google Scholar] [CrossRef] [PubMed]
- Köhler, S.; Ashton, C.H.; Marsh, R.; Thomas, A.J.; Barnett, N.A.; O’Brien, J.T. Electrophysiological changes in late life depression and their relation to structural brain changes. Int. Psychogeriatr. 2011, 23, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Kemp, A.H.; Griffiths, K.; Felmingham, K.L.; Shankman, S.A.; Drinkenburg, W.H.I.M.; Arns, M.; Clark, C.R.; Bryant, R.A. Dis-order specificity despite comorbidity: Resting EEG alpha asymmetry in major depressive disorder and post-traumatic stress disorder. Biol. Psychol. 2010, 85, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Jiang, H.; Bi, K.; Liu, C.; Yao, Z. Discriminative analysis with a limited number of MEG trials in depression. J. Affect. Disord. 2014, 167, 207–214. [Google Scholar] [CrossRef]
- Knott, V.; Mahoney, C.; Kennedy, S.; Evans, K. EEG power, frequency, asymmetry and coherence in male depression. Psychiatry Res. Neuroimaging 2001, 106, 123–140. [Google Scholar] [CrossRef]
- Ricardo-Garcell, J.; González-Olvera, J.J.; Miranda, E.; Harmony, T.; Reyes, E.; Almeida, L.; Galán, L.; Díaz, D.; Ramírez, L.; Fernández-Bouzas, A.; et al. EEG sources in a group of patients with major depressive disorders. Int. J. Psychophysiol. 2009, 71, 70–74. [Google Scholar] [CrossRef]
- Henz, D.; Schöllhorn, W.I. EEG Brain Activity in Dynamic Health Qigong Training: Same Effects for Mental Practice and Physical Training? Front. Psychol. 2017, 8, 154. [Google Scholar] [CrossRef][Green Version]
- Bailey, S.P.; Hall, E.E.; Folger, S.E.; Miller, P.C. Changes in EEG During Graded Exercise on a Recumbent Cycle Ergometer. J. Sports Sci. Med. 2008, 7, 505–511. [Google Scholar]
- Mulders, P.C.; van Eijndhoven, P.F.; Schene, A.H.; Beckmann, C.F.; Tendolkar, I. Resting-state functional connectivity in major depressive disorder: A review. Neurosci. Biobehav. Rev. 2015, 56, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Vogt, T.; Schneider, S.; Brümmer, V.; Strüder, H.K. Frontal EEG asymmetry: The effects of sustained walking in the elderly. Neurosci. Lett. 2010, 485, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Burcal, C.J.; Jeon, M.H.; Gonzales, M.J.M.; Faust, M.E.; Thomas, A.C.; Hubbard-Turner, T.J.; Wikstrom, E.A. Cortical Measures of Motor Planning and Balance Training in Patients with Chronic Ankle Instability. J. Athl. Train. 2019, 54, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Custo, A.; Van De Ville, D.; Wells, W.M.; Tomescu, M.I.; Brunet, D.; Michel, C.M. Electroencephalographic Resting-State Networks: Source Localization of Microstates. Brain Connect. 2017, 7, 671–682. [Google Scholar] [CrossRef] [PubMed]
- Villafaina, S.; Sitges, C.; Collado-Mateo, D.; Fuentes-García, J.P.; Gusi, N. Influence of depressive feelings in the brain processing of women with fibromyalgia: An EEG study. Medicine 2019, 98, e15564. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Ramautar, J.R.; Colombo, M.A.; Lindert, B.H.W.T.; Van Someren, E.J.W. EEG Microstates Indicate Heightened Somatic Awareness in Insomnia: Toward Objective Assessment of Subjective Mental Content. Front. Psychiatry 2018, 9, 395. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicators | HC | DC | EI |
|---|---|---|---|
| Sample size | 20 | 20 | 20 |
| Age (years) | 18–20 | 18–20 | 18–20 |
| BMI (kg/m2), mean (SD) | 22.05 ± 2.66 | 21.97 ± 1.88 | 22.26 ± 2.41 |
| Handedness, left/right | 0/20 | 0/20 | 0/20 |
| Mother’s education level | (UG = 7; HS = 9; MS = 4) | (UG = 3; HS = 9; MS = 6; PS = 2) | (UG = 4; HS = 9; MS = 6; PS = 1) |
| Father’s education level | (UG = 9; HS = 11) | (UG = 5; HS = 7; MS = 7; PS = 1) | (UG = 7; HS = 8; MS = 5) |
| Family patterns | (PF = 18; SPF = 1; EF = 1) | (PF = 13; SPF = 4; EF = 3) | (PF = 15; SPF = 3; EF = 2) |
| Rearing patterns | (PR = 16; MR = 3; FR = 1) | (PR = 11; MR = 5; FR = 1; GR = 3) | (PR = 13; MR = 4; GR = 3) |
| NBV, times | 0.42 ± 0.51 | 3.96 ± 2.07 | 3.17 ± 2.73 |
| Parameters | HC (n = 20) | DC (n = 20) | EI (n = 20) | Cohen’s d | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | HC vs. DC | HC vs. EI | DC vs. EI | |
