
Hematopoietic Stem Cell Transplantation Impact on Patients’ Perceived Quality of Life: A Longitudinal Study


 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Variables
2.3. Data Collection Instruments
2.4. Data Analysis
3. Results
Population Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Conflicts of Interest
References
- Balassa, K.; Danby, R.; Rocha, V. Haematopoietic stem cell transplants: Principles and indications. Br. J. Hosp. Med. 2019, 80, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Godino, C.; Scotti, A.; Marengo, A.; Battini, I.; Brambilla, P.; Stucchi, S.; Slavich, M.; Salerno, A.; Fragasso, G.; Margonato, A. Effectiveness and cost-efficacy of diuretics home administration via peripherally inserted central venous catheter in patients with end-stage heart failure. Int. J. Cardiol. 2022, 365, 69–77. [Google Scholar] [CrossRef]
- World Health Organization. International Agency for Research on Cancer (IARC), Globocan 2012. Available online: https://www.iarc.fr/ (accessed on 24 March 2022).
- Von Ah, D.; Spath, M.; Nielsen, A.; Fife, B. The Caregiver’s Role Across the Bone Marrow Transplantation Trajectory. Cancer Nurs. 2016, 39, E12–E19. [Google Scholar] [CrossRef] [PubMed]
- Rifón, J.J. Transplant of hemopoietic progenitors. An. Sist. Sanit. Navar. 2006, 29, 137–151. [Google Scholar] [CrossRef] [PubMed]
- Ascensión, B. Pilar Moreno Psychosocial risks and psychological intervention in the transplanted bone marrow patients. Psicooncologia 2009, 6, 65–81. [Google Scholar]
- Ochoa-Fernández, B.; Galán-Gómez, V.; Mestre, C.; González-Vicent, M.; Pascual, A.; Alonso, L.; Regueiro, A.; Plaza, M.; Hurtado, J.M.P.; Benito, A.; et al. Haploidentical hematopoietic stem cell transplantation in pediatric and adolescent patients: A study of the Spanish hematopoietic stem cell transplantation group (GETH). Bone Marrow Transplant. 2022, 159, 411–419. [Google Scholar] [CrossRef]
- Jiménez-Ubieto, A.; Grande, C.; Caballero, D.; Yáñez, L.; Novelli, S.; Hernández-Garcia, M.T.; Manzanares, M.; Arranz, R.; Ferreiro, J.J.; Bobillo, S.; et al. Autologous stem cell transplantation may be curative for patients with follicular lymphoma with early therapy failure without the need for immunotherapy. Hematol. Stem Cell Ther. 2019, 12, 194–203. [Google Scholar] [CrossRef]
- Murthy, G.S.G.; Mehta, P.; Jethava, Y.; Dhakal, I.; Makhoul, I. Trends in hospitalization outcomes of elderly patients undergoing allogeneic stem cell transplantation for acute myeloid leukemia/myelodysplastic syndrome (AML/MDS). J. Clin. Oncol. 2014, 32, 7044. [Google Scholar] [CrossRef]
- Torrent, A.; Ferrá, C.; Batlle, M.; Hidalgo, F.; Jiménez-Lorenzo, M.-J.; Ribera, J.-M. Prospective follow-up of adult long-term survivors of allogeneic haematopoietic stem cell transplantation. Med. Clín. 2020, 157, 281–284. [Google Scholar] [CrossRef]
