Anxiety and Bodily Pain in Older Women Participants in a Physical Education Program. A Multiple Moderated Mediation Analysis

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
- Sociodemographic characteristics
- Health-related Quality of life by the SF-36 Health Survey (SF-36)
- Pain coping strategies by Vanderbilt Pain Management Inventory (VPMI)
- Anxiety by Hospital Anxiety and Depression Scale (HADS)
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Anxiety, Passive and Active strategies, the Physical Component, and Bodily Pain
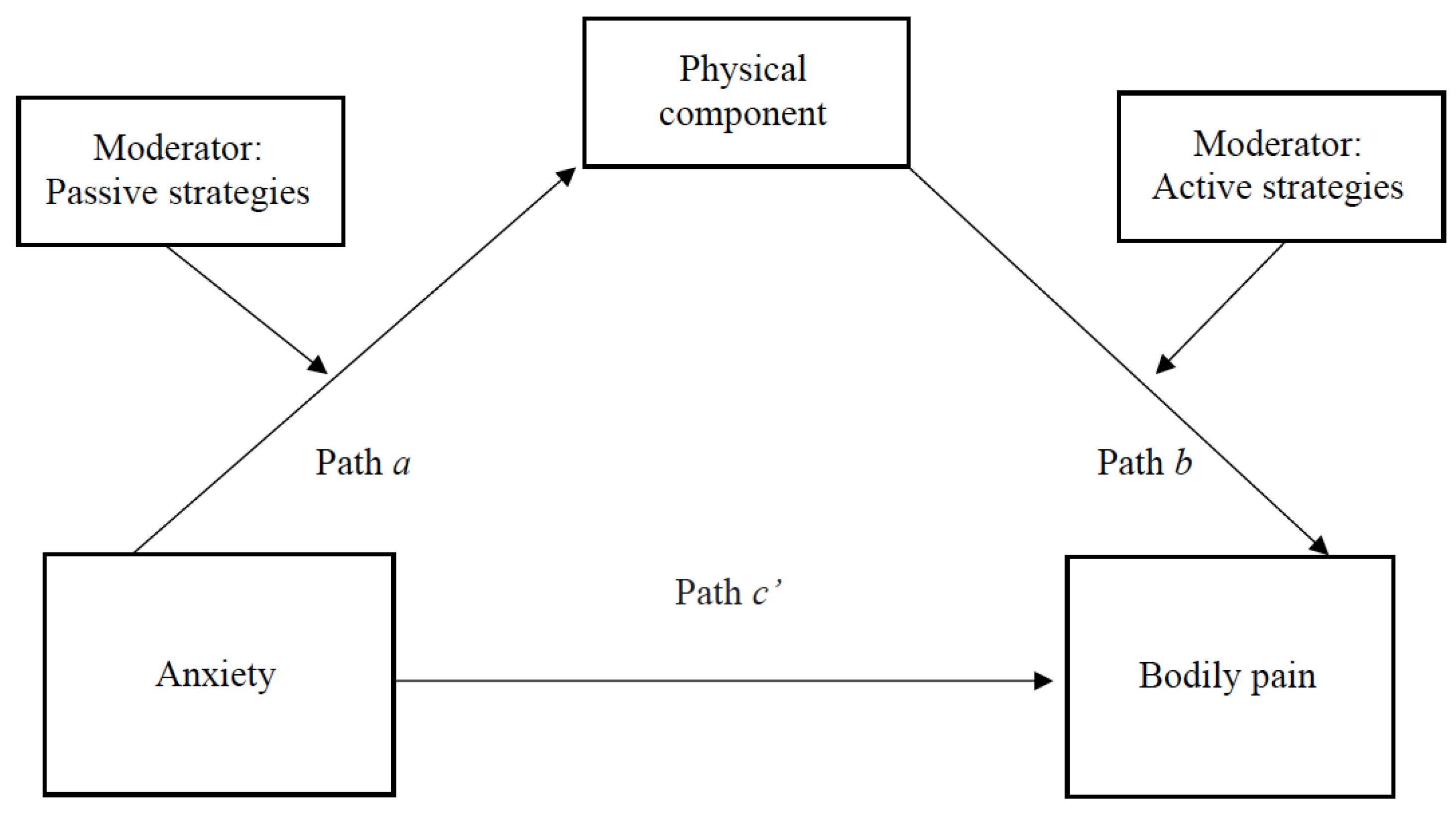
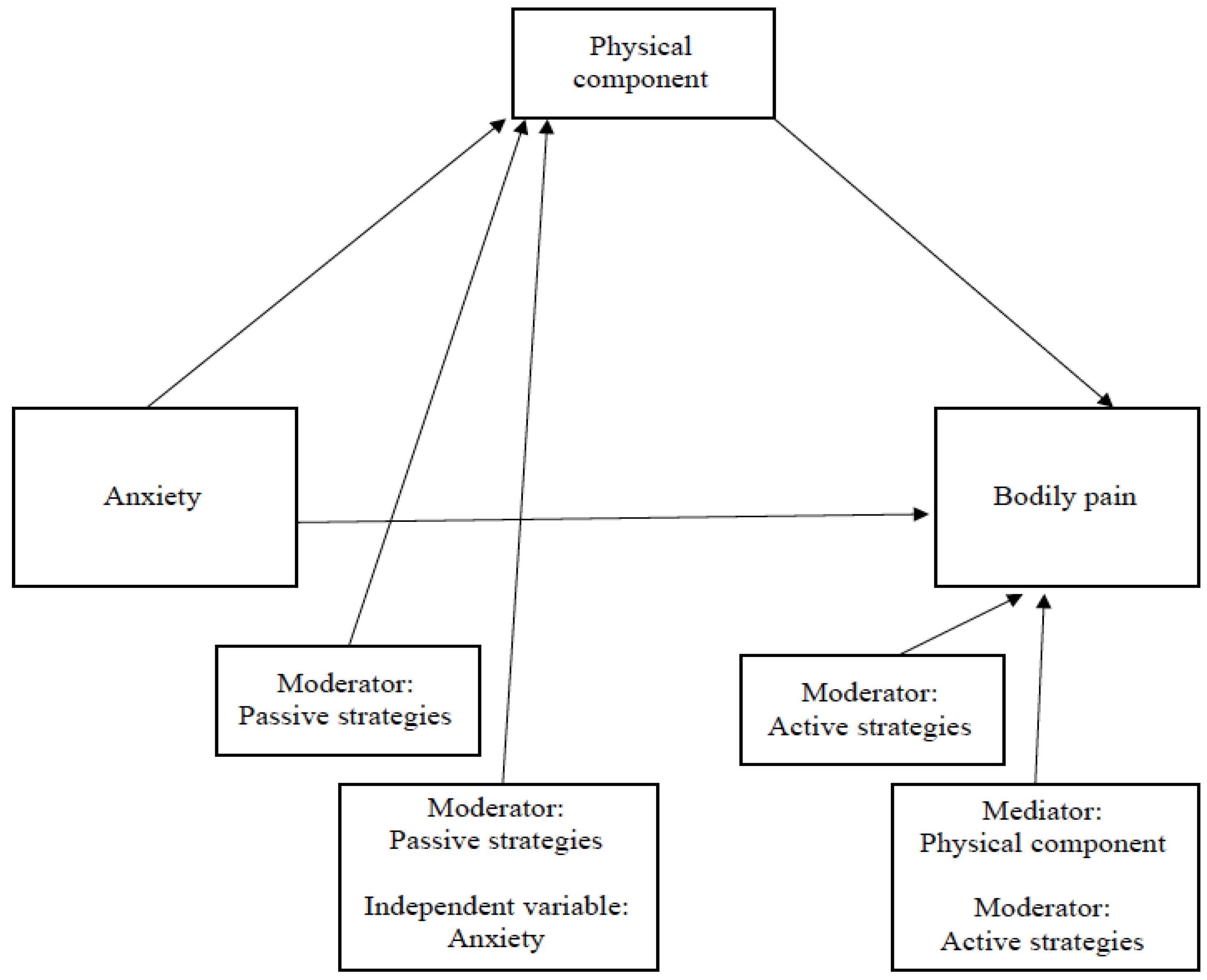
3.2. Results of the Multiple Moderated Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lochner, K.A.; Shoff, C.M. County-level variation in prevalence of multiple chronic conditions among Medicare beneficiaries, 2012. Prev. Chronic. Dis. 2015, 12, E07. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Koroukian, S.M.; Schiltz, N.; Warner, D.F.; Sun, J.; Bakaki, P.M.; Smyth, K.A.; Stange, K.C.; Given, C.W. Combinations of Chronic Conditions, Functional Limitations, and Geriatric Syndromes that Predict Health Outcomes. J. Gen. Intern. Med. 2016, 31, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Onetti-Onetti, W.; Castillo-Rodríguez, C.L.; Castillo-Rodríguez, C. Assessment of elderly people characteristics and their relationship with the perceived quality of sport management. Rev. Iberoam. Ciencias Act. Física Deport. 2018, 8, 110–118. [Google Scholar]
- Ruiz-Montero, P.J.; Ruiz-Rico Ruiz, G.J.; Martín-Moya, R.; González-Matarín, P.J. Do health-related quality of life and pain-coping strategies explain the relationship between older women participants in a pilates-aerobic program and bodily pain? A multiple mediation model. Int. J. Environ. Res. Public Health 2019, 16, 3249. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Montero, P.J.; Castillo-Rodriguez, A.; Mikalacki, M.; Delgado-Fernandez, M. Physical Fitness Comparison and Quality of Life between Spanish and Serbian Elderly Women through a Physical Fitness Program. Coll. Antropol. 2015, 39, 411–417. [Google Scholar] [PubMed]
- Rubio, L.; Dumitrache, C.G.; García, A.J.; Cordón-Pozo, E. Coping strategies in Spanish older adults: A MIMIC model of socio-demographic characteristics and activity level. Aging Ment. Health 2018, 22, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Roh, H.W.; Lee, Y.; Lee, K.; Chang, K.; Jinhee, K.; Lee, S.; Back, J.; Chung, Y.K.; Lim, K.; Noh, J.; et al. Frequency of contact with non-cohabitating adult children and risk of depression in elderly: A community-based three-year longitudinal study in Korea. Arch. Gerontol. Geriatr. 2014, 60, 183–189. [Google Scholar] [CrossRef]
