

Evaluation of Abfraction Lesions Restored with Three Dental Materials: A Comparative Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Educational Measures for Adequate Oral Hygiene Technique
2.2. Dental Materials
2.3. Filling Technique
2.4. Thermoformed Mouthguards
2.5. Assessments Criteria of the Restorations in Treated Abfraction Lesions
- -
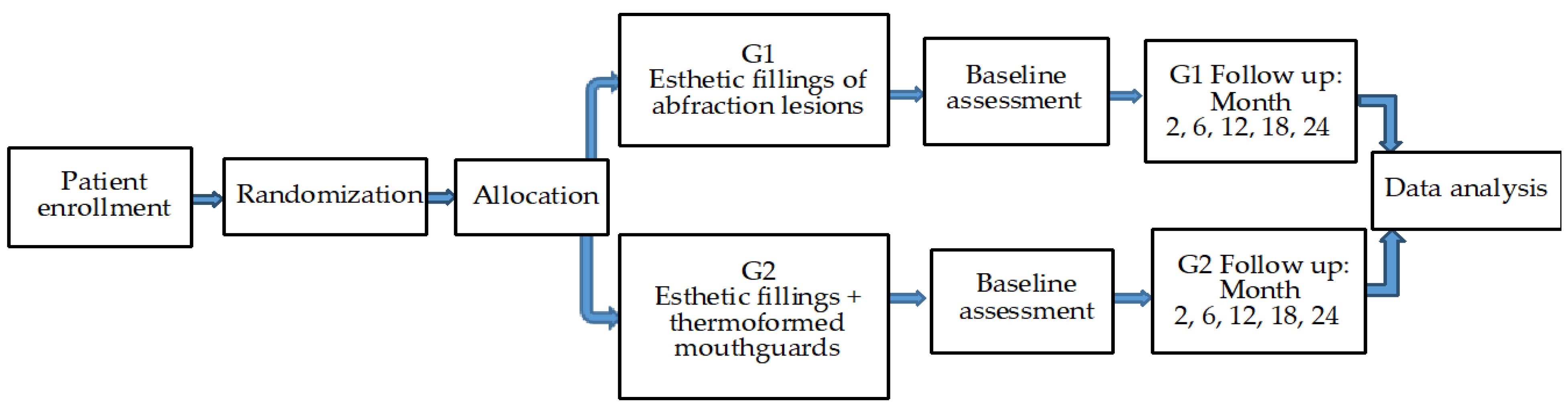
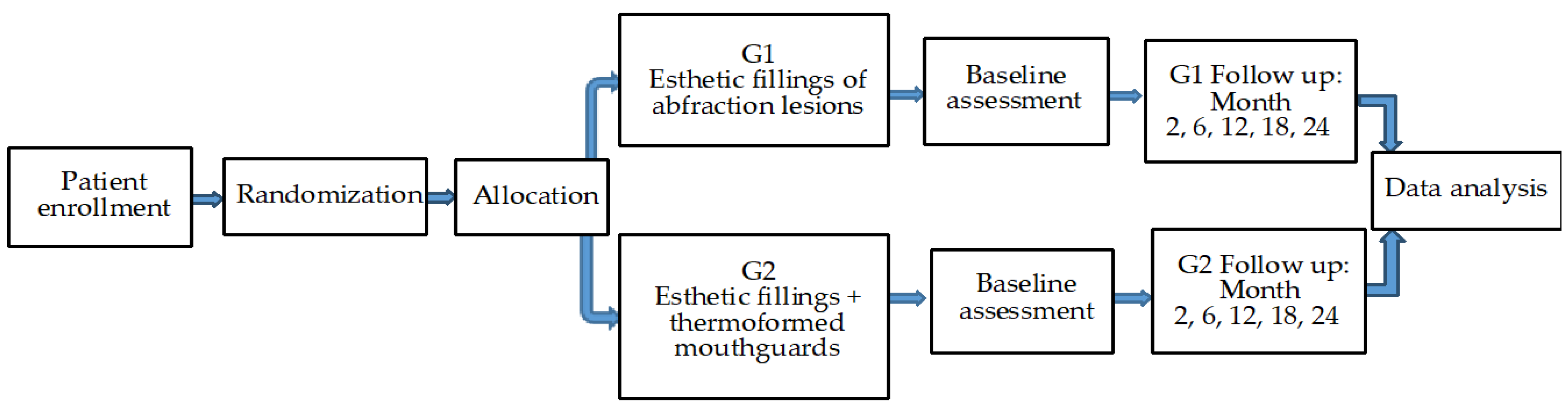
- 1st group (n = 28) with 114 aesthetic fillings for abfraction lesions (61 maxillary and 53 mandibular), where 38 fillings with GC Fuji Bulk were performed, 37 with Omnichroma Flow, and 39 with Beautifil® II;
- -
- 2nd group of patients (n = 25), with 105 esthetic fillings for the abfraction lesions (57 maxillary and 48 mandibular), where 34 fillings were accomplished with GC Fuji Bulk, 36 with Omnichroma Flow, and 35 with Beautifil® II materials; also, the treatment for the patients of this group was associated with the use of thermoformed mouthguards. Of the 118 maxillary abfractions, the most restored teeth were premolars. Maxillary abfractions were represented by 84 premolars (71.18%) and 34 canines (28.81%). Mandibular abfractions were all observed in premolars (101). Of the total 219 abfractions, 185 (=84.47%) were located at the premolars.
2.6. Statistical Analyses
3. Results
3.1. Clinical Results
- -
- -
- -
- We mention that teeth with abfraction that were restored with one of the three types of materials did not require endodontic treatment.