- Peters, W.P.; Ross, M.; Vredenburgh, J.J.; Meisenberg, B.; Marks, L.B.; Winer, E.; Kurtzberg, J.; Bast, R.C., Jr.; Jones, R.; Shpall, E. High-dose chemotherapy and autologous bone marrow support as consolidation after standard-dose adjuvant therapy for high-risk primary breast cancer. J. Clin. Oncol. 1993, 11, 1132–1143. [Google Scholar] [CrossRef]
- Bergkvist, K.; Fossum, B.; Johansson, U.-B.; Mattsson, J.; Larsen, J. Patients’ experiences of different care settings and a new life situation after allogeneic haematopoietic stem cell transplantation. Eur. J. Cancer Care 2017, 27, e12672. [Google Scholar] [CrossRef] [PubMed]
- Kharfan-Dabaja, M.A.; Roy, V.; Murthy, H.; Fischer, D.; Mohty, R.; Greathouse, A.; Brown, A.; Moreno, K.; Godsey, E.; Higginbotham, J.M.; et al. Post autologous hematopoietic cell transplant care in the “home sweet home” setting: A treatment paradigm shift. Hematol. Stem Cell Ther. 2023, 16, 16–411. [Google Scholar] [CrossRef] [PubMed]
- Barba, P.; Elorza, I. Allogeneic stem cell transplantation in the era of novel therapies for acute lymphoblastic leukaemia. Med. Clín. 2019, 153, 28–34. [Google Scholar] [CrossRef]
- Detrait, M.; De Berranger, E.; Dulery, R.; Ménard, A.-L.; Thépot, S.; Toprak, S.K.; Turlure, P.; Yakoub-Agha, I.; Guillaume, T. Complications hépatobiliaires dans le contexte de l’allogreffe de cellules hématopoïétiques: Recommandations de la Société francophone de greffe de moelle et de thérapie cellulaire (SFGM-TC). Bull. Cancer 2020, 107, S18–S27. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wang, J.; Liu, Y.; Liu, J.; Wang, B.; Zhang, Q.; Guan, W.; Zhang, H.; Xu, L.; Liu, G.; et al. Long-term survivors demonstrate superior quality of life after haploidentical stem cell transplantation to matched sibling donor transplantation. J. Transl. Med. 2022, 20, 1–12. [Google Scholar] [CrossRef]
- Janicsák, H.; Ungvari, G.S.; Gazdag, G. Psychosocial aspects of hematopoietic stem cell transplantation. World J. Transplant. 2021, 11, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, D.; Khera, N. Psychosocial and financial issues after hematopoietic cell transplantation. Hematology 2021, 2021, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Mathanda, R.R.; Hamilton, B.K.; Rybicki, L.; Advani, A.S.; Colver, A.; Dabney, J.; Ferraro, C.; Hanna, R.; Kalaycio, M.; Lawrence, C.; et al. Quality-of-Life Trajectories in Adolescent and Young Adult versus Older Adult Allogeneic Hematopoietic Cell Transplantation Recipients. Biol. Blood Marrow Transplant. 2020, 26, 1505–1510. [Google Scholar] [CrossRef]
- Rocha, V.d.; Proença, S.d.F.F.S.; Marques, A.d.C.B.; Pontes, L.; Mantovani, M.d.F.; Kalinke, L.P. Social impairment of patients undergoing hematopoietic stem cell transplant. Rev. Bras. Enferm. 2016, 69, 484–491. [Google Scholar] [CrossRef]
