

Computer-Guided Evaluation of the Use of Two Different Devices in the Reduction of Inferior Tooth Crowding

 ,
,
Abstract
1. Introduction
2. Materials and Methods
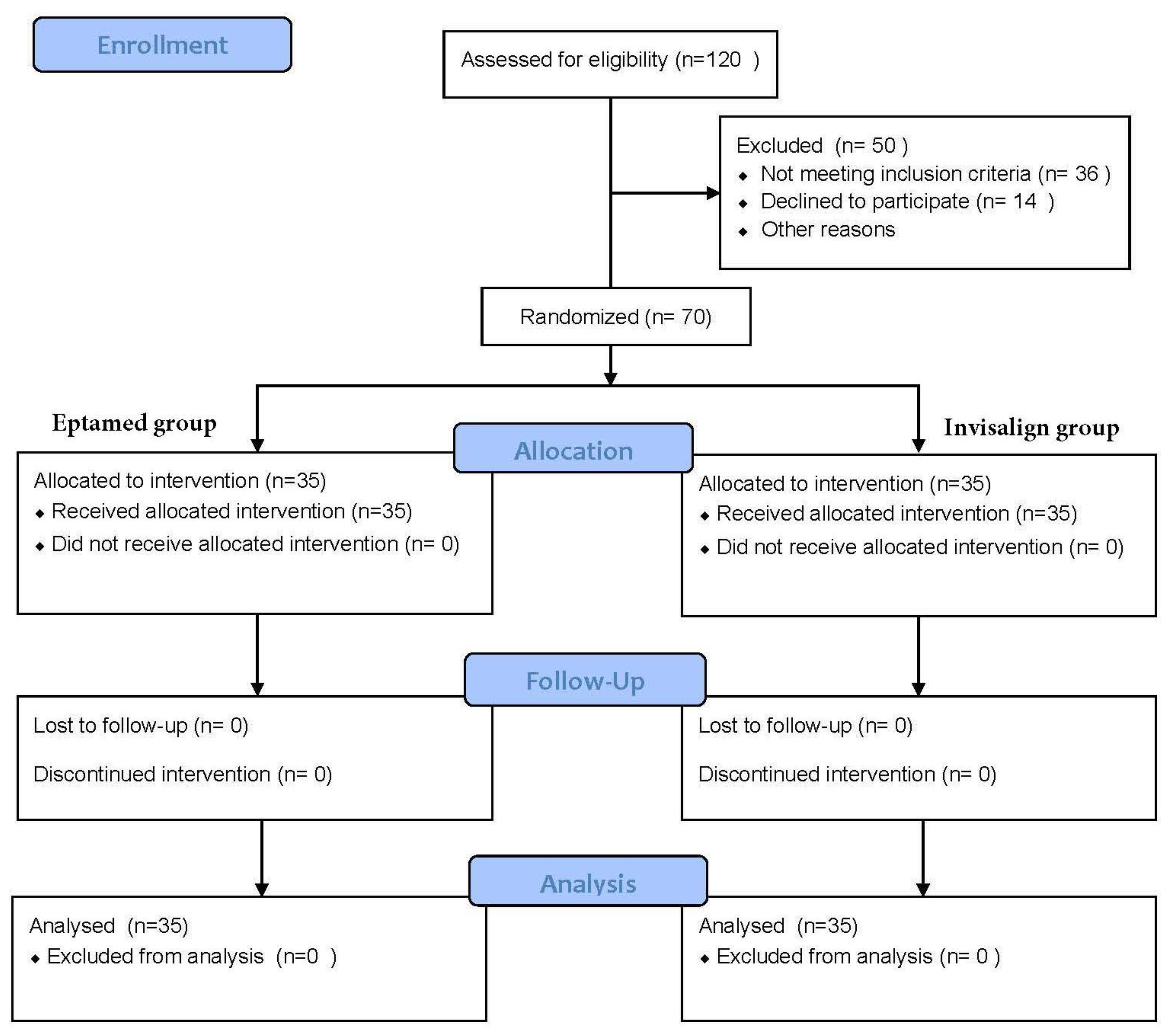
2.1. Study Population
- IOTN index >4;
- Congenitally missing permanent teeth or premature loss of deciduous or permanent teeth;
- Previous orthodontic treatment;
- Presence of epilepsy;
- Systemic disease;
- TMD;
- No written informed consent from a parent or legal guardian.
