Measurement of Particulate Matter (PM2.5) and Health Risk Assessment of Cooking-Generated Particles in the Kitchen and Living Rooms of Apartment Houses


Abstract
1. Introduction
2. Measurement of Cooking-Generated Particles
2.1. Measurement Overview
2.2. Measurement Conditions
3. Cooking-Generated Particles and Occupant Health Risks
3.1. Assessment of the Health Risk Posed by Particulate Matter
3.2. Risk Assessment Based on Particle Exposure
4. Results
4.1. Particle Distribution by Cooking Condition
4.2. Results of the Health Risk Assessment
5. Study Limitations
- (1)
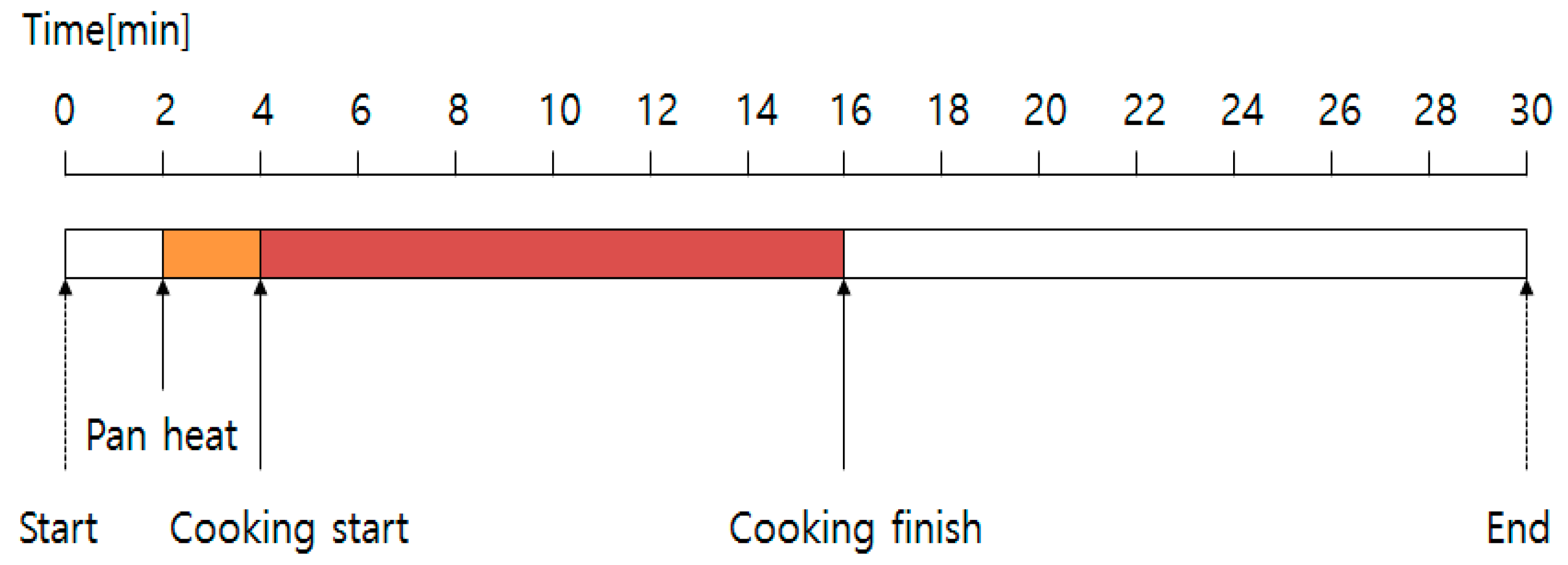
- Field measurement: There were some limitations in the field measurement process. First, Korean cuisine is comprised of a variety of dishes and styles. However, it was difficult to measure particle concentration for every particular type of food. The study was done using grilled fish, which has a large range of effects in terms of fine particles among the various available dishes that could have been chosen. In addition, it was difficult to perform long-term measurement due to logistical problems, so the measurement was performed for 30 min. After that, the prediction model was applied to the decay rate of the fine particles.
- (2)
- Exposure scenario: The main focus of the study is to suggest a method concerning the possible health risks according to the occupant scenario. The amount of time an occupant may stay at home varies depending on the occupant’s job or schedule. In this study, we constructed an exposure scenario for homemakers. The minimum concentration (20 µg/m3) was applied under the remainder of the conditions, assuming that there is no particle generating behavior other than cooking.
