
Disappearance of Plaque Following Treatment with Antioxidants in Peyronie’s Disease Patients—A Report of 3 Cases


Abstract
1. Introduction
2. Case Presentations
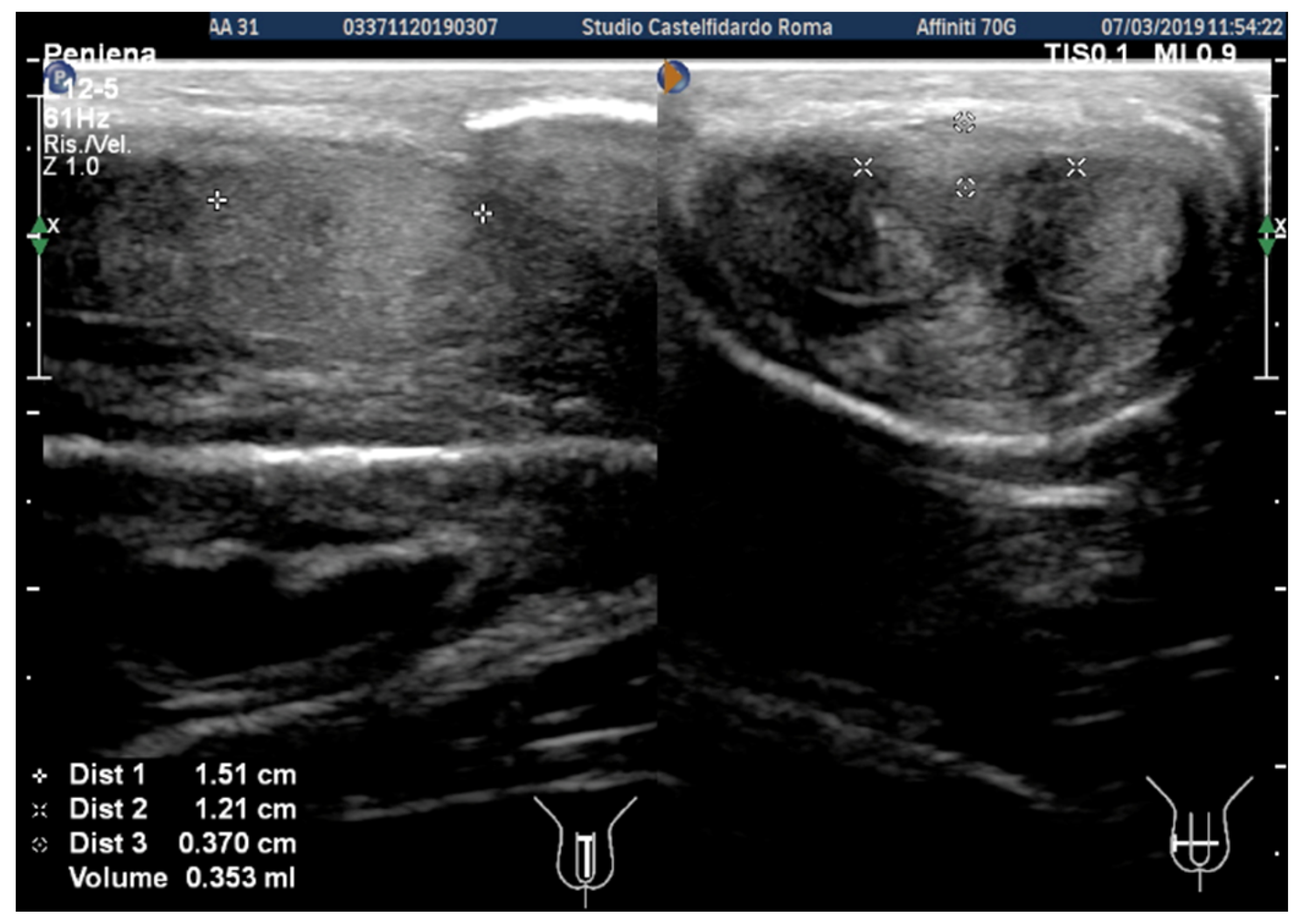
2.1. Case 1
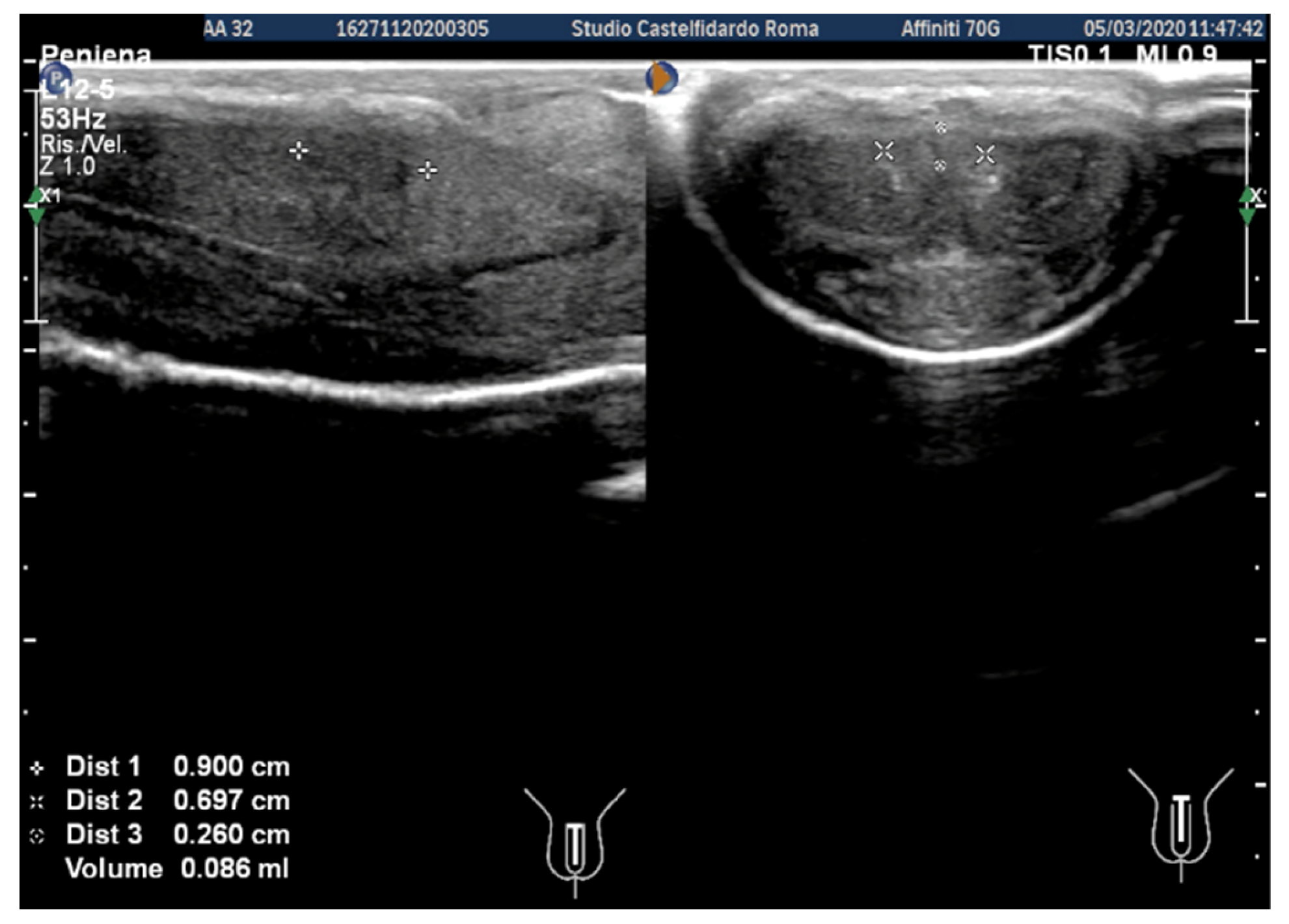
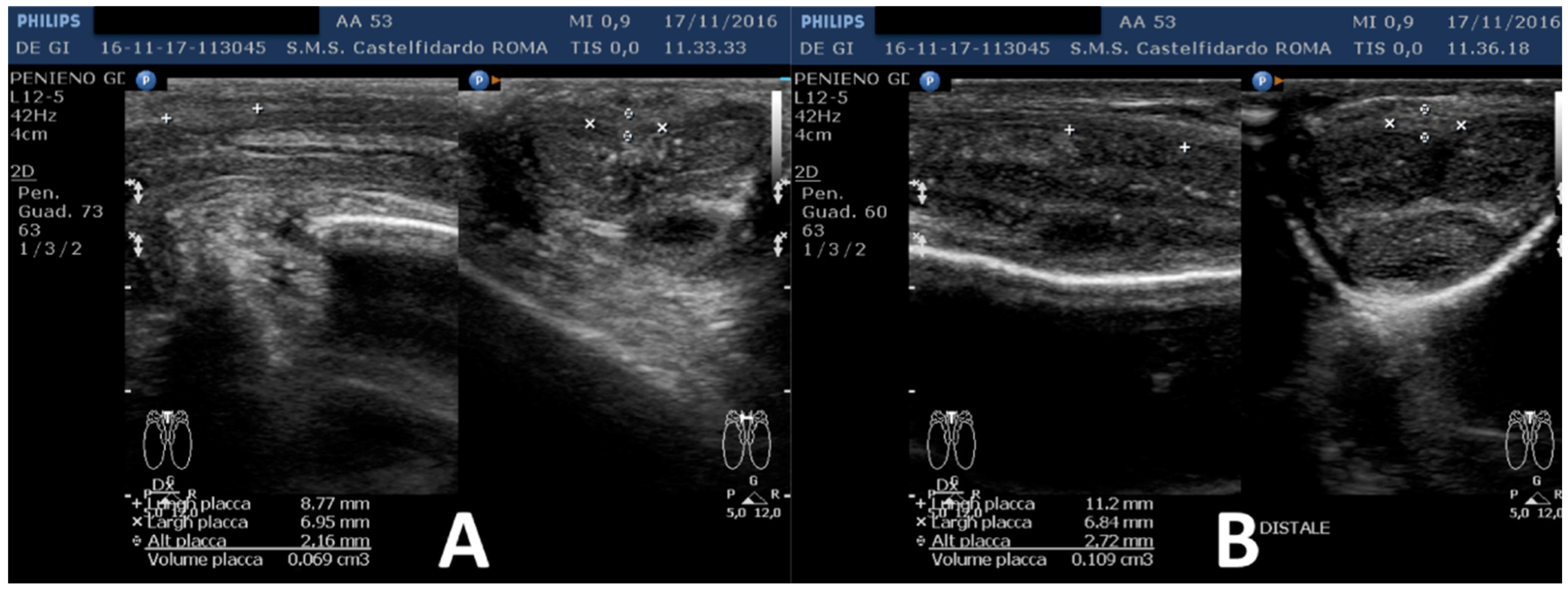
2.2. Case 2
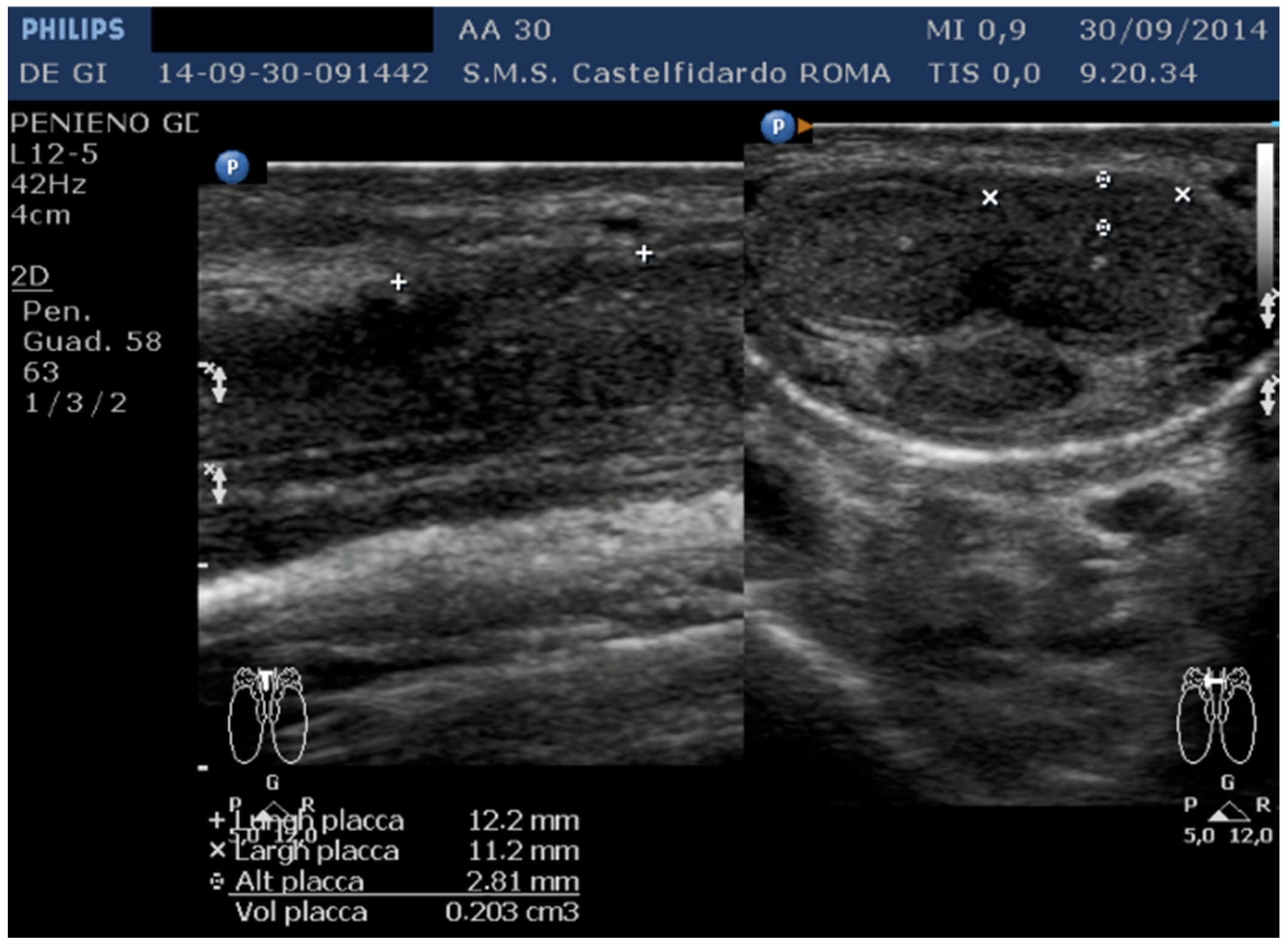
2.3. Case 3
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hellstrom, W.J.; Bivalacqua, T.J. Peyronie’s disease: Etiology, medical, and surgical therapy. J. Androl. 2000, 21, 347–354. [Google Scholar] [PubMed]
- Weidner, W.; Schroeder-Printzen, I.; Weiske, W.H.; Vosshenrich, R. Sexual dysfunction in Peyronie’s disease: An analysis of 222 patients without previous local plaque therapy. J. Urol. 1997, 157, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Paulis, G.; Romano, G.; Paulis, A. Prevalence, psychological impact, and risk factors of erectile dysfunction in patients with Peyronie’s disease: A retrospective analysis of 309 cases. Res. Rep. Urol. 2016, 8, 95–103. [Google Scholar] [PubMed]
- Schwarzer, U.; Sommer, F.; Klotz, T.; Braun, M.; Reifenrath, B.; Engelmann, U. The prevalence of Peyronie’s disease: Results of a large survey. BJU Int. 2001, 88, 727–730. [Google Scholar] [CrossRef] [PubMed]
- DiBenedetti, D.B.; Nguyen, D.; Zografos, L.; Ziemiecki, R.; Zhou, X. A Population-based study of peyronie’s disease: Prevalence and treatment patterns in the United States. Adv. Urol. 2011, 2011, 282503. [Google Scholar] [CrossRef]
- Stuntz, M.; Perlaky, A.; des Vignes, F.; Kyriakides, T.; Glass, D. The Prevalence of Peyronie’s Disease in the United States: A Population-Based Study. PLoS ONE 2016, 11, e0150157. [Google Scholar] [CrossRef]