- Young, L. The family experience following bone marrow or blood cell transplantation. J. Adv. Nurs. 2013, 69, 2274–2284. [Google Scholar] [CrossRef]
- Bryant, A.L.; Drier, S.W.; Lee, S.; Bennett, A.V. A systematic review of patient reported outcomes in phase II or III clinical trials of myelodysplastic syndromes and acute myeloid leukemia. Leuk. Res. 2018, 70, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Jim, H.S.L.; Quinn, G.P.; Barata, A.; Cases, M.; Cessna, J.; Gonzalez, B.; Gonzalez, L.; Koskan, A.; Montiel-Ishino, F.; Pidala, J. Caregivers’ quality of life after blood and marrow transplantation: A qualitative study. Bone Marrow Transplant. 2014, 49, 1234–1236. [Google Scholar] [CrossRef]
- Gifford, G.; Sim, J.; Horne, A.; Ma, D. Health status, late effects and long-term survivorship of allogeneic bone marrow transplantation: A retrospective study. Intern. Med. J. 2013, 44, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Avilés, F.; Carreras, E.; Urbano-Ispizua, A.; Rovira, M.; Martínez, C.; Gaya, A.; Granell, M.; Ramiro, L.; Gallego, C.; Hernando, A.; et al. Case-Control Comparison of At-Home to Total Hospital Care for Autologous Stem-Cell Transplantation for Hematologic Malignancies. J. Clin. Oncol. 2006, 24, 4855–4861. [Google Scholar] [CrossRef] [PubMed]
- Dunavin, N.; Mau, L.-W.; Meyer, C.L.; Divine, C.; Abdallah, A.-O.; Leppke, S.; D’Souza, A.; Denzen, E.; Saber, W.; Burns, L.J.; et al. Health Care Reimbursement, Service Utilization, and Outcomes among Medicare Beneficiaries with Multiple Myeloma Receiving Autologous Hematopoietic Cell Transplantation in Inpatient and Outpatient Settings. Biol. Blood Marrow Transplant. 2020, 26, 805–813. [Google Scholar] [CrossRef]
- Martino, M.; Ciavarella, S.; De Summa, S.; Russo, L.; Meliambro, N.; Imbalzano, L.; Gallo, G.A.; Moscato, T.; Messina, G.; Ferreri, A.; et al. A Comparative Assessment of Quality of Life in Patients with Multiple Myeloma Undergoing Autologous Stem Cell Transplantation Through an Outpatient and Inpatient Model. Biol. Blood Marrow Transplant. 2018, 24, 608–613. [Google Scholar] [CrossRef]
- Murthy, G.S.G.; Hari, P.N.; Szabo, A.; Pasquini, M.; Narra, R.; Khan, M.; Abedin, S.; Chhabra, S.; Dhakal, B.; D’Souza, A.; et al. Outcomes of Reduced-Intensity Conditioning Allogeneic Hematopoietic Cell Transplantation Performed in the Inpatient versus Outpatient Setting. Biol. Blood Marrow Transplant. 2018, 25, 827–833. [Google Scholar] [CrossRef]
- Gutiérrez-García, G.; Rovira, M.; Arab, N.; Gallego, C.; Sánchez, J.; Álvarez, M.; Ayora, P.; Domenech, A.; Borràs, N.; Rodríguez-Lobato, L.G.; et al. A reproducible and safe at-home allogeneic haematopoietic cell transplant program: First experience in Central and Southern Europe. Bone Marrow Transplant. 2020, 55, 965–973. [Google Scholar] [CrossRef]
