
Effects of Mediterranean Diet, DASH Diet, and Plant-Based Diet on Outcomes among End Stage Kidney Disease Patients: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
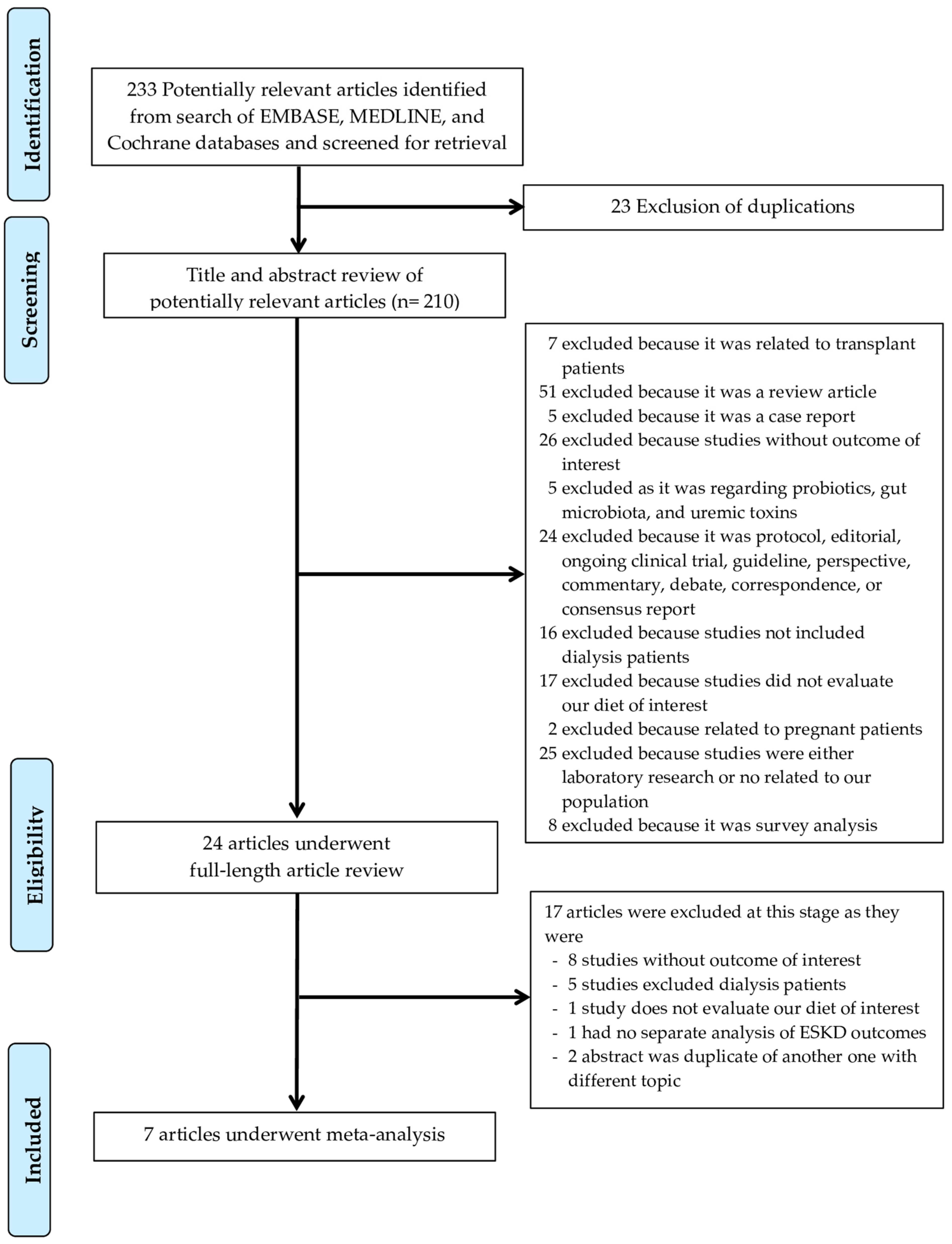
2.1. Information Sources and Search Strategy
2.2. Selection Criteria
2.3. Data Abstraction
2.4. Statistical Analysis
3. Results
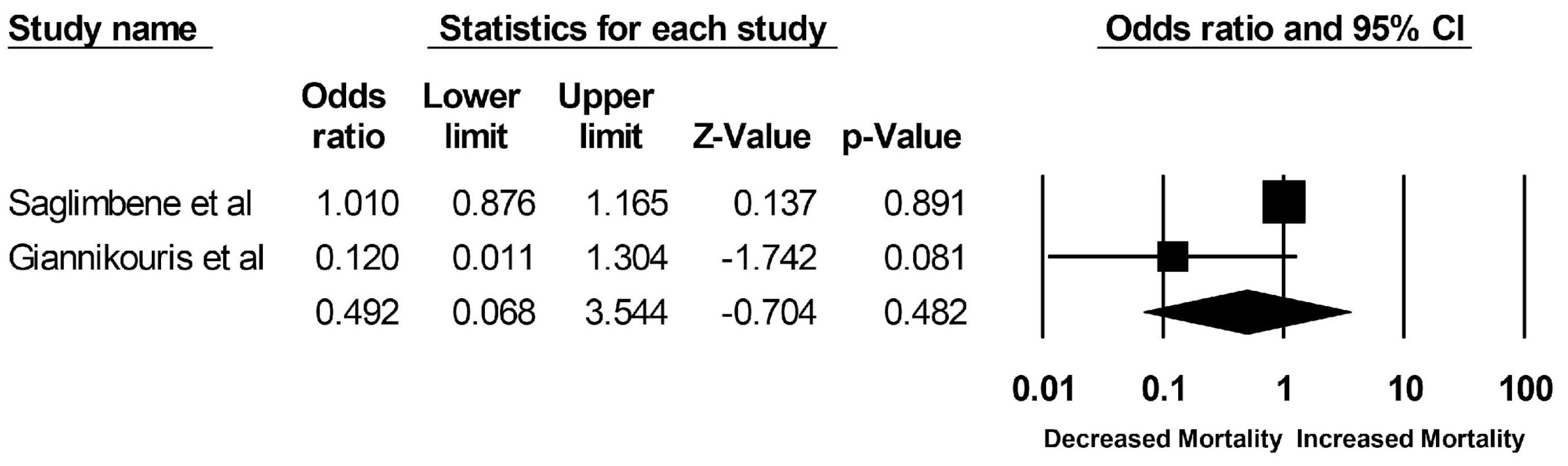
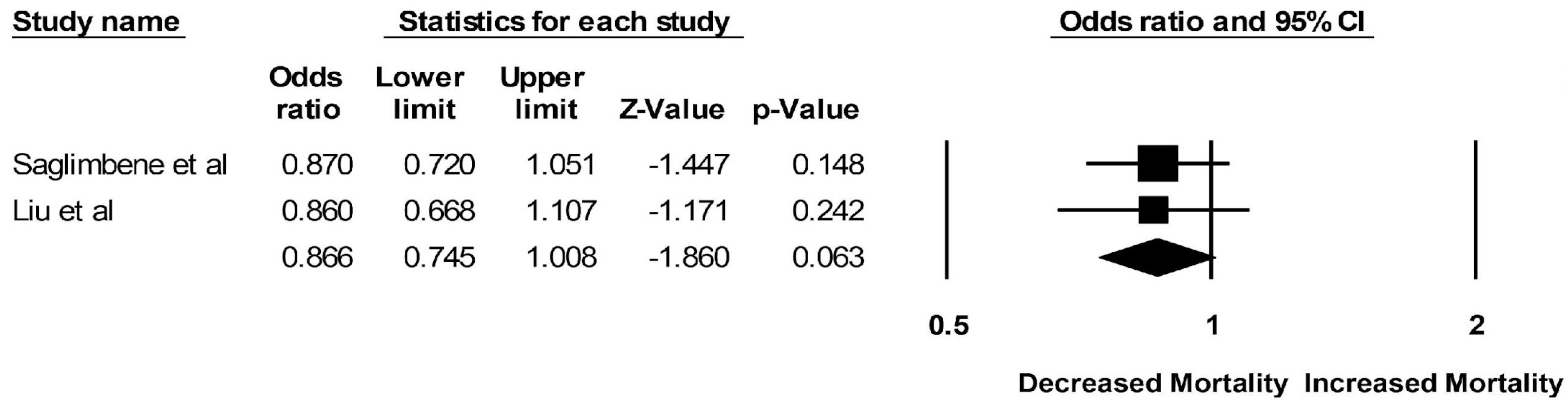
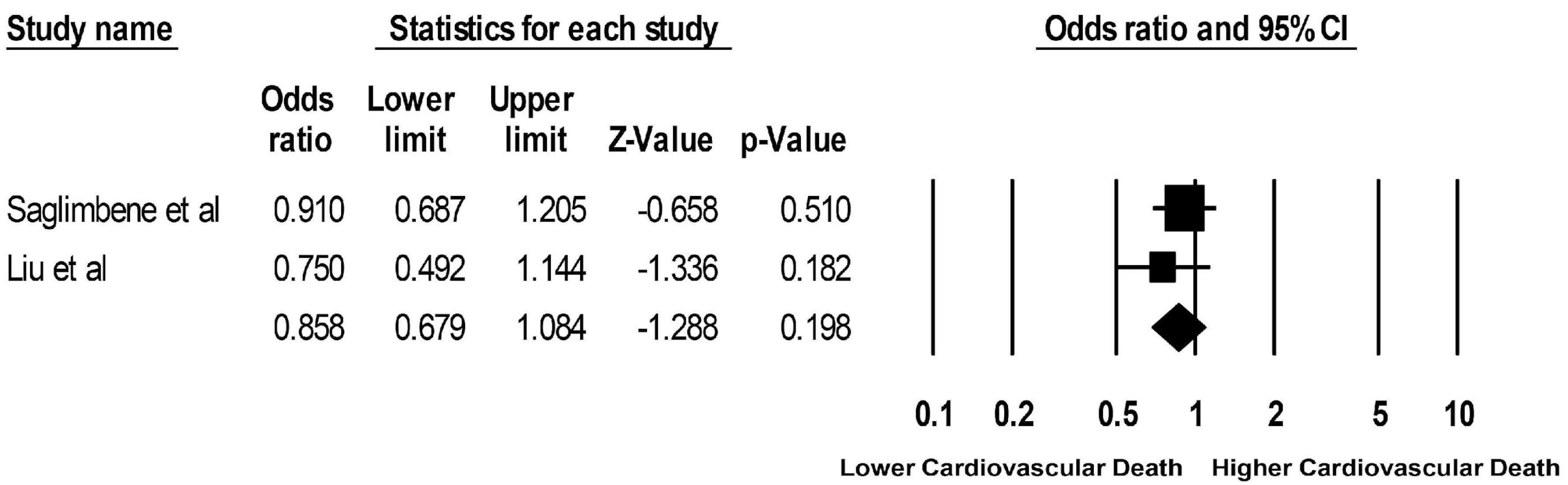
3.1. Incidence of All-Cause and Cardiovascular Mortality in ESKD Patients on DASH, Mediterranean, or Plant-Based Diet
3.2. Incidence of LVH and Hyperkalemia Related to DASH, Mediterranean, and Plant-Based Diet
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saran, R.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.; Bhave, N.; Bragg-Gresham, J.; Balkrishnan, R.; Dietrich, X.; Eckard, A.; Eggers, P.W.; et al. US Renal Data System 2017 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2018, 71, A7. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.; James, M.; Wiebe, N.; Hemmelgarn, B.; Manns, B.; Klarenbach, S.; Tonelli, M. Cause of Death in Patients with Reduced Kidney Function. J. Am. Soc. Nephrol. 2015, 26, 2504–2511. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Plant—Based Diets Are Associated with a Lower Risk of Incident Cardiovascular Disease, Cardiovascular Disease Mortality, and All—Cause Mortality in a General Population of Middle—Aged Adults. J. Am. Heart Assoc. 2019, 8, e012865. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of Animal and Plant Protein Intake With All-Cause and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef]
- Orlich, M.J.; Singh, P.; Sabaté, J.; Jaceldo-Siegl, K.; Fan, J.; Knutsen, S.; Beeson, W.L.; Fraser, G.E. Vegetarian Dietary Patterns and Mortality in Adventist Health Study 2. JAMA Intern. Med. 2013, 173, 1230–1238. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Chen, S.T.; Maruthur, N.M.; Appel, L.J. The Effect of Dietary Patterns on Estimated Coronary Heart Disease Risk: Results from the Dietary Approaches to Stop Hypertension (DASH) trial. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 484–489. [Google Scholar] [CrossRef]
