
The Use of Artificial Intelligence in Medical Imaging: A Nationwide Pilot Survey of Trainees in Saudi Arabia

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Sampling Technique and Sample Size Determination
2.3. Questionnaire and Data Collection
2.4. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Exposure to and Interest in Artificial Intelligence in Radiology
3.3. Levels of Use of AI Radiology
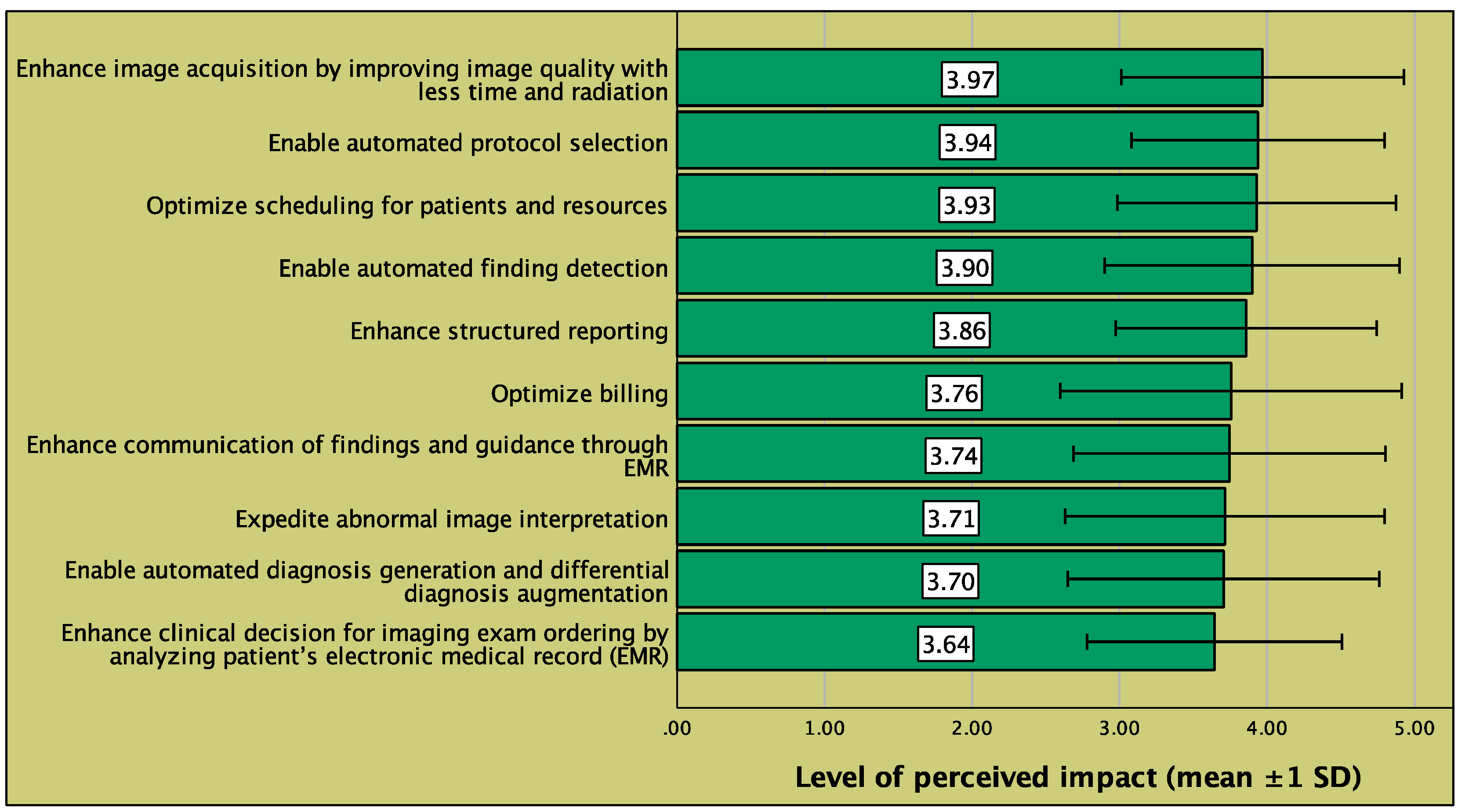
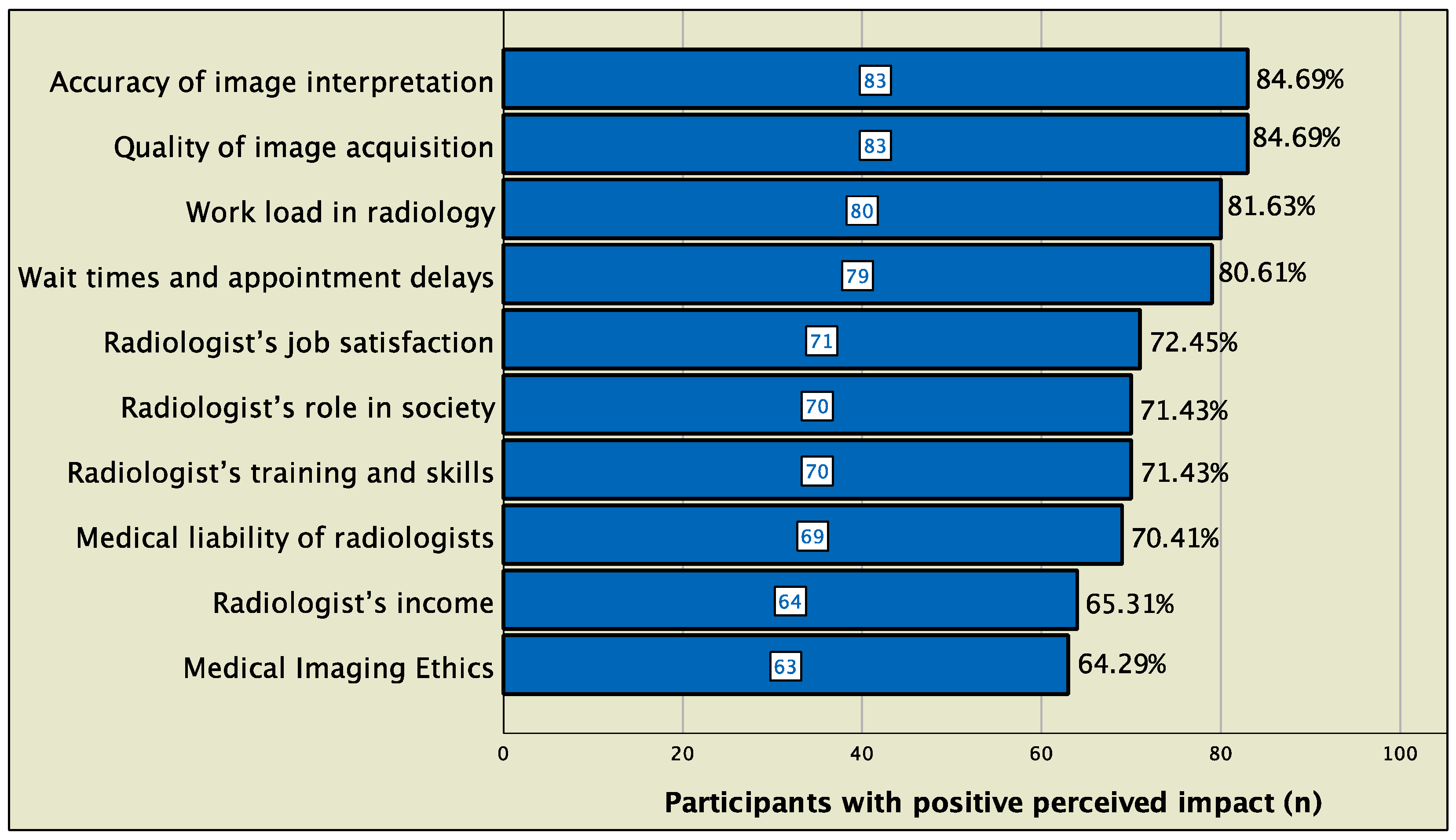
3.4. Perceived Impact of AI on Radiology Workflow and the Radiology Profession
3.5. Internal Consistency of the Study Scales
3.6. Factors Associated with Perceived Impact of AI on Standard Radiology Workflow and on the Radiology Profession
3.7. Factors Associated with Perceived Ease of Use (PEoU) of AI
3.8. Factors Associated with Behavioral Intention (BI) to Use AI
4. Discussion
4.1. Exposure and Levels of Use
4.2. Perceived Impact of AI on Radiology Workflow and Radiologist Profession
4.3. Acceptance of AI in Radiology
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Level of Use of Artificial Intelligence Radiology | |
|---|---|
| LoU0 | I have no experience in AI Radiology; I have no significant knowledge about it and I am doing nothing towards becoming involved in it |
| LoU1 | I have acquired or am acquiring information about AI Radiology; I am exploring its value and its demands upon physicians and health institutions |
| LoU2 | I think I am ready for AI Radiology implementation and am preparing for my first use |
| LoU3 | I have already made my first steps in AI Radiology; I am using it superficially or whenever I need it |
| LoU4a | I am using AI Radiology in my routine practice but I have no idea about its impact on my patients or the quality of care |
| LoU4b | I am using AI Radiology and attempting to optimize my use to meet my patients’ needs and or improve my clinical practice |
| LoU5 | I am using AI Radiology and coordinating my efforts with other colleagues and health professionals for best effect on patient care |
| LoU6 | I am using AI Radiology and I think there are some necessary modifications to the system to achieve increased impact of patients; Or, I am using AI Radiology and I think its scope should be expanded to new goals |
Appendix B
| To What Extent Do You Think Artificial Intelligence Can or Will Impact the Following Steps of Standard Radiology Workflow? | ||||||
|---|---|---|---|---|---|---|
