Investigation and Evaluation of Energy Consumption Performance for Hospital Buildings in China



Abstract
1. Introduction
2. Investigation Methodology and Energy Structure of 100 Hospitals
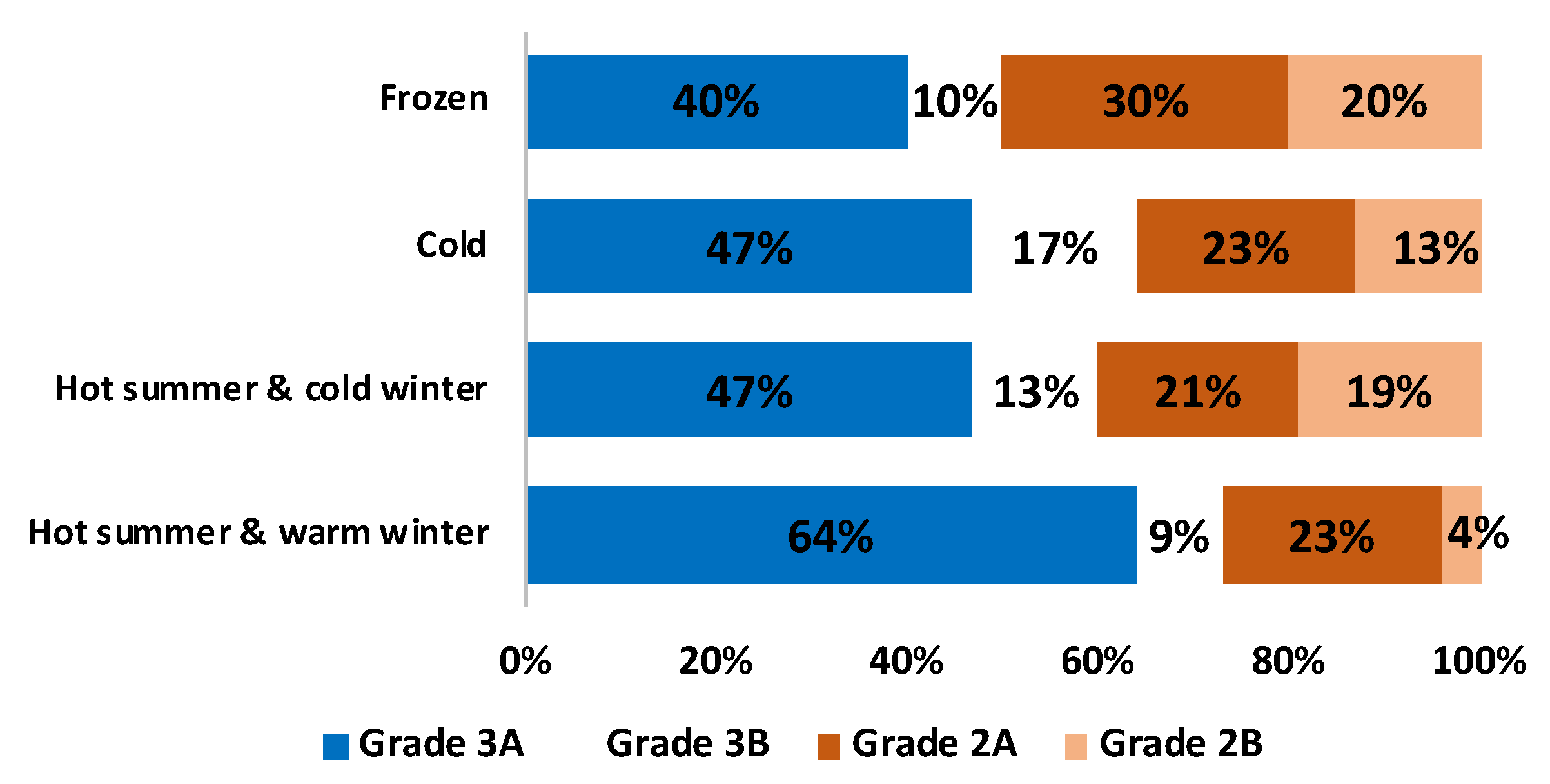
2.1. Sample Description
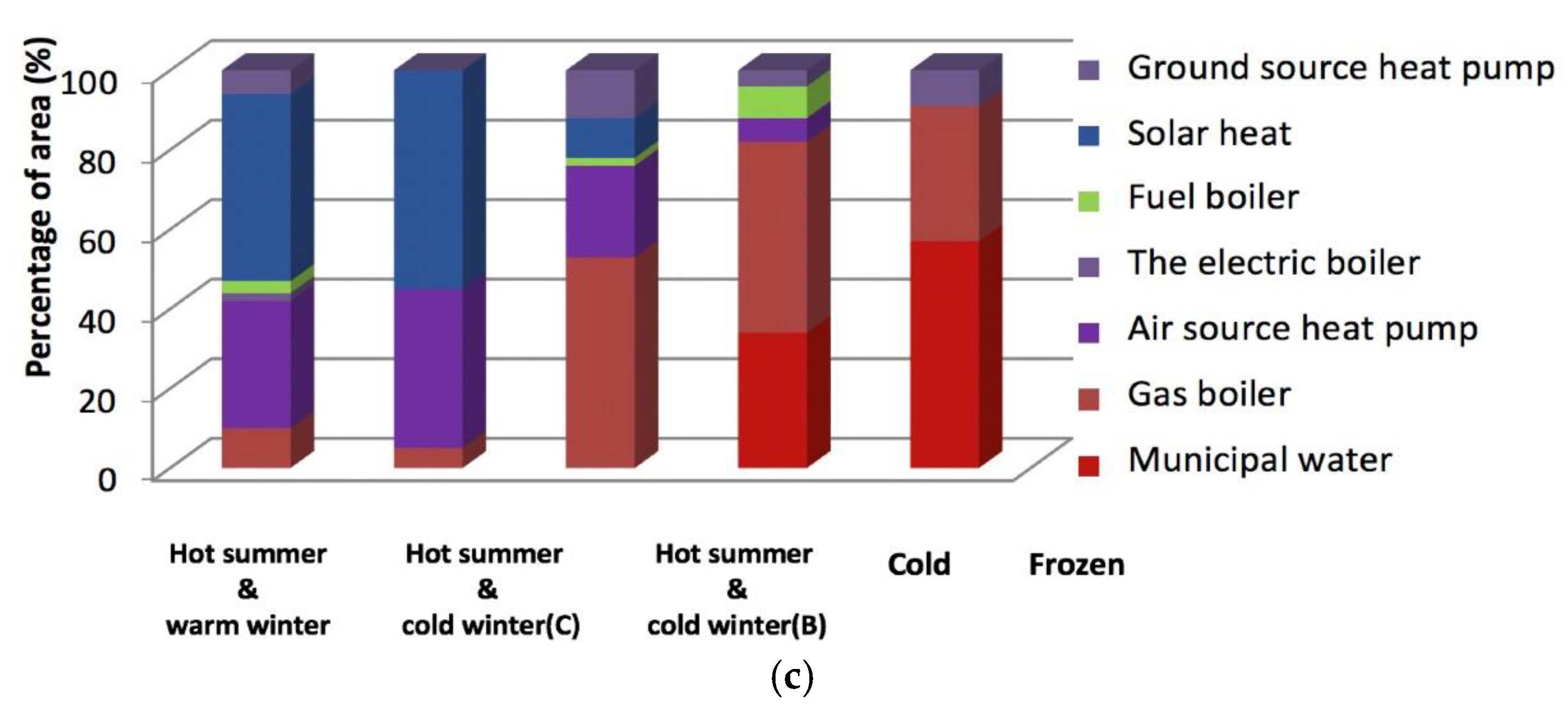
2.2. Analysis of Hospital Building Energy Structure
3. Energy Consumption Investigation Results of 100 Hospitals
3.1. Analysis of Hospital Building Energy Consumption
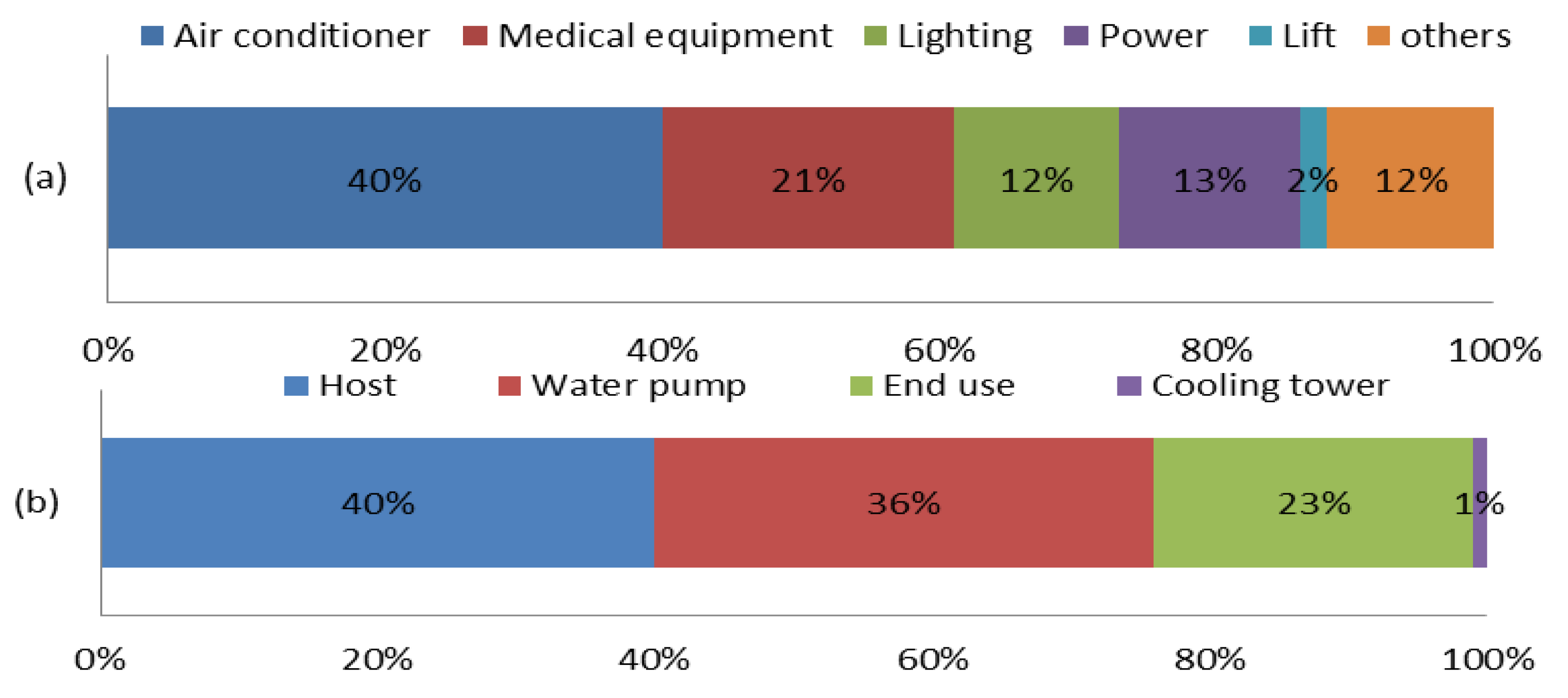
3.1.1. Electrical Consumption
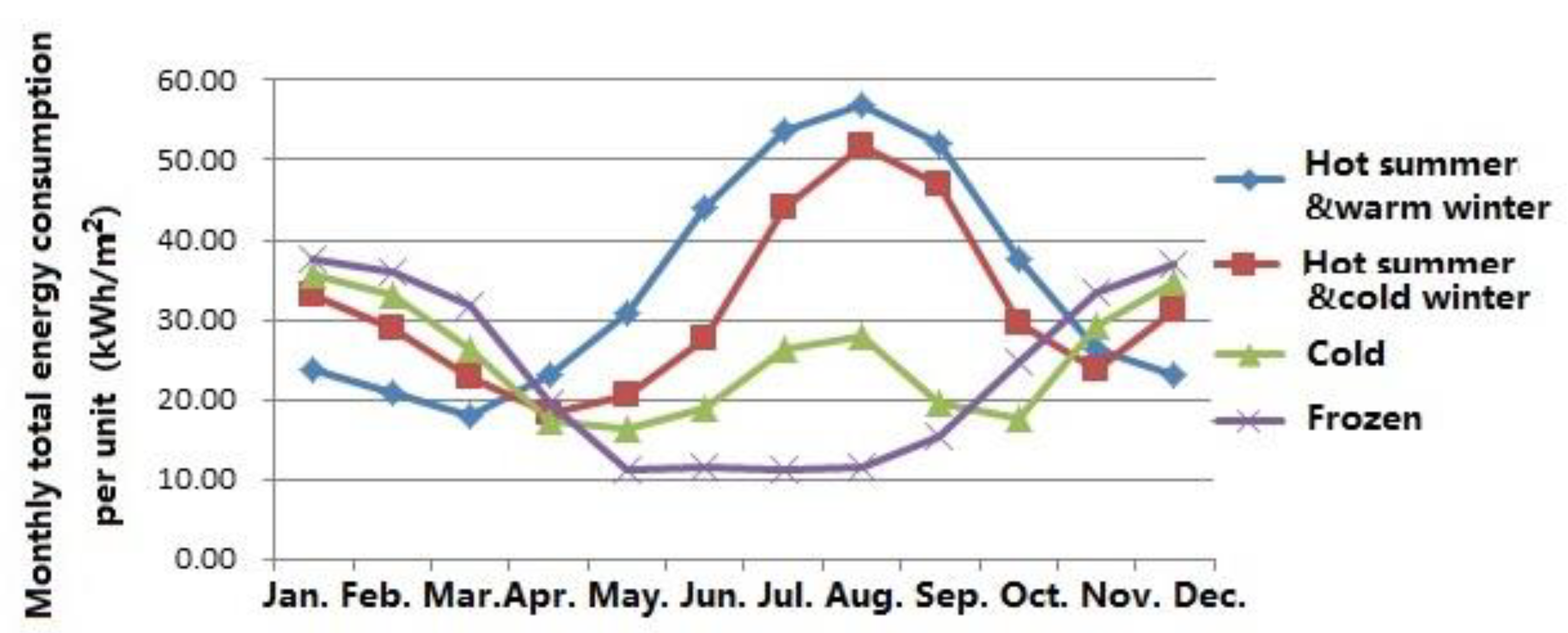
3.1.2. Total Energy Consumption
3.2. Analysis on the Energy Consumption Cost
4. Evaluation of Building Energy-Saving
4.1. The Index of Energy Saving Level
4.2. The Index of Energy Saving Performance
4.3. The Comprehensive Index
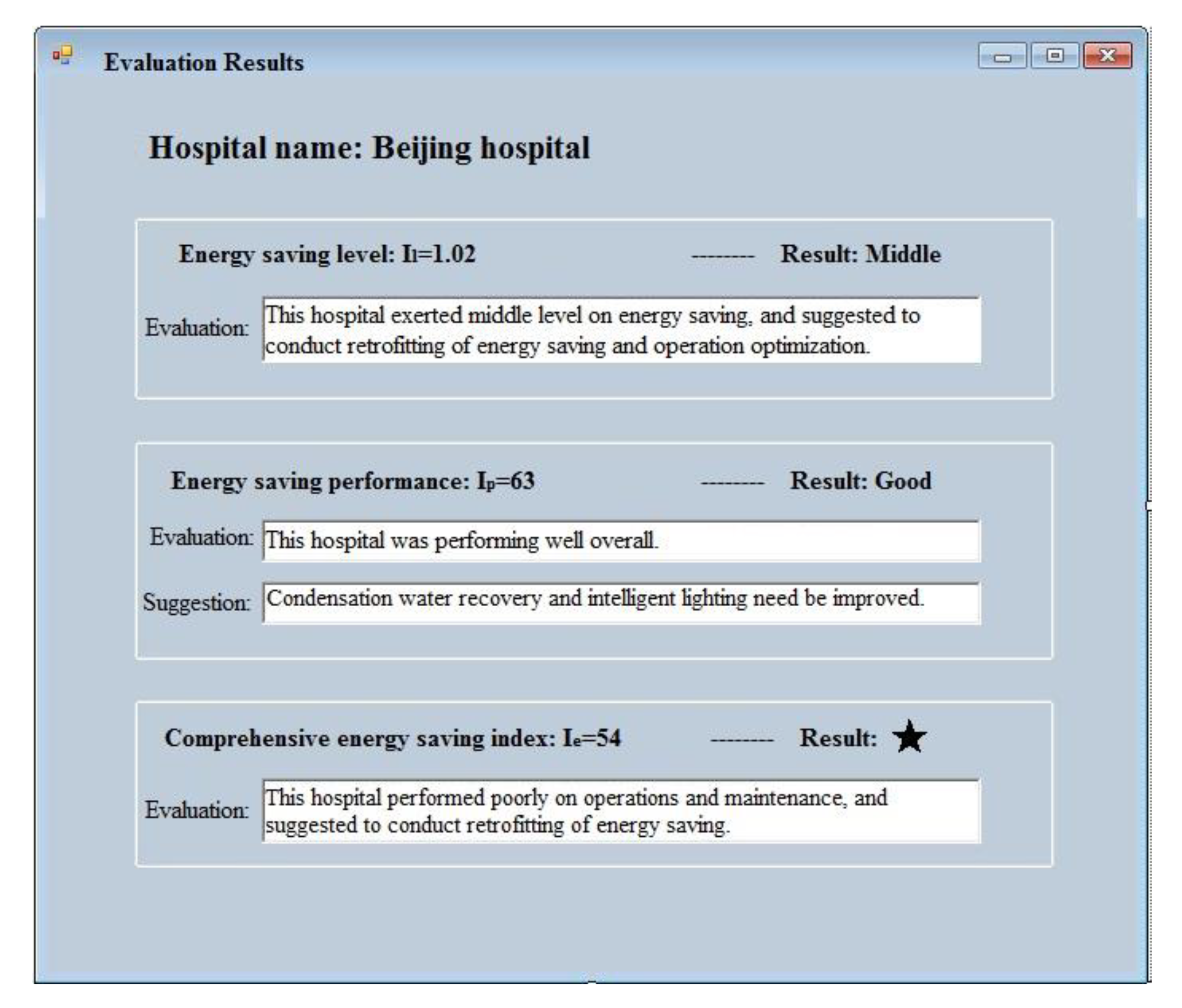
4.4. Visual Application of Evaluation System
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vanhoutteghem, L.; Skarning, G.C.J.; Hviid, C.A.; Svendsen, S. Impact of façade window design on energy, day lighting and thermal comfort in nearly zero-energy houses. Energy Build. 2015, 102, 149–156. [Google Scholar] [CrossRef]
- Alfano, F.R.D.A.; Olesen, B.W.; Palella, B.I.; Riccio, G. Thermal comfort: Design and assessment for energy saving. Energy Build. 2014, 81, 326–336. [Google Scholar] [CrossRef]
