Effect of a Service-Learning Program on the Active Lifestyle of Children with Autism Spectrum Disorder: A Pilot Study

 ,
,  , and
, and 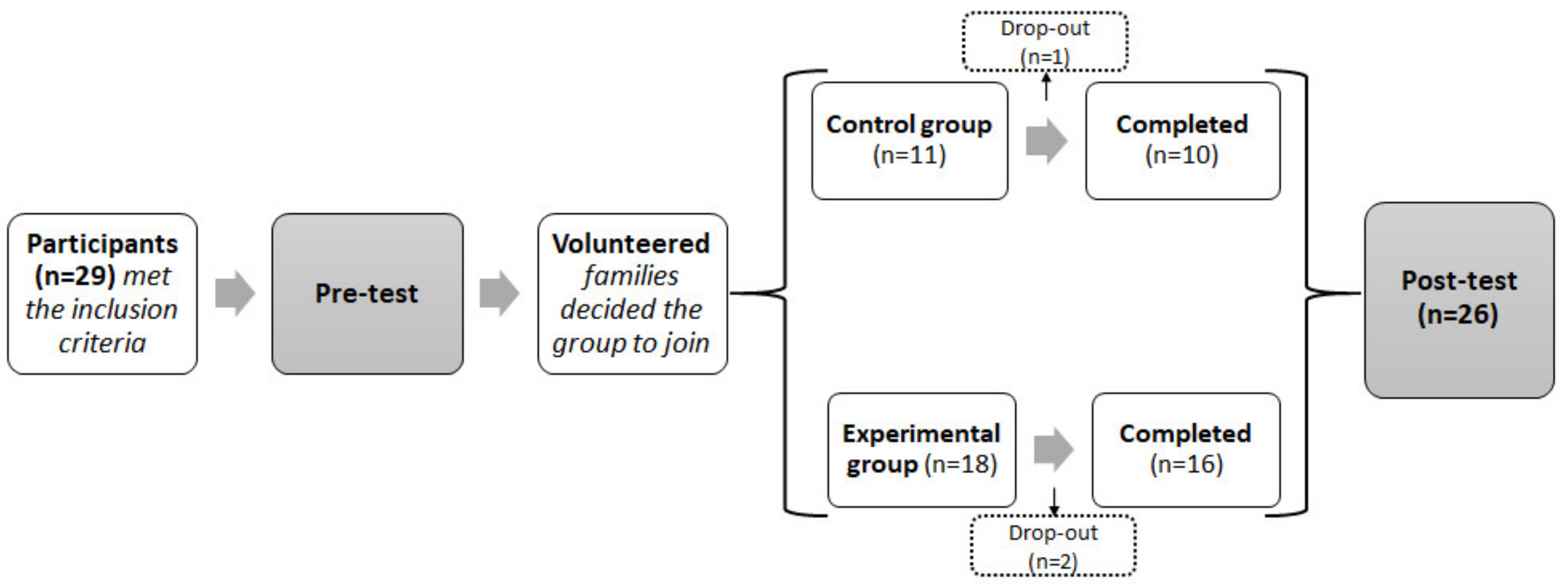{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methodology
2.1. Design
2.2. Sample
2.3. Intervention Program
2.4. Materials and Procedure
2.5. Physical Activity Data Reduction
2.6. Data Analysis
2.7. Ethical Considerations
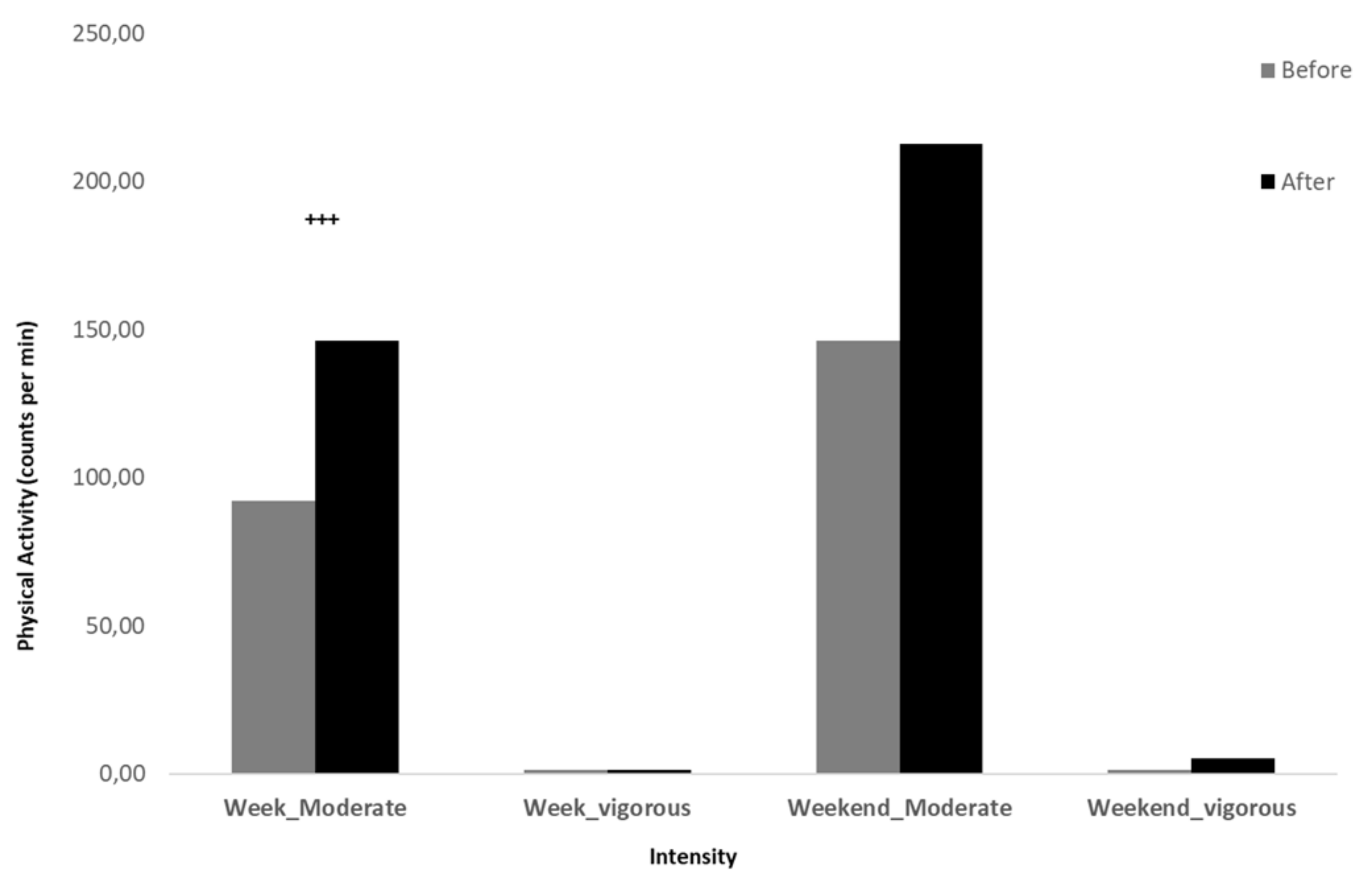
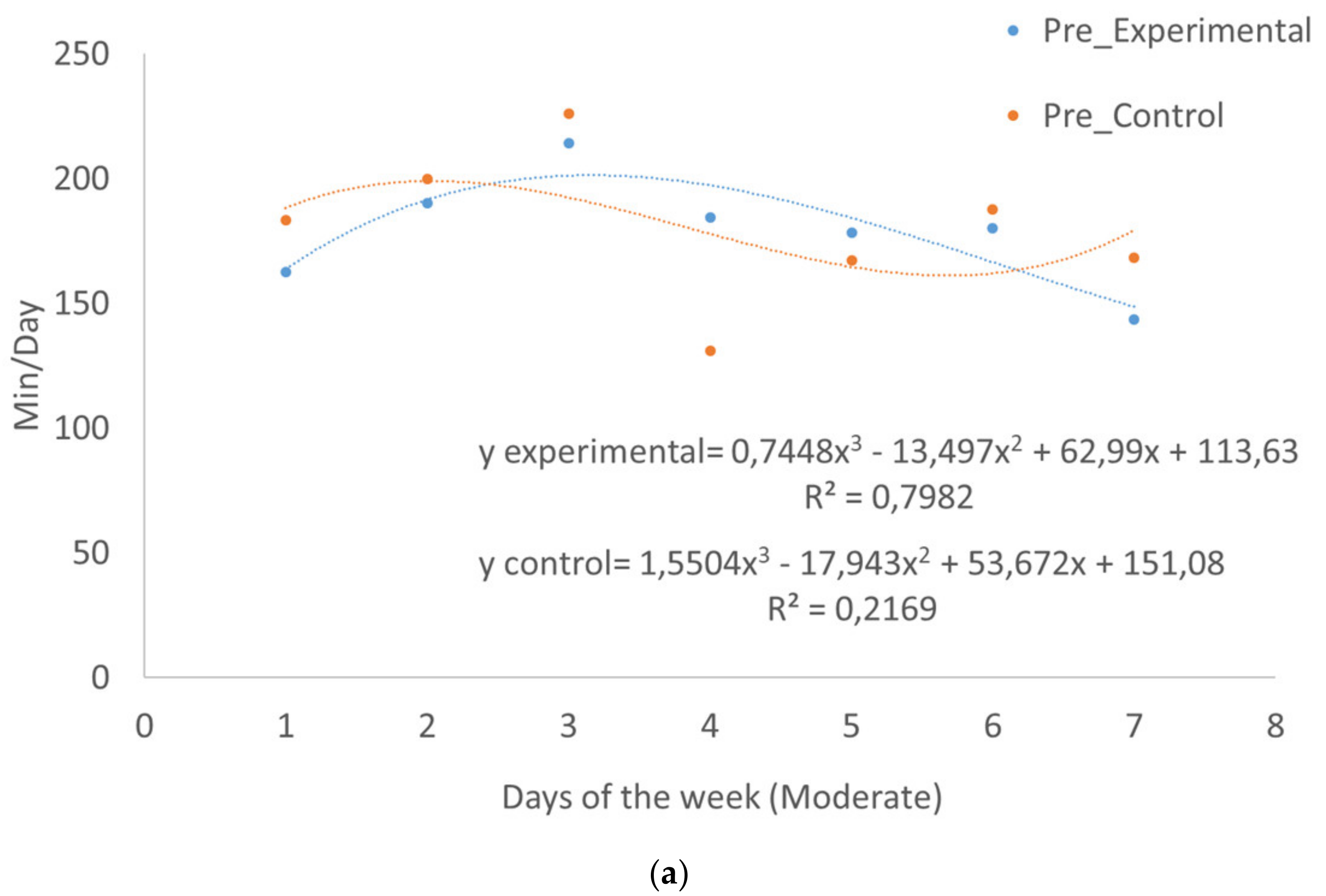
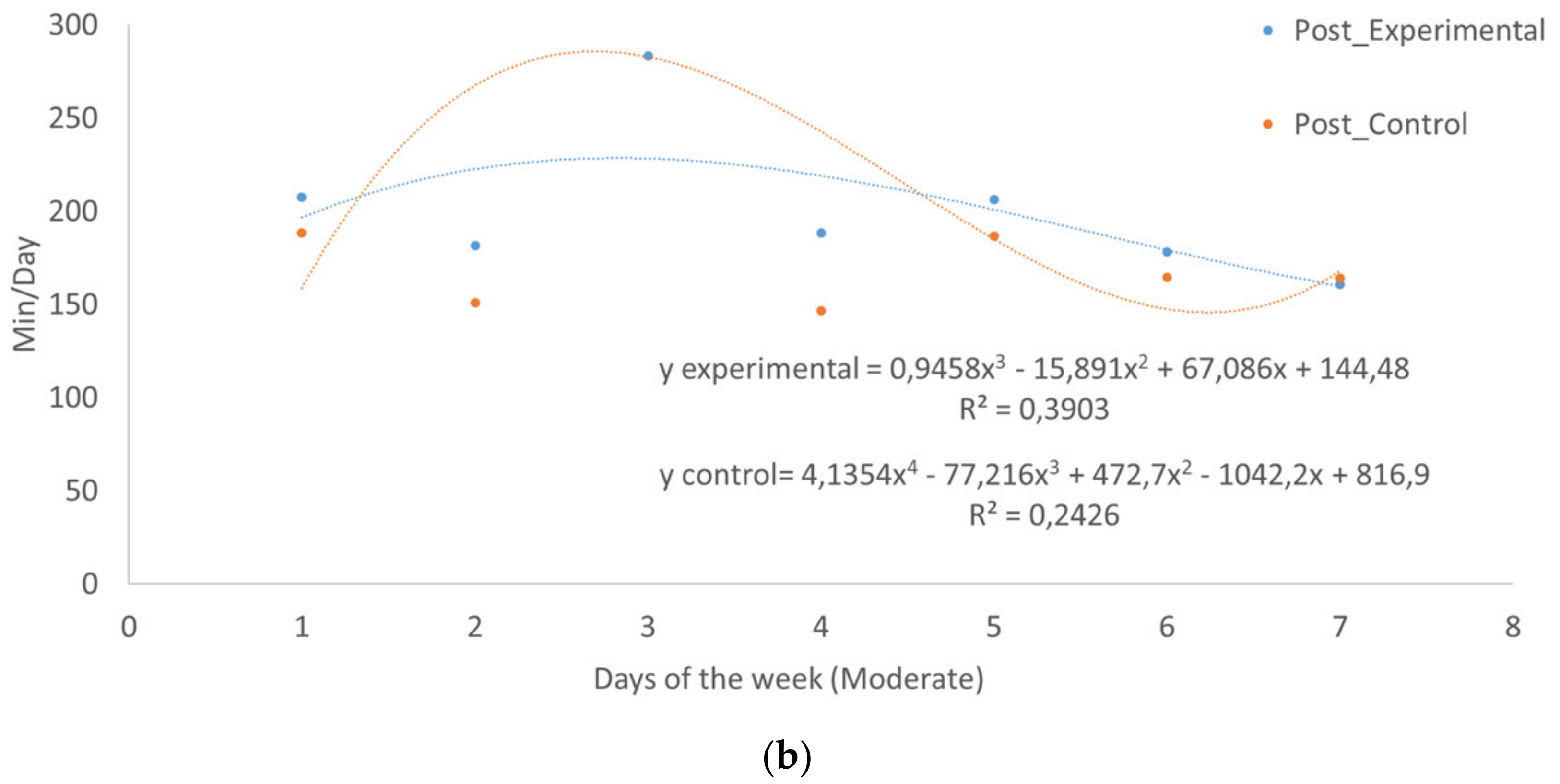
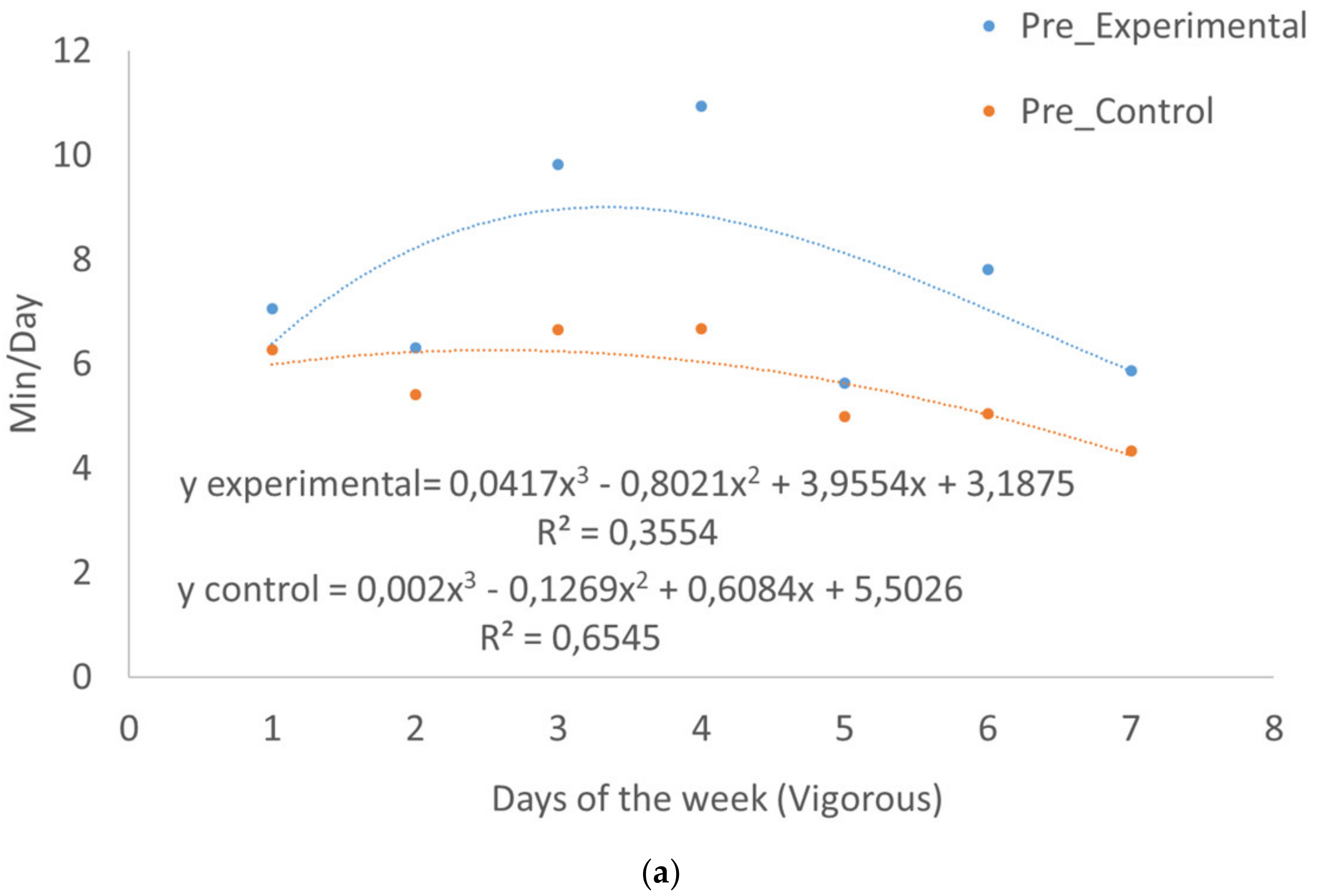
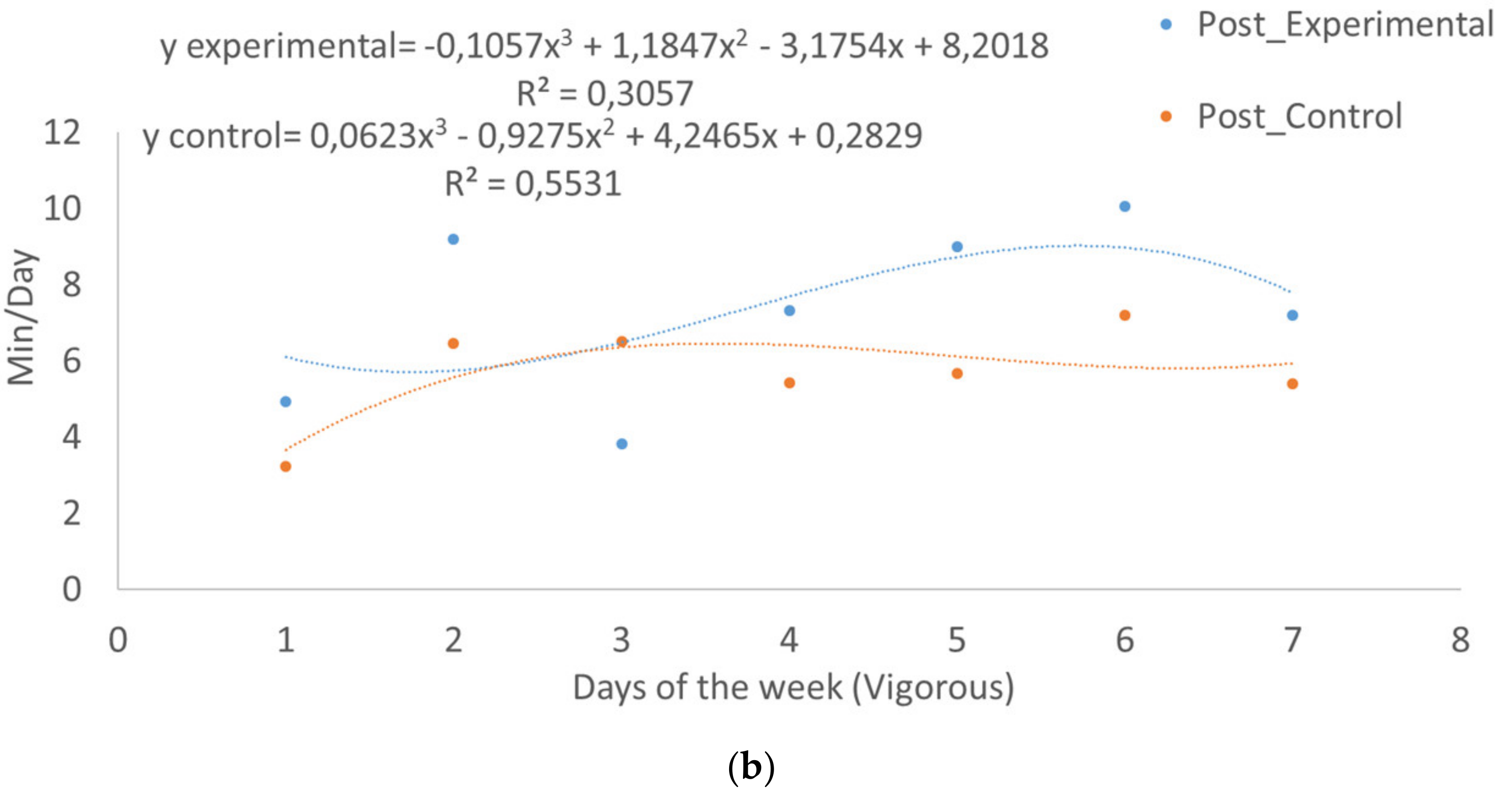
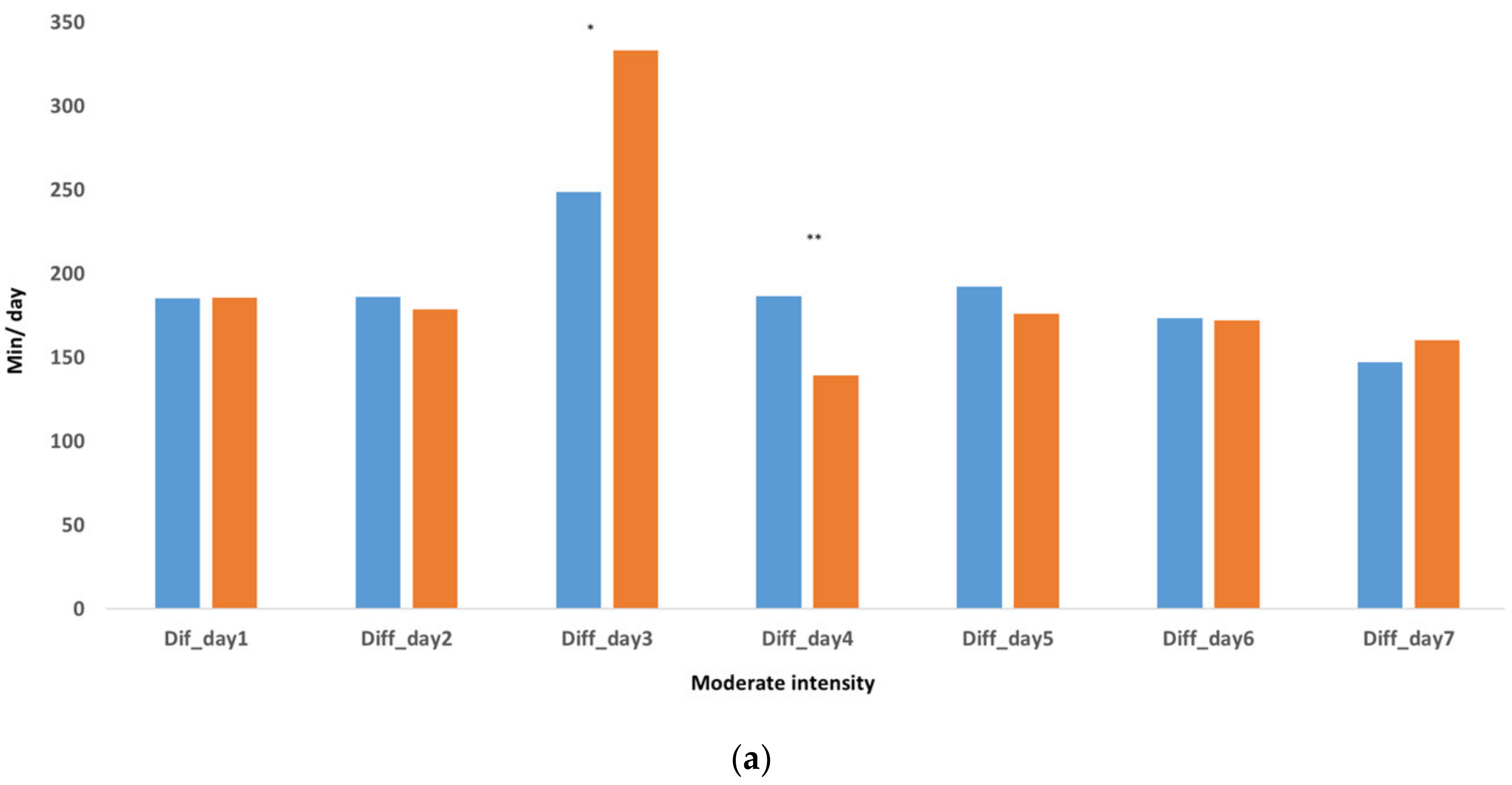
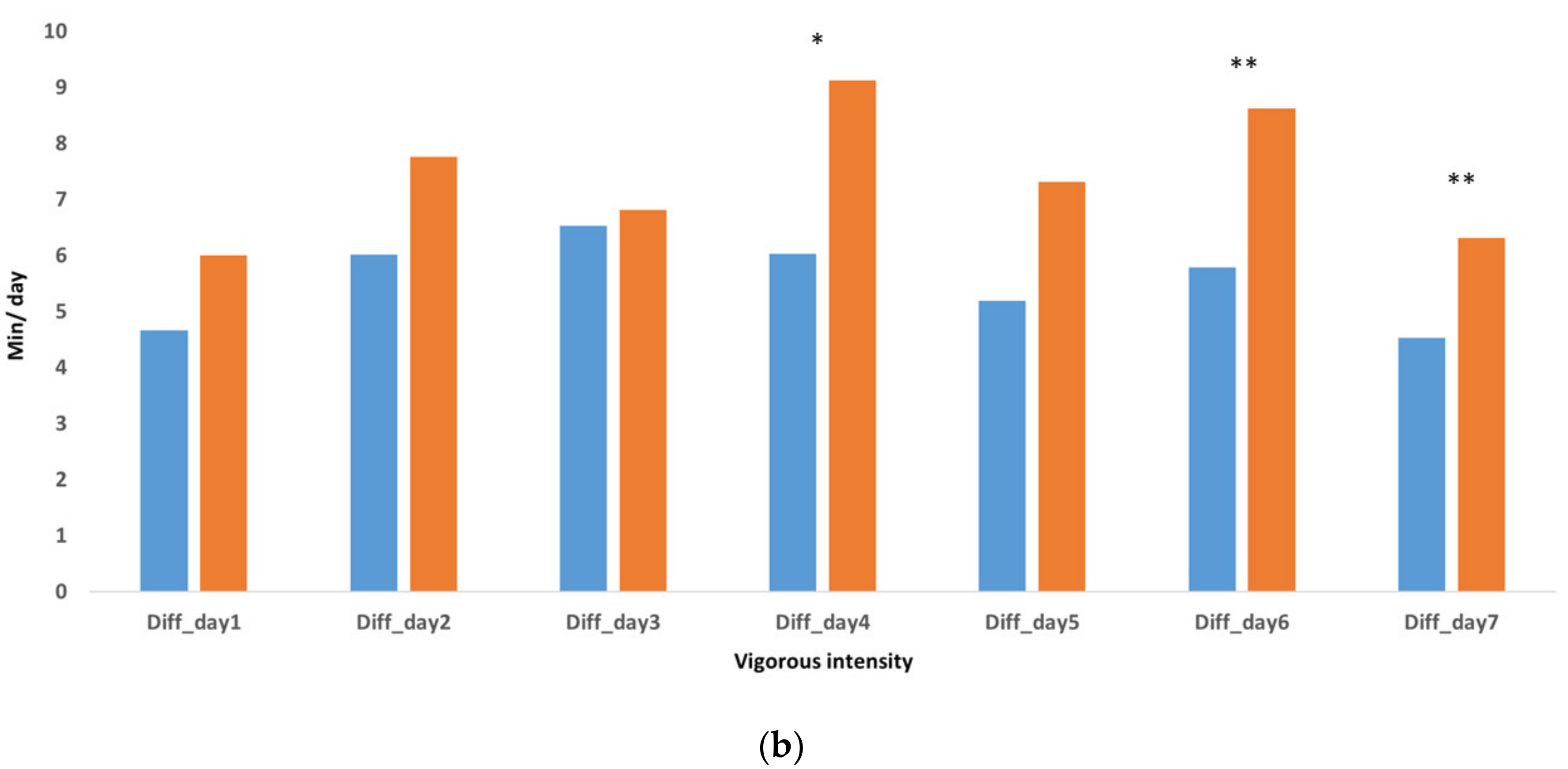
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The World Health Report 2000: Health Systems: Improving Performance; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-García, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V.; et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: A systematic review and meta-analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef]