- Salehi-Abargouei, A.; Maghsoudi, Z.; Shirani, F.; Azadbakht, L. Effects of Dietary Approaches to Stop Hypertension (DASH)-style diet on fatal or nonfatal cardiovascular diseases—Incidence: A systematic review and meta-analysis on observational prospective studies. Nutrition 2013, 29, 611–618. [Google Scholar] [CrossRef]
- Shen, J.; Wilmot, K.A.; Ghasemzadeh, N.; Molloy, D.L.; Burkman, G.; Mekonnen, G.; Gongora, M.C.; Quyyumi, A.A.; Sperling, L.S. Mediterranean Dietary Patterns and Cardiovascular Health. Annu. Rev. Nutr. 2015, 35, 425–449. [Google Scholar] [CrossRef]
- Hummel, S.L.; Seymour, E.M.; Brook, R.D.; Kolias, T.J.; Sheth, S.S.; Rosenblum, H.R.; Wells, J.M.; Weder, A.B. Low-Sodium Dietary Approaches to Stop Hypertension Diet Reduces Blood Pressure, Arterial Stiffness, and Oxidative Stress in Hypertensive Heart Failure With Preserved Ejection Fraction. Hypertension 2012, 60, 1200–1206. [Google Scholar] [CrossRef]
- Huang, X.; Jiménez-Moleón, J.J.; Lindholm, B.; Cederholm, T.; Ärnlöv, J.; Risérus, U.; Sjögren, P.; Carrero, J.J. Mediterranean Diet, Kidney Function, and Mortality in Men with CKD. Clin. J. Am. Soc. Nephrol. 2013, 8, 1548–1555. [Google Scholar] [CrossRef] [PubMed]
- Caldiroli, L.; Molinari, P.; Abinti, M.; Rusconi, C.; Castellano, G.; Vettoretti, S. Can Mediterranean Diet Have a Positive Impact on Kidney Health? A Pending Answer to a Long-Time Question. Nutrients 2022, 14, 4366. [Google Scholar] [CrossRef] [PubMed]
- Hansrivijit, P.; Oli, S.; Khanal, R.; Ghahramani, N.; Thongprayoon, C.; Cheungpasitporn, W. Mediterranean diet and the risk of chronic kidney disease: A systematic review and meta-analysis. Nephrology 2020, 25, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Bacharaki, D.; Ikonomidis, I.; Dermitzaki, E.-K.; Lygerou, D.; Theodoridis, M.; Stylianou, K.; Tsotsorou, O.; Georgoulidou, A.; Balafa, O.; Katsoudas, S.; et al. Adherence to Mediterranean Diet Predicts the Presence of Left Ventricular Hypertrophy (LVH) and Patterns of LV Remodeling in Peritoneal Dialysis (PD) Patients. J. Am. Soc. Nephrol. 2017, 2017, SA-PO738. [Google Scholar]