- Morone, N.E.; Greco, C.M. Mind-body interventions for chronic pain in older adults: A structured review. Pain Med. 2007, 8, 359–375. [Google Scholar] [CrossRef]
- Helme, R.D.; Gibson, S.J. The epidemiology of pain in elderly people. Clin. Geriatr. Med. 2001, 17, 417–431. [Google Scholar] [CrossRef]
- Castillo, R.C.; Wegener, S.T.; Heins, S.E.; Haythornthwaite, J.A.; Mackenzie, E.J.; Bosse, M.J. Longitudinal relationships between anxiety, depression, and pain: Results from a two-year cohort study of lower extremity trauma patients. Pain 2013, 154, 2860–2866. [Google Scholar] [CrossRef]
- Novotny, S.A.; Warren, G.L.; Hamrick, M.W. Aging and the muscle-bone relationship. Physiology 2015, 30, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.G.; Alvarelhao, J.; Queiros, A.; Rocha, N.P. Pain intensity is associated with self-reported disability for several domains of life in a sample of patients with musculoskeletal pain aged 50 or more. Disabil. Health J. 2013, 6, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Ikezoe, T.; Asakawa, Y.; Shima, H.; Kishibuchi, K.; Ichihashi, N. Daytime physical activity patterns and physical fitness in institutionalized elderly women: An exploratory study. Arch. Gerontol. Geriatr. 2013, 57, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Johannes, C.B.; Le, T.K.; Zhou, X.; Johnston, J.A.; Dworkin, R.H. The prevalence of chronic pain in United States adults: Results of an Internet-based survey. J. Pain 2010, 11, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Gerino, E.; Rolle, L.; Sechi, C.; Brustia, P. Loneliness, Resilience, Mental Health, and Quality of Life in Old Age: A Structural Equation Model. Front. Psychol. 2017, 8, 2003. [Google Scholar] [CrossRef] [PubMed]
- Smit, F.; Ederveen, A.; Cuijpers, P.; Deeg, D.; Beekman, A. Opportunities for cost-effective prevention of late-life depression: An epidemiological approach. Arch. Gen. Psychiatry 2006, 63, 290–296. [Google Scholar] [CrossRef]
- Wariso, B.A.; Guerrieri, G.M.; Thompson, K.; Koziol, D.E.; Haq, N.; Martinez, P.E.; Rubinow, D.R.; Schmidt, P.J. Depression during the menopause transition: Impact on quality of life, social adjustment, and disability. Arch. Womens. Ment. Health 2017, 20, 273–282. [Google Scholar] [CrossRef]
- Ormel, J.; Petukhova, M.; Chatterji, S.; Aguilar-Gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Bromet, E.J.; Burger, H.; Demyttenaere, K.; de Girolamo, G.; et al. Disability and treatment of specific mental and physical disorders across the world. Br. J. Psychiatry 2008, 192, 368–375. [Google Scholar] [CrossRef]
