Air Quality Standards and Extreme Ozone Events in the São Paulo Megacity

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. WRF/Chem Simulation
2.2. Air Quality Standards
- AQSE = air quality standard exceedance
- ATTE = attention level exceedance
- TH = concentration at the analyzed hour
- TH−n = concentration n hours earlier than the analyzed hour
- SP = State of São Paulo
- WHO = World Health Organization
2.3. Socioeconomic and Health Vulnerability
2.4. Simplified Cost Analysis
3. Results
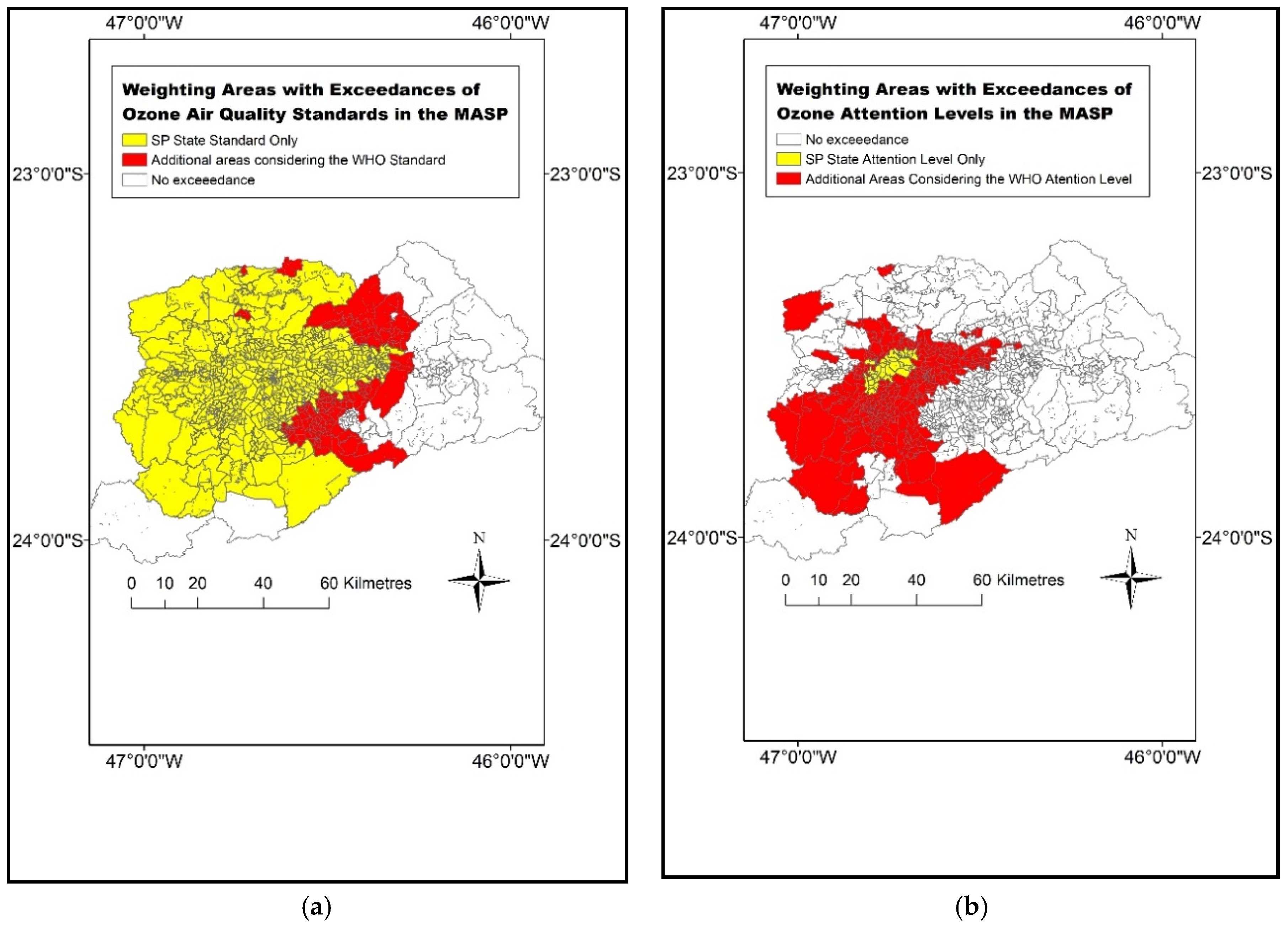
3.1. Exceedances of Air Quality and Attention Levels in the MASP According to SP State and WHO Limits
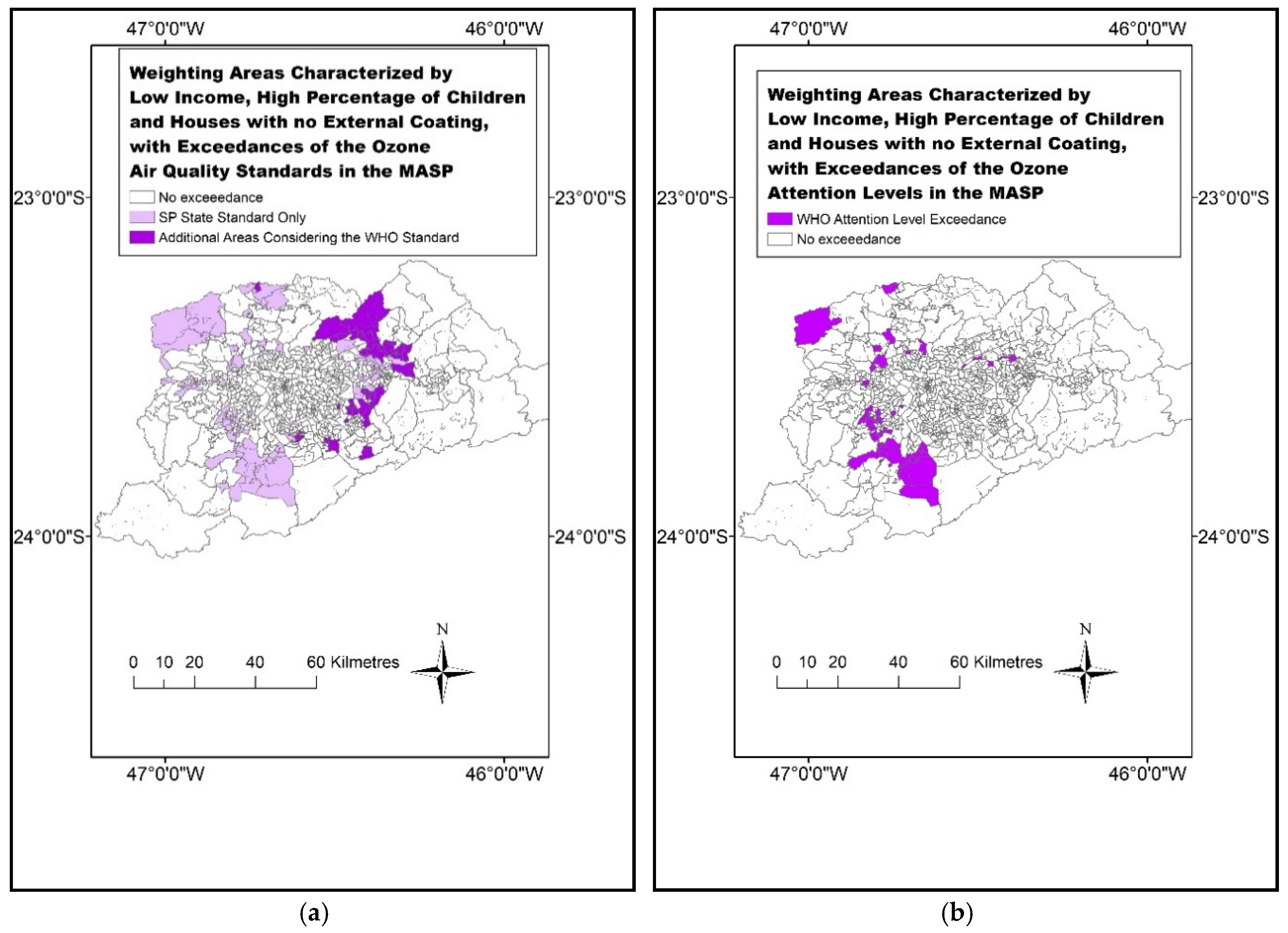
3.2. Ozone Exceedances and Socioeconomic Vulnerability
3.3. Number of People Affected
3.4. Cost Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A
- Four vehicle categories: light, trucks, buses and motorbikes:
- Km driven per day for each category
- Emission factors—gasoline (with 22% ethanol), ethanol, flex-fuel and diesel
- Proportion of vehicles per type
- Chemical mechanism RADM2
- Photolysis Madronich [41]
- Reactions Stockwell [42]
- Ethanol as an explicit chemical species
- Period: 28/01–02/02/2014 (anomalies of temperature (+3 °C) and OLR (+60 Wm−2))
- Spatial resolution: land use/surface 30 s (approximately 800 m)/emissions 1 km
- Spatial resolution (timestep): 6 s
References
- World Health Organization. Air Quality Guidelines: Global Update 2005: Particulate Matter, Ozone, Nitrogen Dioxide, and Sulfur Dioxide. World Health Organization, 2006. Available online: http://www.euro.who.int/en/health-topics/environment-and-health/air-quality/publications/pre2009/air-quality-guidelines.-global-update-2005.-particulate-matter,-ozone,-nitrogen-dioxide-and-sulfur-dioxide (accessed on 10 January 2019).