| 1 ○ No impact 2 ○ Small impact 3 ○ Moderate impact 4 ○ Large impact 5 ○ Drastic impact | ||||||
| 01 | Enhance clinical decision for imaging exam ordering by analyzing patient’s EMR | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| 02 | Optimize scheduling for patients and resources | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| 03 | Enable automated protocol selection | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| 04 | Enhance image acquisition by improving image quality with less time and radiation | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| 05 | Enable automated finding detection | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| 06 | Enable automated diagnosis generation and differential diagnosis augmentation | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| 07 | Expedite abnormal image interpretation | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| 08 | Enhance structured reporting | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| 09 | Enhance communication of findings and guidance through EMR | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| 10 | Optimize billing | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
Appendix C
| How Would the Implementation of Artificial Intelligence Impact Each of the Following Aspects of the Radiologist Profession? | ||||||
|---|---|---|---|---|---|---|
| −2 ○ Very negative impact −1 ○ Negative impact 0 ○ Mixed opinion, or no impact +1 ○ Positive impact +2 ○ Very positive impact | ||||||
| 01 | Medical Imaging Ethics | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
| 02 | Medical liability of radiologists | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
| 03 | Quality of image acquisition | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
| 04 | Accuracy of image interpretation | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
| 05 | Wait times and appointment delays | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
| 06 | Work load in radiology | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
| 07 | Radiologist’s role in society | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
| 08 | Radiologist’s income | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
| 09 | Radiologist’s training and skills | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
| 10 | Radiologist’s job satisfaction | −2 ○ | −1 ○ | 0 ○ | +1 ○ | +2 ○ |
Appendix D