- Skeletal Class I relationship (ANB 2° +/− 2°);
- Molar Class I relationship;
- Eruption of permanent lower incisors and canines;
- Presence of moderate lower tooth crowding;
- SNA angle between 82° +/− 2 °;
- SNB angle between 80° +/− 2 °.
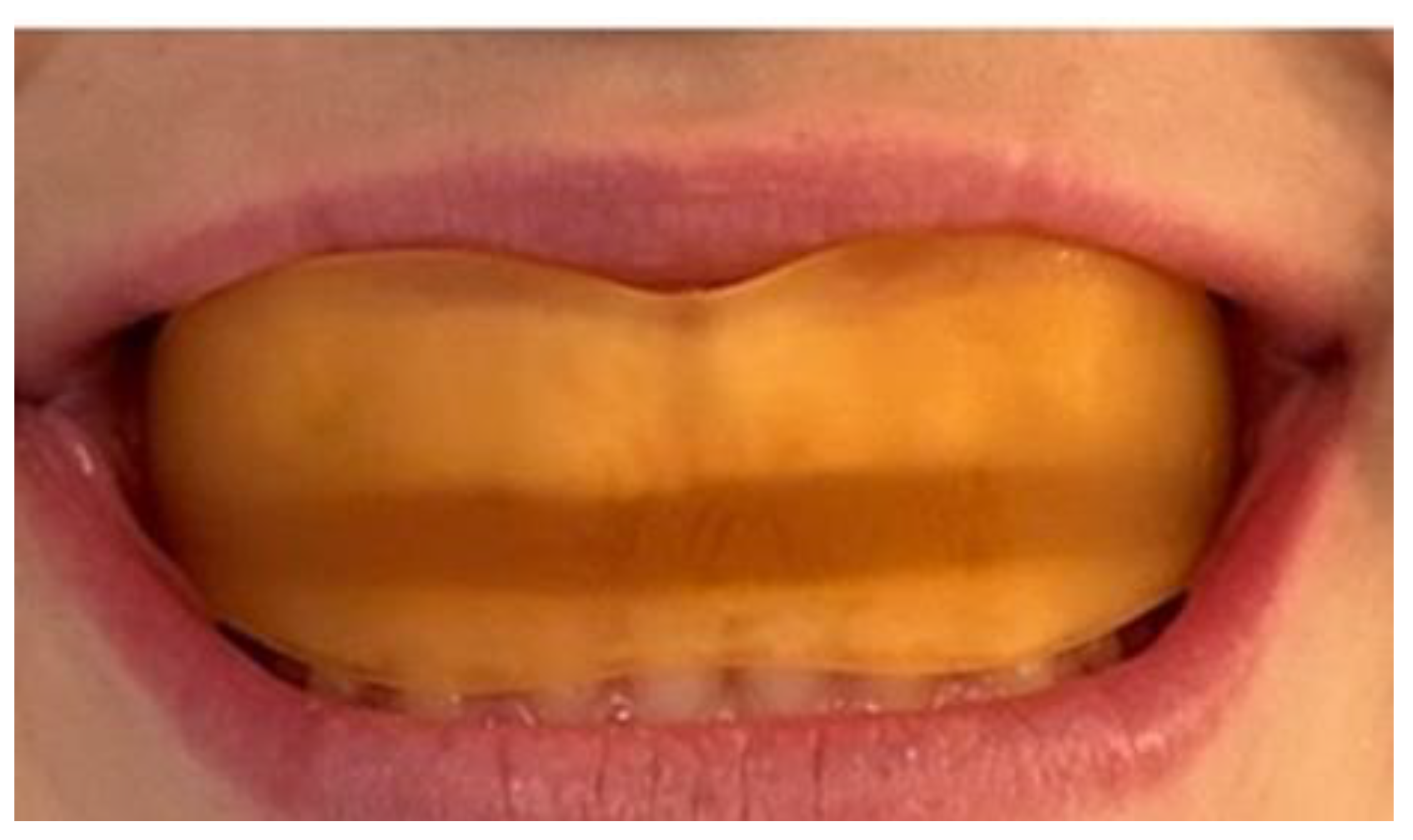
2.2. Experimental Settings
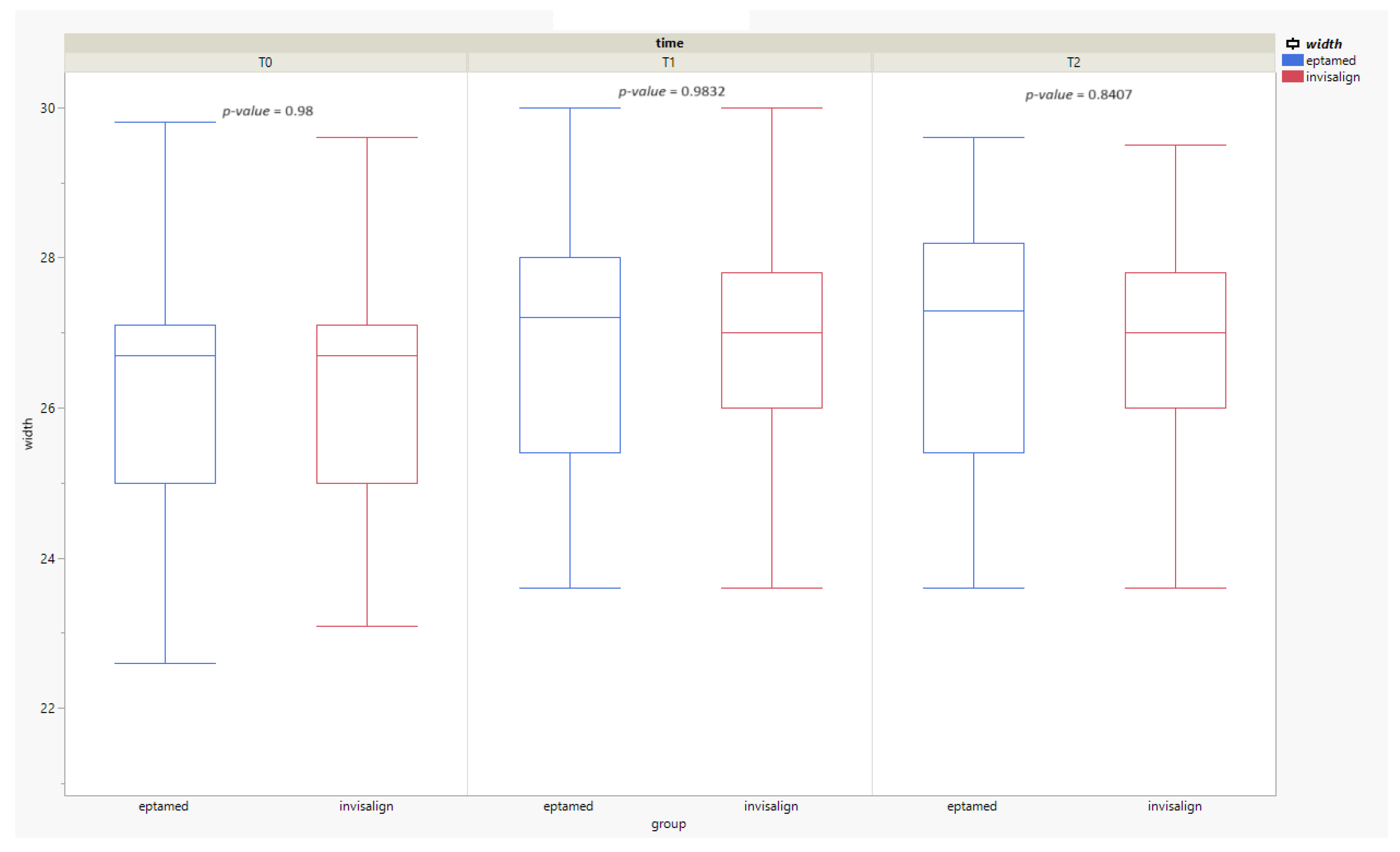
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lombardo, G.; Vena, F.; Negri, P.; Pagano, S.; Barilotti, C.; Paglia, L.; Colombo, S.; Orso, M.; Cianetti, S. Worldwide prevalence of malocclusion in the different stages of dentition: A systematic review and meta-analysis. Eur. J. Paediatr. Dent. 2020, 21, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Buschang, P.H. Class I malocclusion—The development and etiology of mandibular malaligments. Semin. Orthod. 2014, 20, 3–15. [Google Scholar] [CrossRef]
- Louly, F.; Nouer, P.R.; Janson, G.; Pinzan, A. Dental arch dimensions in the mixed dentition: A study of Brazilian children from 9 to 12 years of age. J. Appl. Oral Sci. 2011, 19, 169–174. [Google Scholar] [CrossRef]
- Stanaitytė, R.; Trakinienė, G.; Gervickas, A. Do wisdom teeth induce lower anterior teeth crowding? A systematic literature review. Stomatol. Balt. Dent. Maxillofac. J. 2014, 16, 15–18. [Google Scholar] [PubMed]
- Fields, H.W.; Sarver, D.M.; Proffit, W.R. Ortodonzia Moderna, 6th ed.; Edra Masson: Milano, Italy, 2020. [Google Scholar]
- Mortezai, O.; Rahimi, H.; Tofangchiha, M.; Radfar, S.; Ranjbaran, M.; Pagnoni, F.; Reda, R.; Testarelli, L. Relationship of the Morphology and Size of Sella Turcica with Dental Anomalies and Skeletal Malocclusions. Diagnostics 2023, 13, 3088. [Google Scholar] [CrossRef]