- van ’t Veer-Tazelaar, N.; van Marwijk, H.; van Oppen, P.; Nijpels, G.; van Hout, H.; Cuijpers, P.; Stalman, W.; Beekman, A. Prevention of anxiety and depression in the age group of 75 years and over: A randomised controlled trial testing the feasibility and effectiveness of a generic stepped care programme among elderly community residents at high risk of developing anxiety a. BMC Public Health 2006, 6, 186. [Google Scholar] [CrossRef]
- Cuijpers, P.; Van Straten, A.; Smit, F. Preventing the incidence of new cases of mental disorders: A meta-analytic review. J. Nerv. Ment. Dis. 2005, 193, 119–125. [Google Scholar] [CrossRef]
- Miller, K.J.; Mesagno, C.; McLaren, S.; Grace, F.; Yates, M.; Gomez, R. Exercise, Mood, Self-Efficacy, and Social Support as Predictors of Depressive Symptoms in Older Adults: Direct and Interaction Effects. Front. Psychol. 2019, 10, 2145. [Google Scholar] [CrossRef] [PubMed]
- Akram, M.J.; Malik, A.N. Frequency of chronic neuropathic pain and its association with depression in the elderly in Pakistan. J. Pak. Med. Assoc. 2019, 69, 1907–1909. [Google Scholar] [CrossRef] [PubMed]
- Carbonell-Baeza, A.; Ruiz, J.R.; Aparicio, V.A.; Ortega, F.B.; Delgado-Fernandez, M. The 6-minute walk test in female fibromyalgia patients: Relationship with tenderness, symptomatology, quality of life, and coping strategies. Pain Manag. Nurs. 2013, 14, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Esteve, M.R.; Ramírez, C.; López, A.E. Índices generales versus específicos en la evaluación del afrontamiento al dolor crónico. = General versus specific indexes in chronic pain coping assessment. Psicothema 2004, 16, 421–428. [Google Scholar]
- Spanish Government National Institute of Statistics. Available online: http://www.ine.es (accessed on 12 May 2020).
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed]
- Rubio Castañeda, F.J.; Tomas Aznar, C.; Muro Baquero, C. Validity, Reliability and Associated Factors of the International Physical Activity Questionnaire Adapted to Elderly (IPAQ-E). Available online: https://europepmc.org/article/med/28098134 (accessed on 12 May 2020).
- Alonso, J.; Prieto, L.; Anto, J.M. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Brown, G.K.; Nicassio, P.M. Development of a questionnaire for the assessment of active and passive coping strategies in chronic pain patients. Pain 1987, 31, 53–64. [Google Scholar] [CrossRef]
- Quintana, J.M.; Padierna, A.; Esteban, C.; Arostegui, I.; Bilbao, A.; Ruiz, I. Evaluation of the psychometric characteristics of the Spanish version of the Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 2003, 107, 216–221. [Google Scholar] [CrossRef]