- Saglimbene, V.M.; Wong, G.; Craig, J.; Ruospo, M.; Palmer, S.C.; Campbell, K.; Larsen, V.G.; Natale, P.; Teixeira-Pinto, A.; Carrero, J.-J.; et al. The Association of Mediterranean and DASH Diets with Mortality in Adults on Hemodialysis: The DIET-HD Multinational Cohort Study. J. Am. Soc. Nephrol. 2018, 29, 1741–1751. [Google Scholar] [CrossRef]
- Bacharaki, D.; Petrakis, I.; Kyriazis, P.; Markaki, A.; Pleros, C.; Tsirpanlis, G.; Theodoridis, M.; Balafa, O.; Georgoulidou, A.; Drosataki, E.; et al. Adherence to the Mediterranean Diet Is Associated with a More Favorable Left Ventricular Geometry in Patients with End-Stage Kidney Disease. J. Clin. Med. 2022, 11, 5746. [Google Scholar] [CrossRef]
- Liu, X.; Hu, Z.; Xu, X.; Li, Z.; Chen, Y.; Dong, J. The associations of plant-based protein intake with all-cause and cardiovascular mortality in patients on peritoneal dialysis. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 967–976. [Google Scholar] [CrossRef]
- Saglimbene, V.M.; Wong, G.; Teixeira-Pinto, A.; Ruospo, M.; Garcia-Larsen, V.; Palmer, S.C.; Natale, P.; Campbell, K.; Carrero, J.-J.; Stenvinkel, P.; et al. Dietary Patterns and Mortality in a Multinational Cohort of Adults Receiving Hemodialysis. Am. J. Kidney Dis. 2020, 75, 361–372. [Google Scholar] [CrossRef]
- González-Ortiz, A.; Xu, H.; Ramos-Acevedo, S.; Avesani, C.M.; Lindholm, B.; Correa-Rotter, R.; Espinosa-Cuevas, Á.; Carrero, J.J. Nutritional status, hyperkalaemia and attainment of energy/protein intake targets in haemodialysis patients following plant-based diets: A longitudinal cohort study. Nephrol. Dial. Transplant. 2020, 36, 681–688. [Google Scholar] [CrossRef]
- Giannikouris, I.E.; Georgoulidou, A.; Dermitzaki, E.; Korovesi, A.; Kokkalis, A.; Stavroulopoulos, A.; Perakis, K.; Theodoridis, M.; Passadakis, P.; Dounousi, E.; et al. sp386mediterranean diet and mortality in chronic kidney disease (ckd) stage 5d (dialysis) patients. Nephrol. Dial. Transplant. 2019, 34, gfz103-SP386. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Fouque, D. Nutritional Management of Chronic Kidney Disease. N. Engl. J. Med. 2017, 377, 1765–1776. [Google Scholar] [CrossRef] [PubMed]
