

Evaluation of the Effects of Photobiomodulation on Bone Density After Placing Dental Implants: A Pilot Study Using Cone Beam CT Analysis
 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
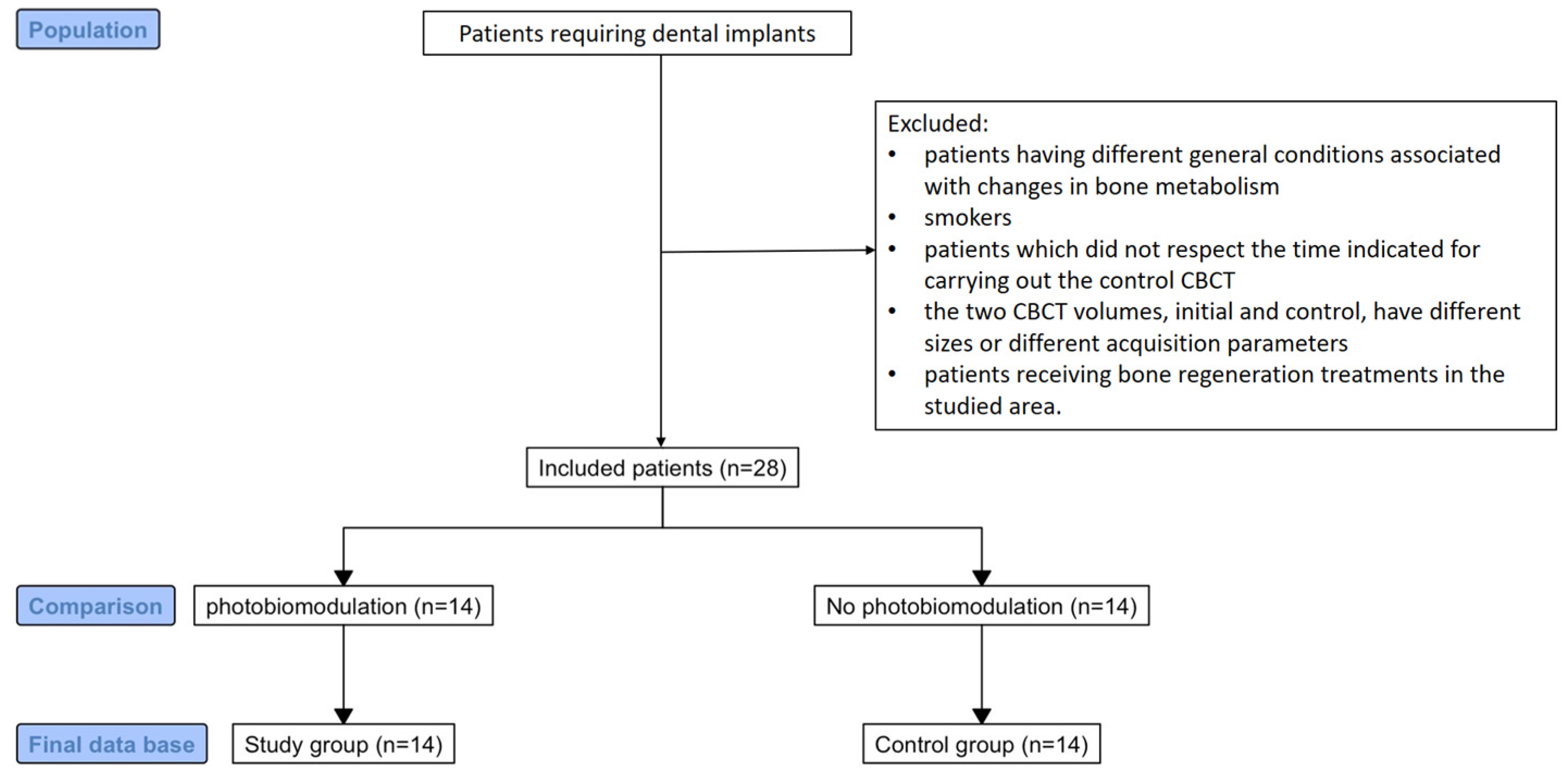
2. Materials and Methods
- Relatively healthy patient, who does not have associated general pathologies known to influence bone metabolism or drug treatments with the same effect;
- Existence of an initial CBCT investigation, prior to a surgical intervention;
- Patient underwent an oral surgery treatment (implant insertion), followed by a PBM treatment protocol of same dosage as shown below;
- The existence of a control CBCT investigation, after 8–12 months;
- The initial and the control CBCT were performed using the same device with the same acquisition parameters.
