
Metformin Sustained-Release and Vildagliptin Fixed-Dose Combination for Optimizing Glycemic Control: A Review with Real-World Case Reports


Abstract
1. Background
1.1. Burden of Diabetes and Its Complications
1.2. Current Unmet Needs in the Management of Glycemic Control
2. Metformin SR–Vildagliptin FDC Therapy: Evidence-Based Rationale
2.1. Metformin IR–Vildagliptin FDC Therapy
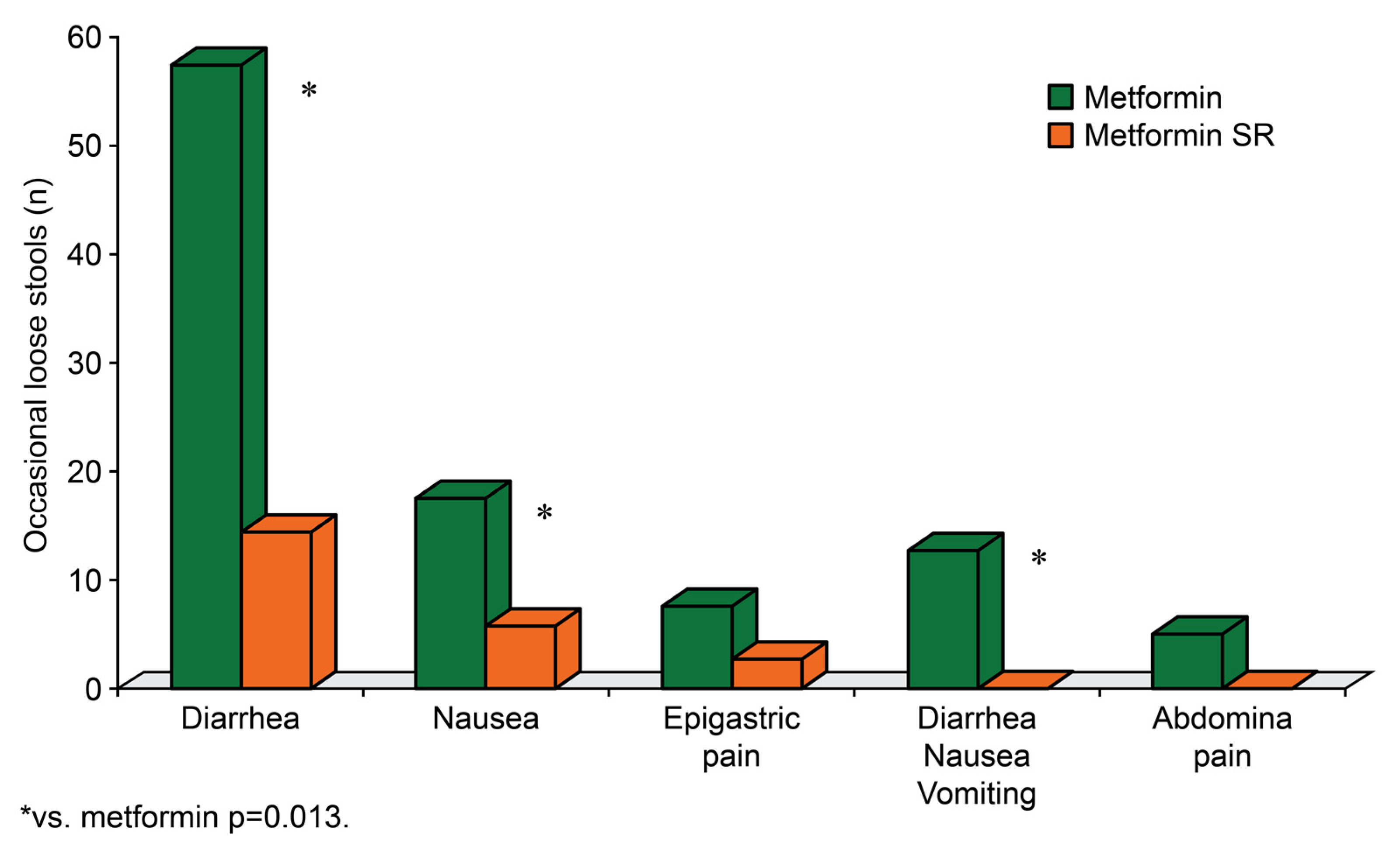
2.2. Role of Metformin SR Therapy in Improved Treatment Satisfaction
3. Clinical and Real-World Benefits of the Metformin SR–Vildagliptin FDC
3.1. Efficacy, Safety, and Therapy Compliance with the FDC of Metformin and Vildagliptin: Clinical Evidence
3.2. Sustained-Release vs. Immediate-Release Metformin and Vildagliptin Combination
4. Real-World Effectiveness of Metformin SR–Vildagliptin FDC: Case Presentation
4.1. Objective
4.2. Methods
4.3. Results
4.4. Discussion
Opinion on the Timing of Administration of Metformin SR–Vildagliptin Combination
- Use of metformin SR instead of IR formulation in the FDC may help promote adherence to OAD therapy, resulting in improved clinical outcomes and GI tolerability.