- Devine, C.J., Jr.; Somers, K.D.; Ladaga, L.E. Peyronie’s disease: Pathophysiology. Prog. Clin. Biol. Res. 1991, 370, 355–358. [Google Scholar]
- Devine, C.J.J.; Somers, K.D.; Jordan, G.H.; Schlossberg, S.M. Proposal: Trauma as a cause of Peyronie’s lesion. J. Urol. 1997, 157, 285–290. [Google Scholar] [CrossRef]
- Jarow, J.P.; Lowe, F.C. Penile trauma: An etiologic factor in Peyronie’s disease and erectile dysfunction. J. Urol. 1997, 158, 1388–1390. [Google Scholar] [CrossRef]
- Segundo, A.; Glina, S. Prevalence, Risk Factors, and Erectile Dysfunction Associated with Peyronie’s Disease Among Men Seeking Urological Care. Sex Med. 2020, 8, 230–236. [Google Scholar] [CrossRef]
- Somers, K.D.; Dawson, D.M. Fibrin deposition in Peyronie’s disease plaque. J. Urol. 1997, 157, 311–315. [Google Scholar] [CrossRef]
- Sikka, S.C.; Hellstrom, W.J. Role of oxidative stress and antioxidants in Peyronie’s disease. Int. J. Impot. Res. 2002, 14, 353–360. [Google Scholar] [CrossRef]
- El-Sakka, A.I.; Salabas, E.; Dinçer, M.; Kadioglu, A. The pathophysiology of Peyronie’s disease. Arab. J. Urol. 2013, 11, 272–277. [Google Scholar] [CrossRef]
- Paulis, G.; Romano, G.; Paulis, L.; Barletta, D. Recent Pathophysiological Aspects of Peyronie’s Disease: Role of Free Radicals, Rationale, and Therapeutic Implications for Antioxidant Treatment-Literature Review. Adv. Urol. 2017, 2017, 4653512. [Google Scholar] [CrossRef]
- Levine, L.A.; Larsen, S. Diagnosis and management of Peyronie disease. In Campbell-Walsh Urology, 11th ed.; Wein, A.J., Kavoussi, L.R., Partin, A.W., Peters, C.A., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2015; pp. 722–748. [Google Scholar]