- Del Ferraro, S.; Iavicoli, S.; Russo, S.; Molinaro, V. A field study on thermal comfort in an Italian hospital considering differences in gender and age. Appl. Ergon. 2015, 50, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Golbazi, M.; Aktas, C.B. Analysis of Credits Earned by LEED Healthcare Certified Facilities. Procedia Eng. 2016, 145, 203–210. [Google Scholar] [CrossRef]
- Han, J.; Zhang, G.; Zhang, Q.; Zhang, J.; Liu, J.; Tian, L.; Zheng, C.; Hao, J.; Lin, J.; Liu, Y.; et al. Field study on occupants’ thermal comfort and residential thermal environment in a hot-humid climate of China. Build. Environ. 2007, 42, 4043–4050. [Google Scholar] [CrossRef]
- Pourshaghaghy, A.; Omidvari, M. Examination of thermal comfort in a hospital using PMV-PPD model. Appl. Ergon. 2012, 43, 1089–1095. [Google Scholar] [CrossRef] [PubMed]
- Sattayakorn, S.; Ichinose, M.; Sasaki, R. Clarifying thermal comfort of healthcare occupants in tropical region: A case of indoor environment in Thai hospitals. Energy Build. 2017, 149, 45–57. [Google Scholar] [CrossRef]
- Skoog, J.; Fransson, N.; Jagemar, L. Thermal environment in Swedish hospitals: Summer and winter measurements. Energy Build. 2005, 37, 872–877. [Google Scholar] [CrossRef]