3.2. Statistical Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bănuț Oneț, D.; Barbu Tudoran, L.; Delean, A.G.; Șurlin, P.; Ciurea, A.; Roman, A.; Bolboacă, S.D.; Gasparik, C.; Muntean, A.; Soancă, A. Adhesion of Flowable Resin Composites in Simulated Wedge-Shaped Cervical Lesions: An In Vitro Pilot Study. Appl. Sci. 2021, 11, 3173. [Google Scholar] [CrossRef]
- Nascimento, M.M.; Dilbone, D.A.; Pereira, P.N.; Duarte, W.R.; Geraldeli, S.; Delgado, A.J. Abfraction lesions: Etiology, diagnosis, and treatment options. Clin. Cosmet. Investig. Dent. 2016, 8, 79–87. [Google Scholar] [CrossRef]
- Nguyen, K.-C.T.; Yan, Y.; Kaipatur, N.R.; Major, P.W.; Lou, E.H.; Punithakumar, K.; Le, L.H. Computer-Assisted Detection of Cemento-Enamel Junction in Intraoral Ultrasonographs. Appl. Sci. 2021, 11, 5850. [Google Scholar] [CrossRef]
- Koju, S.; Maharjan, N.; Yadav, D.K.; Bajracharya, D.; Baral, R.; Ojha, B. Morphological analysis of cementoenamel junction in permanent dentition based on gender and arches. J. Kantipur Dent. Coll. 2021, 2, 24–28. [Google Scholar]
- Goldberg, M. Non-carious cervical lesions (NCCL). J. Dent. Health Oral Disord Ther. 2021, 12, 67–72. [Google Scholar] [CrossRef]
- Zuza, A.; Racic, M.; Ivkovic, N.; Krunic, J.; Stojanovic, N.; Bozovic, D.; Bankovic-Lazarevic, D.; Vujaskovic, M. Prevalence of non-carious cervical lesions among the general population of the Republic of Srpska, Bosnia and Herzegovina. Int. Dent. J. 2019, 69, 281–288. [Google Scholar] [CrossRef]
- Medeiros, T.L.M.; Mutran, S.C.A.N.; Espinosa, D.G.; do Carmo Freitas Faial, K.; Pinheiro, H.H.C.; D’Almeida Couto, R.S. Prevalence and risk indicators of non-carious cervical lesions in male footballers. BMC Oral Health 2020, 20, 215. [Google Scholar] [CrossRef]
- Warreth, A.; Abuhijleh, E.; Almaghribi, M.A.; Mahwal, G.; Ashawish, A. Tooth surface loss: A review of literature. Saudi Dent. J. 2020, 32, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Bhullar, K.K.; Malhotra, S.; Bhagat, G.; Handa, A.; Kaur, R. Non- Carious Cervical Lesions: A Review. Sci. Prog. Res. 2021, 4, 391–399. [Google Scholar] [CrossRef]
- Peliz Senos Tróia, P.M.B.; Spuldaro, T.R.; Barroso da Fonseca, P.A.; de Oliveira Fernandes, G.V. Presence of Gingival Recession or Noncarious Cervical Lesions on Teeth under Occlusal Trauma: A Systematic Review. Eur. J. Gen. Dent. 2021, 10, 50–59. [Google Scholar] [CrossRef]
- Stănuşi, A.; Mercuţ, V.; Scrieciu, M.; Popescu, M.S.; Crăiţoiu Iacob, M.M.; Dăguci, L.; Castravete, S.; Vintilă, D.D.; Vătu, M. Effects of occlusal loads in the genesis of non-carious cervical lesions—A finite element study. Rom. J. Oral Rehabil. RJOR 2019, 11, 73–81. [Google Scholar]
- El-Marakby, A.M.; Al-Sabri, F.A.; Alharbi, S.A.; Halawani, S.M.; Yousef, M.T.B. Noncarious Cervical Lesions as Abfraction: Etiology, Diagnosis, and Treatment Modalities of Lesions: A Review Article. Dentistry 2017, 7, 438–442. [Google Scholar] [CrossRef]
- Trushkowsky, R.D. Esthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical Concepts; Springer International Publishing: Cham, Switzerland, 2020; pp. 336–339. Available online: https://books.google.ro/books?id=xqrdDwAAQBAJ&pg=PA336&lpg=PA336&dq=abfraction+Present+a+multifactorial+etiology+and+may+be+associated+with+the+pathological+wear+(abrasion,+erosion)&source=bl&ots=GW9FMEuG5J&sig=ACfU3U1H595jeLE5hw6wv0zaP0nuzTFklg&hl=ro&sa=X&ved=2ahUKEwj1nL2o58L2AhWat6QKHdXPAN4Q6AF6BAgqEAM#v=onepage&q=abfraction%20Present%20a%20multifactorial%20etiology%20and%20may%20be%20associated%20with%20the%20pathological%20wear%20(abrasion%2C%20erosion)&f=false (accessed on 13 March 2021).