- Seixas, M.R.; Rodríguez, L.L.; Fernández, J.M.P.; Moncada, M.V.; Quijano-Campos, J.C. Quality of life related to health in patients with hematopoietic stem cell transplantation. Index Enferm. 2014, 23, 209–213. [Google Scholar] [CrossRef]
- Sorror, M.L.; Maris, M.B.; Storb, R.; Baron, F.; Sandmaier, B.M.; Maloney, D.G.; Storer, B. Hematopoietic cell transplantation (HCT)-specific comorbidity index: A new tool for risk assessment before allogeneic HCT. Blood 2005, 106, 2912–2919. [Google Scholar] [CrossRef]
- Cella, D.; Hernandez, L.; Bonomi, A.E.; Corona, M.; Vaquero, M.; Shiomoto, G.; Baez, L. Spanish Language Translation and Initial Validation of the Functional Assessment of Cancer Therapy Quality-of-Life Instrument. Med. Care 1998, 36, 1407–1418. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.; Cella, D.; Yost, K. The Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System: Properties, applications, and interpretation. Health Qual. Life Outcomes 2003, 1, 79. [Google Scholar] [CrossRef] [PubMed]
- Montan, I.; Löwe, B.; Cella, D.; Mehnert, A.; Hinz, A. General Population Norms for the Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue Scale. Value Health 2018, 21, 1313–1321. [Google Scholar] [CrossRef]
- Marques, A.d.C.B.; Szczepanik, A.P.; Machado, C.A.M.; Santos, P.N.D.; Guimarães, P.R.B.; Kalinke, L.P. Hematopoietic stem cell transplantation and quality of life during the first year of treatment. Rev. Latino-Am. Enferm. 2018, 26, e3065. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, C.L.T.; Sawada, N.O.; dos Santos, J.L.F. Evaluation of the health-related quality of life of hematopoietic stem cell transplantation patients. Rev. Latino-Am. Enferm. 2011, 19, 1322–1328. [Google Scholar] [CrossRef]
- D’Souza, A.; Brazauskas, R.; Stadtmauer, E.A.; Pasquini, M.C.; Hari, P.; Bashey, A.; Callander, N.; Devine, S.; Efebera, Y.; Ganguly, S.; et al. Trajectories of quality of life recovery and symptom burden after autologous hematopoietic cell transplantation in multiple myeloma. Am. J. Hematol. 2022, 98, 140–147. [Google Scholar] [CrossRef]
- Ovayolu, O.; Ovayolu, N.; Kaplan, E.; Pehlivan, M.; Karadağ, G. Symptoms and Quality of Life: Before and after stem cell transplantation in cancer. Pak. J. Med Sci. 2013, 29, 803–808. [Google Scholar] [CrossRef]
- Kenzik, K.; Huang, I.-C.; Rizzo, J.D.; Shenkman, E.; Wingard, J. Relationships among symptoms, psychosocial factors, and health-related quality of life in hematopoietic stem cell transplant survivors. Support. Care Cancer 2014, 23, 797–807. [Google Scholar] [CrossRef]