- Khalid, W.; Salim, S.A.Z.S.; Rijal, H.B.; Yakub, F. Thermal Comfort in Hospitals in Hot and Humid Climates: A Literature Review. In Proceedings of the 1st Green Environmental Energy and Building Science (GEEBS) International Conference, Johor Bahru, Malaysia, 16–17 October 2017. [Google Scholar]
- Yau, Y.H.; Chew, B.T. Thermal comfort study of hospital workers in Malaysia. Indoor Air 2009, 19, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Alfano, F.R.D.; Olesen, B.W.; Palella, B.I. Povl Ole Fanger’s Impact Ten Years Later. Energy Build. 2017, 15, 243–249. [Google Scholar] [CrossRef]
- Si, B.; Tian, Z.; Chen, W.; Jin, X.; Zhou, X.; Shi, X. Performance Assessment of Algorithms for Building Energy Optimization Problems with Different Properties. Sustainability 2018, 11, 18. [Google Scholar] [CrossRef]
- Ji, R.; Zhang, Z.; He, Y.; Liu, J.; Qu, S. Simulating the effects of anchors on the thermal performance of building insulation systems. Energy Build. 2017, 140, 501–507. [Google Scholar] [CrossRef]
- Wang, Q.; Zhou, P.; Zhao, Z.; Shen, N. Energy Efficiency and Energy Saving Potential in China: A Directional Meta-Frontier DEA Approach. Sustainability 2014, 6, 5476–5492. [Google Scholar] [CrossRef]
- Balaras, C.A.; Dascalaki, E.; Gaglia, A. HVAC and indoor thermal conditions in hospital operating rooms. Build. Environ. 2007, 39, 454–470. [Google Scholar] [CrossRef]