- Sallis, J.F. Measuring physical activity environments: A brief history. Am. J. Prev. Med. 2009, 36, S86–S92. [Google Scholar] [CrossRef] [PubMed]
- Acree, L.S.; Longfors, J.; Fjeldstad, A.S.; Fjeldstad, C.; Schank, B.; Nickel, K.J.; Montgomery, P.S.; Gardner, A. Physical activity is related to quality of life in older adults. Health Qual. Life Outcomes 2006, 4, 37. [Google Scholar]
- Molina-García, J.; Castillo, I.; Queralt, A.; Sallis, J.F. Bicycling to university: Evaluation of a bicycle-sharing program in Spain. Health Promot. Int. 2015, 30, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Pulgaron, E.R.; Delamater, A.M. Obesity and type 2 diabetes in children: Epidemiology and treatment. Curr. Diabetes Rep. 2014, 14, 508. [Google Scholar] [CrossRef] [PubMed]
- Bauminger, N.; Kasari, C. Loneliness and friendship in high-functioning children with autism. Child Dev. 2000, 71, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Bauminger, N.; Shulman, C.; Agam, G. Peer interaction and loneliness in high-functioning children with autism. J. Autism Dev. Disord. 2003, 33, 489–507. [Google Scholar] [CrossRef]
- Llewellyn, A.; Hogan, K. The use and abuse of models of disability. Disabil. Soc. 2000, 15, 157–165. [Google Scholar] [CrossRef]