| Please Rate Your Level of Agreement to the Following Statements: | ||||||
|---|---|---|---|---|---|---|
| 1 ○ Extremely disagree 2 ○ Disagree 3 ○ I do not know 4 ○ Agree 5 ○ Extremely agree | ||||||
| PEoU1 | Understanding the principles of AI Radiology would be easy for me | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| PEoU2 | Learning to operate AI Radiology would be easy for me | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| PEoU3 | I would find it easy to do all what I need to do in my practice using AI Radiology | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| BI1 | Assuming I have access to the system, I intend to use AI Radiology | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| BI2 | To the extent possible, I intend to use AI technology in all dimensions of my radiology practice | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
| BI3 | I intend to encourage my colleagues to use AI Radiology | 1 ○ | 2 ○ | 3 ○ | 4 ○ | 5 ○ |
References
- Sohail, A.; Yu, Z.; Nutini, A. COVID-19 Variants and Transfer Learning for the Emerging Stringency Indices. Neural Process. Lett. 2022, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Arel, I.; Rose, D.C.; Karnowski, T.P. Deep machine learning-a new frontier in artificial intelligence research [research frontier]. IEEE Comput. Intell. Mag. 2010, 5, 13–18. [Google Scholar] [CrossRef]
- Ongsulee, P. Artificial intelligence, machine learning and deep learning. In Proceedings of the 2017 15th International Conference on ICT and Knowledge Engineering (ICT&KE), Bangkok, Thailand, 22–24 November 2017. [Google Scholar]
- Miotto, R.; Wang, F.; Wang, S.; Jiang, X.; Dudley, J.T. Deep learning for healthcare: Review, opportunities and challenges. Brief Bioinf. 2018, 19, 1236–1246. [Google Scholar] [CrossRef] [PubMed]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef]
- Ting, D.S.W.; Pasquale, L.R.; Peng, L.; Campbell, J.P.; Lee, A.Y.; Raman, R.; Tan, G.S.W.; Schmetterer, L.; Keane, P.A.; Wong, T.Y. Artificial intelligence and deep learning in ophthalmology. Br. J. Ophthalmol. 2019, 103, 167–175. [Google Scholar] [CrossRef]
- Sohail, A.; Bég, O.A.; Li, Z.; Celik, S. Physics of fractional imaging in biomedicine. Prog. Biophys. Mol. Biol. 2018, 140, 13–20. [Google Scholar] [CrossRef]
- Syed, A.B.; Zoga, A.C. Artificial Intelligence in Radiology: Current Technology and Future Directions. Semin. Musculoskelet. Radiol. 2018, 22, 540–545. [Google Scholar]
