
Interrater Agreement between Bedside and Video Raters Using the CPOT-Neuro for Pain Assessment in Critically Ill Patients with a Brain Injury

Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample and Setting
2.3. Procedures
2.4. Instruments
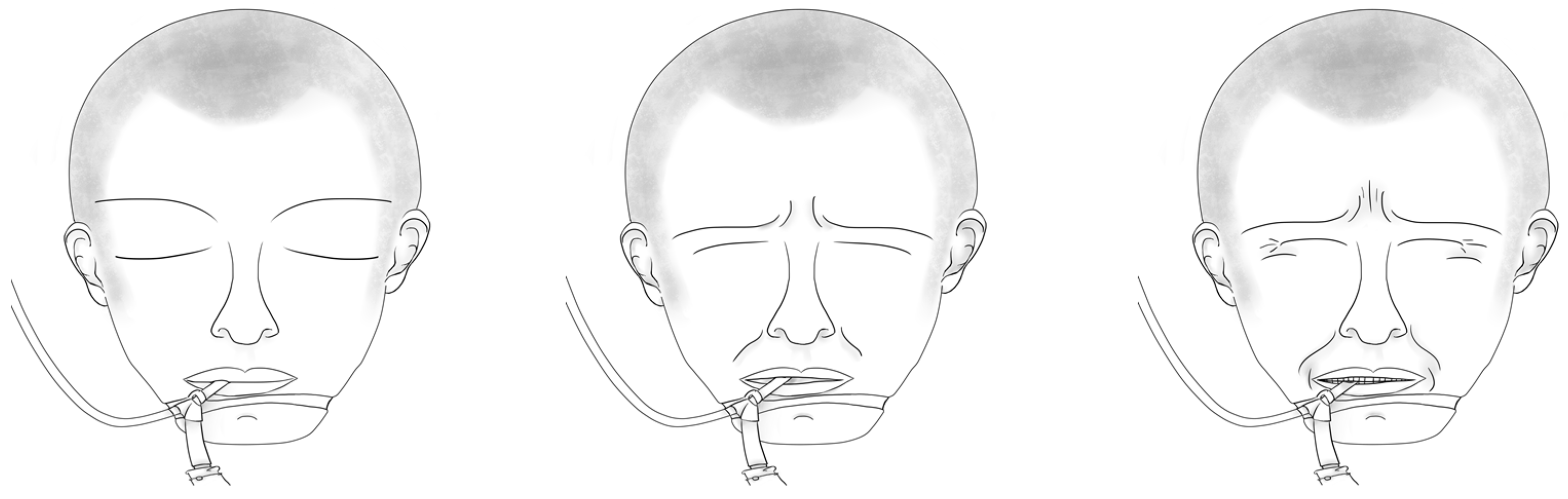
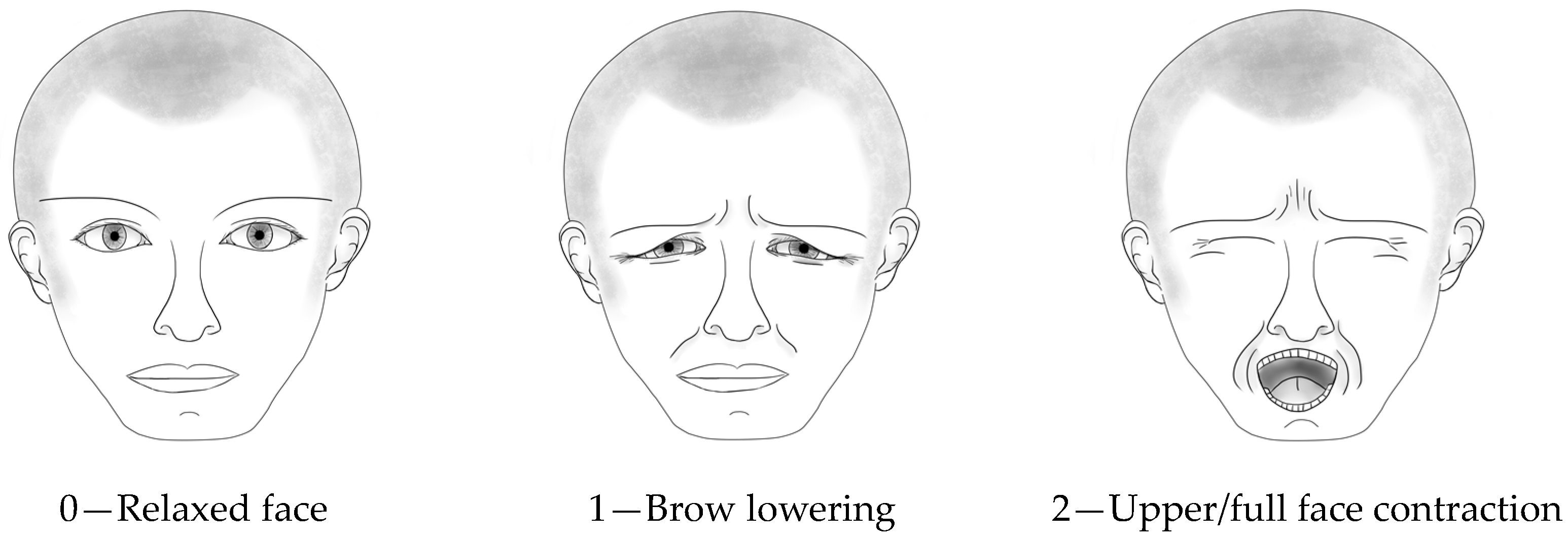
2.4.1. Critical-Care Pain Observation Tool–Neuro
2.4.2. Sociodemographic and Clinical Variables
2.4.3. Data Analysis
3. Results
3.1. Sample Description
3.2. CPOT-Neuro Scores of the Bedside and Video Raters
3.3. Interrater Agreement of CPOT-Neuro Scores between Pairs of Bedside and Video Raters
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Acknowledgments
Conflicts of Interest
References
- Roulin, M.J.; Ramelet, A.S. Generating and selecting pain indicators for brain-injured critical care patients. Pain. Manag. Nurs. 2015, 16, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Puntillo, K.A.; Max, A.; Timsit, J.F.; Vignoud, L.; Chanques, G.; Robleda, G.; Roche-Campo, F.; Mancebo, J.; Divatia, J.V.; Soares, M.; et al. Determinants of procedural pain intensity in the intensive care unit. The Europain(R) study. Am. J. Respir. Crit. Care Med. 2014, 189, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef]
- Herr, K.; Coyne, P.J.; Ely, E.; Gélinas, C.; Manworren, R.C.B. Pain assessment in the patient unable to self-report: Clinical practice recommendations in support of the ASPMN 2019 position statement. Pain Manag. Nurs. 2019, 20, 404–417. [Google Scholar] [CrossRef] [PubMed]
- Gélinas, C.; Joffe, A.M.; Szumita, P.M.; Payen, J.F.; Bérubé, M.; Shahiri, T.S.; Boitor, M.; Chanques, G.; Puntillo, K. A psychometric analysis update of behavioral pain assessment tools for noncommunicative, critically ill adults. AACN Adv. Crit. Care 2019, 30, 365–387. [Google Scholar] [CrossRef] [PubMed]
- Payen, J.F.; Bru, O.; Bosson, J.L.; Lagrasta, A.; Novel, E.; Deschaux, I.; Lavagne, P.; Jacquot, C. Assessing pain in critically ill sedated patients by using a behavioral pain scale. Crit. Care Med. 2001, 29, 2258–2263. [Google Scholar] [CrossRef]
