Improving Water Access and Health through Rainwater Harvesting: Perceptions of an Indigenous Community in Jalisco, Mexico

Abstract
1. Introduction
2. Background
2.1. Traditional Knowledge, Practices, and Beliefs
2.2. Access to Water for the Wixarika People
2.3. Sustainable Development in an Indigenous Context
3. Materials and Methods
3.1. The La Laguna Social–Ecological System Case Study
3.2. Data Collection
3.2.1. Epidemiological Data at the Community Level
3.2.2. Statistical Analysis
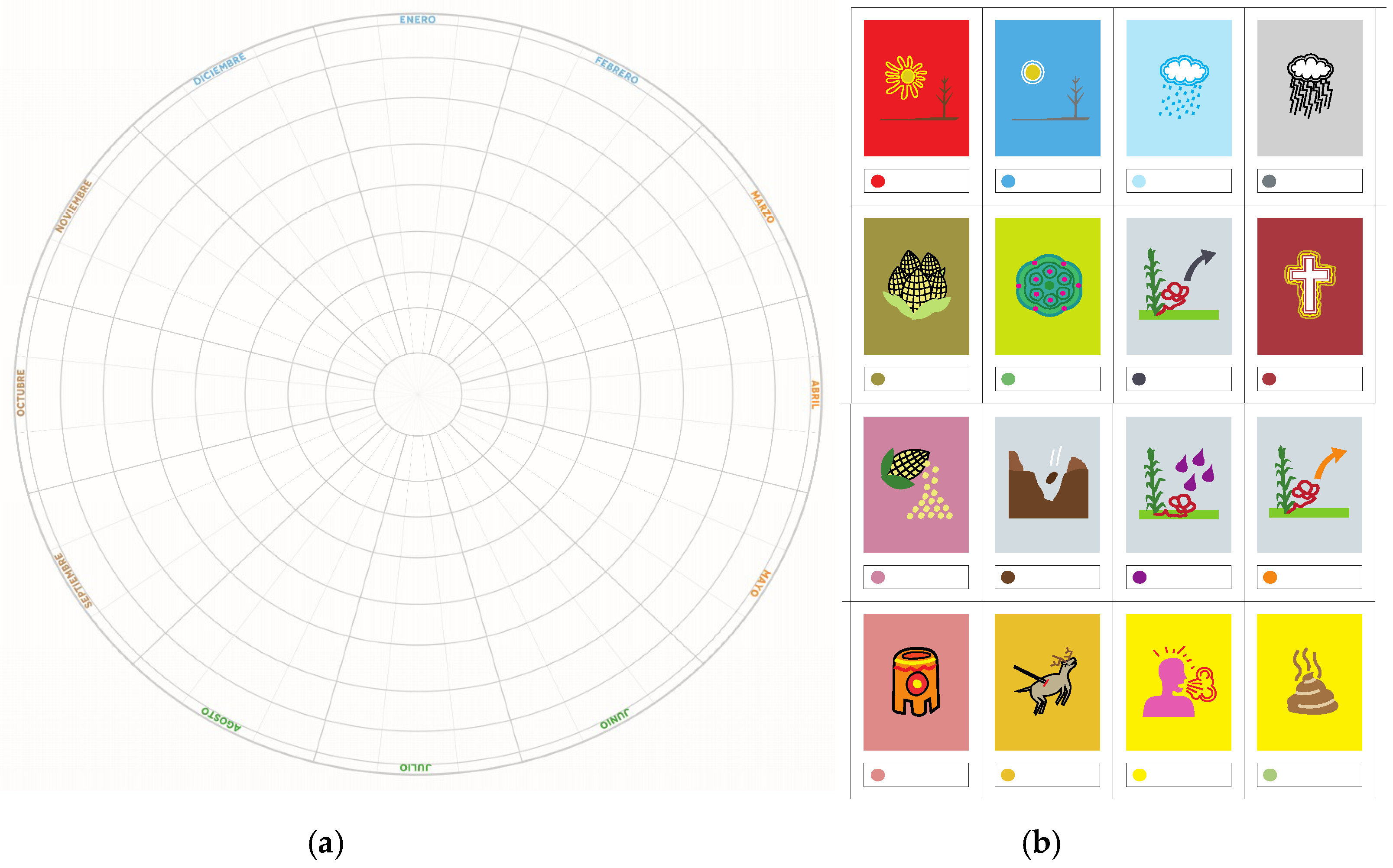