- Hafez, H.S.; Shaarawy, S.M.; Al-Sakiti, A.A.; Mostafa, Y.A. Dental crowding as a caries risk factor: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Alsulaiman, A.A.; Kaye, E.; Jones, J.; Cabral, H.; Leone, C.; Will, L.; Garcia, R. Incisor malalignment and the risk of periodontal disease progression. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.; E Harrison, J.; Sharif, F.N.; Owens, D.; Millett, D.T. Orthodontic treatment for crowded teeth in children. Cochrane Database Syst. Rev. 2021, CD003453. [Google Scholar] [CrossRef]
- Naish, H.; Dunbar, C.; Crouch-Baker, J.; Shah, K.; Wallis, C.; Atack, N.E.; Sherriff, M.; Sandy, J.R.; Ireland, A.J. Does a true knowledge of dental crowding affect orthodontic treatment decisions? Eur. J. Orthod. 2016, 38, 66–70. [Google Scholar] [CrossRef]
- Ortu, E.; Di Nicolantonio, S.; Severino, M.; Cova, S.; Pietropaoli, D.; Monaco, A. Effectiveness of elastodontic appliances in the treatment of malocclusions: A review of the literature. Eur. J. Paediatr. Dent. 2024, 25, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Caruso, S.; Nota, A.; Caruso, S.; Severino, M.; Gatto, R.; Meuli, S.; Mattei, A.; Tecco, S. Mandibular advancement with clear aligners in the treatment of skeletal Class II. A retrospective controlled study. Eur. J. Paediatr. Dent. 2021, 22, 26–30. [Google Scholar]
- Brook, P.H.; Shaw, W.C. The development of an index of orthodontic treatment priority. Eur. J. Orthod. 1989, 11, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Aprile, G.; Ortu, E.; Cattaneo, R.; Pietropaoli, D.; Giannoni, M.; Monaco, A. Orthodontic management by functional activator treatment: A case report. J. Med. Case Rep. 2017, 11, 336. [Google Scholar] [CrossRef]
- Muro, M.P.; Caracciolo, A.C.A.; Patel, M.P.; Feres, M.F.N.; Roscoe, M.G. Effectiveness and predictability of treatment with clear orthodontic aligners: A scoping review. Int. Orthod. 2023, 21, 100755. [Google Scholar] [CrossRef] [PubMed]