- Ash, S.; Campbell, K.L.; Bogard, J.; Millichamp, A. Nutrition Prescription to Achieve Positive Outcomes in Chronic Kidney Disease: A Systematic Review. Nutrients 2014, 6, 416–451. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.-J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76 (Suppl. S1), S1–S107. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Easterbrook, P.; Gopalan, R.; Berlin, J.; Matthews, D. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Jankowski, J.; Floege, J.; Fliser, D.; Böhm, M.; Marx, N. Cardiovascular Disease in Chronic Kidney Disease: Pathophysiological Insights and Therapeutic Options. Circulation 2021, 143, 1157–1172. [Google Scholar] [CrossRef] [PubMed]
- Carracedo, J.; Alique, M.; Vida, C.; Bodega, G.; Ceprián, N.; Morales, E.; Praga, M.; de Sequera, P.; Ramírez, R. Mechanisms of Cardiovascular Disorders in Patients With Chronic Kidney Disease: A Process Related to Accelerated Senescence. Front. Cell Dev. Biol. 2020, 8, 185. [Google Scholar] [CrossRef] [PubMed]
- Ejaz, A.; Junejo, A.M.; Ali, M.; Ashfaq, A.; Hafeez, A.R.; Khan, S.A. Outcomes of Dialysis Among Patients With End-Stage Renal Disease (ESRD). Cureus 2021, 13, e17006. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Moissl, U.; Chazot, C.; Mallamaci, F.; Tripepi, G.; Arkossy, O.; Wabel, P.; Stuard, S. Chronic Fluid Overload and Mortality in ESRD. J. Am. Soc. Nephrol. 2017, 28, 2491–2497. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Regidor, D.L.; Kovesdy, C.P.; Van Wyck, D.; Bunnapradist, S.; Horwich, T.B.; Fonarow, G.C. Fluid Retention Is Associated With Cardiovascular Mortality in Patients Undergoing Long-Term Hemodialysis. Circulation 2009, 119, 671–679. [Google Scholar] [CrossRef]
- Drost, D.; Kalf, A.; Vogtlander, N.; Van Munster, B.C. High prevalence of frailty in end-stage renal disease. Int. Urol. Nephrol. 2016, 48, 1357–1362. [Google Scholar] [CrossRef]
- Oki, R.; Hamasaki, Y.; Tsuji, S.; Suzuki, K.; Tsuneishi, S.; Imafuku, M.; Komaru, Y.; Miyamoto, Y.; Matsuura, R.; Doi, K.; et al. Clinical frailty assessment might be associated with mortality in incident dialysis patients. Sci. Rep. 2022, 12, 17651. [Google Scholar] [CrossRef]
- Ward, M.M. Socioeconomic Status and the Incidence of ESRD. Am. J. Kidney Dis. 2008, 51, 563–572. [Google Scholar] [CrossRef]