- Tang, A.; Tam, R.; Cadrin-Chênevert, A.; Guest, W.; Chong, J.; Barfett, J.; Chepelev, L.; Cairns, R.; Mitchell, J.R.; Cicero, M.D.; et al. Canadian Association of Radiologists White Paper on Artificial Intelligence in Radiology. Can. Assoc. Radiol. J. 2018, 69, 120–135. [Google Scholar] [CrossRef]
- Eltorai, A.E.M.; Bratt, A.K.; Guo, H.H. Thoracic Radiologists’ Versus Computer Scientists’ Perspectives on the Future of Artificial Intelligence in Radiology. J. Thorac. Imaging 2020, 35, 255–259. [Google Scholar] [CrossRef]
- Qurashi, A.A.; Alanazi, R.K.; Alhazmi, Y.M.; Almohammadi, A.S.; Alsharif, W.M.; Alshamrani, K.M. Saudi Radiology Personnel’s Perceptions of Artificial Intelligence Implementation: A Cross-Sectional Study. J. Multidiscip. Healthc. 2021, 14, 3225–3231. [Google Scholar] [CrossRef]
- Abuzaid, M.M.; Elshami, W.; McConnell, J.; Tekin, H.O. An extensive survey of radiographers from the Middle East and India on artificial intelligence integration in radiology practice. Health Technol. 2021, 11, 1045–1050. [Google Scholar] [CrossRef] [PubMed]
- Tajaldeen, A.; Alghamdi, S. Evaluation of radiologist’s knowledge about the Artificial Intelligence in diagnostic radiology: A survey-based study. Acta Radiol. Open 2020, 9, 20–58. [Google Scholar] [CrossRef] [PubMed]
- Ooi, S.K.G.; Makmur, A.; Soon, A.Y.Q.; Fook-Chong, S.; Liew, C.; Sia, S.Y.; Ting, Y.H.; Lim, C.Y. Attitudes toward artificial intelligence in radiology with learner needs assessment within radiology residency programmes: A national multi-programme survey. Singap. Med. J. 2021, 62, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Abuzaid, M.M.; Elshami, W.; Tekin, H.; Issa, B. Assessment of the Willingness of Radiologists and Radiographers to Accept the Integration of Artificial Intelligence Into Radiology Practice. Acad. Radiol. 2022, 29, 87–94. [Google Scholar] [CrossRef]
- Coppola, F.; Faggioni, L.; Regge, D.; Giovagnoni, A.; Golfieri, R.; Bibbolino, C.; Miele, V.; Neri, E.; Grassi, R. Artificial intelligence: Radiologists’ expectations and opinions gleaned from a nationwide online survey. Radiol. Med. 2021, 126, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Reznick, R.K.; Harris, K.; Horsley, T. Task Force Report on Artificial Intelligence and Emerging Digital Technologies. 2020. Available online: https://www.royalcollege.ca/rcsite/health-policy/initiatives/ai-task-force-e (accessed on 21 February 2022).
