
RETRACTED: Traditional and Recent Root Canal Irrigation Methods and Their Effectiveness: A Review



 ,
,  and
and
Abstract
:1. Introduction
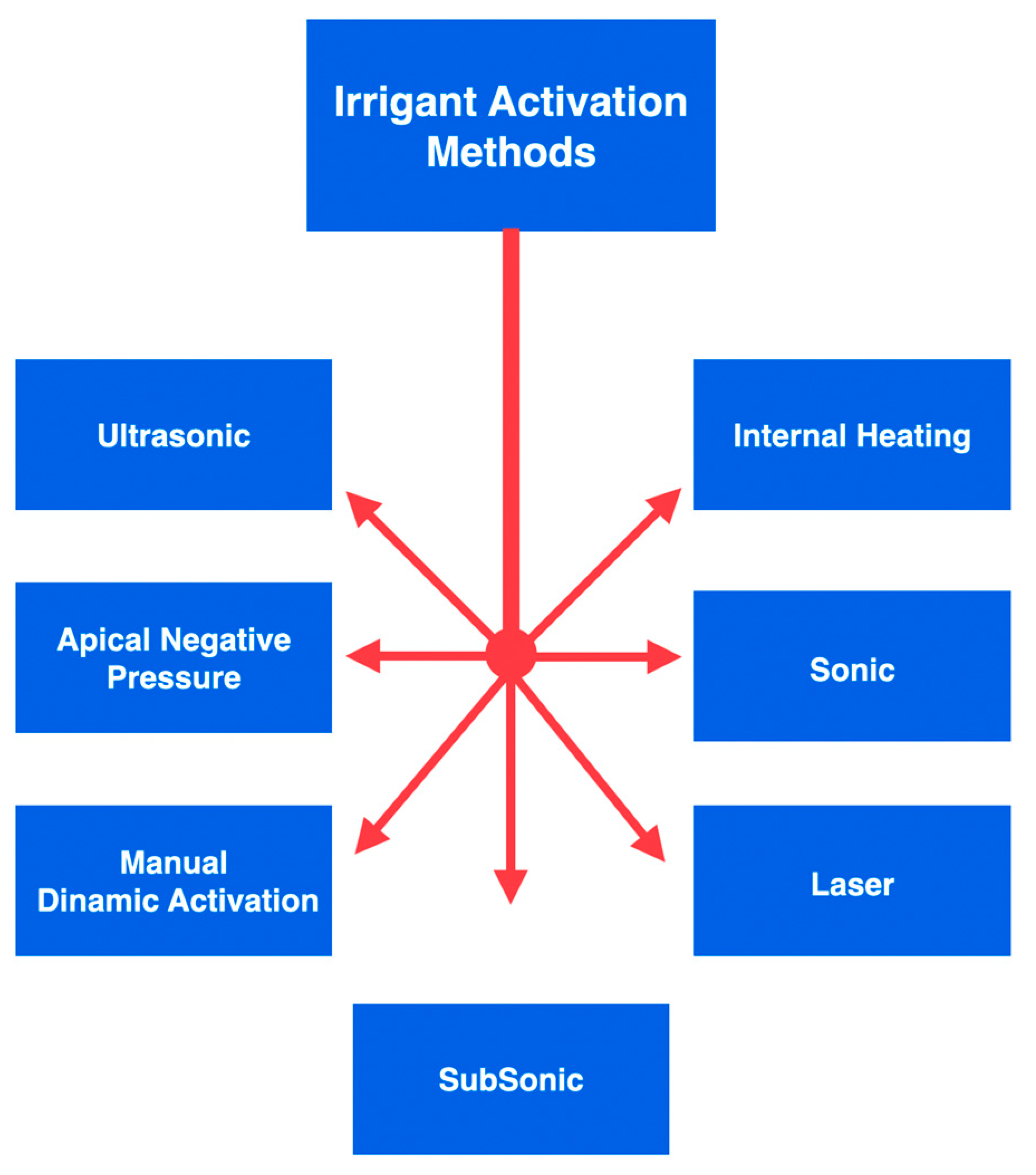
- Manual dynamic activation;
- Heating (internal or external);
- Negative apical pressure (EndoVac, Kerr Endodontics, Gilbert, AZ, USA; Rinsendo, Dürr Dental, Bietigheim, Germany);
- Subsonic technique (EndoAcivator, Dentsply Maillefer, Ballaigues, Switzerland);
- Sonic technique (EDDY, VDW, München, Germany);
- Passive ultrasonic irrigation (PUI);
- −
- Lateral canals: canals of small, medium, and large dimensions that start from the main canal at any height and communicate with the periodontium. They can be located in the root canal’s coronal third, middle third, and apical third. They can also be present in the furcation area in the case of multi-rooted teeth. By communicating with the periodontium, they can give rise to lateral lesions.