6. Conclusions
- (1)
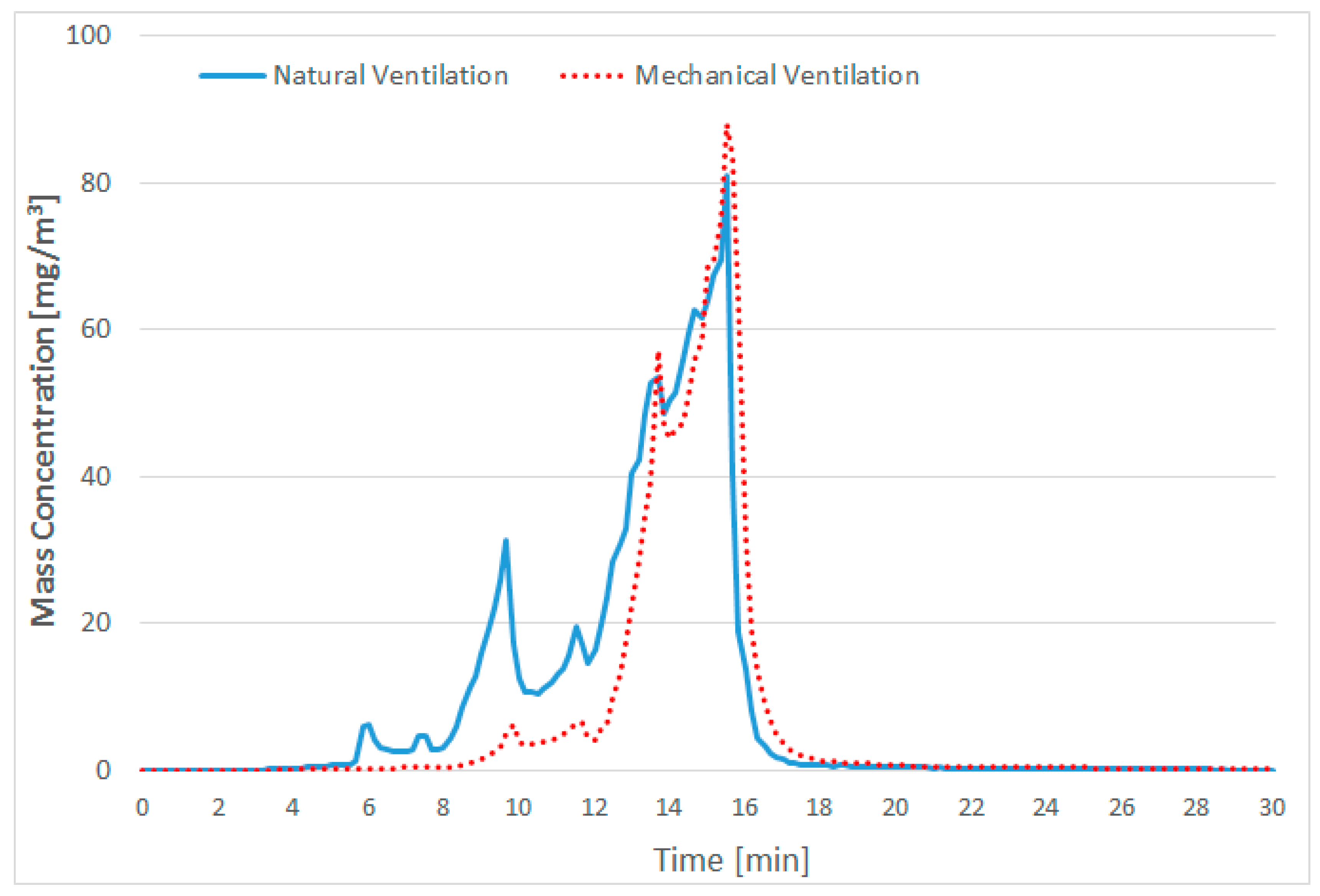
- The fine-particle emissions rapidly increase after food is heated for a certain amount of time since after the start of cooking.