- Collado-Mesa, F.; Alvarez, E.; Arheart, K. The Role of Artificial Intelligence in Diagnostic Radiology: A Survey at a Single Radiology Residency Training Program. J. Am. Coll. Radiol. 2018, 15, 1753–1757. [Google Scholar] [CrossRef]
- European Society of Radiology (ESR). Impact of artificial intelligence on radiology: A EuroAIM survey among members of the European Society of Radiology. Insights Imaging 2019, 10, 105. [Google Scholar] [CrossRef]
- Khafaji, M.A.; Safhi, M.A.; Albadawi, R.H.; Al-Amoudi, S.O.; Shehata, S.S.; Toonsi, F. Artificial intelligence in radiology: Are Saudi residents ready, prepared, and knowledgeable? Saudi Med. J. 2022, 43, 53–60. [Google Scholar] [CrossRef]
- Hall, G.E.; Dirksen, D.J.; George, A.A. Measuring Implementation in Schools: Levels of Use; Southwest Educational Development Laboratory: Austin, TX, USA, 2006. [Google Scholar]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef]
- Lai, P.C. The literature review of technology adoption models and theories for the novelty technology. J. Inf. Technol. Manag. 2017, 14, 21–38. [Google Scholar] [CrossRef]
- Ministry of Health. National E-Health Strategy. Available online: https://www.moh.gov.sa/en/Ministry/nehs/Pages/default.aspx (accessed on 10 May 2022).
- Rahman, R.; Al-Borie, H.M. Strengthening the Saudi Arabian healthcare system: Role of Vision 2030. J. Healthc. Manag. 2021, 14, 1483–1491. [Google Scholar] [CrossRef]
- Alelyani, M.; Alamri, S.; Alqahtani, M.S.; Musa, A.; Almater, H.; Alqahtani, N.; Alshahrani, F.; Alelyani, S. Radiology Community Attitude in Saudi Arabia about the Applications of Artificial Intelligence in Radiology. Healthcare 2021, 9, 834. [Google Scholar] [CrossRef]
- Alexander, A.; Jiang, A.; Ferreira, C.; Zurkiya, D. An Intelligent Future for Medical Imaging: A Market Outlook on Artificial Intelligence for Medical Imaging. J. Am. Coll. Radiol. 2020, 17 Pt B, 165–170. [Google Scholar] [CrossRef]
- Hardy, M.; Harvey, H. Artificial intelligence in diagnostic imaging: Impact on the radiography profession. Br. J. Radiol. Suppl. 2020, 93, 20190840. [Google Scholar] [CrossRef]
- Tran, W.T.; Sadeghi-Naini, A.; Lu, F.I.; Gandhi, S.; Meti, N.; Brackstone, M.; Rakovitch, E.; Curpen, B. Computational Radiology in Breast Cancer Screening and Diagnosis Using Artificial Intelligence. Can. Assoc. Radiol. J. 2021, 72, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Scheetz, J.; Rothschild, P.; McGuinness, M.; Hadoux, X.; Soyer, H.P.; Janda, M.; Condon, J.J.J.; Oakden-Rayner, L.; Palmer, L.J.; Keel, S.; et al. A survey of clinicians on the use of artificial intelligence in ophthalmology, dermatology, radiology and radiation oncology. Sci. Rep. 2021, 11, 5193. [Google Scholar] [CrossRef]