- Badavannavar, A.N.; Anjari, S.; Nayak, K.; Khijmatgar, S. Abfraction: Etiopathogenesis, clinical aspect, and diagnostic-treatment modalities: A review. Indian J. Dent. Res. 2020, 31, 305–311. [Google Scholar] [PubMed]
- Mercut, V.; Popescu, S.M.; Scrieciu, M.; Amărăscu, M.O.; Vătu, M.; Diaconu, O.A.; Osiac, E.; Ghelase, Ş.M. Optical coherence tomography applications in tooth wear diagnosis. Rom. J. Morphol. Embryol. 2017, 58, 99–106. [Google Scholar]
- Tamgadge, S.; Pereira, T.; Tamgadge, A. Visualization of enamel rods in hunter-schreger bands and enamel in incipient lesion under polarized and light microscopy. Saudi J. Oral Sci. 2020, 7, 76–79. [Google Scholar] [CrossRef]
- Roberts, W.E.; Mangum, J.E.; Schneider, P.M. Pathophysiology of Demineralization, Part I: Attrition, Erosion, Abfraction, and Noncarious Cervical Lesions. Curr. Osteoporos. Rep. 2022, 20, 90–105. [Google Scholar] [CrossRef] [PubMed]
- Peumans, M.; Politano, G.; Van Meerbeek, B. Treatment of noncarious cervical lesions: When, why, and how. Int. J. Esthet. Dent. 2020, 15, 16–42. [Google Scholar]
- Rusu Olaru, A.; Popescu, M.R.; Dragomir, L.P.; Rauten, A.M. Clinical Study on Abfraction Lesions in Occlusal Dysfunction. Curr. Health Sci. J. 2019, 45, 390–397. [Google Scholar] [CrossRef]
- Demjaha, G.; Kapusevska, B.; Pejkovska-Shahpaska, B. Bruxism Unconscious Oral Habit in Everyday Life. Open Access Maced. J. Med. Sci. 2019, 7, 876–881. [Google Scholar] [CrossRef]
- Winocur-Arias, O.; Winocur, E.; Shalev-Antsel, T.; Reiter, S.; Levratovsky, S.; Emodi-Perlman, A.; Friedman-Rubin, P. Painful Temporomandibular Disorders, Bruxism and Oral Parafunctions before and during the COVID-19 Pandemic Era: A Sex Comparison among Dental Patients. J. Clin. Med. 2022, 11, 589. [Google Scholar] [CrossRef] [PubMed]
- Bustos, A.J.; Al-Talib, T.; Abubakr, N. Retrospective Analysis of the Association of Non-Carious Cervical Lesions with Bruxism. Open J. Stomatol. 2020, 10, 11–18. [Google Scholar] [CrossRef]
- Thanathornwong, B.; Suebnukarn, S. Clinical Decision Support Model to Predict Occlusal Force in Bruxism Patients. Healthc. Inform. Res. 2017, 23, 255–261. [Google Scholar] [CrossRef]
- Ladino, L.G.; Vargas, M.; Rodriguez, J.; López, E. Bruxism Management: A Comprehensive Review. Clin. Med. Rev. Case Rep 2020, 7, 316. [Google Scholar] [CrossRef]
- Beddis, H.; Pemberton, M.; Davies, S. Sleep bruxism: An overview for clinicians. Br. Dent. J. 2018, 225, 497–501. [Google Scholar] [CrossRef]
- Available online: https://www.Sensodyne.In/Blogs/Tooth-Brushing-Techniques.html (accessed on 12 April 2021).
- Perera, D.; Yu, S.C.H.; Zeng, H.; Meyers, I.A.; Walsh, L.J. Acid Resistance of Glass Ionomer Cement Restorative Materials. Bioengineering 2020, 7, 150. [Google Scholar] [CrossRef]
- Available online: https://www.gcaustralasia.com/Upload/product/pdf/1/BROCHURE_FUJI_BULK.pdf (accessed on 20 March 2019).
- Sharma, N.; Singh Samant, P. Omnichroma: The See-It -To-Believe -It Technology. EAS J. Dent. Oral Med. 2021, 3, 100–104. [Google Scholar]
- Available online: https://www.shofu.com/wp-content/uploads/Giomer-BRO-US.pdf (accessed on 22 June 2021).
- Takahashi, M.; Bando, Y. Effective thermoforming method for maintaining mouthguards thickness with a circular sheet using a circular frame. Dent. Traumatol. 2022, 38, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Cavalheiro, C.P.; Souza, P.S.; Rocha, R.O.; Mendes, F.M.; Braga, M.M.; Raggio, D.P.; Lenzi, T.L. Choosing the criteria for clinical evaluation of composite restorations: An analysis of impact on reliability and treatment decision. Pesqui. Bras. Odontopediatria Clín Integr. 2020, 20, e5088. [Google Scholar] [CrossRef]
- Marquillier, T.; Doméjean, S.; Le Clerc, J.; Chemla, F.; Gritsch, K.; Maurin, J.-C.; Millet, P.; Perard, M.; Grosgogeat, B.; Dursun, E. The use of FDI criteria in clinical trials on direct dental restorations: A scoping review. Am. J. Dent. 2018, 68, 1–9. [Google Scholar] [CrossRef]
- Nicholson, J.W. Maturation processes in glass-ionomer dental cements. Acta Biomater. Odontol. Scand. 2018, 4, 63–71. [Google Scholar] [CrossRef]
- Roberts, H.; Berzins, D.; Nicholson, J. Long-Term Water Balance Evaluation in Glass Ionomer Restorative Materials. Materials 2022, 15, 807. [Google Scholar] [CrossRef] [PubMed]
- Özcan, M.; Garcia, L.F.R.; Volpato, C.A.M. Bioactive Materials for Direct and Indirect Restorations: Concepts and Applications. Front. Dent. Med. 2021, 2, 647267. [Google Scholar] [CrossRef]
- Faridi, M.A.; Khabeer, A.; Haroon, S. Flexural Strength of Glass Carbomer Cement and Conventional Glass Ionomer Cement Stored in Different Storage Media over Time. Med. Princ. Pract. 2018, 27, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Rolim, F.G.; de Araújo Lima, A.D.; Lima Campos, I.C.; de Sousa Ferreira, R.; da Cunha Oliveira-Júnior, C.; Gomes Prado, V.L.; Vale, G.C. Fluoride Release of Fresh and Aged Glass Ionomer Cements after Recharging with High-Fluoride Dentifrice. Int. J. Dent. 2019, 2019, 9785364. [Google Scholar] [CrossRef] [PubMed]