- Meegoda, J.; Hsieh, H.N.; Rodriguez, P.; Jawidzik, J. Sustainable Community Sanitation for a Rural Hospital in Haiti. Sustainability 2012, 4, 3362–3376. [Google Scholar] [CrossRef]
- Sherif, A.H. Hospitals of Developing Countries: Design and Construction Economics. J. Archit. Eng. 1999, 5, 74–81. [Google Scholar] [CrossRef]
- Shu, Y.; Ito, K.; Yokoyama, R. Sensitivity analysis in structure optimization of energy supply systems for a hospital. Energy Conv. Manag. 2007, 48, 2836–2843. [Google Scholar]
- Schweber, L. The effect of BREEAM on clients and construction professionals. Build. Res. Inf. 2013, 41, 129–145. [Google Scholar] [CrossRef]
- Schweber, L.; Haroglu, H. Comparing the fit between BREEAM assessment and design processes. Build. Res. Inf. 2014, 42, 300–317. [Google Scholar] [CrossRef]
- Alhorr, Y.; Arif, M.; Bano, T.; Egbu, C.; Mazroei, A.; Elsarrag, E. Creating a better healing environment in Qatari healthcare sector: Exploring the research agenda for the future. Int. J. Sustain. Built. Environ. 2015, 4, 158–164. [Google Scholar] [CrossRef]
- Ferreira, J.; Pinheiro, M.D.; Brito, J.D. Portuguese sustainable construction assessment tools benchmarked with BREEAM and LEED: An energy analysis. Energy Build. 2014, 69, 451–463. [Google Scholar] [CrossRef]