- DiSalvo, C.A.; Oswald, D.P. Peer-mediated interventions to increase the social interaction of children with autism: Consideration of peer expectancies. Focus Autism Other Dev. Disabil. 2002, 17, 198–207. [Google Scholar] [CrossRef]
- Kamps, D.M.; Barbetta, P.M.; Leonard, B.R.; Delquadri, J. Classwide peer tutoring: An integration strategy to improve reading skills and promote peer interactions among students with autism and general education peers. J. Appl. Behav. Anal. 1994, 27, 49–61. [Google Scholar] [CrossRef]
- Memari, A.H.; Ghaheri, B.; Ziaee, V.; Kordi, R.; Hafizi, S.; Moshayedi, P. Physical activity in children and adolescents with autism assessed by triaxial accelerometry. Pediatr. Obes. 2013, 8, 150–158. [Google Scholar] [CrossRef]
- Pan, C.Y.; Frey, G.C. Identifying physical activity determinants in youth with autistic spectrum disorders. J. Phys. Act. Health 2005, 2, 412–422. [Google Scholar] [CrossRef]
- Schultheis, S.F.; Boswell, B.B.; Decker, J. Successful physical activity program-ming for students with autism. Focus Autism Other Dev. Disabil. 2000, 15, 159–162. [Google Scholar] [CrossRef]