- 2017. Available online: http://www.euro.who.int/__data/assets/pdf_file/0019/331660/Evolution-air-quality.pdf (accessed on 12 January 2019).
- CETESB (São Paulo), Relatório Anual da Qualidade do Ar do Estado de São Paulo, 2017, Divisão de Análise de dados, São Paulo, 2018. Available online: https://cetesb.sp.gov.br/ar/wp-content/uploads/sites/28/2018/05/relatorio-qualidade-ar-2017.pdf (accessed on 3 March 2019).
- Brasseur, G.; Orlando, J.J.; Tyndall, G.S. Atmospheric Chemistry and Global Change; Oxford University Press: Oxford, UK, 1999. [Google Scholar]
- Nobre, C.A.; Marengo, J.A.; Seluchi, M.E.; Cuartas, L.A.; Alves, L.M. Some characteristics and impacts of the drought and water crisis in Southeastern Brazil during 2014 and 2015. J. Water Resour. Prot. 2016, 8, 252. [Google Scholar] [CrossRef]
- Chiquetto, J.B.; Ribeiro, F.N.D.; Alvim, D.S.; Ynoue, R.Y.; Silva, J.; Silva, M.E.S. Transport of Pollutants by the Sea Breeze in São Paulo under the South Atlantic High. Rev. Dep. Geogr. 2018, 148–161. [Google Scholar] [CrossRef]
- International Pannel on Climate Change, II Working Group. Assessment Report 5. 2014. Available online: https://www.ipcc.ch/report/ar5/wg2/ (accessed on 27 February 2019).
- Rede Nossa São Paulo, Atlas da Desigualdade 2018. Available online: https://www.cidadessustentaveis.org.br/arquivos/mapa_desigualdade_2018_apresentacao.pdf (accessed on 20 February 2019).
- Rauh, V.A.; Landrigan, P.J.; Claudio, L. Housing and Health, Intersection of poverty and environmental exposures. Ann. N. Y. Acad. Sci. 2008, 1136, 276–288. [Google Scholar] [CrossRef] [PubMed]
- Branis, M.; Linhartova, M. Association between unemployment, income, education level, population size and air pollution in Czech cities: Evidence for environmental inequality? A pilot national scale analysis. Health Place 2012, 18, 1110–1114. [Google Scholar] [CrossRef]
- Hurley, F.; Hunt, A.; Cowie, H.; Holland, M.; Miller, B.; Pye, S.; Watkiss, P. Service Contract for Carrying out Cost-Benefit Analysis of Air Quality Related Issues, in Particular in the Clean Air for Europe (CAFE) Programme. AEA Technology Environment 2005. Available online: http://ec.europa.eu/environment/archives/cafe/pdf/cba_methodology_vol2.pdf (accessed on 27 February 2019).