- Patients having different general conditions associated with changes in bone metabolism (diabetes mellitus, osteoporosis, bisphosphonate treatment, malignancy, renal or liver malfunctions, endocrine disorders);
- Smokers;
- Patients that did not respect the time indicated for carrying out the control CBCT
- the two CBCT volumes, initial and control, have different sizes or different acquisition parameters;
- Patients receiving bone regeneration treatments in the studied area.
3. Results
Power Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Della Coletta, B.B.; Jacob, T.B.; Moreira, L.A.C.; Pomini, K.T.; Buchaim, D.V.; Eleutério, R.G.; Pereira, E.S.B.; Roque, D.D.; Rosso, M.P.O.; Shindo, J.V.T.C.; et al. Photobiomodulation Therapy on the Guided Bone Regeneration Process in Defects Filled by Biphasic Calcium Phosphate Associated with Fibrin Biopolymer. Molecules 2021, 26, 847. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Forte, C.P.F.; Matos, A.P.; Mendes, F.H.; Dias, C.C.; Ferreira, A.E.C.; Bezerra, T.P.; Sousa, F.B.; Silva, P.G.D.B. Photobiomodulation Therapy Reduces the Inflammatory Process without Inhibiting Bone Deposition in Rats in an Extraction Model. Photobiomodul. Photomed. Laser Surg. 2020, 38, 673–678. [Google Scholar] [CrossRef]
- Pinheiro, A.; Gerbi, M. Photo-engineering of bone repair processes. Photomed. Laser Surg. 2006, 24, 169–178. [Google Scholar] [CrossRef]
- Tani, A.; Chellini, F.; Giannelli, M.; Nosi, D.; Zecchi-Orlandini, S.; Sassoli, C. Red (635 nm), Near-Infrared (808 nm) and Violet-Blue (405 nm) Photobiomodulation Potentiality on Human Osteoblasts and Mesenchymal Stromal Cells: A Morphological and Molecular In Vitro Study. Int. J. Mol. Sci. 2018, 19, 1946. [Google Scholar] [CrossRef]
- De Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 348–364. [Google Scholar] [CrossRef]
- Zein, R.; Selting, W.; Hamblin, M.R. Review of light parameters and photobiomodulation efficacy: Dive into complexity. J. Biomed. Opt. 2018, 23, 120901. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ediz, D.; Ahmet, A.; Nurettin, D.; Vakur, O.; Ertugrul, K. Evaluation of light-emitting diode photobiomodulation on bone healing of rat calvarial defects. Biotechnol. Biotechnol. Equip. 2015, 29, 758–765. [Google Scholar] [CrossRef]
- Kuzu, T.E.; Öztürk, K.; Gürgan, C.A.; Üşümez, A.; Yay, A.; Göktepe, Ö. Effect of Photobiomodulation Therapy on Peri-Implant Bone Healing in Extra-Short Implants in a Rabbit Model: A Pilot Study. Photobiomodul. Photomed. Laser Surg. 2022, 40, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Luca, R.E.; Todea, C.D.; Duma, V.F.; Bradu, A.; Podoleanu, A.G. Quantitative assessment of rat bone regeneration using complex master-slave optical coherence tomography. Quant. Imaging Med. Surg. 2019, 9, 782–798. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Luca, R.E.; Giuliani, A.; Mănescu, A.; Heredea, R.; Hoinoiu, B.; Constantin, G.D.; Duma, V.-F.; Todea, C.D. Osteogenic Potential of Bovine Bone Graft in Combination with Laser Photobiomodulation: An Ex Vivo Demonstrative Study in Wistar Rats by Cross-Linked Studies Based on Synchrotron Microtomography and Histology. Int. J. Mol. Sci. 2020, 21, 778. [Google Scholar] [CrossRef]