- Nguyen, H.N.T.; Anaissie, J.; DeLay, K.J.; Yafi, F.A.; Sikka, S.C.; Hellstrom, W.J. Safety and efficacy of collagenase Clostridium histolyticum in the treatment of acute-phase Peyronie’s disease. J. Sex Med. 2017, 14, 1220–1225. [Google Scholar] [CrossRef]
- Chung, E.; Ralph, D.; Kagioglu, A.; Garaffa, G.; Shamsodini, A.; Bivalacqua, T.; Glina, S.; Hakim, H.; Sadeghi-Nejad, H.; Broderick, G. Evidence-based management guidelines on Peyronie’s disease. J. Sex Med. 2016, 13, 905–923. [Google Scholar] [CrossRef]
- Lee, J.S.; Chung, B.H. Transrectal ultrasound versus magnetic resonance imaging in the estimation of prostate volume as compared with radical prostatectomy specimens. Urol. Int. 2007, 78, 323–327. [Google Scholar] [CrossRef]
- Eri, L.M.; Thomassen, H.; Brennhovd, B.; Håheim, L.L. Accuracy and repeatability of prostate volume measurements by transrectal ultrasound. Prostate Cancer Prostatic Dis. 2002, 5, 273–278. [Google Scholar] [CrossRef]
- Gallo, L.; Sarnacchiaro, P. Ten-year experience with multimodal treatment for acute phase Peyronie’s disease: A real life clinical report. Actas Urol. Esp. (Engl. Ed.). 2019, 43, 182–189. [Google Scholar] [CrossRef]
- Paulis, G.; Barletta, D.; Turchi, P.; Vitarelli, A.; Dachille, G.; Fabiani, A.; Romano, G. Efficacy and safety evaluation of pentoxifylline associated with other antioxidants in medical treatment of Peyronie’s disease: A case-control study. Res. Rep. Urol. 2016, 8, 1–10. [Google Scholar] [CrossRef]
- Paulis, G.; Cavallini, G.; De Giorgio, G.; Quattrocchi, S.; Brancato, T.; Alvaro, R. Long-term multimodal therapy (verapamil associated with propolis, blueberry, vitamin E and local diclofenac) on patients with Peyronie’s disease (chronic inflammation of the tunica albuginea). Results of a controlled study. Inflamm. Allergy Drug