- −
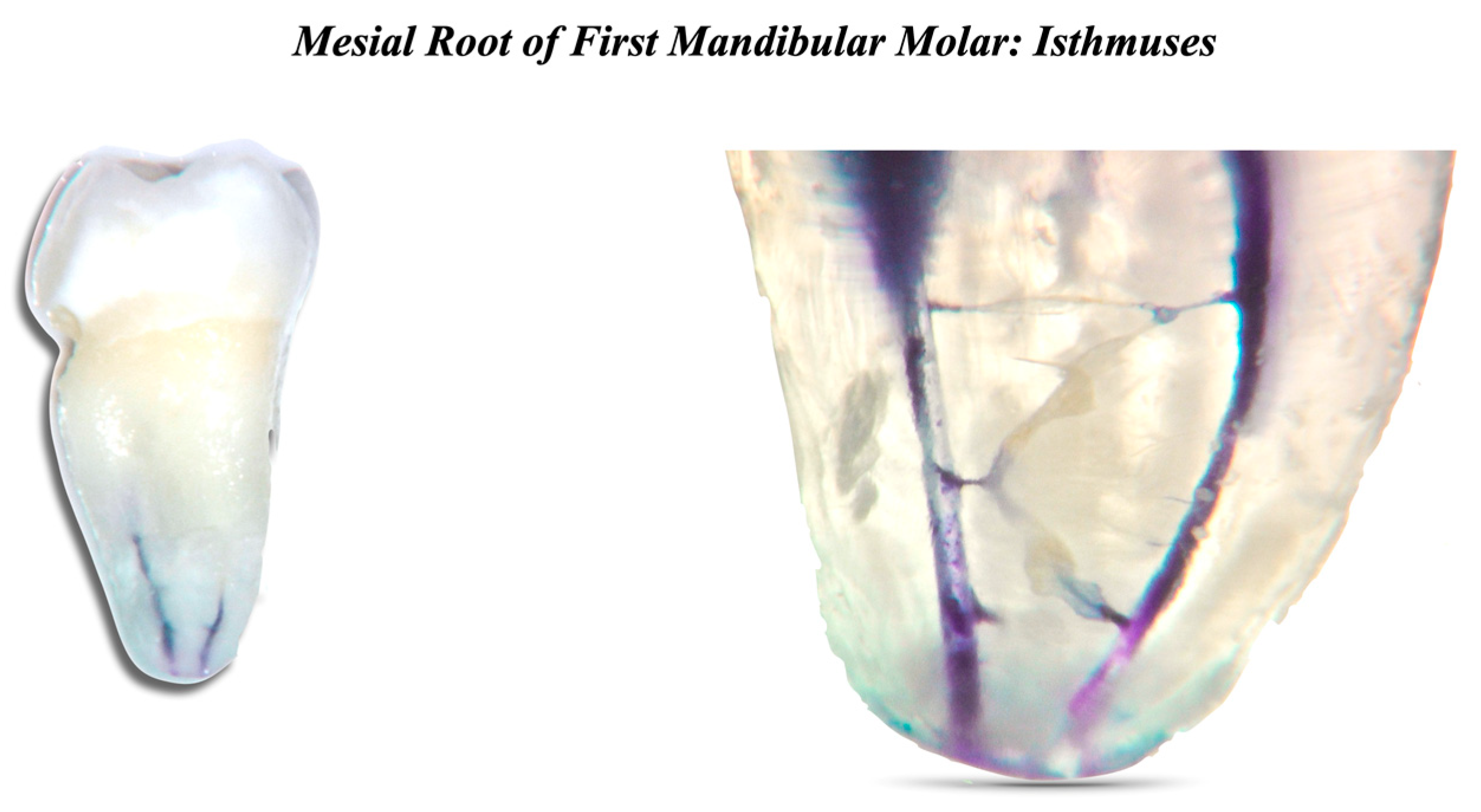
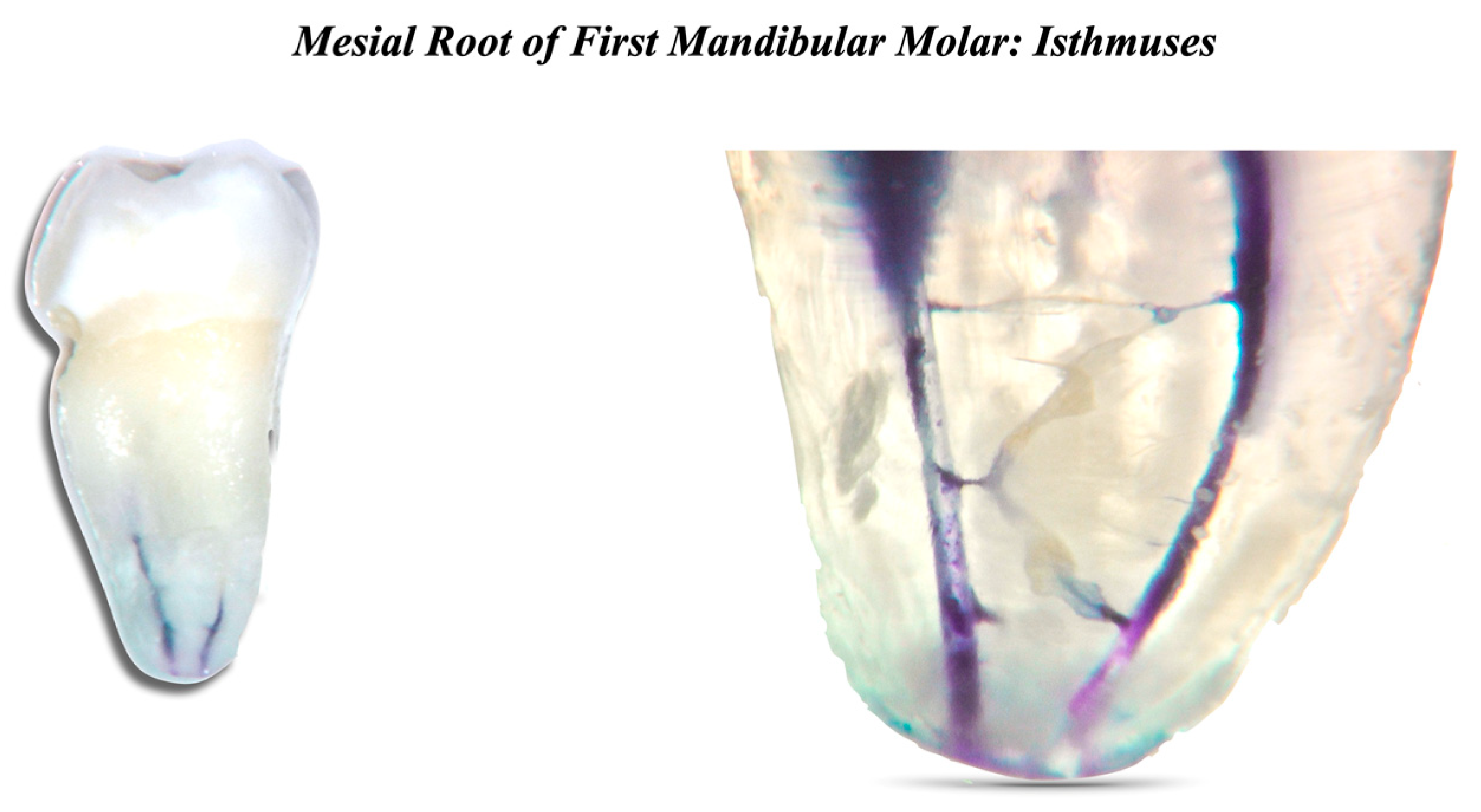
- Isthmuses: connections of small, medium, and large dimensions between two main canals. Isthmuses contain pulp tissue and may also retain bacteria in the case of necrotic teeth. Additionally, the incomplete removal of the infected tissues within these areas can jeopardize the treatment outcome after performing endodontic therapy [34].