| Total Time (s) | 55.480 | 3.196 | 58.524 | 5.778 | 60.101 | 6.281 | −0.652 | −0.927 | −0.261 |
| Duration (s) | |||||||||
| A | 0.073 | 0.005 | 0.069 | 0.006 | 0.071 | 0.004 | 0.724 | 0.442 | −0.392 |
| B | 0.069 | 0.007 | 0.067 | 0.007 | 0.068 | 0.004 | 0.286 | 0.175 | −0.175 |
| C | 0.070 | 0.002 | 0.068 | 0.002 ** | 0.069 | 0.001# | 1.000 | 0.632 | −0.632 |
| D | 0.068 | 0.006 | 0.063 | 0.007 | 0.064 | 0.003 | 0.614 | 0.614 | −0.186 |
| Mean Duration | 0.070 | 0.003 | 0.067 | 0.004 * | 0.068 | 0.061 | 0.849 | 0.046 | −0.023 |
| Occurrence | |||||||||
| A | 3.649 | 0.179 | 3.700 | 0.266 | 3.760 | 0.049 | −0.225 | −0.225 | −0.314 |
| B | 3.474 | 0.314 | 3.922 | 0.229 ** | 3.716 | 0.140# | −1.630 | −0.995 | 1.085 |
| C | 3.840 | 0.371 | 3.597 | 0.326 | 3.837 | 0.241 | 0.696 | 0.010 | −0.102 |
| D | 3.593 | 0.240 | 3.805 | 0.213 * | 3.727 | 0.533 | −0.934 | −0.324 | 0.192 |
| Mean Occurrence | 14.556 | 0.583 | 15.024 | 0.677 * | 15.041 | 0.475 | −0.741 | −0.912 | −0.029 |
| Contribution (%) | |||||||||
| A | 0.260 | 0.054 | 0.252 | 0.051 | 0.259 | 0.057 | 0.152 | 0.018 | −0.129 |
| B | 0.239 | 0.047 | 0.263 | 0.042 | 0.242 | 0.040 | −0.538 | −0.069 | 0.512 |
| C | 0.248 | 0.048 | 0.259 | 0.054 | 0.287 | 0.072 | −0.215 | −0.637 | −0.440 |
| D | 0.254 | 0.034 | 0.213 | 0.056 * | 0.227 | 0.035 | 0.885 | 0.783 | 0.300 |
| Bands | Groups | Duration | Occurrence | Contribution | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | C | D | A | B | C | D | A | B | C | D | ||
| δ | HC | 0.430 | −0.376 | 0.091 | −0.233 | 0.084 | 0.202 | 0.250 | −0.109 | 0.009 | 0.221 | −0.420 | 0.280 |
| DC | −0.122 | −0.044 | −0.007 | 0.191 | −0.440 | −0.331 | 0.016 | −0.122 | −0.171 | −0.578 * | 0.604 * | 0.023 | |
| EI | −0.437 | 0.011 | 0.357 | −0.134 | 0.161 | 0.057 | −0.842 * | −0.161 | −0.196 | −0.467 | 0.286 | 0.165 | |
| θ | HC | 0.406 | −0.134 | −0.254 | −0.203 | −0.154 | 0.346 | −0.083 | −0.270 | −0.071 | 0.364 | −0.003 | −0.388 |
| DC | −0.564 * | 0.150 | 0.478 | 0.196 | −0.569 * | −0.485 | −0.399 | −0.587 * | −0.509 | −0.402 | 0.650 ** | 0.228 | |
| EI | −0.026 | 0.262 | −0.379 | −0.220 | 0.312 | −0.176 | −0.703 | −0.289 | −0.125 | −0.510 | 0.624 | −0.304 | |
| α | HC | 0.470 | −0.340 | −0.240 | −0.416 | 0.412 | 0.391 | 0.027 | −0.242 | −0.382 | 0.554 * | −0.293 | 0.263 |
| DC | −0.354 | −0.068 | 0.006 | −0.235 | −0.522 | 0.193 | −0.034 | 0.080 | −0.337 | −0.118 | 0.547 * | −0.203 | |
| EI | −0.572 | 0.160 | 0.328 | 0.112 | −0.032 | 0.084 | −0.885 ** | 0.036 | −0.451 | −0.430 | 0.484 | 0.148 | |
| β | HC | 0.213 | −0.162 | 0.066 | −0.036 | 0.024 | −0.025 | −0.107 | 0.296 | −0.027 | −0.445 | 0.389 | 0.106 |
| DC | −0.471 | −0.222 | −0.071 | −0.207 | −0.196 | −0.038 | −0.318 | 0.319 | 0.065 | 0.041 | 0.039 | −0.201 | |
| EI | −0.577 | −0.189 | 0.900 ** | 0.026 | −0.042 | −0.080 | 0.323 | −0.101 | 0.303 | −0.008 | −0.176 | −0.079 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, A.; Zhao, S.; Song, J.; Zhang, Y.; Zhang, Y.; Niu, X.; Xiao, T.; Chi, A. Treatment Effect of Exercise Intervention for Female College Students with Depression: Analysis of Electroencephalogram Microstates and Power Spectrum. Sustainability 2021, 13, 6822. https://doi.org/10.3390/su13126822
Liang A, Zhao S, Song J, Zhang Y, Zhang Y, Niu X, Xiao T, Chi A. Treatment Effect of Exercise Intervention for Female College Students with Depression: Analysis of Electroencephalogram Microstates and Power Spectrum. Sustainability. 2021; 13(12):6822. https://doi.org/10.3390/su13126822
Chicago/Turabian StyleLiang, Andi, Shanguang Zhao, Jing Song, Yan Zhang, Yue Zhang, Xiaodan Niu, Tao Xiao, and Aiping Chi. 2021. "Treatment Effect of Exercise Intervention for Female College Students with Depression: Analysis of Electroencephalogram Microstates and Power Spectrum" Sustainability 13, no. 12: 6822. https://doi.org/10.3390/su13126822
APA StyleLiang, A., Zhao, S., Song, J., Zhang, Y., Zhang, Y., Niu, X., Xiao, T., & Chi, A. (2021). Treatment Effect of Exercise Intervention for Female College Students with Depression: Analysis of Electroencephalogram Microstates and Power Spectrum. Sustainability, 13(12), 6822. https://doi.org/10.3390/su13126822