- Jesus Ruiz-Montero, P.; Castillo-Rodriguez, A.; Mikalacki, M.; Nebojsa, C.; Korovljev, D. 24-weeks Pilates-aerobic and educative training to improve body fat mass in elderly Serbian women. Clin. Interv. Aging 2014, 9, 243–248. [Google Scholar] [CrossRef]
- American College of Sport Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Mannerkorpi, K.; Svantesson, U.; Broberg, C. Relationships between performance-based tests and patients’ ratings of activity limitations, self-efficacy, and pain in fibromyalgia. Arch. Phys. Med. Rehabil. 2006, 87, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Al-Amer, R.; Subih, M.; Aldaraawi, H.; Randall, S.; Othman, W.M.M.; Salamonson, Y. Prevalence of Depression and Its Influence on the Quality of Life of Jordanians Living in Residential Care Facilities. J. Nurs. Res. 2019, 27, e54. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, D.; El Shair, I.H.; Taher, E.; Zyada, F. Prevalence and predictors of depression and anxiety among the elderly population living in geriatric homes in Cairo, Egypt. J. Egypt. Public Health Assoc. 2014, 89, 127–135. [Google Scholar] [CrossRef]
- Creighton, A.S.; Davison, T.E.; Kissane, D.W. The correlates of anxiety among older adults in nursing homes and other residential aged care facilities: A systematic review. Int. J. Geriatr. Psychiatry 2017, 32, 141–154. [Google Scholar] [CrossRef]
- Marshall, P.W.M.; Schabrun, S.; Knox, M.F. Physical activity and the mediating effect of fear, depression, anxiety, and catastrophizing on pain related disability in people with chronic low back pain. PLoS ONE 2017, 12, e0180788. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Sherman, A.M. The relationship of optimism, pain and social support to well-being in older adults with osteoarthritis. Aging Ment. Health 2007, 11, 89–98. [Google Scholar] [CrossRef]
- Warner, C.B.; Roberts, A.R.; Jeanblanc, A.B.; Adams, K.B. Coping Resources, Loneliness, and Depressive Symptoms of Older Women With Chronic Illness. J. Appl. Gerontol. 2017. [Google Scholar] [CrossRef]
- Schiltenwolf, M.; Schwarze, M. Diagnostics and therapy of back pain: What is advisable? What should be avoided and why is it still done? Bundesgesundheitsblatt Gesundh. Gesundh. 2020, 63, 527–534. [Google Scholar] [CrossRef]
- Amin, F.M.; Aristeidou, S.; Baraldi, C.; Czapinska-Ciepiela, E.K.; Ariadni, D.D.; Di Lenola, D.; Fenech, C.; Kampouris, K.; Karagiorgis, G.; Braschinsky, M.; et al. The association between migraine and physical exercise. J. Headache Pain 2018, 19, 83. [Google Scholar] [CrossRef]