- Wu, P.; Song, Y.; Shou, W.; Chi, H.; Chong, H.Y.; Sutrisna, M. A comprehensive analysis of the credits obtained by LEED 2009 certified green buildings. Renew. Sustain. Energy Rev. 2017, 68, 370–379. [Google Scholar] [CrossRef]
- Azhar, S.; Carlton, W.A.; Olsen, D.; Ahmad, I. Building information modeling for sustainable design and LEED rating analysis. Autom. Constr. 2011, 20, 217–224. [Google Scholar] [CrossRef]
- Pradinuk, R. Incentivizing the Daylit Hospital: The Green Guide for Health Care Approach. HERD Health Environ. Res. Des. J. 2009, 2, 92–112. [Google Scholar] [CrossRef]
- Younger, M.; Morrow-Almeida, H.R.; Vindigni, S.M.; Dannenberg, A.L. The Built Environment, Climate Change, and Health: Opportunities for Co-Benefits. Am. J. Prev. Med. 2008, 35, 517–526. [Google Scholar] [CrossRef]
- Liu, Y.; Guo, X.; Hu, F. Cost-benefit analysis on green building energy efficiency technology application: A case in China. Energy Build. 2014, 82, 37–46. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, J.; Hu, F.; Wang, Y. Comparison of evaluation standards for green building in China, Britain, United States. Renew. Sustain. Energy Rev. 2017, 68 Pt 1, 262–271. [Google Scholar] [CrossRef]