- Nicholas, S.B.; Kalantar-Zadeh, K.; Norris, K.C. Socioeconomic Disparities in Chronic Kidney Disease. Adv. Chronic Kidney Dis. 2015, 22, 6–15. [Google Scholar] [CrossRef]
- D’Elia, L.; Rossi, G.; Ippolito, R.; Cappuccio, F.P.; Strazzullo, P. Habitual salt intake and risk of gastric cancer: A meta-analysis of prospective studies. Clin. Nutr. 2012, 31, 489–498. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-De-Mesquita, B.; Ocké, M.C.; Peeters, P.H.; Van Der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ 2005, 330, 991. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; La Vecchia, C.; Morrison, H.; Negri, E.; Mery, L. Salt, processed meat and the risk of cancer. Eur. J. Cancer Prev. 2011, 20, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-Style Diet for the Primary and Secondary Prevention of Cardiovascular Disease: A Cochrane Review. Glob. Heart 2020, 15, 56. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.H.; Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Oh, K.-H.; Lee, J.; Jung, J.Y.; Lee, K.-B.; Ma, S.K.; et al. Association Between Left Ventricular Geometry and Renal Outcomes in Patients With Chronic Kidney Disease: Findings From Korean Cohort Study for Outcomes in Patients With Chronic Kidney Disease Study. Front. Cardiovasc. Med. 2022, 9, 848692. [Google Scholar] [CrossRef]
- Lee, Y.-T.; Chiu, H.-C.; Su, H.-M.; Voon, W.-C.; Lin, T.-H.; Lai, W.-T.; Sheu, S.-H. Presence of Chronic Kidney Disease and Subsequent Changes of Left Ventricular Geometry over 4 Years in an Apparently Healthy Population Aged 60 and Older. Hypertens. Res. 2008, 31, 913–920. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gallieni, M.; Pedone, M. Left ventricular hypertrophy and serum phosphate in peritoneal dialysis patients. Kidney Int. 2013, 84, 850. [Google Scholar] [CrossRef]
- Ozkahya, M.; Ok, E.; Cirit, M.; Aydin, S.; Akçiçek, F.; Başçi, A.; Mees, E.J.D. Regression of left ventricular hypertrophy in haemodialysis patients by ultrafiltration and reduced salt intake without antihypertensive drugs. Nephrol. Dial. Transplant. 1998, 13, 1489–1493. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Saglimbene et al. [15] | Saglimbene et al. [18] | Bacharaki et al. [16] | Gonzalez-Ortiz et al. [19] | Liu et al. [17] | Giannikouris et al. [20] | Bacharaki et al. [14] |