- Xie, Z.; Poon, A.N.; Wu, Z.; Jian, W.; Chan, K.Y. Is Occupation a Good Predictor of Self-Rated Health in China? PLoS ONE 2015, 10, e0125274. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Pan, Y.; Guo, C.; Li, F.; Xu, R.; Liu, M.; Liu, Z.; Liu, F.; Cai, H.; Ke, Y.; et al. Health-related quality of life among rural residents aged 45–69 years in Hua County, Henan Province, China: Results of ESECC Trial for esophageal cancer screening with endoscopy. Chin. J. Cancer Res. 2018, 30, 240. [Google Scholar] [CrossRef] [PubMed]
- Andrade-Gomez, E.; Martinez-Gomez, D.; Rodriguez-Artalejo, F.; Garcia-Esquinas, E. Sedentary behaviors, physical activity, and changes in depression and psychological distress symptoms in older adults. Depress. Anxiety 2018, 35, 884–897. [Google Scholar] [CrossRef] [PubMed]
- Arts, M.H.L.; Collard, R.M.; Comijs, H.C.; Zuidersma, M.; de Rooij, S.E.; Naarding, P.; Oude Voshaar, R.C. Physical Frailty and Cognitive Functioning in Depressed Older Adults: Findings From the NESDO Study. J. Am. Med. Dir. Assoc. 2016, 17, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Bennett, E.; Clarke, L.; Kowalski, K.; Crocker, P. From pleasure and pride to the fear of decline: Exploring the emotions in older women’s physical activity narratives. Psychol. Sport Exerc. 2017, 33, 113–122. [Google Scholar] [CrossRef]
- Cheung, C.; Park, J.; Wyman, J.F. Effects of Yoga on Symptoms, Physical Function, and Psychosocial Outcomes in Adults with Osteoarthritis: A Focused Review. Am. J. Phys. Med. Rehabil. 2016, 95, 139–151. [Google Scholar] [CrossRef]
- Davenport, M.H.; Marchand, A.-A.; Mottola, M.F.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; Barrowman, N.; Sobierajski, F.; James, M.; Meah, V.L.; et al. Exercise for the prevention and treatment of low back, pelvic girdle and lumbopelvic pain during pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 90–98. [Google Scholar] [CrossRef]
- Zeng, Y.; Feng, Q.; Hesketh, T.; Christensen, K.; Vaupel, J.W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: A cohort study. Lancet 2017, 389, 1619–1629. [Google Scholar] [CrossRef]
- Milanovic, Z.; Pantelic, S.; Trajkovic, N.; Sporis, G.; Kostic, R.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 8, 549–556. [Google Scholar] [CrossRef]
- Dorgo, S.; Robinson, K.M.; Bader, J. The effectiveness of a peer-mentored older adult fitness program on perceived physical, mental, and social function. J. Am. Acad. Nurse Pract. 2009, 21, 116–122. [Google Scholar] [CrossRef]
- Ren, Y.; Li, M. Influence of physical exercise on social anxiety of left-behind children in rural areas in China: The mediator and moderator role of perceived social support. J. Affect. Disord. 2020, 266, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Lesser, I.; Fritz, J.-A.; Belanger, L. The Evaluation of a Health-Based Education and Behavioral Change Retreat on Quality of Life, Physical Activity and Psychosocial Health in Adult Cancer Survivors: An Exploratory Analysis. J. Cancer Educ. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sociodemographic and Clinical Variables | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Age | - | |||||