- Ott, W.R. Concepts of human exposure to air pollution. Environ. Int. 1982, 7, 179–196. [Google Scholar] [CrossRef]
- Martins, M.C.H.; Fatigati, F.L.; Vespoli, T.C.; Martins, L.C.; Pereira, L.A.A.; Martins, M.A.; Saldiva, P.H.N.; Braga, A.L.F. Influence of socioeconomic conditions on air pollution adverse health effects in elderly people: An analysis of six regions in Sao Paulo, Brazil. J. Epidemiol. Community Health 2004, 58, 41–46. [Google Scholar] [CrossRef]
- Gouveia, N.B.; Fletcher, T. Time series analysis of air pollution and mortality: Effects by cause, age and socioeconomic status. J. Epidemiol. Community Health 2000, 54, 750–755. [Google Scholar] [CrossRef]
- Habermann, M.; Souza, M.; Prado, R.; Gouveia, N.B. Socioeconomic inequalities and exposure to traffic-related air pollution in the city of Sao Paulo, Brazil. Cad. Saude Publica 2014, 30, 119–125. [Google Scholar] [CrossRef]
- Harlan, S.L.; Ruddell, D.M. Climate change and health in cities: Impacts of heat and air pollution and potential co-benefits from mitigation and adaptation. Curr. Opin. Environ. Sustain. 2011, 3, 126–134. [Google Scholar] [CrossRef]
- Amann, M. Health Risks of Ozone from Long-Range Transboundary Air Pollution; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- Knowlton, K.; Rotkin-Ellman, M.; Geballe, L.; Max, W.; Solomon, G.M. Six climate change–related events in the United States accounted for about $14 billion in lost lives and health costs. Health Aff. 2011, 30, 2167–2176. [Google Scholar] [CrossRef]
- Costa, E.; Caetano, R.; Werneck, G.L.; Bregman, M.; Araújo, D.V.; Rufino, R. Estimated cost of asthma in outpatient treatment: A real-world study. Rev. Saúde Pública 2018, 52, 27. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.; Miraglia, S. Health impact assessment of air pollution in São Paulo, Brazil. Int. J. Environ. Res. Public Health 2016, 13, 694. [Google Scholar] [CrossRef] [PubMed]
- Kolbe, A.; Gilchrist, K.L. An extreme bushfire smoke pollution event: Health impacts and public health challenges. N. S. W. Public Health Bull. 2009, 20, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Bae, H.J.; Kang, J.E.; Lim, Y.R. Assessing the Health Vulnerability Caused by Climate and Air Pollution in Korea Using the Fuzzy TOPSIS. Sustainability 2019, 11, 2894. [Google Scholar] [CrossRef]
- Brandt, J.; Silver, J.D.; Christensen, J.H.; Andersen, M.S.; Bønløkke, J.H.; Sigsgaard, T.; Geels, C.; Gross, A.; Hansen, A.B.; Hansen, K.M.; et al. Contribution from the ten major emission sectors in Europe and Denmark to the health-cost externalities of air pollution using the EVA model system—An integrated modelling approach. Atmos. Chem. Phys. 2013, 13, 7725–7746. [Google Scholar] [CrossRef]
- CETESB (São Paulo), Relatório Anual da Qualidade do Ar do Estado de São Paulo, 2014, Divisão de Análise de dados, São Paulo, 2015. Available online: https://cetesb.sp.gov.br/ar/publicacoes-relatorios/ (accessed on 2 February 2019).
- Silva Dias, M.A.F.; Jaschke Machado, A. The Role of Local Circulations in Summertime Convective Development and Nocturnal Fog in São Paulo, Brazil. Boundary Layer Meteorol. 1997, 82, 135–157. [Google Scholar] [CrossRef]
- Oliveira, A.P.; Bornstein, R.D.; Soares, J. Annual and diurnal wind patterns in the city of São Paulo. Water Air Soil Pollut. Focus 2003, 3, 3–15. [Google Scholar] [CrossRef]
- Grell, G.A.; Peckham, S.E.; Schmitz, R.; McKeen, S.A.; Frost, G.; Skamarock, W.C.; Eder, B. Fully coupled “online” chemistry within the WRF model. Atmos. Environ. 2005, 39, 6957–6975. [Google Scholar] [CrossRef]
- Andrade, M.D.; Ynoue, R.Y.; Freitas, E.D.; Todesco, E.; Vara Vela, A.; Ibarra, S.; Martins, L.D.; Martins, J.A.; Carvalho, V.S. Air quality forecasting system for Southeastern Brazil. Front. Environ. Sci. 2015, 3, 9. [Google Scholar] [CrossRef]
- Ibarra-Espinosa, S.; Ynoue, R.; O’Sullivan, S.; Pebesma, E.; Andrade, M.D.F.; Osses, M. VEIN v0.2.2: An R package for bottom–up vehicular emissions inventories. Geosci. Model Dev. 2018, 11, 2209–2229. [Google Scholar] [CrossRef]
- LAC Equity Lab: Income Inequality—Income Distribution. The World Bank 2017. Available online: http://www.worldbank.org/en/topic/poverty/lac-equity-lab1/income-inequality/income-distribution (accessed on 10 March 2019).
