Scheduling Sustainable Homecare with Urban Transport and Different Skilled Nurses Using an Approximate Algorithm

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Homecare Algorithm Approach
- where , where 0 and n + 1 are the CCE,
- is the arc set,
- With each arc a travel cost is associated and a travel time ,
- Pj: j-th is the patient set, mainly one patient, who requires HC services given by certain nurse types Nns from the CCE and is found in a given urban area,
- With each HC service to the patient, cost and service time are associated.
- Rks: k-th existing routes, s-th nurse type, chosen by the CCE, in accordance with the location of patients, geography, infrastructure, the HC required, nurse-patient history and so forth. For example, when the CCE defines six routes for nurse type 1, on which the required services are to be provided to all the patients daily, then indicator k varies from 1 to 6 and this indicator will take the value 1. Rks = (R11, R21, R31, R41, R51, R61)
- Ti: i-th type of vehicle for nurse transportation, classified according to its costs and availability for use by the CCE. For example, if the CCE is to use five different vehicle types (T1, T2,…, T5), then i varies from 1 to 5.
- Nns: n-th number of nurses corresponding to each s-th types of nurses, classified according to their skills and their availability for care giving. For example, if the CCE is to use five nurses skilled 3 level 1 and 2 level 3, then Nns = (N11, N21, N31, N13, N23).
- Pjks: j-th patient who requires assistance from a given (s-th) nurse type, assigned to route k by the CCE, where patients’ assignment to each route is carried out according to the proximity between patients and the route, the qualifications required for care tasks and patients’ personal preferences. One patient might require more than one different HC type, which must be carried out by a different nurse type.
- HCmsj: m-th HC issued by s-th nurse type to the j-th patient. For example, if a patient (P2) requires three HC services to be provided, two by nurse type 1 and one by nurse type 3, nurses scheduled by the CCE, then j = 2, s = 1, 3 and m = 1, 2, 3. Therefore, HCms2 = [HC112, HC212, HC322] are all the requirements issued by patient 2.
- Ck: the cost assigned to the k-th transport route (Rks), generally by transport type (Ti). For example, if the CCE uses for nurse type 3 only routes R23 and R43 on a single day, the costs that the algorithm must consider are c2 and c4.