- Early combination therapy of metformin SR and vildagliptin in patients with T2DM is associated with significant and clinically relevant HbA1c reduction, good tolerability, good patient compliance and treatment satisfaction.
- The FDC of vildagliptin and metformin SR is effective with good GI tolerability.
- Current evidence indicates that administration of vildagliptin before meals may ensure optimal effect. Thus, the metformin SR–vildagliptin FDC may be prescribed before meals.
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation Diabetes Atlas 10th Edition 2021. Available online: https://diabetesatlas.org/idfawp/resource-files/2021/07/IDF_Atlas_10th_Edition_2021.pdf (accessed on 1 February 2023).
- Borgharkar, S.S.; Das, S.S. Real-world evidence of glycemic control among patients with type 2 diabetes mellitus in India: The TIGHT study. BMJ Open Diabetes Res. Care 2019, 7, e000654. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.; Das, A.K.; Priya, G.; Ghosh, S.; Mehrotra, R.N.; Das, S.; Shah, P.; Bajaj, S.; Deshmukh, V.; Sanyal, D.; et al. Fixed-dose combination in management of type 2 diabetes mellitus: Expert opinion from an international panel. J. Family Med. Prim. Care 2020, 9, 5450–5457. [Google Scholar] [CrossRef] [PubMed]
- Mohan, V.; Zargar, A.; Chawla, M.; Joshi, A.; Ayyagari, U.; Sethi, B.; Gaurav, K.; Patted, U.R.H.; Bhagat, S.V.; Mane, A.I. Efficacy of a combination of metformin and vildagliptin in comparison to metformin alone in type 2 diabetes mellitus: A multicentre, retrospective, real-world evidence study. Diabetes Metab. Syndr. Obes. 2021, 14, 2925–2933. [Google Scholar] [CrossRef] [PubMed]
- Cahn, A.; Cafelu, W.T. Clinical considerations for use of initial combination therapy in type 2 diabetes. Diabetes. Care 2016, 39, S137–S145. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 3, S98–S110. [Google Scholar] [CrossRef]
- Vyas, N.D.; Gor, A.P.; Suthar, J.V. Evaluation of prescribing pattern of fixed dose combinations of antihypertensives and antidiabetic agents. Asian J. Pharm. Clin. Res. 2017, 10, 164–168. [Google Scholar] [CrossRef]
- Vijayakumar, T.M.; Jayram, J.; Cheekireddy, M.V.; Himaja, D.; Teja, Y.D.; Narayanasamy, D. Safety, efficacy, and bioavailability of fixed-dose combinations in type 2 diabetes mellitus: A systematic updated review. Curr. Ther. Res. Clin. Exp. 2017, 84, 4–9. [Google Scholar] [CrossRef]
- Dovc, K.; Battelino, T. Time in range centered diabetes care. Clin. Pediatr. Endocrinol. 2021, 30, 1–10. [Google Scholar] [CrossRef]
- Eucreas Scientific Discussion. Available online: https://www.ema.europa.eu/en/documents/scientific-discussion/eucreas-epar-scientific-discussion_en.pdf. (accessed on 7 September 2021).