Targets 2013, 12, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Favilla, V.; Russo, G.I.; Privitera, S.; Castelli, T.; Madonia, M.; la Vignera, S.; Condorelli, R.; Calogero, A.E.; Farina, F.P.; Cimino, S.; et al. Combination of intralesional verapamil and oral antioxidants for Peyronie’s disease: A prospective, randomised controlled study. Andrologia 2014, 46, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Riedl, C.R.; Sternig, P.; Gallé, G.; Langmann, F.; Vcelar, B.; Vorauer, K.; Wagner, A.; Katinger, H.; Pflüger, H. Liposomal recombinant human superoxide dismutase for the treatment of Peyronie’s disease: A randomized placebo-controlled double-blind prospective clinical study. Eur. Urol. 2005, 48, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, M.; Karimi, F.; Fallah, M.R. Evaluation of verapamil efficacy in Peyronie’s disease comparing with pentoxifylline. Glob. J. Health Sci. 2014, 6, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Hatzimouratidis, K.; Eardley, I.; Giuliano, F.; Hatzichristou, D.; Moncada, I.; Salonia, A.; Vardi, Y.; Wespes, E. EAU guidelines on penile curvature. Eur. Urol. 2012, 62, 543–552. [Google Scholar] [CrossRef]
- Nehra, A.; Alterowitz, R.; Culkin, D.J.; Faraday, M.M.; Hakim, L.S.; Heidelbaugh, J.J.; Khera, M.; Kirkby, E.; McVary, K.T.; Miner, M.M. Peyronie’s disease: AUA guideline. J. Urol. 2015, 194, 745–753. [Google Scholar] [CrossRef]
- Paulis, G.; De Giorgio, G. Complete Plaque Regression in Patients with Peyronie’s Disease After Multimodal Treatment with Antioxidants. A Report of 2 Cases. Am. J. Case Rep. 2022, 23, e936146. [Google Scholar] [CrossRef]
- Paulis, G.; De Giorgio, G. Full Regression of Peyronie’s Disease Plaque Following Combined Antioxidant Treatment: A Three-Case Report. Antioxidants 2022, 11, 1661. [Google Scholar] [CrossRef]