3.2.3. Semi-Structured Interviews and the Cosmo–Eco–Health Calendar
3.2.4. Samples of Water Quality Indicators at the Household Level
4. Results
4.1. Population Demographics of La Laguna Community
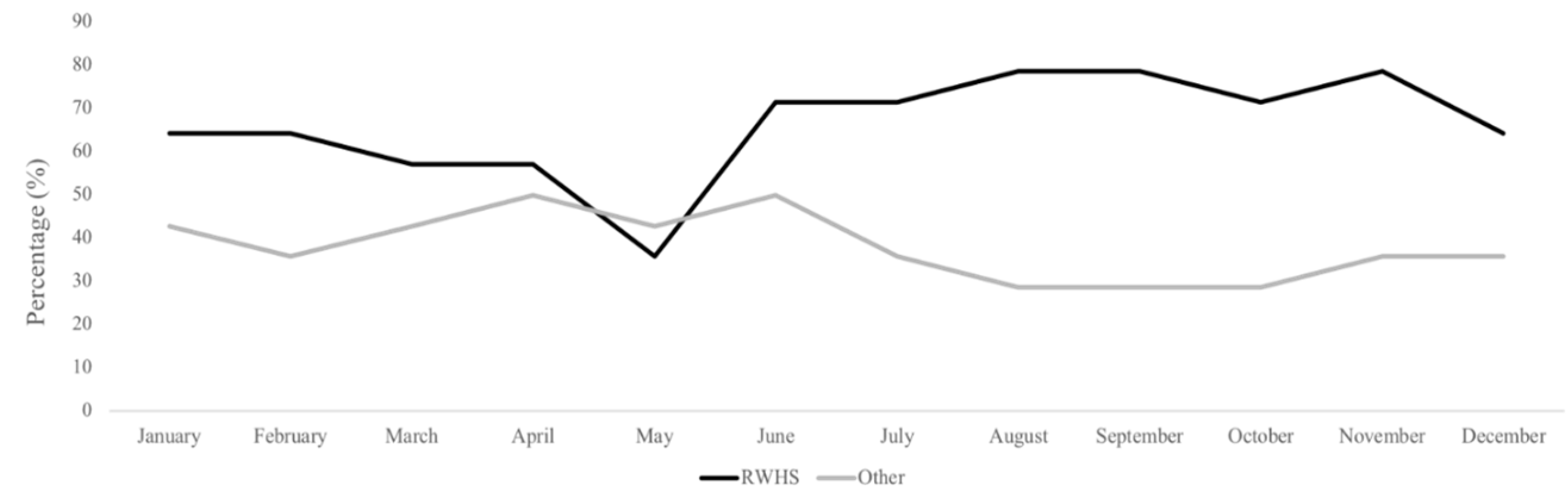
4.2. Water Use and Management at Household Level (Rainy and Dry Season)
4.3. Microbiological Contamination
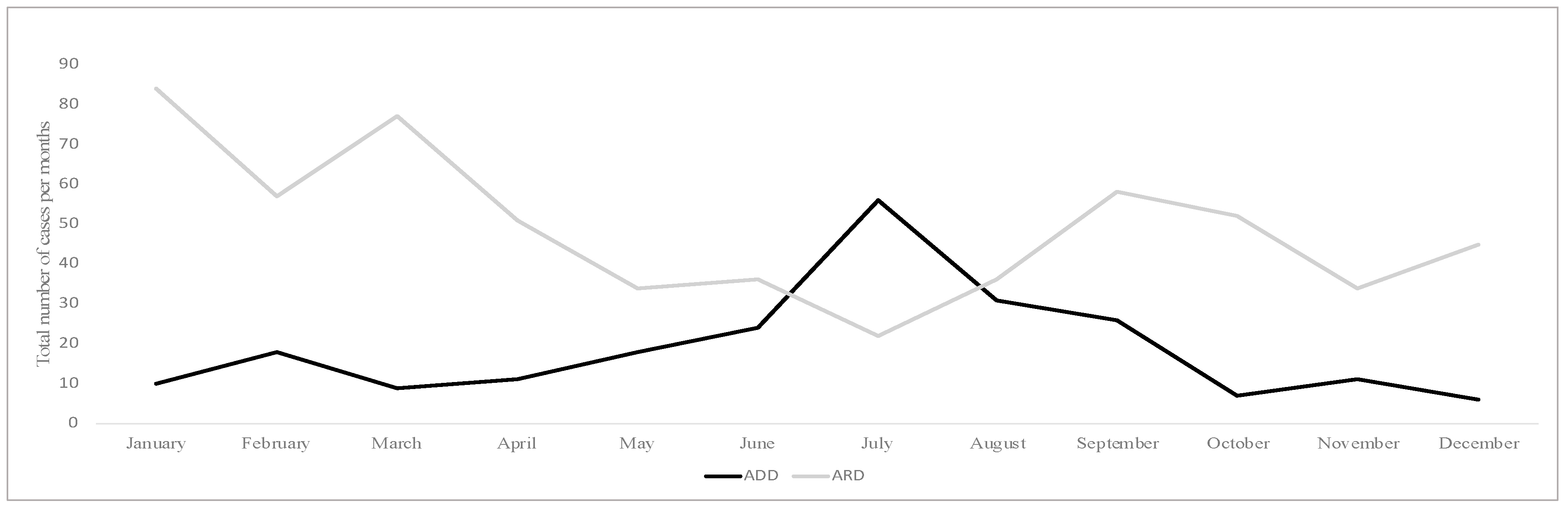
4.4. The Epidemiological Data and Cases of Acute Diarrheal Diseases from 2014 to 2017
4.5. Health Perceptions at the Household Level