- −
- Loop: a small area that leaves the main canal and then reconnects to it.
- −
- Ramifications: microscopic extensions from the main canal at any height.
- −
- Apical delta: bifurcation of the main canal at the apical level.
- −
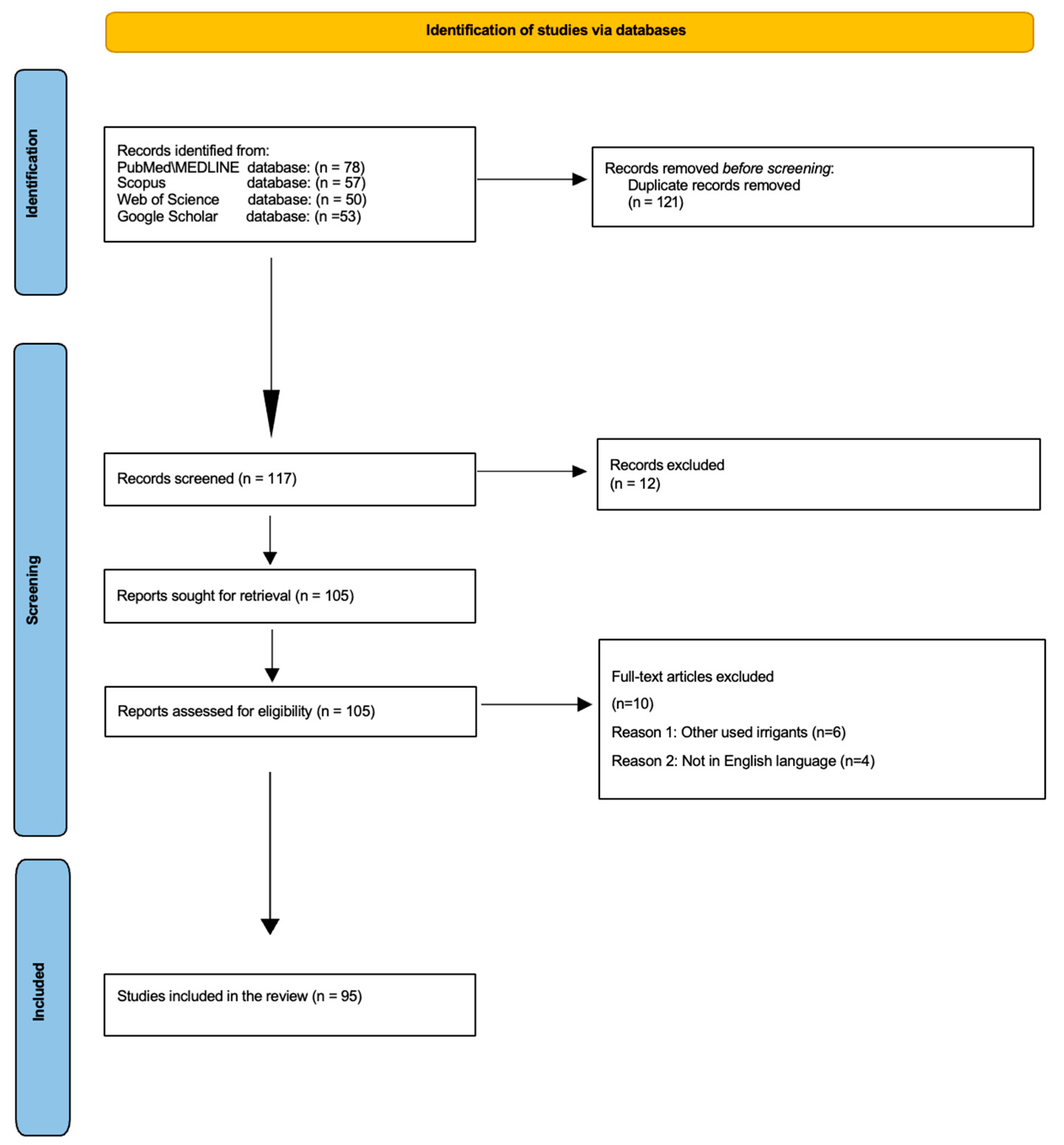
2. Materials and Methods
- −
- Studies published in the English language.