- (2)
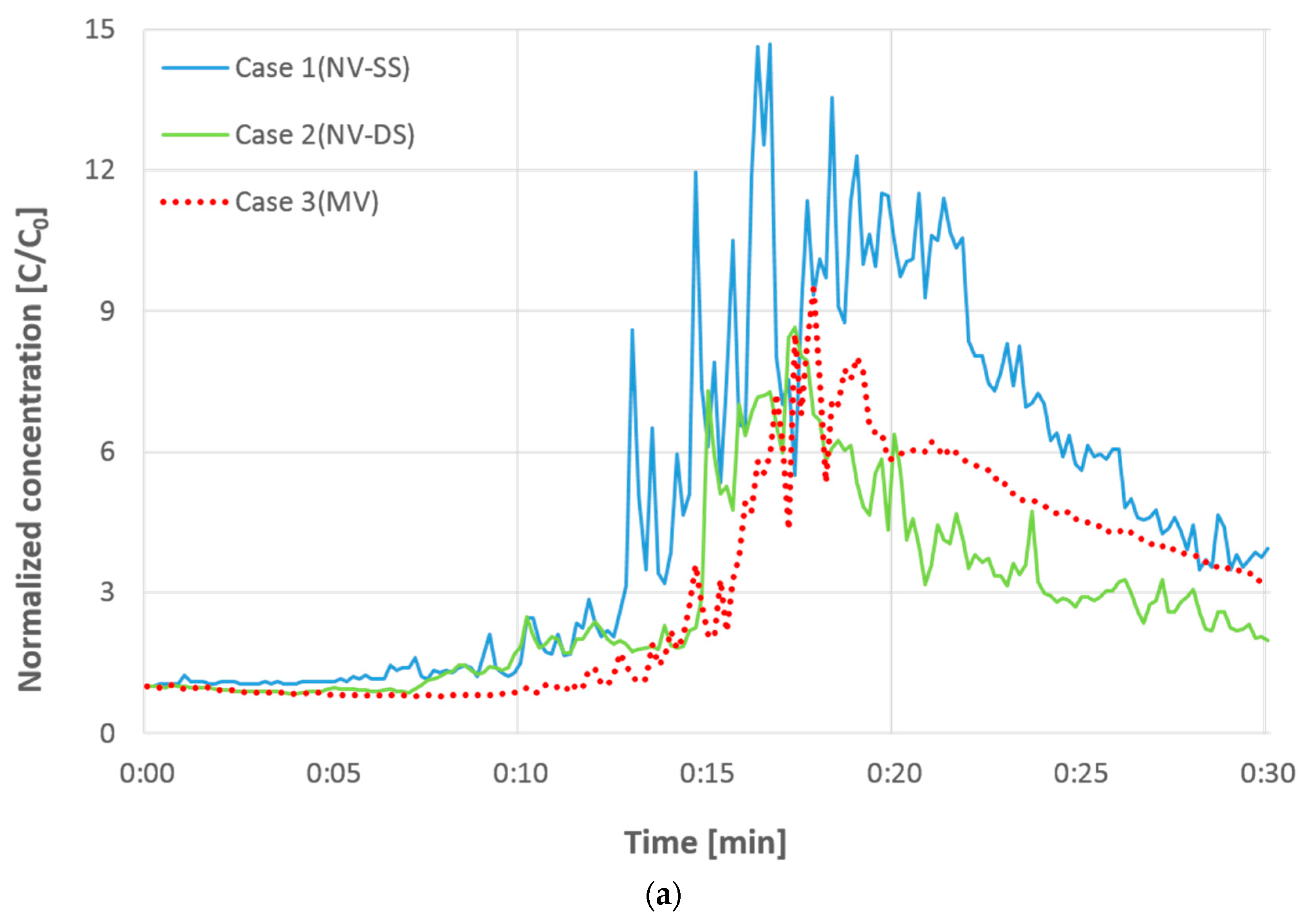
- The concentration of indoor fine particles decreases relatively more rapidly with natural ventilation than with mechanical ventilation, but the effect of fine-particle reduction is diminished if cross-ventilation is not performed properly.