- Ching, H.S.; Luddin, N.; Kannan, T.P.; Ab Rahman, I.; Abdul Ghani, N.R.N. Modification of glass ionomer cements on their physical-mechanical and antimicrobial properties. J. Esthet. Restor. Dent. 2018, 30, 557–571. [Google Scholar] [CrossRef] [PubMed]
- Leão, I.F.; Araújo, N.; Scotti, C.K.; Mondelli, R.F.L.; de Amoêdo Campos Velo, M.M.; Bombonatti, J.F.S. The Potential of a Bioactive, Pre-reacted, Glass-Ionomer Filler Resin Composite to Inhibit the Demineralization of Enamel in Vitro. Oper. Dent. 2021, 46, E11–E20. [Google Scholar] [CrossRef]
- Kim, H.J.; Bae, H.E.; Lee, J.E. Effects of bioactive glass incorporation into glass ionomer cement on demineralized dentin. Sci. Rep. 2021, 11, 7016. [Google Scholar] [CrossRef]
- Singh, S.; Patil, A.; Mali, S.; Jaiswal, H. Bioglass: A New Era in Modern Dentistry. Eur. J. General. Dent. 2022, 11, 1–6. [Google Scholar] [CrossRef]
- Skallevold, H.E.; Rokaya, D.; Khurshid, Z.; Zafar, M.S. Bioactive Glass Applications in Dentistry. Int. J. Mol. Sci. 2019, 20, 5960. [Google Scholar] [CrossRef]
- Sesiliana, M.; Riyanti, E. Giomer S-PRG Technology as an Alternative Restoration in Early Childhood Caries. World J. Dent. 2021, 12, 241–246. [Google Scholar] [CrossRef]
- Mayumi, K.; Miyaji, H.; Miyata, S.; Nishida, E.; Furihata, T.; Kanemoto, Y.; Sugaya, T.; Shitomi, K.; Akasaka, T. Antibacterial coating of tooth surface with ion-releasing pre-reacted glass-ionomer (S-PRG) nanofillers. Heliyon 2021, 7, e06147. [Google Scholar] [CrossRef] [PubMed]
- Colceriu Burtea, L.; Prejmerean, C.; Prodan, D.; Baldea, I.; Vlassa, M.; Filip, M.; Moldovan, M.; Moldovan, M.L.; Antoniac, A.; Prejmerean, V.; et al. New Pre-reacted Glass Containing Dental Composites (giomers) with Improved Fluoride Release and Biocompatibility. Materials 2019, 12, 4021. [Google Scholar] [CrossRef] [PubMed]
- Rusnac, M.E.; Gasparik, C.; Irimie, A.I.; Grecu, A.G.; Mesaroş, A.Ş.; Dudea, D. Giomers in dentistry—At the boundary between dental composites and glass-ionomers. Med. Pharm. Rep. 2019, 92, 123–128. [Google Scholar] [CrossRef]
- Francois, P.; Fouquet, V.; Attal, J.-P.; Dursun, E. Commercially Available Fluoride-Releasing Restorative Materials: A Review and a Proposal for Classification. Materials 2020, 13, 2313. [Google Scholar] [CrossRef]
- Pratap, B.; Gupta, R.K.; Bhardwaj, B.; Nag, M. Resin based restorative dental materials: Characteristics and future perspectives. Jpn. Dent. Sci. Rev. 2019, 55, 126–138. [Google Scholar] [CrossRef]
- Francisconi-Dos-Rios, L.F.; Tavares, J.; Oliveira, L.; Moreira, J.C.; Nahsan, F. Functional and aesthetic rehabilitation in posterior tooth with bulk-fill resin composite and occlusal matrix. Restor. Dent. Endod. 2020, 45, e9. [Google Scholar] [CrossRef]
- Baroudi, K.; Rodrigues, J.C. Flowable Resin Composites: A Systematic Review and Clinical Considerations. J. Clin. Diagn. Res. 2015, 9, ZE18–ZE24. [Google Scholar] [CrossRef]
- Omnichroma Flow. Available online: https://www.tokuyama-us.com/omnichroma-flow-dental-composite/ (accessed on 14 May 2019).
- Lai, Y.-J.; Takahashi, R.; Lin, P.-Y.; Kuo, L.; Zhou, Y.; Matin, K.; Chiang, Y.-C.; Shimada, Y.; Tagami, J. Anti-Demineralization Effects of Dental Adhesive-Composites on Enamel–Root Dentin Junction. Polymers 2021, 13, 3327. [Google Scholar] [CrossRef]
- Bezerra, I.M.; Brito, A.; de Sousa, S.A.; Santiago, B.M.; Cavalcanti, Y.W.; de Almeida, L. Glass ionomer cements compared with composite \resin in restoration of noncarious cervical lesions: A systematic review and meta-analysis. Heliyon 2020, 6, e03969. [Google Scholar] [CrossRef] [PubMed]
- Yeo, H.W.; Loo, M.Y.; Alkhabaz, M.; Li, K.C.; Choi, J.J.E.; Barazanchi, A. Bulk-Fill Direct Restorative Materials: An In Vitro Assessment of Their Physio-Mechanical Properties. Oral 2021, 1, 75–87. [Google Scholar] [CrossRef]
- Boing, T.F.; de Geus, J.L.; Wambier, L.M.; Loguercio, A.D.; Reis, A.; Gomes, O.M.M. Are Glass-Ionomer Cement Restorations in Cervical Lesions More Long-Lasting than Resin-based Composite Resins? A Systematic Review and Meta-Analysis. J. Adhes. Dent. 2018, 20, 435–452. [Google Scholar] [CrossRef] [PubMed]
- Heintze, S.D.; Loguercio, A.D.; Hanzen, T.A.; Reis, A.; Rousson, V. Clinical efficacy of resin-based direct posterior restorations and glass-ionomer restorations—An updated meta-analysis of clinical outcome parameters. Dent. Mater. 2022, 38, e109–e135. [Google Scholar] [CrossRef] [PubMed]
- Ferracane, J.L. Models of Caries Formation around Dental Composite Restorations. J. Dent. Res. 2017, 96, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Serin-Kalay, T. Discoloration of Bulk-Fill Versus Conventional Composites: A Spectrophotometric Evaluation. Odovtos Int. J. Dent. Sci. 2021, 23, 63–72. [Google Scholar] [CrossRef]