- −
- In vivo and in vitro studies.
- −
- Reviews and systematic reviews.
- −
- Studies that examine the effects of NaOCl, EDTA, and CHX.
- −
- Studies highlighting suitable clinical techniques to be adopted to activate the irrigants.
- −
- Studies that were not published in the English language.
- −
- Studies that used other irrigants.
3. Types of Irrigants and Irrigant Activation Methods
3.1. Sodium Hypochlorite
3.2. Chlorhexidine (CHX)
3.3. EDTA (Ethylene-Diamino-Tetra-Acetic Acid)
3.3.1. Smear Layer
3.3.2. EDTA
3.3.3. Chemical Properties of EDTA
3.4. Interactions
3.5. Activation of Irrigants
4. Effectiveness of Activation Methods in Conservative Shaping
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wong, J.; Cheung, G.S.P.; Lee, A.H.C.; McGrath, C.; Neelakantan, P. PROMs following Root Canal Treatment and Surgical Endodontic Treatment. Int. Dent. J. 2023, 73, 28–41. [Google Scholar] [CrossRef]
- Baumgartner, J.C.; Cuenin, P.R. Efficacy of Several Concentrations of Sodium Hypochlorite for Root Canal Irrigation. J. Endod. 1992, 18, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Iandolo, A.; Pisano, M.; Scelza, G.; Abdellatif, D.; Martina, S. Three-Dimensional Evaluation of the Root Apex of Permanent Maxillary Premolars: A Multicentric Study. Appl. Sci. 2022, 12, 6159. [Google Scholar] [CrossRef]
- Kumar, N.; Maher, N.; Amin, F.; Ghabbani, H.; Zafar, M.S.; Rodríguez-Lozano, F.J.; Oñate-Sánchez, R.E. Biomimetic Approaches in Clinical Endodontics. Biomimetics 2022, 7, 229. [Google Scholar] [CrossRef]
- Ali, A.; Bhosale, A.; Pawar, S.; Kakti, A.; Bichpuriya, A.; Agwan, M.A. Current Trends in Root Canal Irrigation. Cureus 2022, 14, e24833. [Google Scholar] [CrossRef]
- Vivekananda Pai, A.R. Factors Influencing the Occurrence and Progress of Sodium Hypochlorite Accident: A Narrative and Update Review. J. Conserv. Dent. 2023, 26, 3–11. [Google Scholar] [CrossRef]
- Peters, O.A.; Boessler, C.; Zehnder, M. Effect of Liquid and Paste-Type Lubricants on Torque Values during Simulated Rotary Root Canal Instrumentation. Int. Endod. J. 2005, 38, 223–229. [Google Scholar] [CrossRef]
- Wong, S.; Mundy, L.; Chandler, N.; Upritchard, J.; Purton, D.; Tompkins, G. Antibacterial Properties of Root Canal Lubricants: A Comparison with Commonly Used Irrigants. Aust. Endod. J. 2014, 40, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Hou, B.X.; Wesselink, P.R.; Wu, M.-K.; Shemesh, H. The incidence of root microcracks caused by 3 different single-file systems versus the ProTaper system. J. Endod. 2013, 39, 1054–1056. [Google Scholar] [CrossRef]
- Park, E.; Shen, Y.A.; Haapasalo, M. Irrigation of the apical root canal. Endod. Top. 2012, 27, 54–73. [Google Scholar] [CrossRef]
- Boessler, C.; Peters, O.A.; Zehnder, M. Impact of Lubricant Parameters on Rotary Instrument Torque and Force. J. Endod. 2007, 33, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Jahromi, M.Z.; Fathi, M.H.; Zamiran, S. Experimental Study of Smear Layer and Debris Remaining following the Use of Four Root Canal Preparation Systems Using Scanning Electron Microscopy. J. Islam. Dent. Assoc. Iran 2013, 25, 235–241. [Google Scholar]
- Jena, A.; Sahoo, S.K.; Govind, S. Root Canal Irrigants: A Review of Their Interactions, Benefits, and Limitations. Compend. Contin. Educ. Dent. 2015, 36, 256–261. [Google Scholar]
- Pisano, M.; Di Spirito, F.; Martina, S.; Sangiovanni, G.; D’Ambrosio, F.; Iandolo, A. Intentional Replantation of Single-Rooted and Multi-Rooted Teeth: A Systematic Review. Healthcare 2022, 11, 11. [Google Scholar] [CrossRef]
- Narayanan, L.L.; Vaishnavi, C. Endodontic microbiology. J. Conserv. Dent. 2010, 13, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr. Microbiology of apical periodontitis. In Essential Endodontology; Pitt Ford, T., Ed.; Blackwell: Oxford, UK, 2008; pp. 135–139. [Google Scholar]
- Olivieri, J.G.; García Font, M.; Stöber, E.; de Ribot, J.; Mercadé, M.; Duran-Sindreu, F. Effect of Manual Dynamic Activation with Citric Acid Solutions in Smear Layer Removal: A Scanning Electron Microscopic Evaluation. J. Dent. Sci. 2016, 11, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.E.; Cardon, J.W.; Drake, D.R. Antimicrobial Susceptibility of Monoculture Biofilms of a Clinical Isolate of Enterococcus Faecalis. J. Endod. 2009, 35, 95–97. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rôças, I.N. Present status and future directions: Microbiology of endodontic infections. Int. Endod. J. 2022, 55, 512–530. [Google Scholar] [CrossRef]