- Tay, J.; Beattie, S.; Bredeson, C.; Brazauskas, R.; He, N.; Ahmed, I.A.; Aljurf, M.; Askar, M.; Atsuta, Y.; Badawy, S.; et al. Pre-Transplant Marital Status and Hematopoietic Cell Transplantation Outcomes. Curr. Oncol. 2020, 27, 596–606. [Google Scholar] [CrossRef]
- Gomà, A.S.; Peris, P.A.; Alcario, A.B.R. Calidad de vida en pacientes con insuficiencia renal crónica en tratamiento con diálisis. Rev. Soc. Esp. Enferm. Nefrol. 2010, 13, 155–160. [Google Scholar] [CrossRef]
- Vivaldi, F.; Barra, E. Psychological Well-Being, Perceived Social Support and Health Perception Among Older Adults. Ter. Psicol. 2012, 30, 23–29. [Google Scholar] [CrossRef]
- Alfonso Figueroa, L.; Soto Carballo, D.; Santos Fernández, N.A. Calidad de vida y apoyo social percibido en adultos mayores. Rev. Cienc. Méd. 2016, 20. [Google Scholar]
- Rodrigue, J.R.; Hoffmann, R.G.; Macnaughton, K.; Graham-Pole, J.; Andres, J.M.; A Novak, D.; Fennell, R.S. Mothers of children evaluated for transplantation: Stress, coping resources, and perceptions of family functioning. Clin. Transplant. 1996, 10, 447–450. [Google Scholar]
- Wochna, V. Anxiety, needs, and coping in family members of the bone marrow transplant patient. Cancer Nurs. 1997, 20, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, T.C.; de Carvalho, E.C.; Canini, S.R.M.d.S.; Sawada, N.O. Family crisis in the context of bone marrow transplantation: An integrative review. Rev. Latino-Am. Enferm. 2007, 15, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Z.M.; Nash, R.P.; Quillen, L.J.; Richardson, D.R.; McCall, R.C.; Park, E.M. Psychiatric Care in Hematopoietic Stem Cell Transplantation. Psychosomatics 2019, 60, 227–237. [Google Scholar] [CrossRef]
- El-Jawahri, A.; Chen, Y.; Brazauskas, R.; He, N.; Lee, S.J.; Knight, J.M.; Majhail, N.; Buchbinder, D.; Schears, R.M.; Wirk, B.M.; et al. Impact of pre-transplant depression on outcomes of allogeneic and autologous hematopoietic stem cell transplantation. Cancer 2017, 123, 1828–1838. [Google Scholar] [CrossRef]
- Sancho, J.M.; Ribera, J.M.; Oriol, A.; Batlle, M.; Flores, A.; Rodríguez, L.; Torrabadella, M.; Millá, F.; Feliu, E. Reasons for not carrying out stem cell transplantation in patients referred to a transplant unit. Med. Clín. 2003, 121, 401–404. [Google Scholar] [CrossRef]
- Fundación Josep Carreras Memoria Anual REDMO Fundación Carreras. Fundación Josep Carreras Contra la Leucemia 2023. pp. 1–72. Available online: https://www.fcarreras.org/es/MemoriaREDMO_2022 (accessed on 23 November 2023).
- Organización Nacional de Trasplantes. Balance de Actividad de Donación y Trasplante en España. 2023. Available online: https://www.ont.es/2023/02/10/balanceont20230117-3/ (accessed on 23 November 2023).