- Bi, W.L.; Hosny, A.; Schabath, M.B.; Giger, M.L.; Birkbak, N.J.; Mehrtash, A.; Allison, T.; Arnaout, O.; Abbosh, C.; Dunn, I.F.; et al. Artificial intelligence in cancer imaging: Clinical challenges and applications. CA Cancer J. Clin. 2019, 69, 127–157. [Google Scholar] [CrossRef]
- Coppola, F.; Faggioni, L.; Gabelloni, M.; de Vietro, F.; Mendola, V.; Cattabriga, A.; Cocozza, M.A.; Vara, G.; Piccinino, A.; Monaco, S.L.; et al. Human, All Too Human? An All-Around Appraisal of the “Artificial Intelligence Revolution” in Medical Imaging. Front. Psychol. 2021, 12, 710982. [Google Scholar] [CrossRef]
- Alsharif, W.; Qurashi, A.; Toonsi, F.; Alanazi, A.; Alhazmi, F.; Abdulaal, O.; Aldahery, S.; Alshamrani, K. A qualitative study to explore opinions of Saudi Arabian radiologists concerning AI-based applications and their impact on the future of the radiology. BJR Open 2022, 4, 20210029. [Google Scholar] [CrossRef]



| Parameter | Unit | Mean | SD |
|---|---|---|---|
| Age | years | 27.59 | 2.02 |
| Parameter | Category | Frequency | Percentage |
| Gender | Male | 51 | 52.04 |
| Female | 47 | 47.96 | |
| Province | Makkah | 55 | 56.70 |
| Riyadh | 17 | 17.53 | |
| Eastern Province | 16 | 16.49 | |
| Madinah | 4 | 4.12 | |
| Jizan | 3 | 3.09 | |
| Aseer | 2 | 2.06 | |
| Sector | Ministry of Health | 77 | 78.57 |
| University | 7 | 7.14 | |
| Military | 9 | 9.18 | |
| Other | 5 | 5.10 | |
| Academic degree | Bachelor’s | 94 | 95.92 |
| Masters or PhD | 4 | 4.08 | |
| Current professional activity | Academic | 10 | 10.20 |
| Non-academic | 28 | 28.57 | |
| Mixed | 60 | 61.22 |
| Item | Levels, % (n = 98) | ||||
|---|---|---|---|---|---|
| Familiarity | 1 ○ Never heard about it | 2 ○ Heard about it but not familiar with what it stands for | 3 ○ Heard about it but barely understand what it is | 4 ○ Familiar with its basics | 5 ○ Have accurate knowledge about it |
| AI | 8.2% | 15.3% | 31.6% | 42.9% | 2.0% |
| ML | 16.3% | 15.3% | 29.6% | 36.7% | 2.0% |
| DL | 19.4% | 19.4% | 25.5% | 33.7% | 2.0% |
| Data science | 16.3% | 17.3% | 25.5% | 38.8% | 2.0% |
| Involvement | 1 ○ No, and not interested | 2 ○ No, but interested | 3 ○ Yes | ||
| Reading journal articles about AI radiology | 14.3% | 46.9% | 38.8% | ||
| Attending AI radiology courses | 15.3% | 60.2% | 24.5% | ||
| Scale | No. Items | Cronbach’s Alpha | Internal Consistency Level | Score Statistics | Ref. Scale Range | ||
|---|---|---|---|---|---|---|---|
| Mean | SD | Range | |||||
| Perceptions about AI impact on the radiology workflow | 10 | 0.955 | Very high | 38.15 | 8.37 | 10, 50 | 10, 50 |