- Haupt, F.; Meinel, M.; Gunawardana, A.; Hülsmann, M. Effectiveness of Different Activated Irrigation Techniques on Debris and Smear Layer Removal from Curved Root Canals: A SEM Evaluation. Aust. Endod. J. 2020, 46, 40–46. [Google Scholar] [CrossRef]
- Ruksakiet, K.; Hanák, L.; Farkas, N.; Hegyi, P.; Sadaeng, W.; Czumbel, L.M.; Sang-ngoen, T.; Garami, A.; Mikó, A.; Varga, G.; et al. Antimicrobial Efficacy of Chlorhexidine and Sodium Hypochlorite in Root Canal Disinfection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Endod. 2020, 46, 1032–1041.e7. [Google Scholar] [CrossRef]
- Zamany, A.; Safavi, K.; Spångberg, L.S.W. The Effect of Chlorhexidine as an Endodontic Disinfectant. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 578–581. [Google Scholar] [CrossRef] [PubMed]
- Iandolo, A.; Amato, A.; Martina, S.; Abdellatif, D.A.; Pantaleo, G. Management of severe curvatures in root canal treatment with the new generation of rotating files using a safe and predictable protocol. Open Dent J. 2020, 14, 421–425. [Google Scholar] [CrossRef]
- Iandolo, A.; Simeone, M.; Riccitiello, F. The preparation of coronal isthmus is a fundamental step for long term success. G. Ital. Endod. 2012, 26, 150–154. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Arias-Moliz, M.T. Present Status and Future Directions—Irrigants and Irrigation Methods. Int. Endod. J. 2022, 55 (Suppl. S3), 588–612. [Google Scholar] [CrossRef]
- Rito Pereira, M.; Silva, G.; Semiao, V.; Silverio, V.; Martins, J.N.R.; Pascoal-Faria, P.; Alves, N.; Dias, J.R.; Ginjeira, A. Experimental Validation of a Computational Fluid Dynamics Model Using Micro-Particle Image Velocimetry of the Irrigation Flow in Confluent Canals. Int. Endod. J. 2022, 55, 1394–1403. [Google Scholar] [CrossRef]
- Pladisai, P.; Ampornaramveth, R.S.; Chivatxaranukul, P. Effectiveness of Different Disinfection Protocols on the Reduction of Bacteria in Enterococcus Faecalis Biofilm in Teeth with Large Root Canals. J. Endod. 2016, 42, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Stojicic, S.; Zivkovic, S.; Qian, W.; Zhang, H.; Haapasalo, M. Tissue Dissolution by Sodium Hypochlorite: Effect of Concentration, Temperature, Agitation, and Surfactant. J. Endod. 2010, 36, 1558–1562. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Lambrianidis, T.; Kastrinakis, E. Irrigant Flow within a Prepared Root Canal Using Various Flow Rates: A Computational Fluid Dynamics Study. Int. Endod. J. 2009, 42, 144–155. [Google Scholar] [CrossRef]
- Abou-Rass, M.; Piccinino, M.V. The Effectiveness of Four Clinical Irrigation Methods on the Removal of Root Canal Debris. Oral Surg. Oral Med. Oral Pathol. 1982, 54, 323–328. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Lambrianidis, T.; Kastrinakis, E.; Bekiaroglou, P. Measurement of Pressure and Flow Rates during Irrigation of a Root Canal Ex Vivo with Three Endodontic Needles. Int. Endod. J. 2007, 40, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.V.; Guedes, D.F.C.; Pécora, J.D.; da Cruz-Filho, A.M. Time-Dependent Effects of Chitosan on Dentin Structures. Braz. Dent. J. 2012, 23, 357–361. [Google Scholar] [CrossRef]
- Nair, P.N. On the causes of persistent apical periodontitis, a review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef]
- Yamada, R.S.; Armas, A.; Goldman, M.; Lin, P.S. A Scanning Electron Microscopic Comparison of a High Volume Final Flush with Several Irrigating Solutions: Part 3. J. Endod. 1983, 9, 137–142. [Google Scholar] [CrossRef]
- Kakehashi, S.; Stanley, H.R.; Fitzgerald, R.J. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg. Oral Med. Oral Pathol. 1965, 20, 340–349. [Google Scholar] [CrossRef]
- Berber, V.B.; Gomes, B.P.F.A.; Sena, N.T.; Vianna, M.E.; Ferraz, C.C.R.; Zaia, A.A.; Souza-Filho, F.J. Efficacy of Various Concentrations of NaOCl and Instrumentation Techniques in Reducing Enterococcus Faecalis within Root Canals and Dentinal Tubules. Int. Endod. J. 2006, 39, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F.; Rôças, I.N.; Favieri, A.; Lima, K.C. Chemomechanical Reduction of the Bacterial Population in the Root Canal after Instrumentation and Irrigation with 1%, 2.5%, and 5.25% Sodium Hypochlorite. J. Endod. 2000, 26, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Yesilsoy, C.; Whitaker, E.; Cleveland, D.; Phillips, E.; Trope, M. Antimicrobial and Toxic Effects of Established and Potential Root Canal Irrigants. J. Endod. 1995, 21, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Önçaǧ, Ö.; Hoşgör, M.; Hilmioǧlu, S.; Zekioǧlu, O.; Eronat, C.; Burhanoǧlu, D. Comparison of Antibacterial and Toxic Effects of Various Root Canal Irrigants. Int. Endod. J. 2003, 36, 423–432. [Google Scholar] [CrossRef]