- Obrusnikova, I.; Miccinello, D.L. Parent perceptions of factors influencing after-school physical activity of children with autism spectrum disorders. Adapt. Phys. Act. Q. 2012, 29, 63–80. [Google Scholar] [CrossRef]
- Sandt DD, R.; Frey, G.C. Comparison of physical activity levels between children with and without autistic spectrum disorders. Adapt. Phys. Act. Q. 2005, 22, 146–159. [Google Scholar] [CrossRef]
- Weiss, M.J.; Harris, S.L. Teaching social skills to people with autism. Behav. Modif. 2001, 25, 785–802. [Google Scholar] [CrossRef]
- Lord, C.; Cook, E.H.; Leventhal, B.L.; Amaral, D.G. Autism spectrum disorders. Neuron 2000, 28, 355–363. [Google Scholar] [CrossRef]
- Rosenthal-Malek, A.; Mitchell, S. Brief report: The effects of exercise on the self-stimulatory behaviours and positive responding of adolescents with autism. J. Autism Dev. Disord. 1997, 27, 193–202. [Google Scholar] [CrossRef]
- Houwen, S.; Hartman, E.; Visscher, C. Physical activity and motor skills in children with and without visual impairments. Med. Sci. Sports Exerc. 2009, 41, 103–109. [Google Scholar] [CrossRef]