- Semez, G.; Luca, R.E.; Cescato, A.; Faoro, V.; Mocuţa, D.E.; Todea, D.C.M. Effect of the laser beam on implant site preparation: A preliminary pilot study. Rom. J. Morphol. Embryol. 2018, 59, 861–867. [Google Scholar] [PubMed]
- Semez, G.; Cescato, A.; Luca, R.E.; Tonetti, L.; Todea, D.C. A Comparative Analysis Regarding the Osseointegration of Immediate Loaded Implants Using Two Different Implant Site Preparations: Erbium:Yttrium-Aluminum-Garnet Laser Versus Surgical Conventional Way-An In Vivo and Histological Animal Study. Photobiomodul. Photomed. Laser Surg. 2021, 39, 70–80. [Google Scholar] [CrossRef]
- da Silva Campos, M.J.; de Souza, T.S.; Mota Júnior, S.L.; Fraga, M.R.; Vitral, R.W.F. Bone mineral density in cone beam computed tomography: Only a few shades of gray. World J. Radiol. 2014, 6, 607–612. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- White, S.C.; Pharoah, M.J. The evolution and application of dental maxillofacial imaging modalities. Dent. Clin. N. Am. 2008, 52, 689–705. [Google Scholar] [CrossRef] [PubMed]
- Isayev, A.; Velieva, N.; Isedisha, L.; Isayeva, Z.; Kamburoğlu, K.; Kuyumcu, F. Cone-Beam Computed Tomography as a Prediction Tool for Osteoporosis in PostmenopausalWomen: A Systematic Literature Review. Diagnostics 2023, 13, 1027. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, H.; Moreira-Gonçalves, D.; Coriolano, H.J.; Duarte, J.A. Bone quality: The determinants of bone strength and fragility. Sports Med. 2014, 44, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Turkyilmaz, I.; McGlumphy, E.A. Influence of bone density on implant stability parameters and implant success: A retrospective clinical study. BMC Oral Health 2008, 8, 32. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Burghardt, A.J.; Link, T.M.; Majumdar, S. High-resolution computed tomography for clinical imaging of bone microarchitecture. Clin. Orthop. Relat. Res. 2011, 469, 2179–2193. [Google Scholar] [CrossRef] [PubMed]
- Hatcher, D.C. Operational principles for cone-beam computed tomography. J. Am. Dent. Assoc. 2010, 141 (Suppl. S3), 3S–6S. [Google Scholar] [CrossRef]
- Farman, A.G. Field of view. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2009, 108, 477–478. [Google Scholar] [CrossRef]
- Naitoh, M.; Katsumata, A.; Mitsuya, S.; Kamemoto, H.; Ariji, E. Measurement of mandibles with microfocus x-ray computerized tomography and compact computerized tomography for dental use. Int. J. Oral Maxillofac. Implants 2004, 19, 239–246. [Google Scholar] [PubMed]
- Hua, Y.; Nackaerts, O.; Duyck, J.; Maes, F.; Jacobs, R. Bone quality assessment based on cone beam computed tomography imaging. Clin. Oral Implants Res. 2009, 20, 767–771. [Google Scholar] [CrossRef]
- Schulze, R.; Heil, U.; Gross, D.; Bruellmann, D.D.; Dranischnikow, E.; Schwanecke, U. Artifacts in CBCT: A review. Dentomaxillofac. Radiol. 2011, 40, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Araki, K.; Okano, T. The effect of surrounding conditions on pixel value of cone beam computed tomography. Clin. Oral Implants Res. 2013, 24, 862–865. [Google Scholar] [CrossRef]