| Attitudes regarding AI impact on the radiology profession | 10 | 0.926 | Very high | 9.37 | 7.39 | −9, 20 | −20, +20 |
| Perceived ease of use | 3 | 0.883 | High | 11.88 | 2.00 | 9, 15 | 3, 15 |
| Behavioural intention | 3 | 0.888 | High | 12.21 | 2.00 | 8, 15 | 3, 15 |
| Parameter | Unit | Perceived Impact on Standard Radiology Workflow | Perceived Impact on the Radiology Profession | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | p-Value | Mean | SD | p-Value | ||
| Age | <28 years | 39.83 | 8.00 | 0.007 # | 11.22 | 5.95 | <0.001 # |
| ≥28 years | 35.14 | 8.29 | 6.03 | 8.57 | |||
| Gender | Male | 38.55 | 6.58 | 0.628 # | 9.02 | 6.60 | 0.630 # |
| Female | 37.72 | 10.01 | 9.74 | 8.21 | |||
| Province | Makkah | 38.51 | 8.87 | 0.433 * | 10.11 | 7.47 | 0.592 * |
| Riyadh | 38.59 | 6.39 | 9.94 | 7.89 | |||
| Eastern Province | 35.44 | 8.97 | 6.19 | 7.73 | |||
| Madinah | 40.75 | 1.50 | 10.75 | 4.65 | |||
| Jizan | 34.67 | 12.86 | 8.67 | 7.09 | |||
| Aseer | 47.00 | 0.00 | 10.00 | 0.00 | |||
| Sector | Ministry of Health | 39.30 | 6.98 | 0.057 * | 10.05 | 7.29 | 0.214 * |
| University | 33.43 | 13.05 | 4.71 | 6.50 | |||
| Military | 32.89 | 12.44 | 9.00 | 7.98 | |||
| Other | 36.60 | 8.91 | 6.00 | 7.97 | |||
| Academic degree | Bachelor’s | 37.81 | 8.30 | 0.048 # | 9.07 | 7.28 | 0.028 # |
| Masters or PhD | 46.25 | 6.18 | 16.25 | 7.50 | |||
| Current professional activity | Academic | 27.40 | 9.11 | <0.001 * | 1.50 | 2.88 | <0.001 * |
| Non-academic | 33.96 | 8.38 | 3.82 | 7.89 | |||
| Mixed | 41.90 | 5.31 | 13.27 | 4.41 | |||
| Parameter | Unit | Perceived Ease of Use | Behavioural Intention | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | p-Value | Mean | SD | p-Value | ||||
| Age | <28 years | 13.16 | 1.35 | <0.001 # | 12.76 | 1.64 | <0.001 # | ||
| ≥28 years | 12.17 | 1.34 | 11.23 | 2.22 | |||||
| Gender | Male | 12.78 | 1.29 | 0.875 # | 12.25 | 1.90 | 0.835 # | ||
| Female | 12.83 | 1.56 | 12.17 | 2.13 | |||||
| Province | Makkah | 12.78 | 1.42 | 0.977 * | 12.45 | 2.04 | 0.820 * | ||
| Riyadh | 13.06 | 1.39 | 12.12 | 1.96 | |||||
| Eastern Province | 12.75 | 1.39 | 11.63 | 2.06 | |||||
| Madinah | 12.50 | 2.52 | 12.25 | 2.06 | |||||
| Jizan | 12.67 | 1.53 | 12.00 | 2.65 | |||||
| Aseer | 13.00 | 0.00 | 12.00 | 0.00 | |||||
| Sector | Ministry of Health | 12.88 | 1.40 | 0.402 * | 12.35 | 1.99 | 0.520 * | ||
| University | 12.57 | 0.79 | 11.29 | 2.21 | |||||
| Military | 12.11 | 1.96 | 11.78 | 2.22 | |||||
| Other | 13.20 | 1.10 | 12.20 | 1.64 | |||||
| Academic degree | Bachelor’s | 12.77 | 1.42 | 0.176 # | 12.14 | 1.98 | 0.068 # | ||
| Masters or PhD | 13.75 | 1.26 | 14.00 | 2.00 | |||||