- Fogel, A. Developing through Relationships; University of Chicago Press: Chicago, IL, USA, 1993. [Google Scholar]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Nyström, C.D.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Bandini, L.G.; Gleason, J.; Curtin, C.; Lividini, K.; E Anderson, S.; A Cermak, S.; Maslin, M.; Must, A. Comparison of physical activity between children with autism spectrum disorders and typically developing children. Autism 2013, 17, 44–54. [Google Scholar] [CrossRef]
- MacDonald, M.; Esposito, P.; Ulrich, D. The physical activity patterns of children with autism. BMC Res. Notes 2011, 4, 422. [Google Scholar] [CrossRef]
- Pan, C.Y.; Tsai, C.L.; Hsieh, K.W.; Chu, C.H.; Li, Y.L.; Huang, S.T. Accelerometer-determined physical activity among elementary school-aged children with autism spectrum disorders in Taiwan. Res. Autism Spectr. Disord. 2011, 5, 1042–1052. [Google Scholar] [CrossRef]
- Wali, L.J.; Sanfilippo, F. A Review of the State-of-the-Art of Assistive Technology for People with ASD in the Workplace and in Everyday Life. In Proceedings of the 18th IFIP Conference on e-Business, e-Services, and e-Society, Trondheim, Norway, 18–20 September 2019; Springer: Cham, Switzerland, 2019; pp. 520–533. [Google Scholar]