- Maes, F.; Collignon, A.; Vandermeulen, D.; Marchal, G.; Suetens, P. Multimodality image registration by maximization of mutual information. IEEE Trans. Med. Imaging 1997, 16, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Nackaerts, O.; Maes, F.; Yan, H.; Souza, P.C.; Pauwels, R.; Jacobs, R. Analysis of intensity variability in multislice and cone beam computed tomography. Clin. Oral Implant. Res. 2011, 22, 873–879. [Google Scholar] [CrossRef]
- Aranyarachkul, P.; Caruso, J.; Gantes, B.; Schulz, E.; Riggs, M.; Dus, I. Bone density assessments of dental implant sites: 2. Quantitative cone-beam computerized tomography. Int. J. Oral Maxillofac. Implants 2005, 20, 416–424. [Google Scholar]
- Naitoh, M.; Hirukawa, A.; Katsumata, A.; Ariji, E. Evaluation of voxel values in mandibular cancellous bone: Relationship between cone-beam computed tomography and multislice helical computed tomography. Clin. Oral Implants Res. 2009, 20, 503–506. [Google Scholar] [CrossRef]
- Naitoh, M.; Hirukawa, A.; Katsumata, A.; Ariji, E. Prospective study to estimate mandibular cancellous bone density using large-volume cone-beam computed tomography. Clin. Oral Implants Res. 2010, 21, 1309–1313. [Google Scholar] [CrossRef]
- Nomura, Y.; Watanabe, H.; Honda, E.; Kurabayashi, T. Reliability of voxel values from cone-beam computed tomography for dental use in evaluating bone mineral density. Clin. Oral Implants Res. 2010, 21, 558–562. [Google Scholar] [CrossRef]
- Lagravère, M.O.; Fang, Y.; Carey, J.; Toogood, R.W.; Packota, G.V.; Major, P.W. Density conversion factor determined using a cone-beam computed tomography unit NewTom QR-DVT 9000. Dentomaxillofac. Radiol. 2006, 35, 407–409. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, R.C.; Leles, C.R.; Normanha, L.M.; Lindh, C.; Ribeiro-Rotta, R.F. Assessments of trabecular bone density at implant sites on CT images. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2008, 105, 231–238. [Google Scholar] [CrossRef]
- Kennedy, D.W.; Bolger, W.; Zinreich, S. (Eds.) Diseases of the Sinuses: Diagnosis and Management; BC. Decker Inc.: Hamilton, ON, Canada, 2001; pp. 1–12. [Google Scholar]
- Rice, D.H.; Schaefer, S.D. (Eds.) Endoskopik Paranasal Sinus Surgery; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2003; pp. 1–72. (In Turkish) [Google Scholar]
- Çakur, B.; Sümbüllü, M.A.; Durna, N.B. Aplasia and agenesis of the frontal sinus in Turkish individuals: A retrospective study using dental volumetric tomography. Int. J. Med. Sci. 2011, 8, 278–282. [Google Scholar] [CrossRef]
- Orhan, K. Diş Hekimilıkden konik isınli komputerize tomographinin (KIBT) yeri ve ışımı. Yeditepe J. Dent. 2012, 3, 6–17. (In Turkish) [Google Scholar]
- Mozzo, P.; Procacci, C.; Tacconi, A. A new volumetric ct machine for dental imaging based on the cone-beam technique: Preliminary results. Eur. Radiol. 1998, 8, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Harorli, A.; Akgül, M.; Yilmaz, B. Ağiz, Diş ve Çene Radiolojisi, 1st ed.; Nobel Tip Kitabevi: İstanbul, Türkiye, 2014; pp. 219–529. (In Turkish) [Google Scholar]