- Jian, Z.; Pullen, S.; Rameezdeen, R.; Bennetts, H.; Wang, Y.; Mao, G.; Zhou, Z.; Du, H.; Duan, H. Green building evaluation from a life-cycle perspective in Australia: A critical review. Renew. Sustain. Energy Rev. 2017, 70, 358–368. [Google Scholar]
- Chen, S.; Li, N.; Guan, J.; Xie, Y.; Sun, F.; Ni, J. A statistical method to investigate national energy consumption in the residential building sector of China. Energy Build. 2008, 40, 654–665. [Google Scholar] [CrossRef]
- Benelmir, R.; Feidt, M. Energy cogeneration systems and energy management strategy. Energy Convers. Manag. 1998, 39, 1791–1802. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hospital Category | Climatic Zone | ||||
|---|---|---|---|---|---|
| Frozen | Cold | Hot Summer & Cold Winter | Hot Summer & Warm Winter | Total | |
| Grade 3A | 4 | 14 | 18 | 14 | 50 |
| Grade 3B | 1 | 5 | 5 | 2 | 13 |
| Grade 2A | 3 | 7 | 8 | 5 | 23 |
| Grade 2B | 2 | 4 | 7 | 1 | 14 |
| Total | 10 | 30 | 38 | 22 | 100 |
| Bed Number | 100~500 | 500~1000 | 1000~1500 | >1500 | Total |
|---|---|---|---|---|---|
| Hospital Number | 39 | 40 | 10 | 11 | 100 |
| Number of Beds | Tri-Sectional Quantile of Il | ||
|---|---|---|---|
| 100~500 | 338.42 | 0.86 | 1.19 |
| 500~1000 | 357.83 | 0.90 | 1.44 |
| 1000~1500 | 368.27 | 0.85 | 1.16 |
| >1500 | 382.65 | 0.90 | 1.15 |
| Number of Beds | Level | ||
|---|---|---|---|