- Parente, J.M.; Loushine, R.J.; Susin, L.; Gu, L.; Looney, S.W.; Weller, R.N.; Pashley, D.H.; Tay, F.R. Root Canal Debridement Using Manual Dynamic Agitation or the EndoVac for Final Irrigation in a Closed System and an Open System. Int. Endod. J. 2010, 43, 1001–1012. [Google Scholar] [CrossRef] [PubMed]
- Pitt Ford, T.R.; Riccucci, D.; Saunders, E.M.; Stabholz, A.; Suter, B. Quality Guidelines for Endodontic Treatment: Consensus Report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar]
- Haapasalo, M.; Shen, Y.; Wang, Z.; Gao, Y. Irrigation in endodontics. Br. Dent. J. 2014, 216, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, R.M.; Moule, A.J. Sodium hypochlorite and its use as an endodontic irrigant. Aust. Dent. J. 1998, 43, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Orlowski, N.B.; Schimdt, T.F.; Teixeira, C.D.S.; Garcia, L.D.F.R.; Savaris, J.M.; Tay, F.R.; Bortoluzzi, E.A. Smear Layer Removal Using Passive Ultrasonic Irrigation and Different Concentrations of Sodium Hypochlorite. J. Endod. 2020, 46, 1738–1744. [Google Scholar] [CrossRef]
- Zehnder, M. Root canal irrigants. J. Endod. 2006, 32, 389–398. [Google Scholar] [CrossRef]
- Cunningham, W.T.; Balekjian, A.Y. Effect of temperature on collagen-dissolving ability of sodium hypochlorite endodontic irrigant. Oral Surg. Oral Med. Oral Pathol. 1980, 49, 175–177. [Google Scholar] [CrossRef]
- Plotino, G.; Cortese, T.; Grande, N.M.; Leonardi, D.P.; Di Giorgio, G.; Testarelli, L.; Gambarini, G. New Technologies to Improve Root Canal Disinfection. Braz. Dent. J. 2016, 27, 3–8. [Google Scholar] [CrossRef]
- Gomes, B.P.; Vianna, M.E.; Zaia, A.A.; Almeida, J.F.; Souza-Filho, F.J.; Ferraz, C.C. Chlorhexidine in endodontics. Braz. Dent. J. 2013, 24, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Basrani, B.; Santos, J.M.; Tjäderhane, L.; Grad, H.; Gorduysus, O.; Huang, J.; Lawrence, H.P.; Friedman, S. Substantive antimicrobial activity in chlorhexidine-treated human root dentin. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, A.; Teixeira, C.S. The properties of chlorhexidine and undesired effects of its use in endodontics. Quintessence Int. 2015, 46, 575–582. [Google Scholar]
- Caron, G.; Nham, K.; Bronnec, F.; MacHtou, P. Effectiveness of Different Final Irrigant Activation Protocols on Smear Layer Removal in Curved Canals. J. Endod. 2010, 36, 1361–1366. [Google Scholar] [CrossRef]
- Iandolo, A.; Pisano, M.; Abdellatif, D.; Amato, A.; Giordano, F.; Buonavoglia, A.; Sangiovanni, G.; Caggiano, M. Effectiveness of Different Irrigation Techniques on Post Space Smear Layer Removal: SEM Evaluation. Prosthesis 2023, 5, 539–549. [Google Scholar] [CrossRef]
- Torabinejad, M.; Handysides, R.; Khademi, A.A.; Bakland, L.K. Clinical implications of the smear layer in endodontics: A review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 658–666. [Google Scholar] [CrossRef]
- Jaiswal, S.; Gupta, S.; Nikhil, V.; Bhadoria, A.; Raj, S. Effect of Intracanal and Extracanal Heating on Pulp Dissolution Property of Continuous Chelation Irrigant. J. Conserv. Dent. 2021, 24, 544–548. [Google Scholar]
- Teixeira, C.S.; Felippe, M.C.S.; Felippe, W.T. The Effect of Application Time of EDTA and NaOCI on Intracanal Smear Layer Removal: An SEM Analysis. Int. Endod. J. 2005, 38, 285–290. [Google Scholar] [CrossRef]
- Taweewattanapaisan, P.; Jantarat, J.; Ounjai, P.; Janebodin, K. The Effects of EDTA on Blood Clot in Regenerative Endodontic Procedures. J. Endod. 2019, 45, 281–286. [Google Scholar] [CrossRef]
- Wright, P.P.; Kahler, B.; Walsh, L.J. The Effect of Heating to Intracanal Temperature on the Stability of Sodium Hypochlorite Admixed with Etidronate or EDTA for Continuous Chelation. J. Endod. 2019, 45, 57–61. [Google Scholar] [CrossRef]
- Violich, D.R.; Chandler, N.P. The smear layer in endodontics—A review. Int. Endod. J. 2010, 43, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, U.; Saji, S.; Clarkson, R.; Lalloo, R.; Moule, A.J. Free active chlorine in sodium hypochlorite solutions admixed with octenidine, smearoff, chlorhexidine, and EDTA. J. Endod. 2017, 43, 1354–1359. [Google Scholar] [CrossRef] [PubMed]
- Haapasalo, M.; Shen, Y.; Qian, W.; Gao, Y. Irrigation in endodontics. Dent. Clin. N. Am. 2010, 54, 291–312. [Google Scholar] [CrossRef] [PubMed]
- Wright, P.P.; Kahler, B.; Walsh, L.J. Alkaline Sodium Hypochlorite Irrigant and Its Chemical Interactions. Materials 2017, 10, 1147. [Google Scholar] [CrossRef]
- Paixão, S.; Rodrigues, C.; Grenho, L.; Fernandes, M.H. Efficacy of sonic and ultrasonic activation during endodontic treatment: A Meta-analysis of in vitro studies. Acta Odontol. Scand. 2022, 80, 588–595. [Google Scholar] [CrossRef]