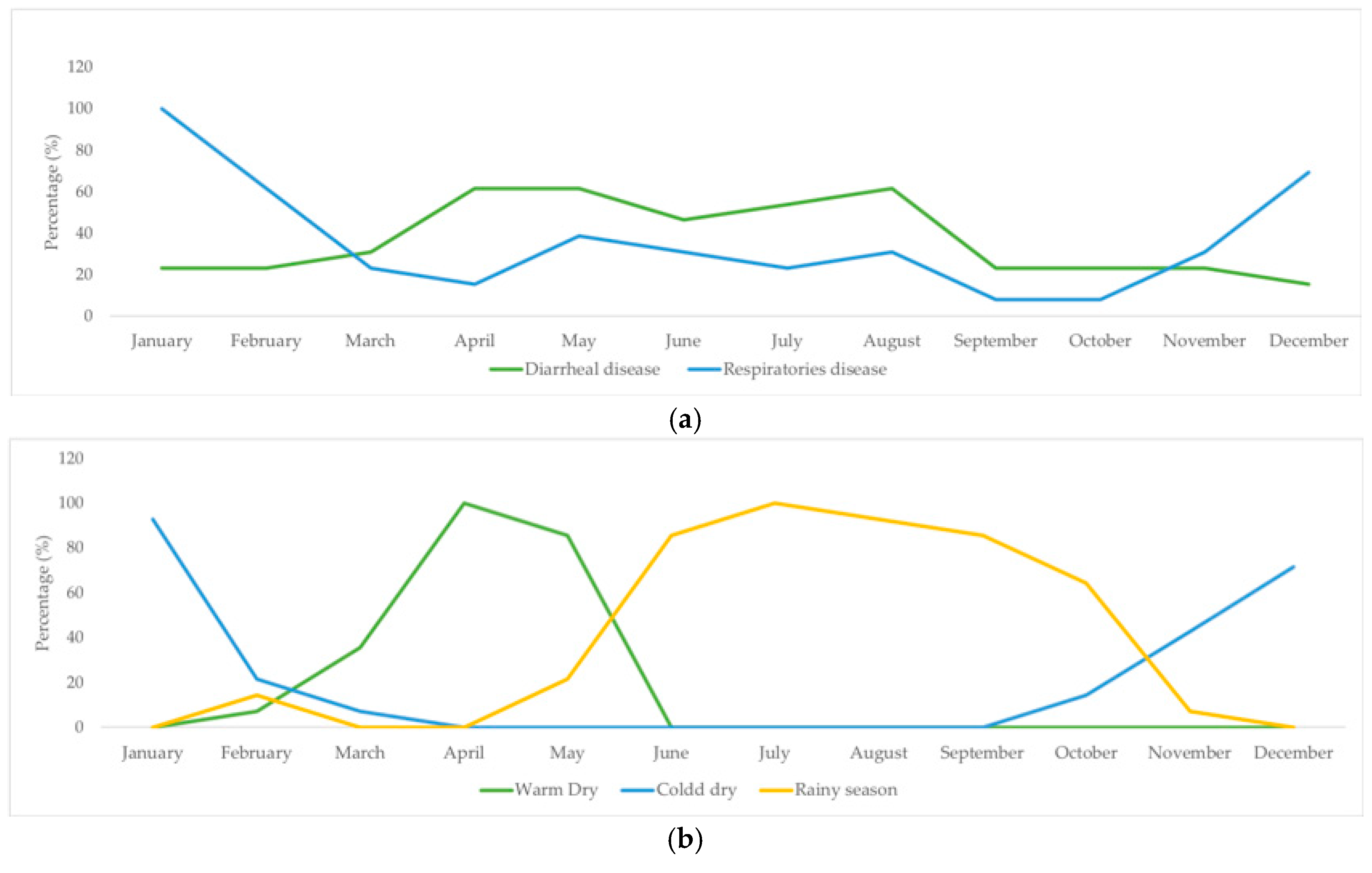
4.5.1. Disease Incidence by Month (perceived and recorded) and Seasonality
4.5.2. Perceptions of Causes and Origins of Disease
4.5.3. Household Hygiene Practices and Sanitation
5. Discussion
5.1. The Potential for RWHSs to Improve Water Quantity and Quality in Indigenous Rural Communities
5.2. Implications for Sustainable Development
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Murthy, S.L. The Human Right to Water and Sanitation: History, Meaning, and the Controversy Over-Privatization. Berkley J. Int. Law 2013, 31, 89–149. [Google Scholar] [CrossRef]
- UN. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations General Assembly: New York, NY, USA, 2015; pp. 1–35. [Google Scholar]
- WWF. Final Report of the 5th World Water Forum. Available online: http://www.Royalcommission.Vic.Gov.Au/Finaldocuments/Summary/Pf/Vbrc_Summary_Pf.Pdf (accessed on 26 August 2006).
- CONAGUA. Estadísticas del Agua en México; Comisión Nacional del Agua: Mexico City, Mexico, 2011.