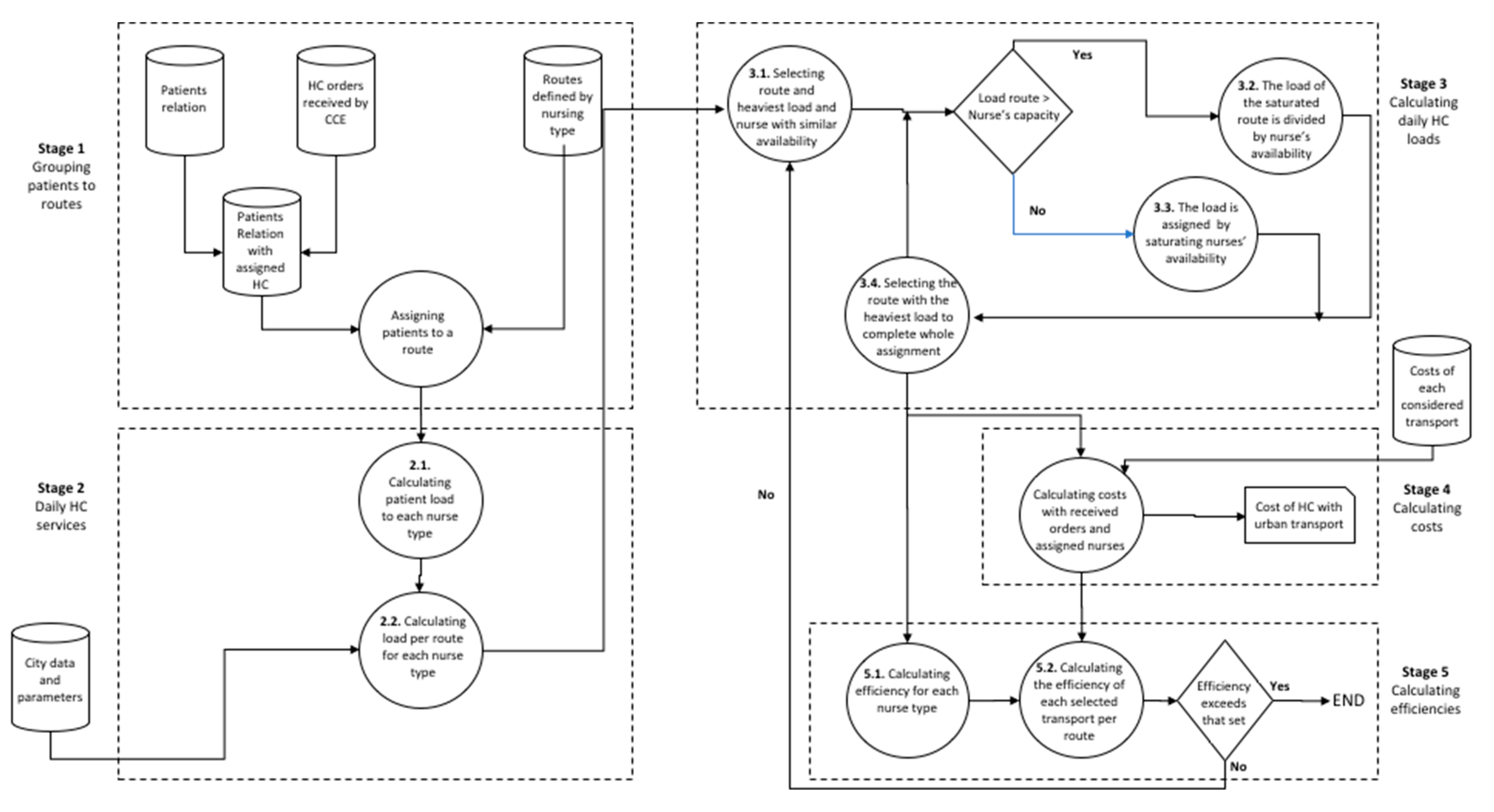
2.2. Homecare Algorithm Stages
- Step 2.1.
- Calculating load according to all the demand orders assigned to each nurse type (units: min):
- Step 2.2.
- Calculation of load according to each route of each nurse type (units: min):
- Step 3.1.
- Selecting the route with the heaviest load and the assignment of nurse Nns with a similar time availability to this load and sufficient qualification.Nns is assigned if:
- Step 3.2.
- If Load HC of a route is greater than the capacity of the non-assigned nurse’s available time, then:The division of routes’ load is done as indicated in Equation (5).According to the following procedure:
- Step 3.3.
- If a Load HC is assigned to a route, Load (Rks) is less than the capacity of allocated nurse Nns. However, when failing to meet the constraint of maximum number of patients Pjsk to be visited (by exceeding that number Psk > Wsk), load is divided as follows:where:
- Step 3.4.
- Having assigned the nurses to the route with the heaviest load, the assignment of nurses continues with the route with the next heaviest load. To do so, the procedure returns to Step 3.1. This process should be continued until all the routes with HC loads are processed. It also includes the routes that are cut because of one algorithm constraint or more.
- Step 5.1.
- Calculating efficiency (α) for each selected nurse Nns in Stage 3:where:
- Step 5.2.
- If the efficiencies calculated for each Ti equal or exceed 0.7, the assignment is final as this level is considered acceptable by the CCE and, as such, the calculation with the algorithm ends. For each Ti where the efficiency calculation gives a result below 0.7, the assignment of transport type Ti should be repeated.
3. Results
4. Discussion and Conclusions
- -
- -
- Economic benefits (in the long term), as transport costs are a variable of the algorithm and form an intrinsic part of a country’s social and healthcare policies. The algorithm links the economic aspects to the environmental ones that the HC service requires
- -
- Environmental benefits (in the short- and mid-terms), by considering a means of transport offer that addresses minimum emissions and is ecological by factoring in an activity that is increasingly present in urban areas of cities.