- Gélinas, C.; Fillion, L.; Puntillo, K.A.; Viens, C.; Fortier, M. Validation of the Critical-Care Pain Observation Tool in adult patients. Am. J. Crit. Care 2006, 15, 420–427. [Google Scholar] [CrossRef]
- Gélinas, C.; Boitor, M.; Puntillo, K.A.; Arbour, C.; Topolovec-Vranic, J.; Cusimano, M.D.; Choiniere, M.; Streiner, D.L. Behaviors indicative of pain in brain-injured adult patients with different levels of consciousness in the intensive care unit. J. Pain. Symptom Manag. 2019, 57, 761–773. [Google Scholar] [CrossRef]
- Roulin, M.J.; Ramelet, A.S. Behavioral changes in brain-injured critical care adults with different levels of consciousness during nociceptive stimulation: An observational study. Intensive Care Med. 2014, 40, 1115–1123. [Google Scholar] [CrossRef]
- Gélinas, C.; Bérubé, M.; Puntillo, K.A.; Boitor, M.; Richard-Lalonde, M.; Bernard, F.; Williams, V.; Joffe, A.M.; Steiner, C.; Marsh, R.; et al. Validation of the Critical-Care Pain Observation Tool-Neuro in brain-injured adults in the intensive care unit: A prospective cohort study. Crit. Care 2021, 25, 142. [Google Scholar] [CrossRef]
- Kottner, J.; Audige, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hrobjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were proposed. Int. J. Nurs. Stud. 2011, 48, 661–671. [Google Scholar] [CrossRef]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Richard-Lalonde, M.; Bérubé, M.; Williams, V.; Bernard, F.; Tsoller, D.; Gélinas, C. Nurses’ Evaluations of the feasibility and clinical utility of the use of the Critical-Care Pain Observation Tool-Neuro in critically ill brain-injured patients. Sci. Nurs. Health Pract. 2019, 2, 1–18. [Google Scholar] [CrossRef]
- Prkachin, K.M. The consistency of facial expressions of pain: A comparison across modalities. Pain 1992, 51, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Solomon, P.E.; Prkachin, K.M.; Farewell, V. Enhancing sensitivity to facial expression of pain. Pain 1997, 71, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Teasdale, G.; Murray, G.; Parker, L.; Jennett, B. Adding up the Glasgow Coma Score. Acta Neurochir. Suppl. 1979, 28, 13–16. [Google Scholar] [CrossRef]