- Paulis, G.; De Giorgio, G. Patients with Peyronie’s disease achieve complete plaque regression after multimodal treatment with antioxidants: A case series. J. Med. Case Rep. 2022, 16, 359. [Google Scholar] [CrossRef]
- Kwon, K.-D.; Choi, M.J.; Park, J.-M.; Song, K.-M.; Kwon, M.-H.; Batbold, D.; Yin, G.N.; Kim, W.J.; Ryu, J.-K.; Suh, J.-K. Silencing histone deacetylase 2 using small hairpin RNA induces regression of fibrotic plaque in a rat model of Peyronie’s disease. BJU Int. 2014, 114, 926–936. [Google Scholar] [CrossRef]
- Búfalo, M.C.; Ferreira, I.; Costa, G.; Francisco, V.; Liberal, J.; Cruz, M.T.; Lopes, M.C.; Batista, M.T.; Sforcin, J.M. Propolis and its constituent caffeic acid suppress LPS-stimulated pro-inflammatory response by blocking NF-κB and MAPK activation in macrophages. J. Ethnopharmacol. 2013, 149, 84–92. [Google Scholar] [CrossRef]
- Karlsen, A.; Paur, I.; Bøhn, S.K.; Sakhi, A.K.; Borge, G.I.; Serafini, M.; Erlund, I.; Laake, P.; Tonstad, S.; Blomhof, R. Bilberry juice modulates plasma concentration of NF-kappaB related inflammatory markers in subjects at increased risk of CVD. Eur. J. Nutr. 2010, 49, 345–355. [Google Scholar] [CrossRef]
- Zhang, D.-M.; Guo, Z.-X.; Zhao, Y.-L.; Wang, Q.-J.; Gao, Y.-S.; Yu, T.; Chen, Y.-K.; Chen, X.-M.; Wang, G.-Q. L-carnitine regulated Nrf2/Keap1 activation in vitro and in vivo and protected oxidized fish oil-induced inflammation response by inhibiting the NF-κB signaling pathway in Rhynchocypris lagowski Dybowski. Fish Shellfish Immunol. 2019, 93, 1100–1110. [Google Scholar] [CrossRef]