Author Contributions
Funding
Conflicts of Interest
References
- Blomqvist, A.; Busby, C. Long-term care for the elderly: Challenges and policy options. CD Howe Inst. Comment. 2012, 367. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2015: OECD Indicators; OECD Publishing: Paris, France, 2015. [Google Scholar]
- Keenan, T.A. Home and Community Preferences of the 45+ Population; AARP Research & Strategic Analysis: Washington, DC, USA, 2010. [Google Scholar]
- Gillsjö, C.; Schwartz-Barcott, D.; von Post, I. Home: The place the older adult can not imagine living without. BMC Geriatr. 2011, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Ageing; Department of Economic and Social Affairs PD: New York, NY, USA, 2013. [Google Scholar]
- Eikemo, T.A.; Bambra, C.; Judge, K.; Ringdal, K. Welfare state regimes and differences in self-perceived health in Europe: A multilevel analysis. Soc. Sci. Med. 2008, 66, 2281–2295. [Google Scholar] [CrossRef] [PubMed]
- Genet, N.; Boerma, W.; Kroneman, M.; Hutchinson, A.; Saltman, R.B. Home Care across Europe: Current Structure and Future Challenges; European Observatory on Health Systems and Policies: London, UK, 2013. [Google Scholar]
- Issaoui, B.; Zidi, I.; Marcon, E.; Laforest, F.; Ghedira, K. Literature review: Home health care. In Proceedings of the 2015 15th International Conference on Intelligent Systems Design and Applications (ISDA), Marrakesh, Morocco, 14–16 December 2015. [Google Scholar]
- Social Protection Committee and the European Commission. Adequate Social Protection for Long-Term Care Needs in an Ageing Society; Report No.: Contract No.: 10406/14 ADD 1; Council of the European Union: Brussels, Belgium, 2014. [Google Scholar]
- Klaus-Dieter, R.; Hirsh, P. Supporting urban home health care in daily business and times disasters. IFAC Pap. Online 2015, 48, 686–691. [Google Scholar] [CrossRef]
- Eveborn, P.; Flisberg, P.; Rönnqvist, M. Laps care—An operational system for staff planning of home care. Eur. J. Oper. Res. 2006, 171, 962–976. [Google Scholar] [CrossRef]
- Trautsamwieser, A.; Gronalt, M.; Hirsch, P. Securing home health care in times of natural disasters. OR Spectr. 2011, 33, 787–813. [Google Scholar] [CrossRef]
- Wirnitzer, J.; Heckmann, I.; Meyer, A.; Nickel, S. Patient-based nurse rostering in home care. Oper. Res. Health Care 2016, 8, 91–102. [Google Scholar] [CrossRef]
- DG MOVE European Commission. Study on Urban Freight Transport; Centro di Ricerca per il Trasporto e la Logistica (CTL): Rome, Italy, 2012. [Google Scholar]
- Haghshenas, H.; Vaziri, M. Urban sustainable transportation indicators for global comparison. Ecol. Indic. 2012, 15, 115–121. [Google Scholar] [CrossRef]
- Ros-McDonnell, L.; De-la-Fuente-Aragon, M.V.; Ros-McDonnell, D.; Cardós, M. Analysis of freight distribution flows in an urban functional area. Cities 2018, 79, 159–168. [Google Scholar] [CrossRef]
- Gilbert, R.; Irwin, N.; Hollingworth, B.; Blais, P. Sustainable Transportation Performance Indicators (STPI); Transportation Research Board (TRB), CD ROM: Washington, DC, USA, 2003. [Google Scholar]
- Okraszewska, R.; Romanowska, A.; Wolek, M.; Oskarbski, J.; Birr, K.; Jamroz, K. Integration of a multilevel transport system model into sustainable urban mobility planning. Sustainability 2018, 10, 479. [Google Scholar] [CrossRef]