- Haidet, K.K.; Tate, J.; Divirgilio-Thomas, D.; Kolanowski, A.; Happ, M.B. Methods to improve reliability of video-recorded behavioral data. Res. Nurs. Health 2009, 32, 465–474. [Google Scholar] [CrossRef]
- Ammaturo, D.A.; Hadjistavropoulos, T.; Williams, J. Pain in Dementia: Use of Observational Pain Assessment Tools by People Who Are Not Health Professionals. Pain. Med. 2017, 18, 1895–1907. [Google Scholar] [CrossRef]
- Kaasa, T.; Wessel, J.; Darrah, J.; Bruera, E. Inter-rater reliability of formally trained and self-trained raters using the Edmonton Functional Assessment Tool. Palliat. Med. 2000, 14, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales—A Practical Guide to Their Development and Use, 5th ed.; Oxford University Press: New York, NY, USA, 2015; pp. 159–199. [Google Scholar]

{kind=link}
{kind=link}
| Conscious (n = 31) | Altered LOC (n = 17) | Unconscious (n = 8) | Total (n = 56) | |
|---|---|---|---|---|
| Male sex: n (%) | 17 (55%) | 13 (77%) | 7 (88%) | 37 (66%) |
| Age: median (IQR) | 61 (34–79) | 60 (28–74) | 45.5 (26.5–54.5) | 57.5 (33.25–75.5) |
| Ethnicity: n (%) | ||||
| Caucasian | 24 (77%) | 13 (76%) | 5 (63%) | 42 (75%) |
| Asian | 2 (7%) | 2 (12%) | 0 | 4 (7%) |
| Black | 3 (10%) | 0 | 0 | 3 (5%) |
| Hispanic | 1 (3%) | 0 | 2 (25%) | 3 (5%) |
| Other | 1 (3%) | 2 (12%) | 1 (12%) | 4 (7%) |
| Diagnosis: n (%) | ||||
| TBI | 24 (77%) | 13 (77%) | 7 (88%) | 44 (79%) |
| Non-TBI | 7 (23%) | 4 (23%) | 1 (12%) | 12 (21%) |
| Mechanical ventilation: n (%) | 12 (39%) | 16 (94%) | 7 (88%) | 35 (63%) |
| APACHE: median (IQR) | 13 (9–16) | 16 (11.5–20.5) | 15.5 (10.25–27.5) | 14 (9–17.75) |
| Procedure | Rater | Conscious (n = 31) | Altered LOC (n = 17) | Unconscious (n = 8) | Total (n = 56) |
|---|---|---|---|---|---|
| NIBP | Bedside | 0 (0–1) | 0 (0–0.5) | 1 (0–2.75) | 0 (0–1.75) |
| VR1 | 0 (0–1) | 0 (0–0) | 0.5 (0–1) | 0 (0–1) | |