- Mohamed, H.A.; Said, R.S. Coenzyme Q10 attenuates inflammation and fibrosis implicated in radiation enteropathy through suppression of NF-kB/TGF-β/MMP-9 pathways. Int. Immunopharmacol. 2021, 92, 107347. [Google Scholar] [CrossRef]
- Tian, M.Y.; Fan, J.H.; Zhuang, Z.W.; Dai, F.; Wang, C.Y.; Hou, H.T.; Ma, Y.Z. Effects of silymarin on p65 NF-κB, p38 MAPK and CYP450 in LPS-induced hoof dermal inflammatory cells of dairy cows. BMC Vet. Res. 2019, 15, 127. [Google Scholar]
- Wang, Y.; Wang, R.; Wang, Y.; Peng, R.; Wu, Y.; Yuan, Y. Ginkgo biloba extract mitigates liver fibrosis and apoptosis by regulating p38 MAPK, NF-κB/IκBα, and Bcl-2/Bax signaling. Drug Des. Devel. Ther. 2015, 9, 6303–6317. [Google Scholar]
- Ji, Q.; Zhang, L.; Jia, H.; Xu, J. Pentoxifylline inhibits endotoxin-induced NF-kappa B activation and associated production of proinflammatory cytokines. Ann. Clin. Lab. Sci. 2004, 34, 427–436. [Google Scholar]
- Tang, Y.Z.; Liu, Z.Q. Evaluation of the free-radical-scavenging activity of diclofenac acid on the free-radical-induced haemolysis of human erythrocytes. J. Pharm. Pharmacol. 2006, 58, 625–631. [Google Scholar] [CrossRef]
- Radermacher, J.; Jentsch, D.; Scholl, M.A.; Lustinetz, T.; Frolich, J.C. Diclofenac concentrations in synovial fluid and plasma after cutaneous application in inflammatory and degenerative joint disease. Br. J. Clin. Pharmacol. 1991, 31, 537–541. [Google Scholar] [CrossRef]
- McCauley, J.F.; Dean, R.C. Diagnostic utility of penile ultrasound in Peyronie’s disease. World J. Urol. 2020, 38, 263–268. [Google Scholar] [CrossRef]