- Murariu, A.; Dinu, C.; Agop Forna, D.; Stefanescu, V.; Topor, G.; Forna, N.C.; Fotea, S.; Gurau, G.; Iordache, C. Composite Resins—Multifunctional Restorative Material and Practical Approaches in Dental Field. Mater. Plast. 2020, 57, 276–284. [Google Scholar] [CrossRef]
- Teixeira, N.; Webber, M.B.F.; Nassar, C.A.; Camilotti, V.; Mendonça, M.J.; Sinhoreti, M.A.C. Influence of Different Composites and Polishing Techniques on Periodontal Tissues near Noncarious Cervical Lesions: A Controlled, Randomized, Blinded Clinical Trial. Eur. J. Dent. 2019, 13, 635–641. [Google Scholar] [CrossRef]
- Nassar, C.A.; Nassar, P.O.; Secundes, M.B.; Ribeiro Busato, P.D.M.; Camilotti, V. Composite resin restorations of non-carious cervical lesions in patients with diabetes mellitus and periodontal disease: Pilot study. Acta Odontológica Latinoam. 2012, 25, 279–286. [Google Scholar]
- Sedghi, L.M.; Bacino, M.; Kapila, Y.L. Periodontal Disease: The Good, The Bad, and The Unknown. Front. Cell. Infect. Microbiol. 2021, 11, 766944. [Google Scholar] [CrossRef]
- Kahon, C.; Sachin, S.S.; Darsha, J. Dimensions of Periodontium (Biotype Versus Phenotype)—A Literature Review. RGUHS J. Dent. Sci. 2022, 14, 24–30. [Google Scholar]
- Malpartida-Carrillo, V.; Tinedo-Lopez, P.L.; Guerrero, M.E.; Amaya-Pajares, S.P.; Özcan, M.; Rösing, C.K. Periodontal phenotype: A review of historical and current classifications evaluating different methods and characteristics. J. Esthet. Restor. Dent. 2021, 33, 432–445. [Google Scholar] [CrossRef]
- Purushotham, S.; Manjunath, N.; D’Souza, M.L.; Shetty, R. An interdisciplinary approach for the management of noncarious lesions. J. Indian Soc. Periodontol. 2016, 20, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Srimaneepong, V.; Heboyan, A.; Zafar, M.S.; Khurshid, Z.; Marya, A.; Fernandes, G.V.O.; Rokaya, D. Fixed Prosthetic Restorations and Periodontal Health: A Narrative Review. J. Funct. Biomater. 2022, 13, 15. [Google Scholar] [CrossRef] [PubMed]
- Bechir, F.; Bataga, S.M.; Tohati, A.; Ungureanu, E.; Cotrut, C.M.; Bechir, E.S.; Suciu, M.; Vranceanu, D.M. Evaluation of the Behavior of Two CAD/CAM Fiber-Reinforced Composite Dental Materials by Immersion Tests. Materials 2021, 14, 7185. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Patients between 38–59 years of age |
| Accomplishment of correct oral hygiene |
| At least four abfraction lesions on the same dental arch (maxillary or mandibular), at the level of upper or lower premolars or upper canines, for greater blinding regarding the location of the dental material used |
| Abfraction lesions in the second stage |
| Teeth without dental and/or periodontal conditions |
| Absence of manifest occlusal wear signs, parafunctional habits, and patients without dento-maxillary anomalies |
| Non-existence of prosthetic rehabilitated or absent antagonistic teeth |
| Patients in a good health state that allows for dental therapy |
| Non-/mild smoking patients |
| Possibility to come to the dental office for dental treatments and follow-ups, as many times as necessary |
| Patient’s acceptance to participate in the study, with signed informed consent |
| Non-vital, fractured, restored teeth with abfraction lesions |
| Absent teeth or incorrect restorations on the antagonistic teeth to the selected tooth with abfraction lesion |
| Rampant caries |
| Poor oral hygiene |
| Acute or chronic periodontal diseases |
| Endodontic conditions |
| Patients diagnosed with or in treatment for dento-maxillary anomalies |
| Occlusal wear, abrasion, erosion, parafunctions Allergic responses to any of the dental materials |
| Heavy smoker patients |
| Acute and chronic systemic disorders/diseases |
| Mental disability |
| Missing data |
| Uncooperative patients with lack of compliance |
| Pregnant and lactating women |
| Patients who refused to be included in the study |
| 1st Group (Only Fillings of Abfraction Lesions) | 2nd Group (Fillings of Abfraction Lesions and Mouth Guard) | |
|---|---|---|
| No. of patients | 28 | 25 |
| Age (mean ± years) | 48.5 ± 10.5 | 48.5 ± 10.5 |
| Gender M/F | 12/16 | 14/11 |
| No. of abfraction lesions | 114 | 105 |
| Localization of abfraction lesions | 61 maxillary: 19 canines, 42 premolars 53 mandibular premolars | 57 maxillary: 15 canines, 42 premolars 48 mandibular premolars |
| Criteria | Rating | Aspect | Method |
|---|---|---|---|
| Color match | Alpha (A) | The restoration arises to fit in with the shade and translucency of adjacent hard tooth structures | Visual inspection |
| Bravo (B) | The restoration does not fit in with the shade and translucency of adjacent tooth hard structures, but the discrepancy is within the standard scale of the tooth shades | Visual inspection | |
| Charlie (C) | The restoration does not fit in with the shade and translucency of neighboring teeth structures; discrepancy is outside of the standard scale of the tooth shades and translucency | Visual inspection | |
| Marginal discoloration | Alpha (A) | No visible marginal discoloration between the restorative material color and of the neighboring hard tooth structure | Visual inspection |