| VR2 | 0 (0–1) | 0 (0–0) | 0.5 (0–2.75) | 0 (0–1) | |
| Turning | Bedside | 3 (1–4) | 2 (0–3.5) | 3.5 (2–4) | 3 (1–4) |
| VR1 | 2 (0–4) | 2 (0.5–3) | 1.5 (1–2) | 2 (1–3) | |
| VR2 | 3 (2–4) | 3 (1.5–4) | 4 (3–4) | 3 (2–4) |
| Procedure | Pairs of Raters | Conscious (n = 31) | Altered LOC (n = 17) | Unconscious (n = 8) | Total (n = 56) |
|---|---|---|---|---|---|
| NIBP | Bedside—VR1 | 0.73 (0.50–0.86) | 0.44 (0.04–0.75) | 0.62 (0.08–0.91) | 0.68 (0.50–0.80) |
| Bedside—VR2 * | 0.63 (0.26–0.84) | 0.65 (0.16–0.89) | --- | 0.65 (0.40–0.80) | |
| VR1–VR2 | 0.69 (0.44–0.84) | 0.69 (0.44–0.84) | 0.61 (0.09–0.91) | 0.69 (0.53–0.81) | |
| Turning | Bedside—VR1 | 0.79 (0.60–0.89) | 0.73 (0.40–0.90) | 0.67 (0.02–0.93) | 0.74 (0.59–0.84) |
| Bedside—VR2 * | 0.90 (0.77–0.96) | 0.66 (0.16–0.89) | --- | 0.80 (0.64–0.89) | |
| VR1–VR2 | 0.82 (0.67–0.91) | 0.78 (0.49–0.91) | 0.66 (0.01–0.92) | 0.79 (0.66–0.87) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, V.; Richard-Lalonde, M.; Gélinas, C. Interrater Agreement between Bedside and Video Raters Using the CPOT-Neuro for Pain Assessment in Critically Ill Patients with a Brain Injury. Nurs. Rep. 2024, 14, 212-219. https://doi.org/10.3390/nursrep14010017
Nguyen V, Richard-Lalonde M, Gélinas C. Interrater Agreement between Bedside and Video Raters Using the CPOT-Neuro for Pain Assessment in Critically Ill Patients with a Brain Injury. Nursing Reports. 2024; 14(1):212-219. https://doi.org/10.3390/nursrep14010017
Chicago/Turabian StyleNguyen, Vivienne, Melissa Richard-Lalonde, and Céline Gélinas. 2024. "Interrater Agreement between Bedside and Video Raters Using the CPOT-Neuro for Pain Assessment in Critically Ill Patients with a Brain Injury" Nursing Reports 14, no. 1: 212-219. https://doi.org/10.3390/nursrep14010017
APA StyleNguyen, V., Richard-Lalonde, M., & Gélinas, C. (2024). Interrater Agreement between Bedside and Video Raters Using the CPOT-Neuro for Pain Assessment in Critically Ill Patients with a Brain Injury. Nursing Reports, 14(1), 212-219. https://doi.org/10.3390/nursrep14010017