- Carson Russell, L.; Raguse, A. Systematic Review of Service-Learning in Youth Physical Activity Settings. Quest 2014, 66, 57–95. [Google Scholar] [CrossRef]
- Cervantes, C.; Karen, M. Examining Service-Learning Literature in Physical Education Teacher Education: Recommendations for Practice and Research. Quest 2013, 65, 332–353. [Google Scholar] [CrossRef]
- Chiva-Bartoll, O.; Ruiz-Montero, P.; Martín Moya, R.; Pérez López, I.; Giles Girela, J.; García-Suárez, J.; Rivera-García, E. University Service-Learning in Physical Education and Sport Sciences: A systematic review. Rev. Complut. Educ. 2019, 30, 1147–1164. [Google Scholar] [CrossRef]
- Meaney, K.S.; Bohler, H.R.; Kopf, K.; Hernandez, L.; Scott, L.S. Service-Learning and Pre-Service Educators’ Cultural Competence for Teaching: An Exploratory Study. J. Exp. Educ. 2008, 31, 189–208. [Google Scholar] [CrossRef]
- Meaney, K.S.; Hart, M.A.; Griffin, K.L. Fun & Fit, Phase I: A program for overweight African American and Hispanic American children from low–income families. J. Phys. Educ. Recreat. Dance 2009, 80, 35–39. [Google Scholar] [CrossRef]
- Capella-Peris, C.; Gil-Gómez, J.; Chiva-Bartoll, Ò. Innovative Analysis of Service-Learning Effects in Physical Education: A Mixed-Methods Approach. J. Teach. Phys. Educ. 2020, 1, 102–110. [Google Scholar] [CrossRef]
- American Psychiatric Association [APA]. Diagnostic and Statistical Manual-Text Revision (DSM-IV-TR); American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- American Psychiatric Association [APA]. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Chiva-Bartoll, O.; Capella-Peris, C.; Salvador-García, C. Service-learning in physical education teacher education: Towards a critical and inclusive perspective. J. Educ. Teach. 2020, 46, 1–13. [Google Scholar] [CrossRef]
- Troiano, R.; Berrigan, D.; Dodd, K.; Masse, L.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- WMA Declaration of Helsinki -Ethical Principles for Medical Research Involving Human Subjects. Available online: http://www.wma.net/en/30publications/10policies/b3/index.html (accessed on 1 July 2016).