- Aktuna, B.C.; Adiguzel, O.; Bud, M. Mandibular buccal bone thickness in southeastern Anatolian people: A Cone-Beam Computed Tomography Study. Int. Dent. Res. 2017, 7, 6–12. [Google Scholar] [CrossRef]
- Eggesba, H.B. Radiological imaging of inflammatory lesions in the nasal cavity and paranasal sinuses. Eur. Radiol. 2006, 16, 872–888. [Google Scholar] [CrossRef]
- Triulzi, F.; Zirpoli, S. Imaging techniques in the diagnosis and management of rhinosinusitis in children. Pediatr. Allergy Immunol. 2007, 18, 46–49. [Google Scholar] [CrossRef]
- Anzai, Y.; Yueh, B. Imaging evaluation of sinusitis: Diagnostic performance and impact on health outcome. Neuroimaging Clin. N. Am. 2003, 13, 251–263. [Google Scholar] [CrossRef]
- Weber, A.L. History of head and neck radiology. Past, present and future. Radiology 2001, 218, 15–24. [Google Scholar] [CrossRef]
- Oliveira, M.L.; Tosoni, G.M.; Lindsey, D.H.; Mendoza, K.; Tetradis, S.; Mallya, S.M. Influence of anatomical location on CT numbers in cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Ovidiu, D.; Leretter, M.; Neagu, A. The quality of trabecular bone assessed using cone-beam computed tomography. Rom. J. Biopys. 2014, 24, 227–241. [Google Scholar]
- Gulsahi, A. Bone quality assessment for dental implants. In Implant Dentistry—The Most Promising Discipline of Dentistry; Turkyilmaz, I., Ed.; InTech: Rijeka, Croatia, 2011; Chapter 20; pp. 437–452. [Google Scholar]
- Mah, P.; Reeves, T.E.; McDavid, W.D. Deriving Hounsfield units using gray levels in cone beam computed tomography. Dentomaxillofac. Radiol. 2010, 39, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Bäuerle, T.; Pan, L.; Dimitrakopoulou-Strauss, A.; Strauss, L.G.; Heiss, C.; Schnettler, R.; Semmler, W.; Cao, L. Calibration of cone beam CT using relative attenuation ratio for quantitative assessment of bone density: A small animal study. Int. J. Comput. Assist. Radiol. Surg. 2013, 8, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Naitoh, M.; Aimiya, H.; Hirukawa, A.; Ariji, E. Morphometric analysis of mandibular trabecular bone using cone beam computed tomography: An in vitro study. Int. J. Oral Maxillofac. Implants 2010, 25, 1093–1098. [Google Scholar] [PubMed]
- Kachelriess, M.; Sourbelle, K.; Kalender, W.A. Empirical cupping correction: A first-order raw data precorrection for conebeam computed tomography. Med. Phys. 2006, 33, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- Bilhan, H.; Arat, S.; Geçkili, O. Hekimin implant cerrahisi sirasinda hissettiği kemik direnci ile radyografiden elde edilen hounsfield ünitesi değerlerinin karşilaştirilmasi: Bir pilotçalişma. Gazi Üniversitesi Dişhekimliği Fakültesi Derg. 2012, 29, 19–24. [Google Scholar]
- Misch, C.E. Contemporary Implant Dentistry, 3rd ed.; Mosby Inc.: St. Louis, MO, USA, 2008. [Google Scholar]
- Parsa, A.; Ibrahim, N.; Hassan, B.; Motroni, A.; van der Stelt, P.; Wismeijer, D. Reliability of voxel gray values in cone beam computed tomography for preoperative implant planning assessment. Int. J. Oral Maxillofac. Implants. 2012, 27, 1438–1442. [Google Scholar]