- Gillis, D.; Semanjski, I.; Lauwers, D. How to monitor sustainable mobility in Cities? Literature review in the frame of creating a set of sustainable mobility indicators. Sustainability 2016, 8, 29. [Google Scholar] [CrossRef]
- Muñuzuri, J.; Onieva, L.; Cortes, P.; Guadix, J. Gestión Pública de la Logística Urbana de Mercancias. Una Normativa, Multiples Necesidades. Economía Industrial Num 400: Logística Urbana; Ministerio de Industria, Energía y Turismo: Madrid, Spain, 2016. [Google Scholar]
- Russo, F.; Comi, A. Urban freight transport planning towards green goals: Synthetic environmental evidence from tested results. Sustainability 2016, 8, 381. [Google Scholar] [CrossRef]
- Szander, N.; Ros-McDonnell, L.; de la Fuente, M.V. Algorithm for efficient and sustainable home health care delivery scheduling. In Lecture Notes in Management and Industrial Engineering: New Global Perspectives on Industrial Engineering and Management; Mula, J., Barbastefano, R., Díaz-Madroñero, M., Poler, R., Eds.; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Szander, N.; RosMcDonnell, L.; de-la-Fuente-Aragón, M.V.; Vodopivec, R. Sustainable urban homecare delivery with different means of transport. Sustainability 2018, 10, 398. [Google Scholar] [CrossRef]
- Trautsamwieser, A.; Hirsh, P. A branch-price-and-cut approach for solving medium-terms home health care planning problem. Networks 2014, 64, 143–159. [Google Scholar] [CrossRef]
- Bertels, S.; Fahle, T. A hybrid setup for a hybrid scenario: Combining heuristics for the home health care problem. Comput. Oper. Res. 2006, 33, 2866–2890. [Google Scholar] [CrossRef]
- Eveborn, P.; Rönnqvist, M.; Einarsdóttir, H.; Eklund, M.; Lidén, K.; Almroth, M. Operations research improves quality and efficiency in home care. Interfaces 2009, 39, 18–34. [Google Scholar] [CrossRef]
- Dohn, A.; Rasmussen, M.S.; Justesen, T.; Larsen, J. The home care crew scheduling problem. In Proceedings of the 1st International Conference on Applied Operational Research (ICAOR’08), Yerevan, Armenia, 15–17 September 2008. [Google Scholar]
- Bredstrom, D.; Rönnqvist, M. A branch and price algorithm for the combined vehicle routing and scheduling problem with synchronization constraints. NHH Dept. Financ. Manag. Sci. Discuss. Paper 2007. [Google Scholar] [CrossRef]
- Rasmussen, M.S.; Justesen, T.; Dohn, A.; Larsen, J. The home care crew scheduling problem: Preference-based visit clustering and temporal dependencies. Eur. J. Oper. Res. 2012, 219, 598–610. [Google Scholar] [CrossRef]
- Bredström, D.; Rönnqvist, M. Combined vehicle routing and scheduling with temporal precedence and synchronization constraints. Eur. J. Oper. Res. 2008, 191, 19–31. [Google Scholar] [CrossRef]
- Mankowska, D.S.; Meisel, F.; Bierwirth, C. The home health care routing and scheduling problem with interdependent services. Health Care Manag. Sci. 2013, 17, 15–30. [Google Scholar] [CrossRef]
- Hiermann, G.; Prandtstetter, M.; Rendl, A.; Puchinger, J.; Raidl, G.R. Metaheuristics for solving a multimodal home-healthcare scheduling problem. Cent. Eur. J. Oper. Res. 2015, 23, 89–113. [Google Scholar] [CrossRef]
- Fikar, C.; Hirsch, P. A matheuristic for routing real-world home service transport systems facilitating walking. J. Clean. Prod. 2014, 105, 300–310. [Google Scholar] [CrossRef]
- Braekers, K.; Hartl, R.F.; Parragh, S.N.; Tricoire, F. A bi-objective home care scheduling problem: Analyzing the trade-off between costs and client inconvenience. Eur. J. Oper. Res. 2016, 248, 428–443. [Google Scholar] [CrossRef]