| Current professional activity | Academic | 11.40 | 1.51 | <0.001 * | 10.10 | 1.29 | <0.001 * | ||
| Non-academic | 11.79 | 1.17 | 11.18 | 2.29 | |||||
| Mixed | 13.52 | 1.00 | 13.05 | 1.40 | |||||
| Score | B | 95% CI | R | p-Value | B | 95% CI | R | p-Value | |
| Level of use of AI radiology | 0.40 | 0.22, 0.58 | 0.41 | <0.001 † | 0.50 | 0.24, 0.75 | 0.36 | <0.001 † | |
| Perceived impact on workflow | 0.10 | 0.08, 0.13 | 0.62 | <0.001 † | 0.18 | 0.14, 0.21 | 0.74 | <0.001 † | |
| Perceived impact on profession | 0.14 | 0.11, 0.16 | 0.70 | <0.001 † | 0.22 | 0.19, 0.25 | 0.82 | <0.001 † | |
| Parameter | No. of Levels | Perceived Ease of Use # | Behavioural Intention † | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B | 95% CI | p-Value | B | 95% CI | p-Value | ||||
| Current professional activity | 3 | 0.55 | 0.17 | 0.93 | 0.005 * | NI | |||
| Level of use of AI radiology | (discrete) | 0.15 | 0.01 | 0.29 | 0.043 * | NI | |||
| Perceived impact on workflow | (discrete) | NI | 0.07 | 0.03 | 0.11 | <0.001 * | |||
| Perceived impact on profession | (discrete) | 0.09 | 0.06 | 0.13 | <0.001 * | 0.16 | 0.12 | 0.21 | <0.001 * |
| Model goodness-of-fit (R2) | 0.557 | 0.712 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirza, A.A.; Wazgar, O.M.; Almaghrabi, A.A.; Ghandour, R.M.; Alenizi, S.A.; Mirza, A.A.; Alraddadi, K.S.; Al-Adwani, F.H.; Alsakkaf, M.A.; Aljuaid, S.M. The Use of Artificial Intelligence in Medical Imaging: A Nationwide Pilot Survey of Trainees in Saudi Arabia. Clin. Pract. 2022, 12, 852-866. https://doi.org/10.3390/clinpract12060090
Mirza AA, Wazgar OM, Almaghrabi AA, Ghandour RM, Alenizi SA, Mirza AA, Alraddadi KS, Al-Adwani FH, Alsakkaf MA, Aljuaid SM. The Use of Artificial Intelligence in Medical Imaging: A Nationwide Pilot Survey of Trainees in Saudi Arabia. Clinics and Practice. 2022; 12(6):852-866. https://doi.org/10.3390/clinpract12060090
Chicago/Turabian StyleMirza, Ahmad A., Omar M. Wazgar, Ammar A. Almaghrabi, Roaa M. Ghandour, Sarah A. Alenizi, Abdulrahim A. Mirza, Khalid S. Alraddadi, Fayzah H. Al-Adwani, Mohammed A. Alsakkaf, and Sattam M. Aljuaid. 2022. "The Use of Artificial Intelligence in Medical Imaging: A Nationwide Pilot Survey of Trainees in Saudi Arabia" Clinics and Practice 12, no. 6: 852-866. https://doi.org/10.3390/clinpract12060090
APA StyleMirza, A. A., Wazgar, O. M., Almaghrabi, A. A., Ghandour, R. M., Alenizi, S. A., Mirza, A. A., Alraddadi, K. S., Al-Adwani, F. H., Alsakkaf, M. A., & Aljuaid, S. M. (2022). The Use of Artificial Intelligence in Medical Imaging: A Nationwide Pilot Survey of Trainees in Saudi Arabia. Clinics and Practice, 12(6), 852-866. https://doi.org/10.3390/clinpract12060090