- Garcés-Carrasco, A.M.; Santacatalina-Roig, E.; Carretero-Márquez, C.; Chover-Sierra, E.; Martínez-Sabater, A.; Balaguer-López, E. Post-Transplant Complications in Patients Undergoing Autologous Hematopoietic Cell Transplantation (HCT)—A Comparative Analysis of Home Care versus Hospitalized Patients. Medicina 2023, 60, 44. [Google Scholar] [CrossRef]

{kind=link}
| Hospitalization | 24 M | |
|---|---|---|
| Variables | n = 121 (%) | n = 39 (%) |
| Sociodemographic | ||
| Age | ||
| 18–30 years | 12 (9.92%) | 4 (10.25%) |
| 31–50 years | 28 (23.14%) | 10 (25.64%) |
| 51–70 years | 74 (61.16%) | 23 (58.97%) |
| More than 70 years | 7 (5.78%) | 2 (5.13%) |
| Gender | ||
| Male | 72 (59.5%) | 27 (69.23%) |
| Female | 49 (40.5%) | 12 (30.77%) |
| Marital status | ||
| Single | 27 (22.31%) | 9 (23.07%) |
| Married/Consensual Union | 76 (62.8%) | 23 (59.97%) |
| Separated | 7 (5.87%) | 5 (12.82%) |
| Widowed | 4 (3.30%) | 1 (2.56%) |
| Family network | ||
| One relative | 14 (11.57%) | 6 (15.38%) |
| Two relatives | 34 (28.1%) | 13 (33.33%) |
| Three or more relatives | 49 (40.5%) | 17 (43.59%) |
| Educational level | ||
| Uneducated | 2 (1.65%) | |
| Primary | 56 (46.28%) | 18 (46.15%) |
| Secondary | 25 (20.66%) | 10 (25.64%) |
| University | 24 (19.83%) | 8 (20.51%) |
| Occupation | ||
| Unqualified | 47 (38.84%) | 9 (23.07%) |
| Qualified | 23 (19%) | 14 (35.90%) |
| Professionals | 6 (4.95%) | 2 (5.13%) |
| Civil servant | 12 (9.92%) | 4 (10.25%) |
| Self-employed | 12 (9.92%) | 3 (7.69%) |
| Student | 5 (4.13%) | 2 (5.13%) |
| Economic income (euros/year) | ||
| <18,000 | 60 (49.59%) | 15 (38.46%) |
| 18,000–22,000 | 7 (5.78%) | 2 (5.13%) |
| 22,000–60,000 | 32 (26.45%) | 17 (43.59%) |
| 60,000–90,000 | 7 (5.78%) | 1 (2.56%) |
| Distance to Hospital (km) | ||
| 0–50 | 48 (39.67%) | 18 (46.15%) |
| 50–100 | 15 (12.39%) | 6 (15.38%) |
| >100 | 37 (30.58%) | 10 (25.64%) |
| Clinicals | ||
| KPS | ||
| <70 | 1 (0.82%) | |
| 70 | 4 (3.30%) | |
| 80 | 14 (11.57%) | 2 (1.65%) |
| 90 | 86 (71.07%) | 33 (27.27%) |
| 100 | 4 (3.30%) | 1 (2.56%) |
| Sorror score | ||
| 0 | 20 (16.53%) | 8 (20.51%) |
| 1 | 9 (7.44%) | 3 (7.69%) |
| 2 | 25 (20.66%) | 10 (25.64%) |
| 3 | 24 (19.83%) | 6 (15.38%) |
| 4 | 18 (14.87%) | 5 (12.82%) |
| 5 | 7 (5.78%) | 2 (5.13%) |
| 6 | 3 (2.48%) | 1 (2.56%) |
| 7 | 2 (1.65%) | |
| Diagnosis 1 | ||
| ALL | 3 (2.48%) | 1 (2.56%) |
| AML | 19 (15.70%) | 5 (12.82%) |
| CLL | 1 (0.82%) | |
| CML | 1 (0.82%) | |
| MDS | 9 (7.42%) | 3 (7.69%) |
| Lymphoma | 52 (42.97%) | 21 (53.84%) |
| Multiple myeloma | 30 (27.79%) | 8 (20.51%) |
| Amyloidosis | 1 (0.82%) | |
| Myelofibrosis | 4 (3.30%) | 1 (2.56%) |
| Embryonal cancer | 1 (0.82%) | |
| Type of HSCT | ||
| Autologous | 71 (56.67%) | 24 (61.54%) |
| Allogeneic | 29 (23.96%) | 10 (25.64%) |
| Haploidentical | 21 (17.35%) | 4 (10.25%) |
| Stem cells’ source | ||
| Bone marrow | 1 (0.82%) | |
| Peripheral Blood | 113 (93.38%) | 39 (100%) |
| Conditioning | ||