| 2. Anxiety | 0.126 ** | - | ||||
| 3. Passive strategies (VPMI) | −0.021 | −0.267 *** | - | |||
| 4. Active strategies (VPMI) | 0.028 | 0.157 ** | −0.149 ** | - | ||
| 5. Physical component (SF-36) | −0.100 * | 0.278 *** | −0.444 *** | 0.084 | - | |
| 6. Bodily pain | −0.019 | 0.286 | −0.510 | 0.049 | 0.753 *** | - |
| M (SD) | 68.8 (5.37) | 11.9 (2.88) | 21.2 (6.07) | 16.7 (4.53) | 56.2 (16.8) | 55.9 (26.8) |
| Moderated Mediation Results | Coefficient | SE | p-Value LLCI | LLCI | ULCI |
|---|---|---|---|---|---|
| Outcome: physical component R = 0.60, F (5, 159) = 17.92, p < 0.001 | |||||
| Anxiety | 0.402 | 1.27 | 0.753 | −2.12 | 2.92 |
| Passive strategies | −1.44 | 0.673 | 0.034 | −2.77 | −0.112 |
| Outcome: bodily pain R = 0.77, F (6, 158) = 39.27, p < 0.001 | |||||
| Physical component | 1.61 | 0.328 | 0.001 | 0.955 | 2.25 |
| Anxiety | 1.03 | 0.515 | 0.046 | 0.014 | 2.05 |
| Active strategies | 1.32 | 1.16 | 0.254 | −0.965 | 3.62 |
| Direct effect of anxiety on bodily pain | Effect | SE | p-value | LLCI | ULCI |
| 1.03 | 0.515 | 0.046 | 0.014 | 2.05 | |
| Conditional moderated mediation at (high): | Index | SE | LLCI | ULCI | |
| Passive strategies | 0.043 | 0.061 | −0.068 | 0.172 | |
| Active strategies | −0.039 | 0.029 | −0.117 | 0.004 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiva-Bartoll, Ó.; Morente-Oria, H.; González-Fernández, F.T.; Ruiz-Montero, P.J. Anxiety and Bodily Pain in Older Women Participants in a Physical Education Program. A Multiple Moderated Mediation Analysis. Sustainability 2020, 12, 4067. https://doi.org/10.3390/su12104067
Chiva-Bartoll Ó, Morente-Oria H, González-Fernández FT, Ruiz-Montero PJ. Anxiety and Bodily Pain in Older Women Participants in a Physical Education Program. A Multiple Moderated Mediation Analysis. Sustainability. 2020; 12(10):4067. https://doi.org/10.3390/su12104067
Chicago/Turabian StyleChiva-Bartoll, Óscar, Honorato Morente-Oria, Francisco Tomás González-Fernández, and Pedro Jesús Ruiz-Montero. 2020. "Anxiety and Bodily Pain in Older Women Participants in a Physical Education Program. A Multiple Moderated Mediation Analysis" Sustainability 12, no. 10: 4067. https://doi.org/10.3390/su12104067
APA StyleChiva-Bartoll, Ó., Morente-Oria, H., González-Fernández, F. T., & Ruiz-Montero, P. J. (2020). Anxiety and Bodily Pain in Older Women Participants in a Physical Education Program. A Multiple Moderated Mediation Analysis. Sustainability, 12(10), 4067. https://doi.org/10.3390/su12104067