|---|---|---|---|---|---|---|---|
| Year | 2018 | 2020 | 2022 | 2021 | 2020 | 2019 | 2017 |
| Study design | Cohort study | Cohort Study | Cross-sectional | Cohort study | Cohort study | Cohort study | Cross-sectional |
| Number of Patients | 8110 HD patients | 8110 HD patients | 127 patients overall, 69 on HD, 58 on PD | 150 HD patients | 884 PD patients | 129 patients overall, 66 on HD, 63 on PD | 53 PD patients |
| Age | mean age 63.1 ± 15 | mean age 63 ± 15 | mean age 62 ± 15 | mean age 42 ± 18 | mean age 57.7 ± 14.8 | mean age 62 ± 15 | mean age 62 ± 14 |
| Sex | 58% male | 58% male | 54% male | 41% male | 49% male | 60% male | 51% male |
| Type of Diet | Mediterranean diet DASH diet | Plant-Based diet | Mediterranean diet | Plant-Based diet | Plant-based protein—total protein ratio | Mediterranean diet | Mediterranean diet |
| Follow Up Time | 2.7 years | 2.7 years | N/A | 1 year | 3.8 years | 1.7 years | N/A |
| All-Cause Mortality OR (95% CI) | Mediterranean diet Q3 vs. Q1 1.01 (0.88–1.17) DASH diet Q3 vs. Q1 1.00 (0.89–1.12) | Q4 vs. Q1 0.87 (0.72–1.05) | N/A | N/A | Q3 vs. Q1 0.86 (0.67–1.11) | High vs. low MDS group 0.12 (0.01–0.96) | N/A |
| Cardiovascular mortality OR (95% CI) | Mediterranean diet Q3 vs. Q1 1.14 (0.90–1.43) DASH diet Q3 vs. Q1 1.19 (0.99–1.43) | Q4 vs. Q1 0.91 (0.69–1.21) | N/A | N/A | Q3 vs. Q1 0.75 (0.49–1.14) | N/A | N/A |
| LVH OR (95% CI) | N/A | N/A | Per 1 point 0.82 (0.68–0.99) | N/A | N/A | N/A | Per 1 point 0.75 (0.57–0.93) |
| Hyperkalemia OR (95% CI) | Per 1 unit 1.00 (0.94–1.07) | ||||||
| Confounder adjustment | Random effect to estimate the associations between dietary pattern scores and mortality, sex, daily physical activity, education, diabetes, smoking, MI, vascular access type, BMI, albumin, Charlson comorbidity index, score, age, phosphorus, calcium, Hemoglobin, Kt/V, energy intake | Random effect to estimate the associations between dietary pattern scores and mortality, sex, daily physical activity, education, diabetes, smoking, MI, vascular access type, BMI, albumin, Charlson comorbidity