- Bosi, E.; Camisasca, R.P.; Collober, C.; Rochotte, E.; Garber, A.J. Effects of vildagliptin on glucose control over 24 weeks in patients with type 2 diabetes inadequately controlled with metformin. Diabetes Care 2007, 30, 890–895. [Google Scholar] [CrossRef]
- Halimi, S.; Schweizer, A.; Minic, B.; Foley, J.; Dejager, S. Combination treatment in the management of type 2 diabetes: Focus on vildagliptin and metformin as a single tablet. Vasc. Health Risk Manag. 2008, 4, 481–492. [Google Scholar]
- Derosa, G.; D’Angelo, A.; Romano, D.; Maffioli, P. Effects of metformin extended release compared to immediate release formula on glycemic control and glycemic variability in patients with type 2 diabetes. Drug Des. Dev. Ther. 2017, 11, 1481–1488. [Google Scholar] [CrossRef]
- Florez, H.; Luo, J.; Castillo-Florez, S.; Mitsi, G.; Hanna, J.; Tamariz, L.; Palacio, A.; Nagendran, S.; Hagan, M. Impact of metformin-induced gastrointestinal symptoms on quality of life and adherence in patients with type 2 diabetes. Postgrad. Med. 2010, 122, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Gohel, N.; Patel, D.M.; Patel, K.; Modi, J. Formulation development and evaluation of modified release tablet using a fixed dose combination of antidiabetic agents. Int. J. Pharm. Sci. Rev. Res. 2017, 42, 139–145. [Google Scholar]
- Bonnet, F.; Scheen, A. Understanding and overcoming metformin gastrointestinal intolerance. Diabetes Obes. Metab. 2017, 19, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Pladeval, M.; Williams, L.K.; Potts, L.A.; Divine, G.; Xi, H.; Lafata, J.E. Clinical outcomes and adherence to medications measured by claims data in patients with diabetes. Diabetes Care 2004, 27, 2800–2805. [Google Scholar] [CrossRef]
- McCreight, L.J.; Bailey, C.J.; Pearson, E.R. Metformin and the gastrointestinal tract. Diabetologia 2016, 59, 426–435. [Google Scholar] [CrossRef]
- Senjoti, F.G.; Mahmood, S.; Jaffri, J.M.; Mandal, U.K. Design and in-vitro evaluation of sustained release floating tablets of metformin HCl based on effervescence and swelling. Iran J. Pharm. Res. 2016, 15, 53–70. [Google Scholar] [PubMed]
- Kim, C.H.; Han, K.A.; Oh, H.J.; Tan, K.E.; Sothiratnam, R.; Tjokroprawiro, A.; Klein, M. Safety, tolerability, and efficacy of metformin extended-release oral antidiabetic therapy in patients with type 2 diabetes: An observational trial in Asia. J. Diabetes 2012, 4, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.; Cobas, R.A.; Gomes, M.B. Assessment of efficacy and tolerability of once-daily extended release metformin in patients with type 2 diabetes mellitus. Diabetol. Metab. Syndr. 2010, 2, 16. [Google Scholar] [CrossRef] [PubMed]
- Blonde, L.; Dailey, G.E.; Jabbour, S.A.; Reasner, C.A.; Mills, D.J. Gastrointestinal tolerability of extended-release metformin tablets compared to immediate-release metformin tablets: Results of a retrospective cohort study. Curr. Med. Res. Opin. 2004, 20, 565–572. [Google Scholar] [CrossRef]
- Hostalek, U.; Ametov, A.; Barykina, I.; Bondar, I.; Vaysberg, A.; Verbovaya, N.; Zhukova, L.; Zamyatina, O.; Kiseleva, T.; Morugova, T.; et al. Multicentre evaluation of adherence to extended-release metformin in daily practice in Russia. Int. J. Diabetes Clin. Res. 2017, 4, 78. [Google Scholar] [CrossRef]
- Matthews, D.R.; Paldánius, P.M.; Proot, P.; Chiang, Y.; Stumvoll, M.; Prato, S.D.; VERIFY study group. VERIFY study group. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): A 5-year, multicentre, randomised, double-blind trial. Lancet 2019, 394, 1519–1529. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.; Del Prato, S.; Mohan, V.; Mathieu, C.; Vencio, S.; Chan, J.C.N.; Stumvoll, M.; Paldánius, P.M. Insights from VERIFY: Early combination therapy provides better glycaemic durability than a stepwise approach in newly diagnosed type 2 diabetes. Diabetes Ther. 2020, 11, 2465–2476. [Google Scholar] [CrossRef]
- Chawla, M.; Kim, T.H.; Mirasol, R.C.; Faruque, P.; Cooke, K.; Hours-Zesiger, P.; Shete, A. Initial combination therapy with vildagliptin plus metformin in drug-naïve patients with T2DM: A 24-week real-life study from Asia. Curr. Med. Res. Opin. 2018, 34, 1605–1611. [Google Scholar] [CrossRef] [PubMed]
- Herman, G.A.; Bergman, A.; Stevens, C.; Kotey, P.; Yi, B.; Zhao, P.; Dietrich, B.; Golor, G.; Schrodter, A.; Keymeulen, B.; et al. Effect of single oral doses of sitagliptin, a dipeptidyl peptidase-4 inhibitor, on incretin and plasma glucose levels after an oral glucose tolerance test in patients with type 2 diabetes. J. Clan. Endocrinal. Metal. 2006, 91, 4612–4619. [Google Scholar] [CrossRef]