- Tepedino, M.; Paoloni, V.; Cozza, P.; Chimenti, C. Movement of anterior teeth using clear aligners: A three-dimensional, retrospective evaluation. Prog. Orthod. 2018, 19, 9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Taffarel, I.A.; Gasparello, G.G.; Mota-Júnior, S.L.; Pithon, M.M.; Taffarel, I.P.; Meira, T.M.; Tanaka, O.M. Distalization of maxillary molars with Invisalign aligners in nonextraction patients with Class II malocclusion. Am. J. Orthod. Dentofac. Orthop. 2022, 162, e176–e182. [Google Scholar] [CrossRef] [PubMed]
- Fiori, A.; Minervini, G.; Nucci, L.; D’apuzzo, F.; Perillo, L.; Grassia, V. Predictability of crowding resolution in clear aligner treatment. Prog. Orthod. 2022, 23, 43. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dai, F.-F.; Xu, T.-M.; Shu, G. Comparison of achieved and predicted tooth movement of maxillary first molars and central incisors: First premolar extraction treatment with Invisalign. Angle Orthod. 2019, 89, 679–687. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ortu, E.; Barrucci, G.; Aprile, G.; Guerrini, L.; Pietropaoli, D.; Monaco, A. Electromyographic evaluation during orthodontic therapy: Comparison of two elastodontic devices. J. Biol. Regul. Homeost. Agents 2020, 34, 1935–1939. [Google Scholar] [CrossRef] [PubMed]
- Ortu, E.; Di Nicolantonio, S.; Cova, S.; Pietropaoli, D.; De Simone, L.; Monaco, A. Efficacy of Elastodontic Devices in Temporomandibular Disorder Reduction Assessed by Computer Aid Evaluation. Appl. Sci. 2024, 14, 1651. [Google Scholar] [CrossRef]
- Patano, A.; Inchingolo, A.M.; Cardarelli, F.; Inchingolo, A.D.; Viapiano, F.; Giotta, M.; Bartolomeo, N.; Di Venere, D.; Malcangi, G.; Minetti, E.; et al. Effects of Elastodontic Appliance on the Pharyngeal Airway Space in Class II Malocclusion. J. Clin. Med. 2023, 12, 4280. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Migliaccio, S.; Aprile, V.; Zicari, S.; Grenci, A. Eruption guidance appliance: A review. Eur. J. Paediatr. Dent. 2014, 15, 163–166. [Google Scholar] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stratified by Treatment | |||