- Ibrahim, N.; Parsa, A.; Hassan, B.; van der Stelt, P.; Aartman, I.H.; Wismeijer, D. Accuracy of trabecular bone microstructural measurement at planned dental implant sites using cone-beam CT datasets. Clin. Oral Implants Res. 2014, 25, 941–945. [Google Scholar] [CrossRef]
- Ogura, I.; Sasaki, Y.; Sue, M.; Oda, T.; Kameta, A.; Hayama, K. Aging and cortical bone density of mandible with CBCT. Int. J. Diagn. Imagiang 2018, 5, 10. [Google Scholar] [CrossRef]
- Saadawy, L.; Fahmy, R.; Matrawy, K.; Zeitoun, M.; Gaweesh, Y. Relation of cone beam computed tomography assessment of mandibular bone density to dual energy x-ray absorptiometry in type 2 diabetes mellitus patients. Alex. Dent. J. 2019, 44, 87–92. [Google Scholar] [CrossRef]
- Marquezan, M.; Lau, T.C.L.; Mattos, C.T.; Cunha, A.C.d.; Nojima, L.I.; Sant’Anna, E.F. Bone mineral density. Angle Orthod. 2012, 82, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Barngkgei, I.; AI Haffar, I.; Khattab, R. Osteoporosis prediction from the mandible using cone-beam computed tomography. Imaging Sci. Dent. 2014, 44, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Güngör, E.; Yildirim, D.; Cevik, R. Evaluation of osteoporosis in jaw bones using cone beam CT and dual-energy X-ray absorptiometry. J. Oral Sci. 2016, 58, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Guerra, E.N.S.; Almeida, F.T.; Bezerra, F.V.; Figueiredo, P.T.D.S.; Silva, M.A.G.; De Luca Canto, G. Capability of CBCT to identify patients with low bone mineral density:a systematic review. Dentomaxillofac. Radiol. 2017, 46, 20160475. [Google Scholar] [CrossRef]
- Ibrahim, N.; Parsa, A.; Hassan, B.; van der Stelt, P.; Aartman, I.H.; Nambiar, P. Influence of object location in different FOVs on trabecular bone microstructure measurements of human mandible: A cone beam CT study. Dentomaxillofac. Radiol. 2014, 43, 20130329. [Google Scholar] [CrossRef]
- Çolak, M. An Evaluation of Bone Mineral Density Using Cone Beam Computed Tomography in Patients with Ectodermal Dysplasia: A Retrospective Study at a Single Center in Turkey. Med. Sci. Monit. 2019, 25, 3503–3509. [Google Scholar] [CrossRef]
- Semez, G.; Todea, C.; Mocuta, D.; Sas, I.T.; Luca, R. Chemical and Morphologic Analysis of Titanium Dental Implants: X-ray Photoemission Techniques (XPS) and Scanning Electron Microscopy (SEM) with EDX Analysis. Rev. Chim. 2018, 69, 474–477. [Google Scholar] [CrossRef]
- Lu, P.; Peng, J.; Liu, J.; Chen, L. The role of photobiomodulation in accelerating bone repair. Prog. Biophys. Mol. Biol. 2024, 188, 55–67. [Google Scholar] [CrossRef]
- Zhu, L.; Gao, X.; Lv, Y.; Yu, S.; Tang, L.; Liu, T.C. Integrated dose-effect relationship of near-infrared light-emitting diode light on bone regeneration in disuse osteoporosis rats. Photobiomodul. Photomed. Laser Surg. 2023, 41, 312–319. [Google Scholar] [CrossRef]
- Na, S.; TruongVo, T.; Jiang, F.; Joll, J.; Guo, Y.; Utreja, A.; Chen, J. Dose analysis of photobiomodulation therapy on osteoblast, osteoclast, and osteocyte. J. Biomed. Opt. 2018, 23, 075008. [Google Scholar] [CrossRef] [PubMed]