- Parmar, M.; Masterson, J.M.; Masterson, T.A. 3rd. The role of imaging in the diagnosis and management of Peyronie’s disease. Curr. Opin Urol. 2020, 30, 283–289. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Patient Age | Associated Disease | Penile Plaque Site | Ultrasound Measurements (Length × Width × Thickness) and Plaque Volume before (A) and after Treatment (B) | Type of Deformity Initial (A) and after Treatment (B) | Pain Score/VAS Scale (1–10) | IIEF Score before and after Treatment | Total Duration of Treatment until Plaque Regression | Complete Combined Multimodal Treatment |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 31 years | Chronic prostatitis and associated anxious and depressive state. | Distal third | (A) 15.1 × 12.1 × 3.7 mm volume = 353 mm3 (B) No plaque detected | (A) 10-degree ventral curvature + 15-degree left curvature (B) None | VAS score = 8 Pain disappeared after 12 months | 26 > 27 | 30 months | Orally: propolis 600 mg + bilberry 160 mg + silymarin 400 mg + ginkgo biloba 250 mg + L-carnitine 1000 mg + coenzyme Q10 100 mg + Boswellia 200 mg + Vitamin E 30 mg/daily/for 30 months + topically: diclofenac gel 4%/2× daily for 30 months Note: The patient refused periplaque penile injections with pentoxifylline |
| 2 | 52 years | Dupuytren’s disease, Ledderhose disease, congenital dorsal penile curvature (5 degrees). | Middle third + distal third | (A) First plaque: 13.4 × 9.15 × 2.83 mm volume = 182 mm3. Second plaque: 14.8 × 8.43 × 3.87 mm. Total volume = 252 mm3 (B) No plaque detected | (A) 20-degree dorsal penile curvature + 20-degree left penile curvature (B) 5-degree dorsal penile curvature. Previous condition = congenital dorsal penile curvature (5 degrees) | VAS score = 0 | 26 > 27 | 51 months | Orally: propolis 600 mg + bilberry 160 mg + silymarin 400 mg + ginkgo biloba 250 mg + L-carnitine 1000 mg + coenzyme Q10 100 mg + Boswellia 200 mg + vitamin E 30 mg/daily for 51 months + topically: diclofenac gel 4%/2× daily for 51 months + periplaque penile injections: pentoxifylline 100 mg (30 G needle) every 2 weeks for 6 months, and then 1 penile injection every month for 12 months, and 1 penile injection every 2 months for 24 months (42 total injections) |
| 3 | 30 years | Left varicocele | Proximal third | (A) 12.2 × 11.2 × 2.81 mm volume = 203 mm3 (B) No plaque detected | (A) No penile deformation (B) No penile deformation | VAS score = 5 Pain disappeared after 4 months | 26 > 26 | 4 months | Orally: propolis 600 mg + bilberry 160 mg + silymarin 400 mg + ginkgo biloba 250 mg + vitamin E 800 IU/daily for 4 months + topically: diclofenac gel 4%/2× daily for 4 months Note: Penile injections not needed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paulis, G.; De Giorgio, G. Disappearance of Plaque Following Treatment with Antioxidants in Peyronie’s Disease Patients—A Report of 3 Cases. Clin. Pract. 2022, 12, 1020-1033. https://doi.org/10.3390/clinpract12060105
Paulis G, De Giorgio G. Disappearance of Plaque Following Treatment with Antioxidants in Peyronie’s Disease Patients—A Report of 3 Cases. Clinics and Practice. 2022; 12(6):1020-1033. https://doi.org/10.3390/clinpract12060105
Chicago/Turabian StylePaulis, Gianni, and Giovanni De Giorgio. 2022. "Disappearance of Plaque Following Treatment with Antioxidants in Peyronie’s Disease Patients—A Report of 3 Cases" Clinics and Practice 12, no. 6: 1020-1033. https://doi.org/10.3390/clinpract12060105
APA StylePaulis, G., & De Giorgio, G. (2022). Disappearance of Plaque Following Treatment with Antioxidants in Peyronie’s Disease Patients—A Report of 3 Cases. Clinics and Practice, 12(6), 1020-1033. https://doi.org/10.3390/clinpract12060105