| Low | Middle | High | |
| 100~500 | Il < 0.86 | 0.86 ≤ Il < 1.19 | Il ≥ 1.19 |
| 500~1000 | Il < 0.90 | 0.90 ≤ Il < 1.44 | Il ≥ 1.44 |
| 1000~1500 | Il < 0.85 | 0.85 ≤ Il < 1.16 | Il ≥ 1.16 |
| >1500 | Il < 0.90 | 0.90≤ Il <1.15 | Il ≥ 1.15 |
| Performance | Score of Ip |
|---|---|
| Bad | 0 ≤ Ip < 25 |
| Middle | 25 ≤ Ip < 50 |
| Good | 50 ≤ Ip < 75 |
| Excellent | 75 ≤ Ip < 100 |
| Level | Score of Ie |
|---|---|
| ☆ | 0 ≤ Ie < 40 |
| ★ | 40 ≤ Ie < 60 |
| ★★ | 60 ≤ Ie < 80 |
| ★★★ | 80 ≤ Ie ≤ 100 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, R.; Qu, S. Investigation and Evaluation of Energy Consumption Performance for Hospital Buildings in China. Sustainability 2019, 11, 1724. https://doi.org/10.3390/su11061724
Ji R, Qu S. Investigation and Evaluation of Energy Consumption Performance for Hospital Buildings in China. Sustainability. 2019; 11(6):1724. https://doi.org/10.3390/su11061724
Chicago/Turabian StyleJi, Ru, and Shilin Qu. 2019. "Investigation and Evaluation of Energy Consumption Performance for Hospital Buildings in China" Sustainability 11, no. 6: 1724. https://doi.org/10.3390/su11061724
APA StyleJi, R., & Qu, S. (2019). Investigation and Evaluation of Energy Consumption Performance for Hospital Buildings in China. Sustainability, 11(6), 1724. https://doi.org/10.3390/su11061724