- Clausen, J. Branch and Bound Algorithms-Principles and Examples; Department of Computer Science, University of Copenhagen: Copenhagen, Denmark, 1999; pp. 1–30. [Google Scholar]
- Rouillon, S.; Desaulniers, G.; Soumis, F. An extended branch-and-bound method for locomotive assignment. Transp. Res. Part B Methodol. 2006, 40, 404–423. [Google Scholar] [CrossRef]
- Albareda-Sambola, M.; Van Der Vlerk, M.H.; Fernández, E. Exact solutions to a class of stochastic generalized assignment problems. Eur. J. Oper. Res. 2006, 173, 465–487. [Google Scholar] [CrossRef]
- Li, V.; Curry, G.L. Solving multidimensional knapsack problems with generalized upper bound constraints using critical event tabu search. Comput. Oper. Res. 2005, 32, 825–848. [Google Scholar] [CrossRef]
- Osorio, M.A.; Laguna, M. Logic cuts for multilevel generalized assignment problems. Eur. J. Oper. Res. 2003, 151, 238–246. [Google Scholar] [CrossRef]
- Martello, S.; Toth, P. An algorithm for the generalized assignment problem. Oper. Res. 1981, 81, 589–603. [Google Scholar]
- Fisher, M.L.; Jaikumar, R.; Van Wassenhove, L.N. A multiplier adjustment method for the generalized assignment problem. Manag. Sci. 1986, 32, 1095–1103. [Google Scholar] [CrossRef]
- de Grancy, G.S.; Reimann, M. Vehicle routing problems with time windows and multiple service workers: A systematic comparison between ACO and GRASP. Cent. Eur. J. Oper. Res. (CEJOR) 2016, 24, 29–48. [Google Scholar] [CrossRef]
- Vidal, T.; Crainic, T.-G.; Gendreau, M.; Prins, C. Heuristics for multi-attribute vehicle routing problems: A survey and systhesis. Eur. J. Oper. Res. 2013, 231, 1–21. [Google Scholar] [CrossRef]
- Cattaruzza, D.; Absi, N.; Feillet, D.; Vidal, T. A memetic algorithm for the multi trip vehicle routing problem. Eur. J. Oper. Res. 2014, 236, 833–848. [Google Scholar] [CrossRef]
- Amini, M.M.; Racer, M. A hybrid heuristic for the generalized assignment problem. Eur. J. Oper. Res. 1995, 87, 343–348. [Google Scholar] [CrossRef]
- Lorena, L.A.N.; Narciso, M.G. Relaxation heuristics for a generalized assignment problem. Eur. J. Oper. Res. 1996, 91, 600–610. [Google Scholar] [CrossRef]
- Ribeiro, J.F.; Pradin, B. A methodology for cellular manufacturing design. Int. J. Prod. Res. 1993, 31, 235–250. [Google Scholar] [CrossRef]
- Sankappanavar, H.P.; Burris, S. A Course in Universal Algebra; Graduate Texts Math; Springer: New York, NY, USA, 1981; Volume 78. [Google Scholar]
- Gallier, J.H. Logic for Computer Science: Foundations of Automatic Theorem Proving; John Wiley & Sons: New York, NY, USA, 1986. [Google Scholar]
- Bogart, K.P. Discrete Mathematics; D. C. Heath & Co.: Lexington, MA, USA, 1988. [Google Scholar]
- Barnes, D.W.; Mack, J.M. An Algebraic Introduction to Mathematical Logic; Springer: New York, NY, USA; Berlin/Heidelberg, Germany, 1975. [Google Scholar]
- Bertoni, M. Introducing sustainability in value models to support design decision making: A systematic review. Sustainability 2017, 9, 994. [Google Scholar] [CrossRef]
- Koeleman, P.M.; Bhulai, S.; van Meersbergen, M. Optimal patient and personnel scheduling policies for care-at-home service facilities. Eur. J. Oper. Res. 2012, 219, 557–563. [Google Scholar] [CrossRef]
- Liu, W.; Bai, E.; Liu, L.; Wei, W. A tramework of sustainable service supply chain management: A literature review and research agenda. Sustainability 2017, 9, 421. [Google Scholar] [CrossRef]