| Myeloablative | 57 (47.10%) | 24 (61.54%) |
| Non-myeloablative | 41 (33.88%) | 11 (28.20%) |
| Study Stage 1 | ||||||
|---|---|---|---|---|---|---|
| Transplantation | Discharge | Three Months | Six Months | 12 Months | 24 Months | |
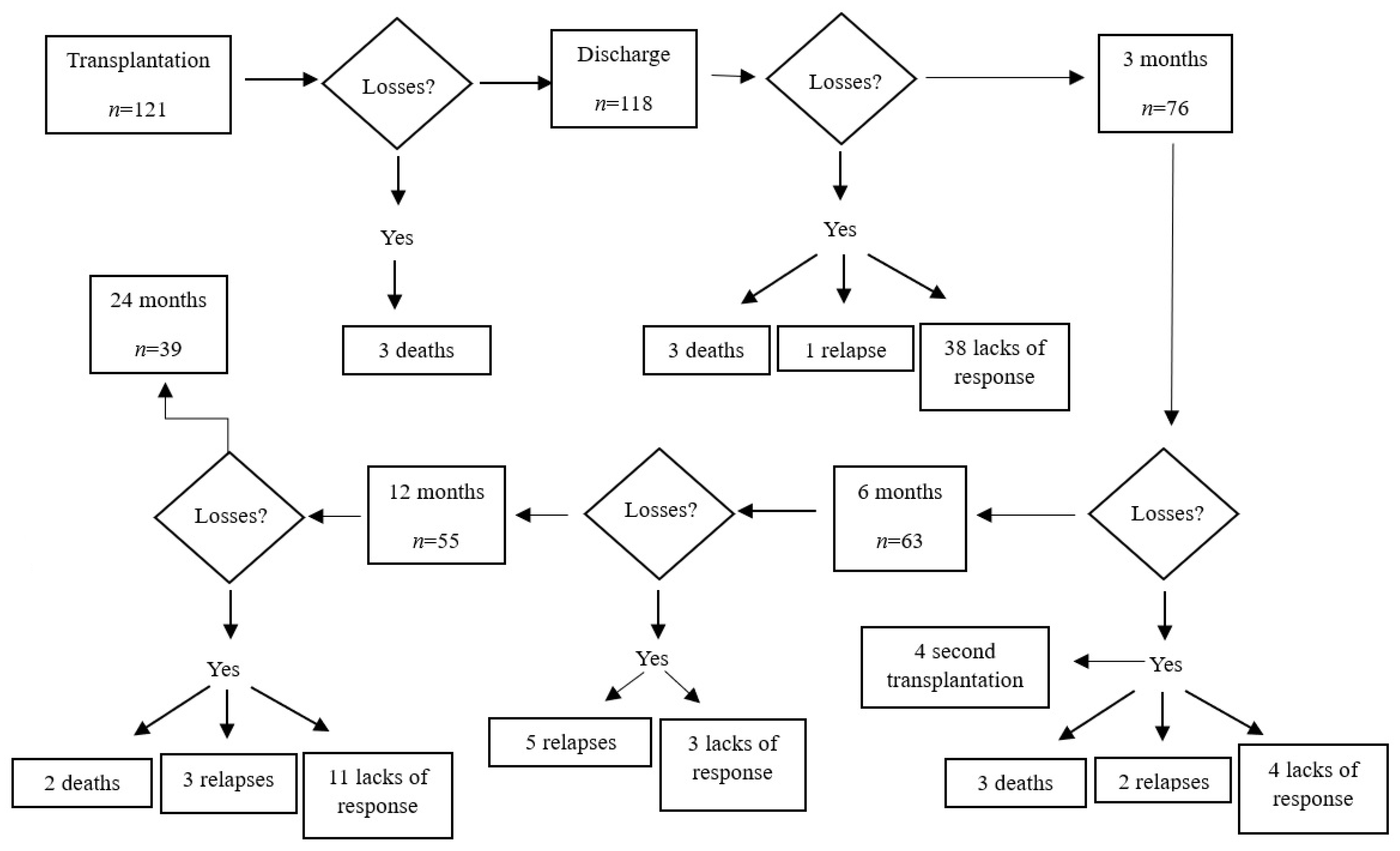
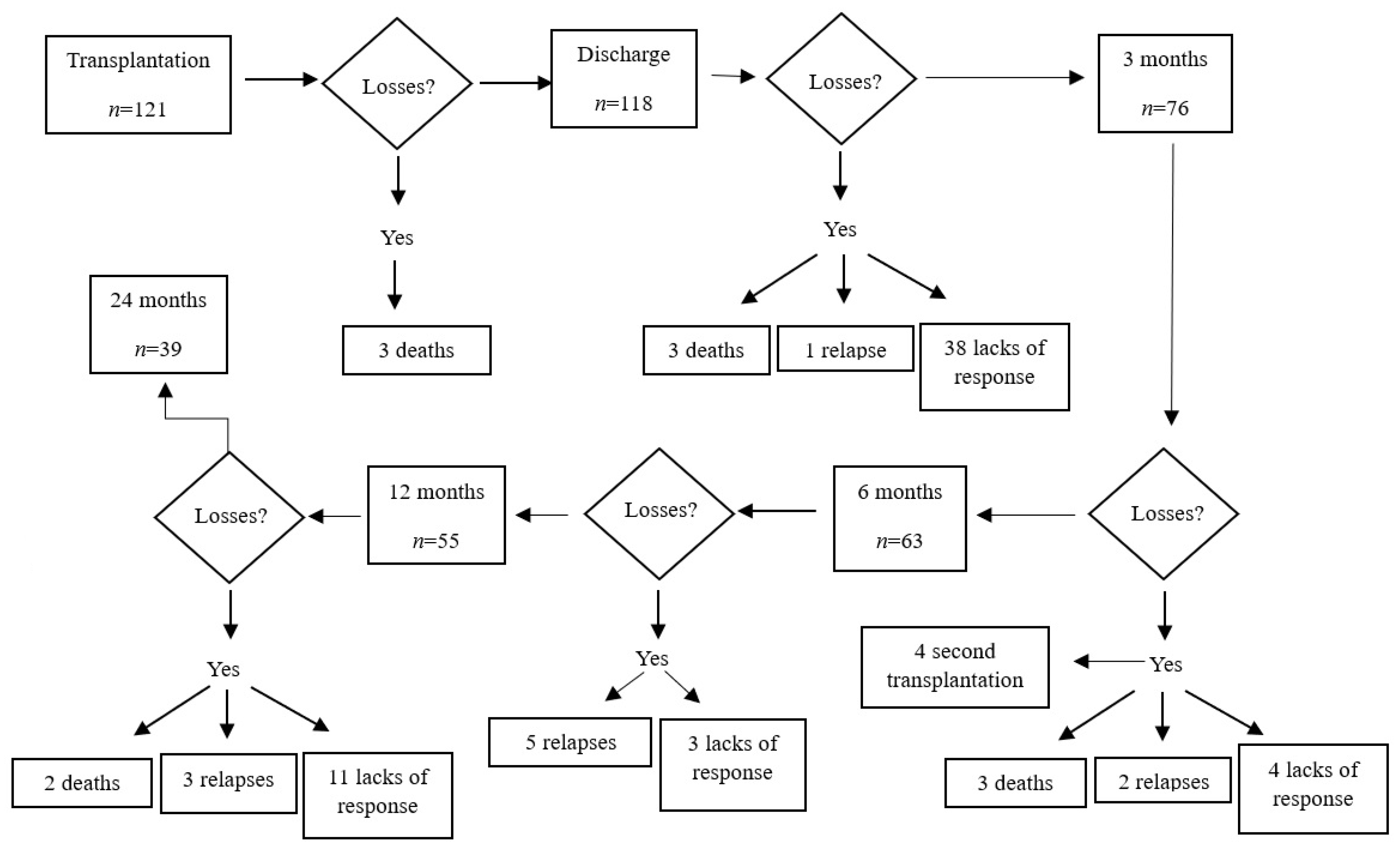
| n | 121 | 118 | 76 | 63 | 55 | 39 |
| FACT-BMT | 101.12 | 97.34 | 97.76 | 100.21 | 104.54 | 97.19 |
| FACT-G | 76.20 | 73.44 | 73.16 | 74.36 | 77.68 | 71.68 |
| FACT-TOI | 62.81 | 58.08 | 60.42 | 62.81 | 66.68 | 61.58 |
| Variable 1 | β | SD | Sig. |
|---|---|---|---|
| Age | 0.271 | 0.281 | p = 0.339 |
| Sex | −20.147 | 6.603 | <0.01 |
| Marital status | −8.789 | 4.305 | <0.015 |
| Cohabitation | 9.452 | 8.509 | p = 0.272 |
| Level of education | −0.303 | 4.435 | p = 0.946 |
| Occupation | 1.749 | 1.845 | p = 0.348 |
| Income | −4.065 | 3.748 | p = 0.284 |
| Diagnosis | 0.199 | 1.281 | p = 0.877 |
| Previous transplants | 4.600 | 6.680 | p = 0.494 |
| Family network | −3.133 | 3.284 | p = 0.345 |
| Type of transplantation | 2.388 | 3.835 | p = 0.536 |
| Marrow source | 0.782 | 21.232 | p = 0.971 |
| Functional Assessment of Cancer Therapy—Bone Marrow Transplantation (FACT-BMT) | ||||||
|---|---|---|---|---|---|---|
| Discharge | 3 M | 6 M | 12 M | 24 M | ||
| N | 118 | 76 | 63 | 55 | 39 | |
| Gender | ||||||
| Male | Average | 102.77 | 105.50 | 107.57 | 111.83 | 103.47 |
| SD 1 | 15.157 | 19.925 | 20.628 | 20.052 | 23.868 | |
| Female | Average | 89.43 | 86.76 | 89.02 | 91.055 | 84.02 |
| SD | 21.7 | 20.611 | 19.744 | 22.199 | 16.138 | |
| p-value | <0.001 | <0.001 | <0.01 | <0.001 | <0.05 | |
| Marital Status | ||||||
| Single | Average | 101.08 | 100.91 | 100.86 | 107.56 | 108.31 |
| SD | 22.094 | 22.140 | 22.115 | 19.377 | 26.010 | |
| Married/consensual union | Average | 98.06 | 97.18 | 101.90 | 107.66 | 98.43 |
| SD | 18.167 | 23.077 | 23.093 | 20.297 | 24.042 | |
| Separated | Average | 88.56 | 88.04 | 90.23 | 88.10 | 82.10 |
| SD | 5.978 | 18.671 | 11.726 | 24.089 | 11.749 | |
| Widowed | Average | 89.66 | 103.91 | 90.16 | 85 | 74.05 |
| SD | 28.479 | 22.745 | 30.641 | |||
| p-value | 0.214 | 0.601 | 0.591 | 0.186 | 0.262 | |
| Functional Assessment of Cancer Therapy—Trial Outcome Index (FACT-TOI) | ||||||
|---|---|---|---|---|---|---|
| Discharge | 3 M | 6 M | 12 M | 24 M | ||
| N | 118 | 76 | 63 | 55 | 39 | |
| Gender a | ||||||
| Male | Average | 62.05 | 66.53 | 68.30 | 72.01 | 66.88 |
| SD | 11.993 | 15.212 | 15.081 | 13.576 | 16.873 | |
| Female | Average | 52.29 | 51.74 | 54.46 | 56.82 | 50.44 |
| SD | 16.265 | 15.192 | 14.597 | 14.429 | 12.628 | |
| p-value | <0.001 | <0.001 | <0.01 | <0.001 | <0.05 | |
| Marital Status b | ||||||
| Single | Average | 61 | 63.58 | 65.33 | 70.49 | 72.03 |