- Murtinho, F.; Tague, C.; de Bievre, B.; Eakin, H.; Lopez-Carr, D. Water Scarcity in the Andes: A Comparison of Local Perceptions and Observed Climate, Land Use and Socioeconomic Changes. Hum. Ecol. 2013, 41, 667–681. [Google Scholar] [CrossRef]
- Sullivan, C. Calculating a Water Poverty Index. World Dev. 2002, 7, 1195–1210. [Google Scholar] [CrossRef]
- Rijsberman, F.R. Water Scarcity: Fact or Fiction? Agric. Water Manag. 2006, 80, 5–22. [Google Scholar] [CrossRef]
- UN-Water. Financing Universal Water, Sanitation and Hygiene under the Sustainable Development Goals: Global Analysis and Assessment of Sanitation and Drinking-Water (GLAAS) 2017 Report; UN-Water: Geneva, Switzerland, 2017. [Google Scholar]
- Assmus, G.C. Agua, Pobreza y Equidad: Un Análisis Asimétrico. Rev. Latinoam. Bioet. 2015, 15, 90–99. [Google Scholar] [CrossRef]
- Johnston, B.R.; Strang, V. Water, Cultural Diversity, and Global Environmental Change: Emerging Trends, Sustainable Futures; UNESCO-IHP: Paris, France, 2012; p. 253. [Google Scholar] [CrossRef]
- Moe, C.L.; Rheingans, R.D. Global Challenges in Water, Sanitation and Health. J. Water Health 2006, 4, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Amos, C.C.; Rahman, A.; Gathenya, J.M. Economic Analysis and Feasibility of Rainwater Harvesting Systems in Urban and Peri-Urban Environments: A Review of the Global Situation with a Special Focus on Australia and Kenya. Water 2016, 8. [Google Scholar] [CrossRef]
- Ímaz Gispert, M.; Armienta Hernández, M.A.; Lomnitz Climent, E.; Torregrosa Flores, M.F. Rainwater Harvesting as a Drinking Water Option for Mexico City. Sustainability 2018, 10, 3890. [Google Scholar] [CrossRef]
- Tanner, T.; Lewis, D.; Wrathall, D.; Bronen, R.; Cradock-Henry, N.; Huq, S.; Lawless, C.; Nawrotzki, R.; Prasad, V.; Rahman, M.A.; et al. Livelihood Resilience in the Face of Climate Change. Nat. Clim. Chang. 2014, 5. [Google Scholar] [CrossRef]
- Fonseca, J.E.; Carneiro, M.; Pena, J.L.; Colosimo, E.A.; da Silva, N.B.; da Costa, A.G.F.C.; Moreira, L.E.; Cairncross, S.; Heller, L. Reducing Occurrence of Giardia Duodenalis in Children Living in Semiarid Regions: Impact of a Large Scale Rainwater Harvesting Initiative. PLoS Negl. Trop. Dis. 2014, 8. [Google Scholar] [CrossRef]
- Jonathan, D.; Paul, R.H. Risk of Gastrointestinal Illness Associated with the Consumption of Rainwater: A Systematic Review. Environ. Sci. Technol. 2012, 46, 2501–2507. [Google Scholar]
- Williams, E. Huichol Ethnography and Archaeological Interpretation. Pap. Inst. Archaeol. 1990, 6–15. [Google Scholar] [CrossRef]
- CONAPO. La Marginación En Los Municipios. Índice Marginación Por Entid. Fed. Y Munic. 2015, 2015, 23–38. [Google Scholar] [CrossRef]
- De la Torre, R. Ten Years of the Human Development Index in Mexico. Real. Datos Espac. 2012, 3, 149–163. [Google Scholar]
- Neurath, J.; Pacheco Bribiesca, R.C. Atlas de Culturas Del Agua En América Latina y El Caribe. In Pueblos Indígenas De México Y Agua: Huicholes (Wixarika); Instituto Mexicano de Tecnología del Agua: Mexico City, Mexico, 2006; pp. 1–53. [Google Scholar]
- Liffman, P.M. Huichol Territory and the Mexican Nation: Indigenous Ritual, Land Conflict, and Sovereignty Claims; University of Arizona Press: Tucson, AZ, USA, 2011. [Google Scholar]