|---|---|---|---|
| Eptamed | Invisalign | p-Value | |
| Sample | 35 | 35 | |
| Sex = M (%) | 15 (42.8) | 15 (42.8) | 1000 |
| Age (mean (SD)) | 10.2 (1.5) | 10.5 (1.4) | 0.18 |
| SNA (mean (SD)) | 82.3 (1.06) | 82.5 (0.92) | 0.39 |
| SNB (mean (SD)) | 80.7 (0.94) | 80.9 (0.90) | 0.09 |
| ANB (mean (SD)) | 1.28 (0.59) | 1.36 (0.59) | 0.12 |
| T0 | T1 | T2 | |
|---|---|---|---|
| EPTAMED (lower ICW, (mean (SD))) | 26.27 (1.79) | 26.85 (1.69) | 27.0 (1.83) |
| INVISALIGN (lower ICW, (mean (SD))) | 26.21 (1.71) | 26.78 (1.66) | 26.9 (1.74) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Nicolantonio, S.; D’Angelo, M.A.; Pietropaoli, D.; Monaco, A.; Ortu, E. Computer-Guided Evaluation of the Use of Two Different Devices in the Reduction of Inferior Tooth Crowding. Clin. Pract. 2024, 14, 1185-1195. https://doi.org/10.3390/clinpract14030094
Di Nicolantonio S, D’Angelo MA, Pietropaoli D, Monaco A, Ortu E. Computer-Guided Evaluation of the Use of Two Different Devices in the Reduction of Inferior Tooth Crowding. Clinics and Practice. 2024; 14(3):1185-1195. https://doi.org/10.3390/clinpract14030094
Chicago/Turabian StyleDi Nicolantonio, Sara, Maria Ausilia D’Angelo, Davide Pietropaoli, Annalisa Monaco, and Eleonora Ortu. 2024. "Computer-Guided Evaluation of the Use of Two Different Devices in the Reduction of Inferior Tooth Crowding" Clinics and Practice 14, no. 3: 1185-1195. https://doi.org/10.3390/clinpract14030094
APA StyleDi Nicolantonio, S., D’Angelo, M. A., Pietropaoli, D., Monaco, A., & Ortu, E. (2024). Computer-Guided Evaluation of the Use of Two Different Devices in the Reduction of Inferior Tooth Crowding. Clinics and Practice, 14(3), 1185-1195. https://doi.org/10.3390/clinpract14030094