- Vigliar, M.F.R.; Marega, L.F.; Duarte, M.A.H.; Alcalde, M.P.; Rosso, M.P.d.O.; Ferreira Junior, R.S.; Barraviera, B.; Reis, C.H.B.; Buchaim, D.V.; Buchaim, R.L. Photobiomodulation Therapy Improves Repair of Bone Defects Filled by Inorganic Bone Matrix and Fibrin Heterologous Biopolymer. Bioengineering 2024, 11, 78. [Google Scholar] [CrossRef] [PubMed]
- Rando, R.G.; Buchaim, D.V.; Cola, P.C.; Buchaim, R.L. Effects of Photobiomodulation Using Low-Level Laser Therapy on Alveolar Bone Repair. Photonics 2023, 10, 734. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nr. Crt. | Patient | Sex | Age | Systemic Disease/Medication | Implant Site |
|---|---|---|---|---|---|
| 1. | T.B. | M | 74 | Ischemic heart disease | 1.2, 1.4, 1.6, 2.2, 2.3, 2.4, 2.5 |
| 2. | D.B. | M | 24 | - | 1.2 |
| 3. | B.D. | F | 51 | - | 1.4 |
| 4. | B.M. | F | 69 | Arterial hypertension | 1.2, 1.3, 2.2, 2.3 |
| 5. | B.M. | F | 61 | - | 2.2, 2.3 |
| 6. | C.A. | F | 63 | Arterial hypertension | 2.5, 2.6 |
| 7. | F.A. | F | 72 | - | 1.4, 1.5 |
| 8. | G.I. | M | 73 | Heart failure | 2.2, 2.3 |
| 9. | I.L. | F | 60 | Arterial hypertension | 2.4, 2.6 |
| 10. | J.A. | F | 60 | - | 1.5, 2.5, 2.6 |
| 11. | L.M. | M | 40 | Chronic hepatitis B | 2.5 |
| 12. | P.I. | F | 55 | - | 1.4, 1.6, 2.4, 2.5, 2.6 |
| 13. | P.R. | M | 49 | - | 1.4 |
| 14. | S.M. | M | 52 | - | 2.4 |
| No. of Patients Included | No. of Measurements Performed | Pre-Operative Trabecular Mean HU Values | Post-Operative Trabecular Mean HU Values | |
|---|---|---|---|---|
| Study group | 14 | 79 | 530.91 | 842.55 |
| Control group | 14 | 112 | 495.19 | 462.16 |
| Group 1—F— cortical | Average difference | Standard error average | p |
| 378.4 | 114.4 | 0.011 < 0.05 |
| Group 2—M— cortical | Average difference | Standard error average | p |
| 245.6 | 102.4 | 0.025 < 0.05 |
| Group 3—F— medullar | Average difference | Standard error average | p |
| 254.1 | 75.8 | 1.28 × 10−3 < 0.05 |
| Group 4—M— medullar | Average difference | Standard error average | p |
| 284.5 | 70.0 | 1.56 × 10−4 < 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luca, R.-E.; Del Vecchio, A.; Munteanu, I.-R.; Margan, M.-M.; Todea, C.D. Evaluation of the Effects of Photobiomodulation on Bone Density After Placing Dental Implants: A Pilot Study Using Cone Beam CT Analysis. Clin. Pract. 2025, 15, 64. https://doi.org/10.3390/clinpract15030064
Luca R-E, Del Vecchio A, Munteanu I-R, Margan M-M, Todea CD. Evaluation of the Effects of Photobiomodulation on Bone Density After Placing Dental Implants: A Pilot Study Using Cone Beam CT Analysis. Clinics and Practice. 2025; 15(3):64. https://doi.org/10.3390/clinpract15030064
Chicago/Turabian StyleLuca, Ruxandra-Elena, Alessandro Del Vecchio, Ioana-Roxana Munteanu, Mădălin-Marius Margan, and Carmen Darinca Todea. 2025. "Evaluation of the Effects of Photobiomodulation on Bone Density After Placing Dental Implants: A Pilot Study Using Cone Beam CT Analysis" Clinics and Practice 15, no. 3: 64. https://doi.org/10.3390/clinpract15030064
APA StyleLuca, R.-E., Del Vecchio, A., Munteanu, I.-R., Margan, M.-M., & Todea, C. D. (2025). Evaluation of the Effects of Photobiomodulation on Bone Density After Placing Dental Implants: A Pilot Study Using Cone Beam CT Analysis. Clinics and Practice, 15(3), 64. https://doi.org/10.3390/clinpract15030064