- (3)
- The risk assessment results obtained in this study showed that there is no significant difference in the health risk posed by the contaminants in the kitchen and the living room, and, therefore, it is necessary to devise optimized countermeasures against the diffusion of contaminants into the living room.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dennekamp, M.; Howarth, S.; Dick, C.A.; Cherrie, J.W.; Donaldson, K.; Seaton, A. Ultrafine particles and nitrogen oxides generated. Occup. Environ. Med. 2011, 58, 511–516. [Google Scholar] [CrossRef]
- Ko, Y.C.; Cheng, L.S.; Lee, C.H.; Huang, J.J.; Huang, M.S.; Kao, E.L.; Wang, H.Z.; Lin, H.J. Chinese food cooking and lung cancer in women nonsmokers. Am. J. Epidemiol. 2000, 151, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.P.; Yang, K.R.; Chen, Y.C.; Gong, J.Y.; Chen, Y.P.; Shih, H.-C.; Lung, S.-C.C. Indoor air pollution from gas cooking in five Taiwanese families. Build. Environ. 2015, 93, 258–266. [Google Scholar] [CrossRef]
- He, C.; Morawska, L.; Hitchins, J.; Gilbert, D. Contribution from indoor sources to particle number and mass concentrations in residential houses. Build. Environ. 2004, 38, 3405–3415. [Google Scholar] [CrossRef]
- Chiang, C.M.; Chang, K.F.; Lee, C.Y.; Chou, P.C. Modelling and monitoring natural ventilation for conventional kitchens in Taiwan with transoms replaced with porous screens. Indoor Built Environ. 2006, 15, 173–178. [Google Scholar] [CrossRef]
- Lai, A.C.K.; Chen, F.Z. Modeling of cooking-emitted particle dispersion and deposition in a residential flat: A real room application. Build. Environ. 2007, 42, 3253–3260. [Google Scholar] [CrossRef]
- Lai, A.C.K.; Ho, Y.W. Spatial concentration variation of cooking-emitted particles in a residential kitchen. Build. Environ. 2008, 43, 871–876. [Google Scholar] [CrossRef]
- Gao, J.; Cao, C.; Xiao, Q.; Xu, B.; Zhou, X.; Zhang, X. Determination of dynamic intake fraction of cooking-generated particles in the kitchen. Build. Environ. 2013, 65, 146–153. [Google Scholar] [CrossRef]
- Gao, J.; Cao, C.; Zhang, X.; Luo, Z. Volume-based size distribution of accumulation and coarse particles (PM0.1–10) from cooking fume during oil heating. Build. Environ. 2013, 59, 575–580. [Google Scholar] [CrossRef]
- Gao, J.; Jian, Y.; Cao, C.; Chen, L.; Zhang, X. Indoor emission, dispersion and exposure of total particle-bound polycyclic aromatic hydrocarbons during cooking. Atmos. Environ. 2015, 120, 191–199. [Google Scholar] [CrossRef]
- Nazaroff, W.W. Indoor particle dynamics. Indoor Air 2004, 7, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III. Epidemiology of Fine Particulate Air Pollution and Human Health: Biologic Mechanisms and Who’s at Risk? Environ. Health Perspect. 2000, 108, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Hodas, N.; Loh, M.; Shin, H.M.; Li, D.; Bennett, D.; McKone, T.E.; Jolliet, O.; Weschler, C.J.; Jantunen, M.; Lioy, P. Indoor inhalation intake fractions of fine particulate matter: Review of influencing factors. Indoor Air 2016, 26, 836–856. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Afshari, A.; Bae, G.N.; Buonanno, G.; Chao, C.Y.; Hänninen, O.; Hofmann, W.; Isaxon, C.; Jayaratne, E.R.; Pasanen, P. Indoor aerosols: From personal exposure to risk assessment. Indoor Air 2013, 23, 462–487. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency (EPA). Risk Assessment Guidance for Superfund Volume 1 Human Health Evaluation Manual (Part A); EPA/540/1-89/002; EPA: Washington, DC, USA, 1989; Volume 1.
- Cannistraro, G.; Cannistraro, M.; Cannistraro, A.; Galvagno, A. Analysis of Air Pollution in the Urban Center of Four Cities Sicilian. Int. J. Heat Technol. 2016, 34, S219–S225. [Google Scholar] [CrossRef]
- Mauro, C.; Lorenzini, E. The Applications of the New Technologies “E-Sensing” in Hospitals. Int. J. Heat Technol. 2016, 34, 551–557. [Google Scholar]
- National Research Council Committee on the Institutional Means for Assessment of Risks to Public Health. Risk Assessment in the Federal Government: Managing the Process; National Academies Press: Washington, DC, USA, 1983; ISBN 0-309-03349-7.