index, score, age, phosphorus, calcium, Hemoglobin, Kt/V, energy intake | Dialysis mode, sex, age, PVD, CAD, diabetes, BMI, plasma phosphorus, serum albumin, serum magnesium | Age, sex, dialysis vintage, occupation, diabetes, hypertension, CVD history, RAS blockers, loop diuretics use and servings of fat | Age, gender, income, Diabetes Mellitus, CVD, time averaged variables, BMI, hemoglobin, albumin, C-reactive protein, plasma protein level, parathyroid hormone, total energy intake, total fiber intake | Age, cardiovascular disease, serum albumin and malnutrition- inflammation score | N/A |
| Quality assessment | S4, C1, O3 | S4, C1, O3, | S2, C1, O3 | S4, C1, O2 | S3, C1, O3 | S4, C1, O3 | S2, C0, O3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charkviani, M.; Thongprayoon, C.; Tangpanithandee, S.; Krisanapan, P.; Miao, J.; Mao, M.A.; Cheungpasitporn, W. Effects of Mediterranean Diet, DASH Diet, and Plant-Based Diet on Outcomes among End Stage Kidney Disease Patients: A Systematic Review and Meta-Analysis. Clin. Pract. 2023, 13, 41-51. https://doi.org/10.3390/clinpract13010004
Charkviani M, Thongprayoon C, Tangpanithandee S, Krisanapan P, Miao J, Mao MA, Cheungpasitporn W. Effects of Mediterranean Diet, DASH Diet, and Plant-Based Diet on Outcomes among End Stage Kidney Disease Patients: A Systematic Review and Meta-Analysis. Clinics and Practice. 2023; 13(1):41-51. https://doi.org/10.3390/clinpract13010004
Chicago/Turabian StyleCharkviani, Mariam, Charat Thongprayoon, Supawit Tangpanithandee, Pajaree Krisanapan, Jing Miao, Michael A. Mao, and Wisit Cheungpasitporn. 2023. "Effects of Mediterranean Diet, DASH Diet, and Plant-Based Diet on Outcomes among End Stage Kidney Disease Patients: A Systematic Review and Meta-Analysis" Clinics and Practice 13, no. 1: 41-51. https://doi.org/10.3390/clinpract13010004
APA StyleCharkviani, M., Thongprayoon, C., Tangpanithandee, S., Krisanapan, P., Miao, J., Mao, M. A., & Cheungpasitporn, W. (2023). Effects of Mediterranean Diet, DASH Diet, and Plant-Based Diet on Outcomes among End Stage Kidney Disease Patients: A Systematic Review and Meta-Analysis. Clinics and Practice, 13(1), 41-51. https://doi.org/10.3390/clinpract13010004