- Pesquisa Nacional de Saúde—2013—Módulo de Doenças Crônicas—Colesterol, Doenças Cardiovasculares (Dcv), Acidente Vascular Cerebral (AVC) e Asma (National Health Research, 2013). Available online: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?pns/pnsqc.def (accessed on 20 January 2019).
- Fauroux, B.; Sampil, M.; Quenel, P.; Lemoullec, Y. Ozone: A trigger for hospital pediatric asthma emergency room visits. Pediatr. Pulmonol. 2000, 30, 41–46. [Google Scholar] [CrossRef]
- Santos, L.A.; Oliveira, M.A.; Faresin, S.M.; Santoro, I.L.; Fernandes, A.L. Direct costs of asthma in Brazil: A comparison between controlled and uncontrolled asthmatic patients. Braz. J. Med. Biol. Res. 2007, 40, 943–948. [Google Scholar] [CrossRef] [PubMed]
- SIGTAP—System for Management of the Table of Procedures and Medications from the National Health System in Brazil. Available online: http://sigtap.datasus.gov.br/tabela-unificada/app/sec/inicio.jsp (accessed on 14 May 2019).
- QUALAR—Online Air Quality Database of the São Paulo State Environmental Company. Available online: https://qualar.cetesb.sp.gov.br/qualar/home.do (accessed on 14 May 2019).
- European Environmental Agency Data and Maps: Exceedances of Air Quality Standards in Urban Areas 2018. Available online: https://www.eea.europa.eu/data-and-maps/indicators/exceedance-of-air-quality-limit-3/assessment-4 (accessed on 21 January 2019).
- Sicard, P.; De Marco, A.; Troussier, F.; Renou, C.; Vas, N.; Paoletti, E. Decrease in surface ozone concentrations at Mediterranean remote sites and increase in the cities. Atmos. Environ. 2013, 79, 705–715. [Google Scholar] [CrossRef]
- Salvo, A.; Geiger, F.M. Reduction in local ozone levels in urban São Paulo due to a shift from ethanol to gasoline use. Nat. Geosci. 2014, 7, 450. [Google Scholar] [CrossRef]
- Alvim, D.S.; Gatti, L.V.; Corrêa, S.M.; Chiquetto, J.B.; Rossatti, C.S.; Pretto, A.; Dos Santos, M.H.; Yamazaki, A.; Orlando, J.P.; Santos, G.M. Main ozone-forming VOCs in the city of Sao Paulo: Observations, modelling and impacts. Air Qual. Atmos. Health 2017, 10, 421–435. [Google Scholar] [CrossRef]
- Dias, D.; Antunes, A.P.; Tchepel, O. Modelling of Emissions and Energy Use from Biofuel Fuelled Vehicles at Urban Scale. Sustainability 2019, 11, 2902. [Google Scholar] [CrossRef]
- Madronich, S. Photodissociation in the atmosphere: 1. Actinic flux and the effects of ground reflections and clouds. J. Geophys. Res. Atmos. 1987, 92, 9740–9752. [Google Scholar] [CrossRef]
- Walcek, C.J.; Yuan, H.H.; Stockwell, W.R. The influence of aqueous-phase chemical reactions on ozone formation in polluted and nonpolluted clouds. Atmos. Environ. 1997, 31, 1221–1237. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Standard (8-h Ozone Average) | WHO | SP | Difference |
|---|---|---|---|
| Air Quality Standard | 100 µgm−3 | 140 µgm−3 | +40% |
| Attention Level | 160 µgm−3 | 200 µgm−3 | +25% |
| Vulnerability Criterion | Explanation |
|---|---|
| Low income | Monthly family income equal to or lower than US$500 [30]. |
| Elderly | Persons with 60 years of age or more. |