- Hamm, J.; Yun, J. Influence of physical activity on the health-related quality of life of young adults with and without autism spectrum disorder. Disabil. Rehabil. 2019, 41, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.A.; Downing, K.L.; Rinehart, N.J.; Barnett, L.M.; May, T.; McGillivray, J.; Papadopoulos, N.; Skouteris, H.; Timperio, A.; Hinkley, T. Physical activity, sedentary behavior and their correlates in children with Autism Spectrum Disorder: A systematic review. PLoS ONE 2017, 12, e0172482. [Google Scholar] [CrossRef] [PubMed]
- Reinders, N.J.; Branco, A.; Wright, K.; Fletcher, P.C.; Bryden, P.J. Scoping review: Physical activity and social functioning in young people with autism spectrum disorder. Front. Psychol. 2019, 10, 120. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Hinkley, T.; Barnett, L.M.; May, T.; Rinehart, N. Young children with ASD participate in the same level of physical activity as children without ASD: Implications for early intervention to maintain good health. J. Autism Dev. Disord. 2019, 49, 3278–3289. [Google Scholar] [CrossRef]
- Garcia, J.M.; Leahy, N.; Rivera, P.; Renziehausen, J.; Samuels, J.; Fukuda, D.H.; Stout, J.R. Brief Report: Preliminary Efficacy of a Judo Program to Promote Participation in Physical Activity in Youth with Autism Spectrum Disorder. J. Autism Dev. Disord. 2019, 50, 1–7. [Google Scholar] [CrossRef]
- Ledford, J.R.; Lane, J.D.; Shepley, C.; Kroll, S.M. Using teacher-implemented playground interventions to increase engagement, social behaviors, and physical activity for young children with autism. Focus Autism Other Dev. Disabil. 2016, 31, 163–173. [Google Scholar] [CrossRef]
- Jeong, I.; Ryu, D.S. Comparison of physical activity between youth with down syndrome and youth with autism spectrum disorders. 한국체육과학회지 2019, 28, 1073–1084. [Google Scholar]
- Stanish, H.I.; Curtin, C.; Must, A.; Phillips, S.; Maslin, M.; Bandini, L.G. Physical activity levels, frequency, and type among adolescents with and without autism spectrum disorder. J. Autism Dev. Disord. 2017, 47, 785–794. [Google Scholar] [CrossRef]
- Garcia-Pastor, T.; Salinero, J.J.; Theirs, C.I.; Ruiz-Vicente, D. Obesity status and physical activity level in children and adults with autism spectrum disorders: A pilot study. J. Autism Dev. Disord. 2019, 49, 165–172. [Google Scholar] [CrossRef]
- WHO (World Health Organization). Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020. 2013. Available online: http://www.who.int/mediacentre/factsheets/fs385/es/ (accessed on 21 May 2020).
- Tyler, K.; MacDonald, M.; Menear, K. Physical activity and physical fitness of school-aged children and youth with autism spectrum disorders. Autism Res. Treat. 2014, 2014, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Healy, S.; Carrie, J.A.; Justin, A.H.; Patterson, F. Meeting the 24-hr movement guidelines: An update on US youth with autism spectrum disorder from the 2016 National Survey of Children’s Health. Autism Res. 2019, 12, 941–951. [Google Scholar] [CrossRef] [PubMed]
- Ketcheson, L.; Hauck, J.; Ulrich, D. The effects of an early motor skill intervention on motor skills, levels of physical activity, and socialization in young children with autism spectrum disorder: A pilot study. Autism 2017, 21, 481–492. [Google Scholar] [CrossRef]
- Bo, J.; Pang, Y.; Dong, L.; Xing, Y.; Xiang, Y.; Zhang, M.; Wright, M.; Shen, B. Brief Report: Does Social Functioning Moderate the Motor Outcomes of a Physical Activity Program for Children with Autism Spectrum Disorders-A Pilot Study. J. Autism Dev. Disord. 2019, 49, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, W.A.; Bell, P. Design-based research methods for studying learning in context: Introduction. Educ. Psychol. 2004, 39, 199–201. [Google Scholar] [CrossRef]








© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valverde-Esteve, T.; Chiva-Bartoll, O.; Salvador-García, C.; Maravé-Vivas, M. Effect of a Service-Learning Program on the Active Lifestyle of Children with Autism Spectrum Disorder: A Pilot Study. Sustainability 2020, 12, 4354. https://doi.org/10.3390/su12114354
Valverde-Esteve T, Chiva-Bartoll O, Salvador-García C, Maravé-Vivas M. Effect of a Service-Learning Program on the Active Lifestyle of Children with Autism Spectrum Disorder: A Pilot Study. Sustainability. 2020; 12(11):4354. https://doi.org/10.3390/su12114354
Chicago/Turabian StyleValverde-Esteve, Teresa, Oscar Chiva-Bartoll, Celina Salvador-García, and María Maravé-Vivas. 2020. "Effect of a Service-Learning Program on the Active Lifestyle of Children with Autism Spectrum Disorder: A Pilot Study" Sustainability 12, no. 11: 4354. https://doi.org/10.3390/su12114354
APA StyleValverde-Esteve, T., Chiva-Bartoll, O., Salvador-García, C., & Maravé-Vivas, M. (2020). Effect of a Service-Learning Program on the Active Lifestyle of Children with Autism Spectrum Disorder: A Pilot Study. Sustainability, 12(11), 4354. https://doi.org/10.3390/su12114354