- Macedo, R.G.; Verhaagen, B.; Rivas, D.F.; Versluis, M.; Wesselink, P.; Van Der Sluis, L. Cavitation Measurement during Sonic and Ultrasonic Activated Irrigation. J. Endod. 2014, 40, 580–583. [Google Scholar] [CrossRef]
- Mortman, R.E. Technologic advances in endodontics. Dent. Clin. N. Am. 2011, 55, 461–480. [Google Scholar] [CrossRef]
- Sirtes, G.; Waltimo, T.; Schaetzle, M.; Zehnder, M. The Effects of Temperature on Sodium Hypochlorite Short-Term Stability, Pulp Dissolution Capacity, and Antimicrobial Efficacy. J. Endod. 2005, 31, 669–671. [Google Scholar] [CrossRef] [PubMed]
- Bukiet, F.; Soler, T.; Guivarch, M.; Camps, J.; Tassery, H.; Cuisinier, F.; Candoni, N. Factors affecting the viscosity of sodium hypochlorite and their effect on irrigant flow. Int. Endod. J. 2013, 46, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Yared, G.; Al Asmar Ramli, G. Antibacterial Ability of Sodium Hypochlorite Heated in the Canals of Infected Teeth: An Ex Vivo Study. Cureus 2020, 12, e6975. [Google Scholar] [CrossRef]
- Iandolo, A.; Simeone, M.; Orefice, S.; Rengo, S. 3D cleaning, a perfected technique: Thermal profile assessment of heated NaOCl. G. Ital. Endod. 2017, 31, 58–61. [Google Scholar] [CrossRef]
- Jain, S.; Patni, P.M.; Jain, P.; Raghuwanshi, S.; Pandey, S.H.; Tripathi, S.; Soni, A. Comparison of Dentinal Tubular Penetration of Intracanal Heated and Preheated Sodium Hypochlorite Through Different Agitation Techniques. J. Endod. 2023, 49, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Damade, Y.; Kabir, R.; Gaddalay, S.; Deshpande, S.; Gite, S.; Bambale, S.; Dubey, N. Root canal debridement efficacy of heated sodium hypochlorite in conjunction with passive ultrasonic agitation: An ex vivo study. J. Dent. Res. Dent. Clin. Dent. Prospect. 2020, 14, 235–238. [Google Scholar] [CrossRef]
- Korkut, E.; Torlak, E.; Gezgin, O.; Özer, H.; Sener, Y. Antibacterial and Smear Layer Removal Efficacy of Er:YAG Laser Irradiation by Photon-Induced Photoacoustic Streaming in Primary Molar Root Canals: A Preliminary Study. Photomed. Laser Surg. 2018, 36, 480–486. [Google Scholar] [CrossRef]
- Koch, J.D.; Jaramillo, D.E.; DiVito, E.; Peters, O.A. Irrigant Flow during Photon-Induced Photoacoustic Streaming (PIPS) Using Particle Image Velocimetry (PIV). Clin. Oral Investig. 2016, 20, 381–386. [Google Scholar] [CrossRef]
- Loroño, G.; Zaldivar, J.R.; Arias, A.; Cisneros, R.; Dorado, S.; Jimenez-Octavio, J.R. Positive and negative pressure irrigation in oval root canals with apical ramifications: A computational fluid dynamics evaluation in micro-CT scanned real teeth. Int. Endod. J. 2020, 53, 671–679. [Google Scholar] [CrossRef]
- Konstantinidi, E.; Psimma, Z.; Chávez de Paz, L.E.; Boutsioukis, C. Apical negative pressure irrigation versus syringe irrigation: A systematic review of cleaning and disinfection of the root canal system. Int. Endod. J. 2017, 50, 1034–1054. [Google Scholar] [CrossRef]
- Hemalatha, S.; Srinivasan, A.; Srirekha, A.; Santhosh, L.; Champa, C.; Shetty, A. An in vitro radiological evaluation of irrigant penetration in the root canals using three different irrigation systems: Waterpik WP-100 device, passive irrigation, and manual dynamic irrigation systems. J. Conserv. Dent. 2022, 25, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Susila, A.; Minu, J. Activated Irrigation vs. Conventional non-activated Irrigation in Endodontics—A Systematic Review. Eur. Endod. J. 2019, 4, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Pisano, M.; Caggiano, M.; Bhasin, P.; Lo Giudice, R.; Abdellatif, D. Root Canal Cleaning after Different Irrigation Techniques: An Ex Vivo Analysis. Medicina 2022, 58, 193. [Google Scholar] [CrossRef] [PubMed]
- Martina, S.; Pisano, M.; Amato, A.; Abdellatif, D.; Iandolo, A. Modern rotary files in minimally invasive endodontics: A case report. Front. Biosci. 2021, 13, 299–304. [Google Scholar] [CrossRef]
- Iandolo, A.; Abdellatif, D.; Pantaleo, G.; Sammartino, P.; Amato, A. Conservative shaping combined with three-dimensional cleaning can be a powerful tool: Case series. J. Conserv. Dent. 2020, 23, 648–652. [Google Scholar] [CrossRef]
- Mozo, S.; Llena, C.; Forner, L. Review of Ultrasonic Irrigation in Endodontics: Increasing Action of Irrigating Solutions. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e512–e516. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Jayaraman, J.; Suresh, A.; Kalyanasundaram, S.; Neelakantan, P. Effectiveness of Ultrasonically Activated Irrigation on Root Canal Disinfection: A Systematic Review of in Vitro Studies. Clin. Oral Investig. 2018, 22, 655–670. [Google Scholar] [CrossRef]