- Drucker, D.J.; Nauck, M.A. The incretin system: Glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet 2006, 368, 1696–1705. [Google Scholar] [CrossRef]
- Keating, G.M. Vildagliptin: A review of its use in type 2 diabetes mellitus. Drugs 2014, 74, 587–610. [Google Scholar] [CrossRef]
- Balas, B.; Baig, M.R.; Watson, C.; Dunning, B.E.; Ligueros-Saylan, M.; Wang, Y.; He, Y.-L.; Darland, C.; Holst, J.J.; Deacon, C.F.; et al. The dipeptidyl peptidase IV inhibitor vildagliptin suppresses endogenous glucose production and enhances islet function after single-dose administration in type 2 diabetic patients. J. Clin. Endocrinol. Metab. 2007, 92, 1249–1255. [Google Scholar] [CrossRef]
- Kikuchi, M.; Abe, N.; Kato, M.; Terao, S.; Mimori, N.; Tachibana, H. Vildagliptin dose-dependently improves glycaemic control in Japanese patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2009, 83, 233–240. [Google Scholar] [CrossRef]
- Ahren, B.; Schweizer, A.; Dejager, S.; Dunning, B.E.; Nilsson, P.M.; Persson, M.; Foley, J.E. Vildagliptin enhances islet responsiveness to both hyper- and hypoglycemia in patients with type 2 diabetes. J. Clin. Endocrinol. Metab. 2009, 94, 1236–1243. [Google Scholar] [CrossRef]
- Aoki, K.; Kamiyama, H.; Masuda, K.; Kamiko, K.; Noguchi, Y.; Tajima, K.; Terauchi, Y. Effects of miglitol, vildagliptin, or their combination on serum insulin and peptide YY levels and plasma glucose, cholecystokinin, ghrelin, and obestatin levels. Endocr. J. 2014, 61, 249–256. [Google Scholar] [CrossRef] [PubMed]
- He, Y.L.; Ito, H.; Yamaguchi, M.; Terao, S.; Shimada, S.; Irie, S.; Sekiguchi, K. Effects of meal timing relative to dosing on the pharmacokinetics and pharmacodynamics of vildagliptin in Japanese patients with Type 2 diabetes. Int. J. Clin. Pharmacol. Ther. 2012, 50, 237–247. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient No. | Baseline Data | Concomitant Antidiabetic Medication | % of TIR | ||||
|---|---|---|---|---|---|---|---|
| Age and Gender | Comorbidity | Duration of Diabetes | HbA1c | At Baseline | After Treatment | ||
| 1 | 49 years, male | Hypertension | 13 years and 8 months | 7.70% | Glimepiride | 70% | 78% |
| 2 | 82 years, female | Hypertension | NA | 12% | Insulin Humalog Mix 25, | 22% | 69% |
| SU (gliclazide) + metformin combination therapy | |||||||
| 3 | 55 years, female | Hypertension, dyslipidemia | 4 years and 11 months | 6.50% | Metformin monotherapy | 93% | 82% |
| 4 | 64 years, male | Hyperthyroidism | 25 years and 7 months | 6.80% | Combination of alpha-glucosidase inhibitor (voglibose) and metformin | 42% | 67% |
| 5 | 47 years, male | Hypertension | 4 years | 11.30% | Nil | 45% | 34% |
| 6 | 40 years, female | Hypertension, dyslipidemia | 5 years | 7.30% | Nil | 94% | 98% |
| 7 | 20 years, female | Hyperthyroidism | 1 year and 7 months | 10.20% | Insulin (mixtard 30/70, a biphasic insulin); | 61% | 65% |
| combination of SU (gliclazide) + metformin | |||||||
| 8 | 53 years, male | Hyperthyroidism | 5 years | 9.00% | SU (gliclazide) monotherapy | 70% | 80% |
| 9 | 52 years, female | Hyperthyroidism, dyslipidemia | 9 years and 11 months | 8.30% | Nil | 66% | 100% |
| 10 | 48 years, female | Dyslipidemia | 1 year and 8 months | 7.90% | Nil | 88% | 87% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chawla, M.; Chawla, P.; Jethwani, P.; Shah, K.; Reddy, S. Metformin Sustained-Release and Vildagliptin Fixed-Dose Combination for Optimizing Glycemic Control: A Review with Real-World Case Reports. Clin. Pract. 2023, 13, 497-504. https://doi.org/10.3390/clinpract13020045
Chawla M, Chawla P, Jethwani P, Shah K, Reddy S. Metformin Sustained-Release and Vildagliptin Fixed-Dose Combination for Optimizing Glycemic Control: A Review with Real-World Case Reports. Clinics and Practice. 2023; 13(2):497-504. https://doi.org/10.3390/clinpract13020045
Chicago/Turabian StyleChawla, Manoj, Purvi Chawla, Pratap Jethwani, Kiran Shah, and Sanjay Reddy. 2023. "Metformin Sustained-Release and Vildagliptin Fixed-Dose Combination for Optimizing Glycemic Control: A Review with Real-World Case Reports" Clinics and Practice 13, no. 2: 497-504. https://doi.org/10.3390/clinpract13020045
APA StyleChawla, M., Chawla, P., Jethwani, P., Shah, K., & Reddy, S. (2023). Metformin Sustained-Release and Vildagliptin Fixed-Dose Combination for Optimizing Glycemic Control: A Review with Real-World Case Reports. Clinics and Practice, 13(2), 497-504. https://doi.org/10.3390/clinpract13020045