- Sánchez Domínguez-Guilarte, M. Los Wixaritari a Través de La Antropologia, La Historia y La Literatura: La Construcción y Popularización de Un Estereotipo. Front. Rev. História 2016, 18, 51–75. [Google Scholar]
- Neurath, J. Ambivalencias Del Poder y Del Don En El Sistema Político Ritual Wixárika. In Los pueblos amerindios más allá del Estado; México Universidad Nacional Autónoma de México, Instituto de Investigaciones Históricas: Mexico City, Mexico, 2011. [Google Scholar]
- Torres, G. La Fuerza del Costumbre. Un Acercamiento a la Realidad Tlapaneca (Me’Phaa). Bachelor’s Thesis, Etnohistoria, Escuela Nacional de Antropología e Historia, Mexico City, Mexico, 2014; p. 102. [Google Scholar]
- Verdín Amaro, K.I.; García, S.S. Red Semántica de Las Enfermedades Del Pueblo Wixárika o Huichol. Alteridades 2012, 22, 97–110. [Google Scholar]
- Takeuchi, K.; Osamu, S.; Lahoti, S.; Gondor, D. Growing up: 10 Years of Publishing Sustainability Science Research. Sustain. Sci. 2017. [Google Scholar] [CrossRef]
- UN-Water. Water for a Sustainable World; UN-Water: Geneva, Switzerland, 2015. [Google Scholar] [CrossRef]
- Johnson, J.T.; Howitt, R.; Cajete, G.; Berkes, F.; Louis, R.P.; Kliskey, A. Weaving Indigenous and Sustainability Sciences to Diversify Our Methods. Sustain. Sci. 2016, 11, 1–11. [Google Scholar] [CrossRef]
- Franquesa-Soler, M.; Sandoval-Rivera, J.C.A. Mentoring Program to Achieve SDGs in Local Contexts: A Case Study in Communities from Southern Mexico. Sustain. J. Rec. 2019, 12, 109–114. [Google Scholar] [CrossRef]
- Barrera, R.O. Consideraciones Geomorfológías Sobre La Sierra Madre Occidental En El Norte de Jalisco, México Geomorphological Considerations about the Sierra Madre Occidental in Northern Jalisco. Investig. Geográficas 2002, 48, 44–75. [Google Scholar]
- Santo Domingo, A.F.; Castro-Díaz, L.; González-Uribe, C.; The Wayúu Community of Marbacella; The Barí Community of Karikachaboquira. Ecosystem Research Experience with Two Indigenous Communities of Colombia: The Ecohealth Calendar as a Participatory and Innovative Methodological Tool. Ecohealth 2016, 13, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Levy, K.; Nelson, K.L.; Hubbard, A.; Eisenberg, J.N.S. Rethinking Indicators of Microbial Drinking Water Quality for Health Studies in Tropical Developing Countries: Case Study in Northern Coastal Ecuador. Am. J. Trop. Med. Hyg. 2012, 86, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Gracey, M.; King, M. Indigenous Health Part 1: Determinants and Disease Patterns. Lancet 2009, 374, 65–75. [Google Scholar] [CrossRef]
- UN. State of the World’s Indigenous People; UN: New York, NY, USA, 2009; p. 250. [Google Scholar]
- Ghebreyesus, T.A. Improving the Health of Indigenous People Globally. Lancet Oncol. 2018, 19, e277. [Google Scholar] [CrossRef]
- Guevara, Y.; De Haro, I.; Cabrera, M.; García De La Torre, G.; Salazar-Schettino, P.M. Enteroparasitosis En Poblaciones Indígenas y Mestizas de La Sierra de Nayarit, México. Parasitol. Latinoam. 2003, 58, 30–34. [Google Scholar] [CrossRef]
- Adler, I.; Hudson-Edwards, K.A.; Campos, L. Converting Rain into Drinking Water: Quality Issues and Technological Advances. Water Sci. Technol. Water Supply 2011, 11, 659–667. [Google Scholar] [CrossRef]
- Rahman, S.; Khan, M.T.R.; Akib, S.; Din, N.B.C.; Biswas, S.K.; Shirazi, S.M. Sustainability of Rainwater Harvesting System in Terms of Water Quality. Sci. World J. 2014, 2014. [Google Scholar] [CrossRef]