| SD | 17.074 | 14.731 | 13.096 | 12.788 | 17.704 | |
| Married/consensual union | Average | 58.26 | 59.36 | 63.85 | 68.66 | 61.97 |
| SD | 14.019 | 18.086 | 18.065 | 14.428 | 17.780 | |
| Separated | Average | 53.49 | 55.28 | 53 | 51.8 | 48.40 |
| SD | 6.508 | 15.304 | 7.071 | 17.398 | 5.594 | |
| Widowed | Average | 52.5 | 69.5 | 51 | 52 | 46.25 |
| SD | 21.625 | 16.263 | 18.384 | |||
| p-value | 0.454 | 0.514 | 0.286 | 0.075 | 0.133 | |
| Functional Assessment of Cancer Therapy—General (FACT-G) | ||||||
|---|---|---|---|---|---|---|
| Discharge | 3 M | 6 M | 12 M | 24 M | ||
| N | 118 | 76 | 63 | 55 | 39 | |
| Gender a | ||||||
| Male | Average | 77.26 | 78.26 | 78.76 | 82.49 | 76.20 |
| SD | 11.186 | 14.382 | 16.706 | 15.022 | 17.987 | |
| Female | Average | 67.88 | 65.93 | 67.68 | 68.78 | 62.18 |
| SD | 16.286 | 15.037 | 14.713 | 15.377 | 12.217 | |
| p-value | <0.001 | <0.01 | <0.01 | <0.01 | <0.05 | |
| Marital Status b | ||||||
| Single | Average | 76.04 | 75.38 | 75.53 | 79.06 | 77.77 |
| SD | 16.085 | 16.382 | 16.686 | 13.348 | 20.640 | |
| Married/consensual union | Average | 74.21 | 72.95 | 74.89 | 79.94 | 73.07 |
| SD | 13.556 | 16.119 | 17.496 | 15.202 | 17.844 | |
| Separated | Average | 66.21 | 65.18 | 69.23 | 66.5 | 62.10 |
| SD | 4.368 | 13.432 | 11.983 | 18.580 | 11.227 | |
| Widowed | Average | 67.41 | 77.41 | 70.66 | 67 | 52.8 |
| SD | 18.125 | 17.795 | 22.863 | |||
| p-value | 0.136 | 0.474 | 0.805 | 0.358 | 0.320 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortolá-Alonso, P.; Santacatalina-Roig, E.; Chover-Sierra, E.; Merelles-Tormo, A.; Ballestar-Tarín, M.L.; Martínez-Sabater, A. Hematopoietic Stem Cell Transplantation Impact on Patients’ Perceived Quality of Life: A Longitudinal Study. Nurs. Rep. 2024, 14, 197-211. https://doi.org/10.3390/nursrep14010016
Ortolá-Alonso P, Santacatalina-Roig E, Chover-Sierra E, Merelles-Tormo A, Ballestar-Tarín ML, Martínez-Sabater A. Hematopoietic Stem Cell Transplantation Impact on Patients’ Perceived Quality of Life: A Longitudinal Study. Nursing Reports. 2024; 14(1):197-211. https://doi.org/10.3390/nursrep14010016
Chicago/Turabian StyleOrtolá-Alonso, Pablo, Enric Santacatalina-Roig, Elena Chover-Sierra, Antoni Merelles-Tormo, María Luisa Ballestar-Tarín, and Antonio Martínez-Sabater. 2024. "Hematopoietic Stem Cell Transplantation Impact on Patients’ Perceived Quality of Life: A Longitudinal Study" Nursing Reports 14, no. 1: 197-211. https://doi.org/10.3390/nursrep14010016
APA StyleOrtolá-Alonso, P., Santacatalina-Roig, E., Chover-Sierra, E., Merelles-Tormo, A., Ballestar-Tarín, M. L., & Martínez-Sabater, A. (2024). Hematopoietic Stem Cell Transplantation Impact on Patients’ Perceived Quality of Life: A Longitudinal Study. Nursing Reports, 14(1), 197-211. https://doi.org/10.3390/nursrep14010016