| Bravo (B) | Marginal discoloration present between the hard tooth tissues and restorative material, without penetration in pulpal direction; possible to be polished | Visual inspection | |
| Charlie (C) | Marginal modification of color shade between the tooth structure and restoration; infiltration in pulpal direction | Visual inspection | |
| Surface texture | Alpha (A) | Restoration surface without any defects | Explorer |
| Bravo (B) | Restoration surface with gritty texture | Explorer | |
| Charlie (C) | Coarse surface of restoration | Explorer | |
| Anatomic contour/ form | Alpha (A) | The restoration is in the normal anatomic form, or is only a little flattened/over-contoured; by the examination of passing between the tooth tissues and the restoration margins, the tip of the dental explorer, positioned tangentially across the restoration material, does not experience two angles at the same time | Visual inspection and explorer |
| Bravo (B) | The restoration surface present an evident concavity; in the examination of passing between the tooth tissues and the restoration margins, the tip of the dental explorer, positioned tangentially across the restoration material, does not experience two angles at the same time, but the dentin or base of filling is not exposed | Visual inspection and explorer | |
| Charlie (C) | There is present a loss of restorative material, and the surface of filling present an evident concavity; the base material of filling and/or the dentin are exposed | Visual inspection and explorer | |
| Marginal adaptation /integrity | Alpha (A) | No noticeable evidence of a crack along the limit between the filling material and tooth structure | Explorer |
| Bravo (B) | Noticeable evidence of a crack along the limit between the filling material and tooth structure, in which the dental explorer penetrates or catches | Explorer | |
| Charlie (C) | The explorer penetrates in the cracked area, which extends to the dento-enamel junction, and dentin or base filling material is exposed | Explorer | |
| Secondary/recurrent caries | Alpha (A) | The restoration is in continuation of the existing anatomic tooth form | Visual inspection and explorer |
| Charlie (C) | There are visual evidences of darkish discoloration in adjoining area of the restoration; caries lesions are present and connected with the filling material | Visual inspection and explorer | |
| Retention of restoration/fracture | Alpha (A) | Restoration is intact and fully retained/fully preserved | Visual inspection |
| Bravo (B) | Restoration is partially retained, but some broken part of the filling material is present | Visual inspection | |
| Charlie (C) | Restorative material was lost in totality | Visual inspection |
| Criteria | Baseline | At 2 Months | At 6 Months | At 12 Months | At 18 Months | At 24 Months | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FuB 38 Fillings | OmF 37 Fillings | BeaII 39 Fillings | FuB 38 Fillings | OmF 37 Fillings | BeaII 39 Fillings | FuB 38 Fillings | OmF 37 Fillings | BeaII 39 Fillings | FuB 38 Fillings | OmF 37 Fillings | BeaII 39 Fillings | FuB 38 Fillings | OmF 37 Fillings | BeaII 39 Fillings | FuB 38 Fillings | OmF 37 Fillings | BeaII 39 Fillings | ||
| Color match/stability | A: n (%) | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 37 100% | 37 100% | 37 100% | 37 97.36% | 37 100% | 37 94.87% | 36 94.73% | 37 100% | 37 94.87% | 34 89.47% | 34 91.89% | 36 92.30% |
| B: n (%) | - | - | - | - | - | - | - | - | - | 1 2.63% | - | 2 5.12% | 2 5.26% | - | 2 5.12% | 3 7.89% | 3 8.10% | 2 5.12% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.63% | - | 1 2.56% | |
| Marginal discoloration | A: n (%) | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 37 97.36% | 37 100% | 38 97.43% | 37 97.36% | 37 100% | 37 94.87% | 35 92.10% | 35 94.59% | 37 94.87% |
| B: n (%) | - | - | - | - | - | - | - | - | - | 1 2.63% | - | 1 2.56% | 1 2.63% | - | 2 5.12% | 3 7.89% | 2 5.40 | 2 5.12% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | |
| Surface texture | A: n (%) | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 37 97.36% | 37 100% | 38 97.43% | 36 94.73% | 37 0% | 38 97.43% | 34 89.47% | 35 94.59% | 36 92.30% |
| B: n (%) | - | - | - | - | - | - | - | - | - | 1 2.63% | - | 1 2.56% | 2 5.26% | - | 1 2.56% | 3 7.89% | 2 5.40% | 3 7.69% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.63% | - | - | |
| Anatomical contour /form | A: n (%) | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 37 97.36% | 36 97.29% | 38 97.43% | 36 92.1 - | 36 97.29% | 38 97.43% | 35 92.10% | 36 97.29% | 37 94.87% |
| B: n (%) | - | - | - | - | - | - | - | - | - | 1 2.63% | 1 2.7% | 1 2.56% | 2 5.26% | 1 2.7% | 1 2.56% | 2 5.26% | 1 2.7% | 2 5.12% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.63% | - | - | |