- Jin, Y.Z.; Zhou, L.W.; Lo, K.F.A. Optimum Matching Model Using Long-Term Computing on Safer Rural Domestic Water Supply Based on Rainwater Harvesting. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef]
- Campisano, A.; Butler, D.; Ward, S.; Burns, M.J.; Friedler, E.; DeBusk, K.; Fisher-Jeffes, L.N.; Ghisi, E.; Rahman, A.; Furumai, H.; et al. Urban Rainwater Harvesting Systems: Research, Implementation and Future Perspectives. Water Res. 2017, 115, 195–209. [Google Scholar] [CrossRef]
- Gorchev, H.G.; Ozolins, G. WHO Guidelines for Drinking-Water Quality. WHO Chron. 1984, 38, 104–108. [Google Scholar] [CrossRef]
- Carrasco Henríquez, N.; Samaniego Sastre, M.; Durán Pérez, T. Indicadores de desarrollo? Alcances antropológicos en torno a los procesos de medición y control del desarrollo social y cultural. Pública Gestión Estatal 2009, 9, 59–72. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group (Years) | Count (%) |
|---|---|
| 0–9 | 36.15 |
| 10–19 | 23.91 |
| 20–64 | 37.69 |
| ≥65 | 2.25 |
| Sex | |
| Male | 47.12 |
| Female | 52.88 |
| Practice | Percentage (%) |
|---|---|
| Using rainwater from cisterns during the rainy season | 80 |
| Using rainwater from cisterns during the dry season | 64 |
| Using rainwater and another source during the rainy season | 36 |
| Using rainwater and another source during the dry season | 40 |
| Annual cleaning frequency of cisterns | 76 |
| Rainy Season | Dry Season | |||
|---|---|---|---|---|
| Range of Contamination (CFU/100 mL) | Percentage of Samples with Contamination: Rainwater Harvesting Systems (RWHS) | Percentage of Samples with Contamination: Another Source | Percentage of Samples with Contamination: RWHS | Percentage of Samples with Contamination: Another Source |
| Total Coliform * | ||||
| 0 | 47.37 | 14.29 | 47.06 | 33.33 |
| 1–10 | N.D. | N.D. | N.D. | N.D. |
| 11–100 | 5.26 | N.D. | 5.88 | 11.11 |
| 101–1000 | 31.58 | 14.29 | 17.65 | N.D. |
| >1000 | 21.05 | 71.43 | 29.41 | 55.56 |
| E. coli * | ||||
| 0 | 94.74 | 71.43 | 100 | 88.89 |
| 1–10 | 5.26 | N.D. | N.D. | 11.11 |
| 11–100 | N.D. | N.D. | N.D. | N.D. |
| 101–1000 | N.D. | 14.29 | N.D. | N.D. |
| >1000 | N.D. | 14.29 | N.D. | N.D. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Padrón, S.K.; Lerner, A.M.; Mazari-Hiriart, M. Improving Water Access and Health through Rainwater Harvesting: Perceptions of an Indigenous Community in Jalisco, Mexico. Sustainability 2019, 11, 4884. https://doi.org/10.3390/su11184884
González-Padrón SK, Lerner AM, Mazari-Hiriart M. Improving Water Access and Health through Rainwater Harvesting: Perceptions of an Indigenous Community in Jalisco, Mexico. Sustainability. 2019; 11(18):4884. https://doi.org/10.3390/su11184884
Chicago/Turabian StyleGonzález-Padrón, Shiara K., Amy M. Lerner, and Marisa Mazari-Hiriart. 2019. "Improving Water Access and Health through Rainwater Harvesting: Perceptions of an Indigenous Community in Jalisco, Mexico" Sustainability 11, no. 18: 4884. https://doi.org/10.3390/su11184884
APA StyleGonzález-Padrón, S. K., Lerner, A. M., & Mazari-Hiriart, M. (2019). Improving Water Access and Health through Rainwater Harvesting: Perceptions of an Indigenous Community in Jalisco, Mexico. Sustainability, 11(18), 4884. https://doi.org/10.3390/su11184884