- Iandolo, A.; Pisano, M.; Abdellatif, D.; Sangiovanni, G.; Pantaleo, G.; Martina, S.; Amato, A. Smear Layer and Debris Removal from Root Canals Comparing Traditional Syringe Irrigation and 3D Cleaning: An Ex Vivo Study. J. Clin. Med. 2023, 12, 492. [Google Scholar] [CrossRef] [PubMed]
- Zamparini, F.; Spinelli, A.; Chersoni, S.; Buonavoglia, A.; Gandolfi, M.G.; Prati, C. Root canal retreatment of the compromised tooth or extraction and implant rehabilitation? Dent. Cadmos 2021, 89, 2–21. [Google Scholar] [CrossRef]
- Iandolo, A.; Amato, M.; Abdellatif, D.; Barbosa, A.F.A.; Pantaleo, G.; Blasi, A.; Franco, V.; Silva, E.J.N.L. Effect of different final irrigation protocols on pulp tissue dissolution from an isthmus model. Aust. Endod. J. 2021, 47, 538–543. [Google Scholar] [CrossRef]
- Troiano, G.; Perrone, D.; Dioguardi, M.; Buonavoglia, A.; Ardito, F.; Lo Muzio, L. In vitro evaluation of the cytotoxic activity of three epoxy resin-based endodontic sealers. Dent. Mater. J. 2018, 37, 374–378. [Google Scholar] [CrossRef]
- Chandler, N.; Chellappa, D. Lubrication during root canal treatment. Aust. Endod. J. 2019, 45, 106–110. [Google Scholar] [CrossRef]
- Lee, O.Y.S.; Khan, K.; Li, K.Y.; Shetty, H.; Abiad, R.S.; Cheung, G.S.P.; Neelakantan, P. Influence of apical preparation size and irrigation technique on root canal debridement: A histological analysis of round and oval root canals. Int. Endod. J. 2019, 52, 1366–1376. [Google Scholar] [CrossRef]
- Mohammadzadeh Akhlaghi, N.; Rahimifard, N.; Moshari, A.; Vatanpour, M.; Darmiani, S. The Effect of Size and Taper of Apical Preparation in Reducing Intra-Canal Bacteria: A Quantitative SEM Study. Iran Endod. J. 2014, 9, 61–65. [Google Scholar]
- Yared, G.; Ramli, G.A. Ex vivo ability of a noninstrumentation technique to disinfect oval-shaped canals. J. Conserv. Dent. 2020, 23, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Abdellatif, D.; Amato, A.; Calapaj, M.; Pisano, M.; Iandolo, A. A novel modified obturation technique using biosealers: An ex vivo study. J. Conserv. Dent. 2021, 24, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Desai, P.; Himel, V. Comparative Safety of Various Intracanal Irrigation Systems. J. Endod. 2009, 35, 545–549. [Google Scholar] [CrossRef]
- Tay, F.R.; Gu, L.S.; Schoeffel, G.J.; Wimmer, C.; Susin, L.; Zhang, K.; Arun, S.N.; Kim, J.; Looney, S.W.; Pashley, D.H. Effect of vapor lock on root canal debridement by using a side-vented needle for positive-pressure irrigant delivery. J. Endod. 2010, 36, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; Pantaleo, G.; Abdellatif, D.; Blasi, A.; Lo Giudice, R.; Iandolo, A. Evaluation of cyclic fatigue resistance of modern Nickel–Titanium rotary instruments with continuous rotation. G. Ital. Endod. 2017, 31, 78–82. [Google Scholar]
- Buonavoglia, A.; Zamparini, F.; Lanave, G.; Pellegrini, F.; Diakoudi, G.; Spinelli, A.; Lucente, M.S.; Camero, M.; Vasinioti, V.I.; Gandolfi, M.G.; et al. Endodontic Microbial Communities in Apical Periodontitis. J. Endod. 2023, 49, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Urban, K.; Donnermeyer, D.; Schäfer, E.; Bürklein, S. Canal Cleanliness Using Different Irrigation Activation Systems: A SEM Evaluation. Clin. Oral Investig. 2017, 21, 2681–2687. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Endodontic Treatment Phases |
|---|
|
|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iandolo, A.; Pisano, M.; Buonavoglia, A.; Giordano, F.; Amato, A.; Abdellatif, D. RETRACTED: Traditional and Recent Root Canal Irrigation Methods and Their Effectiveness: A Review. Clin. Pract. 2023, 13, 1059-1072. https://doi.org/10.3390/clinpract13050094
Iandolo A, Pisano M, Buonavoglia A, Giordano F, Amato A, Abdellatif D. RETRACTED: Traditional and Recent Root Canal Irrigation Methods and Their Effectiveness: A Review. Clinics and Practice. 2023; 13(5):1059-1072. https://doi.org/10.3390/clinpract13050094
Chicago/Turabian StyleIandolo, Alfredo, Massimo Pisano, Alessio Buonavoglia, Francesco Giordano, Alessandra Amato, and Dina Abdellatif. 2023. "RETRACTED: Traditional and Recent Root Canal Irrigation Methods and Their Effectiveness: A Review" Clinics and Practice 13, no. 5: 1059-1072. https://doi.org/10.3390/clinpract13050094
APA StyleIandolo, A., Pisano, M., Buonavoglia, A., Giordano, F., Amato, A., & Abdellatif, D. (2023). RETRACTED: Traditional and Recent Root Canal Irrigation Methods and Their Effectiveness: A Review. Clinics and Practice, 13(5), 1059-1072. https://doi.org/10.3390/clinpract13050094