{kind=link}
| Frequency | Monday to Friday | Monday to Sunday | Tuesday to Friday |
|---|---|---|---|
| 1/day | 34 | 7 | 1 |
| 1/week | 4 | ||
| 2/day | 5 | 3 | |
| 2/week | 13 | ||
| 3/day | 1 | ||
| 3/week | 5 | ||
| Total | 73 | ||
| Ti | Attributes | C(Ti) |
|---|---|---|
| T1 | Walking | €0 |
| T2 | Bus | €20/month |
| T3 | E-bikes | €9/month |
| T4 | Taxi | €3 trip (flat rate in the city) |
| T5 | Car | €0.19/km + parking |
| Patient Address | Location Code | Route (Rks) | Care Need Code | Time Required (minutes) | Pjks |
|---|---|---|---|---|---|
| Location patient 1 | A000 | 11 | Th_1_20 | 20 | P0511 |
| Location patient 2 | A001 | 91 | Mo-Fr_1_20 | 20 | P5091 |
| Location patient 3 | A002 | 81 | Tu-Th_1_30 | 30 | P4381 |
| Location patient 4 | B001 | 91 | Mo-Fr_1_30 | 30 | P5691 |
| Location patient 5 | B002 | 121 | Mo-Fr_2_30 | 30 | P58101 |
| Prioritised Routes | Algorithm Step 3.2 | ||
|---|---|---|---|
| Route (Rks) | Time Load (minute) | Route (Rks) | Time Load (minute) |
| R101 | 667 * | R11 a | 365 |
| R11 | 495 * | R11 b | 30 |
| R41 | 300 | R101 a | 382 |
| R71 | 207 | R101 b | 185 |
| R91 | 200 | ||
| R31 | 190 | ||
| R21 | 187 | ||
| R51 | 186 | ||
| R81 | 177 | ||
| R61 | 165 | ||
| Bus + Walking | E-Bikes | Cars | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Monday | Number of Patients | Care Time (hour) | Travel + Idle Time (hour) | α | Number of Patients | Care Time (hour) | Travel + Idle Time (hour) | α | Number of Patients | Care Time (hour) | Travel + Idle Time (hour) | α |
| Nurse 1 | 9 | 6.4 | 1.6 | 0.9 | 9 | 6.4 | 1.6 | 0.8 | 9 | 6.4 | 1.6 | 0.9 |
| Nurse 2 | 5 | 5.1 | 2.9 | 0.8 | 7 | 7.1 | 0.9 | 0.9 | 5 | 5.1 | 2.9 | 0.7 |
| Nurse 3 | 5 | 5.0 | 3.0 | 0.7 | 5 | 5.0 | 3.0 | 0.7 | 6 | 4.6 | 3.4 | 0.6 |
| Nurse 4 | 6 | 4.6 | 3.4 | 0.7 | 6 | 4.6 | 3.4 | 0.6 | 7 | 7.0 | 1.0 | 0.9 |
| Nurse 5 | 4 | 3.9 | 4.1 | 0.7 | 9 | 6.7 | 1.3 | 0.9 | 9 | 6.7 | 1.3 | 0.9 |
| Nurse 6 | 9 | 6.0 | 2.1 | 0.9 | 13 | 7.1 | 0.9 | 0.9 | 12 | 7.0 | 1.0 | 0.9 |
| Nurse 7 | 5 | 3.5 | 4.6 | 0.6 | 10 | 6.5 | 1.5 | 0.9 | 11 | 6.6 | 1.4 | 0.9 |
| Nurse 8 | 6 | 3.2 | 4.8 | 0.5 | ||||||||
| Nurse 9 | 10 | 5.8 | 2.2 | 0.9 | ||||||||
| Average efficiency | 0.75 | 0.84 | 0.85 | |||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ros-McDonnell, L.; Szander, N.; de-la-Fuente-Aragón, M.V.; Vodopivec, R. Scheduling Sustainable Homecare with Urban Transport and Different Skilled Nurses Using an Approximate Algorithm. Sustainability 2019, 11, 6210. https://doi.org/10.3390/su11226210
Ros-McDonnell L, Szander N, de-la-Fuente-Aragón MV, Vodopivec R. Scheduling Sustainable Homecare with Urban Transport and Different Skilled Nurses Using an Approximate Algorithm. Sustainability. 2019; 11(22):6210. https://doi.org/10.3390/su11226210
Chicago/Turabian StyleRos-McDonnell, Lorenzo, Norina Szander, María Victoria de-la-Fuente-Aragón, and Robert Vodopivec. 2019. "Scheduling Sustainable Homecare with Urban Transport and Different Skilled Nurses Using an Approximate Algorithm" Sustainability 11, no. 22: 6210. https://doi.org/10.3390/su11226210
APA StyleRos-McDonnell, L., Szander, N., de-la-Fuente-Aragón, M. V., & Vodopivec, R. (2019). Scheduling Sustainable Homecare with Urban Transport and Different Skilled Nurses Using an Approximate Algorithm. Sustainability, 11(22), 6210. https://doi.org/10.3390/su11226210