| Marginaladaptation/ integrity | A: n (%) | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 37 97.36% | 37 0% | 38 97.43% | 35 92.1 - | 36 97.29% | 37 94.87% | 34 89.47% | 35 94.59% | 36 92.3% |
| B: n (%) | - | - | - | - | - | - | - | - | - | 1 2.63% | - | 1 2.56% | 1 2.63% | 1 2.7% | 1 2.56% | 3 7.89% | 2 5.40% | 2 5.12% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.63% | - | 1 2.56% | 1 2.63% | - | 1 2.56% | |
| Secondary/
recurrent caries | A: n (%) | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 37 97.36% | 37 0% | 38 97.43% | 36 94.73% | 36 97.29% | 38 97.43% | 36 94.73% | 36 97.29% | 37 94.87% |
| C: n (%) | - | - | - | - | - | - | - | - | - | 1 2.63% | - | 1 2.56% | 2 5.26% | 1 2.7% | 1 2.56% | 2 5.26% | 1 2.7% | 2 5.12% | |
| Retention of restoration/ fracture | A: n (%) | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 38 100% | 37 100% | 39 100% | 36 94.73% | 37 0% | 38 97.43% | 35 92.1 - | 36 97.29% | 38 97.43% | 34 89.47% | 35 94.59% | 36 92.3% |
| B: n (%) | - | - | - | - | - | - | - | - | - | 1 2.63% | - | 1 2.56% | 1 2.63% | 1 2.7% | 1 2.56% | 2 5.26% | 2 5.40% | 2 5.12% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | 2 5.26% | - | - | 2 5.26% | - | 1 2.56% | |
| Criteria | Baseline | At 2 Months | At 6 Months | At 12 Months | At 18 Months | At 24 Months | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FuB 34 Fillings | OmF 36 Fillings | BeaII 35 Fillings | FuB 34 Fillings | OmF 36 Fillings | BeaII 35 Fillings | FuB 34 Fillings | OmF 36 Fillings | BeaII 35 Fillings | FuB 34 Fillings | OmF 36 Fillings | BeaII 35 Fillings | FuB 34 Fillings | OmF 36 Fillings | BeaII 35 Fillings | FuB 34 Fillings | OmF 36 Fillings | BeaII 35 Fillings | ||
| Color match/stability | A: n (%) | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 0% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 32 94.11% | 35 97.22% | 33 94.28% | 30 88.23% | 34 94.44% | 32 91.42% |
| B: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | 2 5.88% | 1 2.77% | 2 5.71% | 3 8.82% | 2 5.55% | 2 5.71% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.94% | - | 1 2.85% | |
| Marginal discoloration | A: n (%) | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 32 94.11% | 36 100% | 33 94.28% | 31 91.17% | 34 94.44% | 32 91.42% |
| B: n (%) | - | - | - - | - | - | - - | - | - | - - | - | - | - | 2 5.88% | - | 2 5.71% | 3 8.82% | 2 5.55% | 3 8.57% | |
| C: n (%) | - | - | - - | - | - | - - | - | - | - - | - | - | - | - | - | - | - | - | - | |
| Surface texture | A: n (%) | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 32 94.11% | 35 97.22% | 33 94.28% | 30 88.23% | 34 94.44% | 33 94.28% |
| B: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | 2 5.88% | 1 2.77% | 2 5.71% | 3 8.82% | 2 5.55% | 2 5.71% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.94% | - | - | |
| Anatomical contour/form | A: n (%) | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 33 97.05% | 35 97.22% | 33 94.28% | 30 88.23% | 34 94.44% | 33 94.28% |
| B: n (%) | - | - |
- | - | - | - - | - | - |
- | - | - | - | 1 2.94% | 1 2.77% | 2 5.71% | 3 8.82% | 2 5.55% | 2 5.71% | |
| C: n (%) | - | - |
- | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.94% | - | - | |
| Marginaladaptation/
integrity | A: n (%) | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 31 91.17% | 35 97.22% | 33 94.28% | 31 91.17% | 34 94.44% | 32 91.42% |
| B: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | 2 5.88% | 1 2.77% | 2 5.71% | 2 5.88% | 2 5.55% | 3 8.57% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.94% | - | - | 1 2.94% | - | - | |
| Secondary/
recurrent caries | A: n (%) | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 33 97.06% | 36 100% | 35 100% | 32 94.11% | 35 97.22% | 33 94.28% |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.94% | - | - | 2 5.88% | 1 2.77% | 2 5.71% | |
| Retention of restoration/ fracture | A: n (%) | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 34 100% | 36 100% | 35 100% | 31 91.17% | 35 97.22% | 32 91.42% | 31 91.17% | 34 94.44% | 32 91.42% |
| B: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | 2 5.88% | 1 2.77% | 3 8.57% | 1 2.94% | 2 5.55% | 2 5.71% | |
| C: n (%) | - | - | - | - | - | - | - | - | - | - | - | - | 1 2.94% | - | - | 2 5.88% | - | 1 2.85% | |
| Rating for Color Match/Stability | Sum of Undesirable Scores in all Assessments (n; %) | p | |||
|---|---|---|---|---|---|
| 1st Group of Patients | 2nd Group of Patients | ||||
| Color match/stability criteria | |||||
| B: n (%) | FuB 38 fillings | 7; (18.42%) | FuB 34 fillings | 5; (13.15%) | 0.65 |
| C: n (%) | 1; (2.63%) | 1; (2.63%) | - | ||
| Cumulative undesirable scores | 8; (21.05%) | 6; (15.78%) | 0.65 | ||
| B: n (%) | OmF 37 fillings | 3; (8.10%) | OmF 36 fillings | 2; (5.55%) | 0.223 |
| C: n (%) | 0; (0%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 3; (8.10%) | 2; (5.55%) | 0.223 | ||
| B: n (%) | BeaII 39 fillings | 6; (15.38%) | BeaII 35 fillings | 4; (10.25%) | 0.709 |
| C: n (%) | 1; (2.56%) | 1; (2.85%) | - | ||