| Children | Persons with 5 years of age or less. |
| No external coating | Persons living in houses made of bricks without external isolation. |
| Asthmatics | Approximately 5% of the MASP population. 1 |
| Ozone Pollution Event | Health Event/Asthmatic or Age-Sensitive Person | Average Value for Each Health Event 1 |
|---|---|---|
| Exceedance of ozone standard (SP state and WHO) | ER visit | US$1.74 |
| Exceedance of ATT (SP state and WHO) | ER visit + hospitalization | US$10.03 |
| 8-h Ozone Average | 140 µgm−3 | 100 µgm−3 | 200 µgm−3 | 160 µgm−3 |
|---|---|---|---|---|
| Standard | AQS SP | AQS WHO | ATT SP | ATT WHO |
| Number of Exceedances (domain) | 37 | 55 | 5 | 26 |
| Size of Area (km2) | 2931 | 4138 | 116 | 1656 |
| 8-h Ozone Average | 140 µgm−3 | 100 µgm−3 | 200 µgm−3 | 160 µgm−3 |
|---|---|---|---|---|
| Standard | AQS SP | AQS WHO | ATT SP | ATT WHO |
| Total Population | 16,187,395 | 20,233,937 | 1,045,076 | 9,726,100 |
| Vulnerable Population | ||||
| Low income | 3,727,234 | 5,305,680 | 0 | 2,019,042 |
| Elderly + children | 93,169 | 107,587 | 6077 | 56,239 |
| No external coating | 1,435,927 | 1,673,286 | 48,475 | 776,048 |
| Asthmatics | 809,369 | 1,011,696 | 52,253 | 486,305 |
| Extremely Vulnerable Population | ||||
| Low-income asthmatics with no external coating | 26,332 | 38,799 | 0 | 14,088 |
| Low-income elderly + children | 20,807 | 29,641 | 0 | 11,190 |
| 8-h Ozone Average | 140 µgm−3 | 100 µgm−3 | 200 µgm−3 | 160 µgm−3 |
|---|---|---|---|---|
| Standard | AQS SP | AQS WHO | ATT SP | ATT WHO |
| Vulnerable Population | ||||
| Elderly + children | 162,114 | 187,201 | 60,952 | 564,077 |
| Asthmatics | 1,408,302 | 1,760,351 | 524,097 | 4,877,639 |
| Total Cost | 1,570,416 | 1,947,552 | 585,049 | 5,441,716 |
| Extremely Vulnerable Population | ||||
| Low income asthmatics with no external coating | 45,817 | 67,510 | 0 | 141,302 |
| Low income elderly + children | 36,204 | 51,575 | 0 | 112,235 |
| Total Cost | 82,021 | 119,085 | 0 | 253,537 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiquetto, J.B.; Silva, M.E.S.; Cabral-Miranda, W.; Ribeiro, F.N.D.; Ibarra-Espinosa, S.A.; Ynoue, R.Y. Air Quality Standards and Extreme Ozone Events in the São Paulo Megacity. Sustainability 2019, 11, 3725. https://doi.org/10.3390/su11133725
Chiquetto JB, Silva MES, Cabral-Miranda W, Ribeiro FND, Ibarra-Espinosa SA, Ynoue RY. Air Quality Standards and Extreme Ozone Events in the São Paulo Megacity. Sustainability. 2019; 11(13):3725. https://doi.org/10.3390/su11133725
Chicago/Turabian StyleChiquetto, Júlio Barboza, Maria Elisa Siqueira Silva, William Cabral-Miranda, Flávia Noronha Dutra Ribeiro, Sergio Alejandro Ibarra-Espinosa, and Rita Yuri Ynoue. 2019. "Air Quality Standards and Extreme Ozone Events in the São Paulo Megacity" Sustainability 11, no. 13: 3725. https://doi.org/10.3390/su11133725
APA StyleChiquetto, J. B., Silva, M. E. S., Cabral-Miranda, W., Ribeiro, F. N. D., Ibarra-Espinosa, S. A., & Ynoue, R. Y. (2019). Air Quality Standards and Extreme Ozone Events in the São Paulo Megacity. Sustainability, 11(13), 3725. https://doi.org/10.3390/su11133725