- Integrated Risk Information System (IRIS), U.S. Environmental Protection Agency (EPA). Available online: https://www.epa.gov/iris (accessed on 15 March 2018).
- Jang, J.Y.; Jo, S.N.; Kim, S.J.; Myung, H.N.; Kim, C.I. General Factors of the Korean Exposure Factors Handbook. J. Prevent. Med. Public Health 2014, 47, 7–17. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency (US EPA). Risk Assessment Guidance for Superfund Volume 1: Human Health Evaluation Manual (Part F, Supplemental Guidance for Inhalation Risk Assessment); EPA-540-R-070-002; EPA: Washington, DC, USA, 2009.
- Greene, N.A.; Morris, V.R. Assessment of Public Health Risks Associated with Atmospheric Exposure to PM2.5 in Washington, DC, USA. Int. J. Environ. Res. Public Health 2006, 3, 86–97. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ventilation | Window Opening | Airflow Rate (CMH; m3/h) | |
|---|---|---|---|
| Case 1 | NV (supply) + rangehood | Single-sided (southern window) | 153 |
| Case 2 | NV (supply) + rangehood | Double-sided (southern, northern windows) | 154 |
| Case 3 | MV (supply) + rangehood | - | 154 |
| Factors | Value | Reference |
|---|---|---|
| Inhalation rate | 14.25 m3/day | Jang et al., 2014 [20] |
| Body weight | 62.8 kg | Jang et al., 2014 [20] |
| Exposure duration | 24 h | - |
| Average time | 70 years | USEPA data [21] |
| Unit risk (PM2.5) | 0.008 µg/m3 | Natasha G. et al., 2006 [22] |
| Case | Location | Decay Rate | Average Conc. (µg/m3) |
|---|---|---|---|
| Case 1 | Kitchen | −0.0827t + 5.8903 | 26.81 |
| Living room | −0.0978t + 6.4237 | 24.99 | |
| Case 2 | Kitchen | −0.0328t + 3.1730 | 23.91 |
| Living room | −0.0372t + 2.8866 | 22.96 | |
| Case 3 | Kitchen | −0.0438t + 4.5920 | 26.15 |
| Living room | −0.0528t + 7.1338 | 25.25 |
| Risk Factor | Location | Base | Case 1 | Case 2 | Case 3 |
|---|---|---|---|---|---|
| SF | 8.02 × 10−6 | ||||
| LADD | Kitchen | 4.54 | 6.08 | 5.43 | 5.93 |
| Living room | 5.67 | 5.21 | 5.73 | ||
| ELCR | Kitchen | 3.64 × 10−5 | 4.88 × 10−5 | 4.35 × 10−5 | 4.76 × 10−5 |
| Living room | 4.55 × 10−5 | 4.18 × 10−5 | 4.59 × 10−5 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Kang, K.; Kim, T. Measurement of Particulate Matter (PM2.5) and Health Risk Assessment of Cooking-Generated Particles in the Kitchen and Living Rooms of Apartment Houses. Sustainability 2018, 10, 843. https://doi.org/10.3390/su10030843
Kim H, Kang K, Kim T. Measurement of Particulate Matter (PM2.5) and Health Risk Assessment of Cooking-Generated Particles in the Kitchen and Living Rooms of Apartment Houses. Sustainability. 2018; 10(3):843. https://doi.org/10.3390/su10030843
Chicago/Turabian StyleKim, Hyungkeun, Kyungmo Kang, and Taeyeon Kim. 2018. "Measurement of Particulate Matter (PM2.5) and Health Risk Assessment of Cooking-Generated Particles in the Kitchen and Living Rooms of Apartment Houses" Sustainability 10, no. 3: 843. https://doi.org/10.3390/su10030843
APA StyleKim, H., Kang, K., & Kim, T. (2018). Measurement of Particulate Matter (PM2.5) and Health Risk Assessment of Cooking-Generated Particles in the Kitchen and Living Rooms of Apartment Houses. Sustainability, 10(3), 843. https://doi.org/10.3390/su10030843