| Cumulative undesirable scores | 7; (17.94%) | 5; (12.82%) | 0.709 | ||
| Marginal discoloration | |||||
| B: n (%) | FuB 38 fillings | 5; (13.15%) | FuB 34 fillings | 5; (14.70%) | 0.233 |
| C: n (%) | 0; (0%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 5; (13.15%) | 5; (14.70%) | 0.172 | ||
| B: n (%) | OmF 37 fillings | 2; (5.40%) | OmF 36 fillings | 2; (5.55%) | 0.386 |
| C: n (%) | 0; (0%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 2; (5.40%) | 2; (5.55%) | 0.385 | ||
| B: n (%) | BeaII 39 fillings | 5; (12.82%) | BeaII 35 fillings | 5; (14.28%) | 0.361 |
| C: n (%) | 0; (%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 5; (12.82%) | 5; (14.28%) | 0.361 | ||
| Surface texture | |||||
| B: n (%) | FuB 38 fillings | 6; (15.78%) | FuB 34 fillings | 5; (14.70%) | 0.659 |
| C: n (%) | 0; (0%) | 1; (2.94%) | - | ||
| Cumulative undesirable scores | 6; (15.78%) | 6; (17.64%) | 0.659 | ||
| B: n (%) | OmF 37 fillings | 2; (5.40%) | OmF 36 fillings | 3; (8.33%) | 0.386 |
| C: n (%) | 0; (0%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 2; (5.40%) | 3; (8.33%) | 0.386 | ||
| B: n (%) | BeaII 39 fillings | 5; (12.82%) | BeaII 35 fillings | 4; (11.42%) | 0.082 |
| C: n (%) | 0; (%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 5; (12.82%) | 4; (11.42%) | 0.082 | ||
| Anatomicalcontour/form | |||||
| B: n (%) | FuB 38 fillings | 5; (13.15%) | FuB 34 fillings | 4; (11.76%) | 0.233 |
| C: n (%) | 1; (2.63%) | 1; (2.940%) | - | ||
| Cumulative undesirable scores | 6; (15.78%) | 5; (14.70%) | 0.405 | ||
| B: n (%) | OmF 37 fillings | 3; (8.1%) | OmF 36 fillings | 3; (8.33%) | 0.171 |
| C: n (%) | 0; (0%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 3; (8.1%) | 3; (8.33%) | 0.171 | ||
| B: n (%) | BeaII 39 fillings | 4; (10.25%) | BeaII 35 fillings | 4; (11.42%) | 0.136 |
| C: n (%) | 0; (%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 4; (10.25%) | 4; (11.42%) | 0.136 | ||
| Marginaladaptation/integrity | |||||
| B: n (%) | FuB 38 fillings | 5; (13.15%) | FuB 34 fillings | 4; (11.76%) | 0.082 |
| C: n (%) | 2; (5.26%) | 2; (5.88%) | 1 | ||
| Cumulative undesirable scores | 7; (19.44%) | 6; (17.64%) | 0.172 | ||
| B: n (%) | OmF 37 fillings | 3; (8.1%) | OmF 36 fillings | 3; (8.33%) | 1 |
| C: n (%) | 0; (0%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 3; (8.1%) | 3; (8.33%) | 1 | ||
| B: n (%) | BeaII 39 fillings | 5; (12.82%) | BeaII 35 fillings | 5; (14.28%) | 0.233 |
| C: n (%) | 2; (5.88%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 7; (17.94%) | 5; (14.28%) | 0.659 | ||
| Secondary/recurrent caries | |||||
| C: n (%) | FuB 38 fillings | 5; (13.15%) | FuB 34 fillings | 3; (8.82%) | 0.709 |
| Cumulative undesirable scores | 5; (13.15%) | 3; (8.82%) | 0.709 | ||
| C: n (%) | OmF 37 fillings | 2; (5.40%) | OmF 36 fillings | 1; (2.77%) | 0.34 |
| Cumulative undesirable scores | 2; (5.40%) | 1; (2.77%) | 0.34 | ||
| C: n (%) | BeaII 39 fillings | 4; (10.25%) | BeaII 35 fillings | 2; (5.71%) | 0.248 |
| Cumulative undesirable scores | 4; (10.25%) | 2; (5.71%) | 0.248 | ||
| Retention of restoration/fracture | |||||
| B: n (%) | FuB 38 fillings | 4; (10.52%) | FuB 34 fillings | 3; (8.82%) | 0.709 |
| C: n (%) | 4; (10.52%) | 3; (8.82%) | 0.248 | ||
| Cumulative undesirable scores | 8; (21.05%) | 6; (17.64%) | 0.329 | ||
| B: n (%) | OmF 37 fillings | 3; (8.1%) | OmF 36 fillings | 3; (8.33%) | 1 |
| C: n (%) | 0; (0%) | 0; (0%) | - | ||
| Cumulative undesirable scores | 3; (8.1%) | 3; (8.33%) | 0.368 | ||
| B: n (%) | BeaII 39 fillings | 4; (10.25%) | BeaII 35 fillings | 5; (14.28%) | 0.233 |
| C: n (%) | 1; (2.56%) | 1; (2.85%) | - | ||
| Cumulative undesirable scores | 5; (12.82%) | 6; (17.14%) | 0.136 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costăchel, B.C.; Bechir, A.; Burcea, A.; Mihai, L.L.; Ionescu, T.; Marcu, O.A.; Bechir, E.S. Evaluation of Abfraction Lesions Restored with Three Dental Materials: A Comparative Study. Clin. Pract. 2023, 13, 1043-1058. https://doi.org/10.3390/clinpract13050093
Costăchel BC, Bechir A, Burcea A, Mihai LL, Ionescu T, Marcu OA, Bechir ES. Evaluation of Abfraction Lesions Restored with Three Dental Materials: A Comparative Study. Clinics and Practice. 2023; 13(5):1043-1058. https://doi.org/10.3390/clinpract13050093
Chicago/Turabian StyleCostăchel, Bogdan Constantin, Anamaria Bechir, Alexandru Burcea, Laurența Lelia Mihai, Tudor Ionescu, Olivia Andreea Marcu, and Edwin Sever Bechir. 2023. "Evaluation of Abfraction Lesions Restored with Three Dental Materials: A Comparative Study" Clinics and Practice 13, no. 5: 1043-1058. https://doi.org/10.3390/clinpract13050093
APA StyleCostăchel, B. C., Bechir, A., Burcea, A., Mihai, L. L., Ionescu, T., Marcu, O. A., & Bechir, E. S. (2023). Evaluation of Abfraction Lesions Restored with Three Dental Materials: A Comparative Study. Clinics and Practice, 13(5), 1043-1058. https://doi.org/10.3390/clinpract13050093