Abstract
Background: Haemophagocytic lymphohistiocytosis (HLH) is a rare and potentially life-threatening systemic hyperinflammatory disease, which can have several aetiologies. Clinical case: a 48-year-old woman affected by a transfusion-dependent β-thalassemia was hospitalized in our haematology unit presenting with intermittent fever, haepatosplenomegaly and pancytopenia, which developed a few days after the booster dose of anti-SARS-CoV-2 mRNA vaccine. The investigations performed during hospitalization led to a diagnosis of HLH and steroid therapy where IV dexamethasone was initiated and provided benefits. Conclusions: the severity of HLH mandates early treatment, but the management of patients with post-vaccine HLH is still challenging and requires further study. No cases of HLH in patients with thalassemia were previously described.
1. Introduction
Haemophagocytic lymphohistiocytosis (HLH) is a rare systemic hyperinflammatory disease characterized by the excessive but ineffective stimulation of the immune system, which leads to an accumulation of macrophages and lymphocytes in target organs. The resulting cytokine storm is responsible for severe, life-threatening clinical manifestations; therefore, early diagnosis and treatment are essential. We report a case of a patient with thalassemia who developed pancytopenia, hepatosplenomegaly and fever a few days after receiving anti-SARS-CoV-2 vaccination and was later diagnosed with HLH.
2. Clinical Case
A 48-year-old woman affected by transfusion-dependent β-thalassemia (genotype IVS-I-110 [G > A]/Cod39 [C > T], pre-transfusion haemoglobin levels of about 9 g/dL, ferritin levels kept around 700 ng/mL with deferasirox) was hospitalized in our haematology unit. She presented with intermittent fever and a maximum temperature of 39 °C, preceded by chills, which started six days after receiving anti-SARS-CoV-2 vaccine (booster dose with Comirnaty) and were accompanied by worsening of the anaemia to haemoglobin levels of 6.8 g/dL (9.3 g/dL at the previous test 7 days before vaccination). At the time of hospitalization, the fever had lasted for over a month and had not been responsive to multiple empiric antibiotic treatments. From the onset of fever to hospitalization, the patient had undergone thirteen blood transfusions, about twice her periodic need. Moreover, before admission, a chest radiography was negative for any pathological findings, while abdomen ultrasonography showed an enlargement of the spleen, compared to a previous abdominal ultrasonography performed 6 months earlier (longitudinal diameter increased from 13 to 20 cm). A physical examination showed no clinical evidence suggestive of infection sites and there were no significant history or additional symptoms in the two weeks prior to the vaccination. The patient had not taken any cytotoxic drugs, had no nutritional deficiencies and no family or personal history of autoimmune diseases or other immunological disorders. Table 1 summarizes the most relevant laboratory examinations upon admission.

Table 1.
Main laboratory tests upon admission.
The chest and abdomen computer tomography (CT) scan with contrast showed the already known paravertebral foci of extramedullary erythropoiesis and hepatosplenomegaly with homogeneous density. A positron emission tomography (PET)-CT showed liver and spleen of increased size with heterogeneous hypercaptation of the radiotracer (18F-FDG), mainly affecting the spleen, in absence of other significant findings. Four sets of blood cultures tested negative, and the echocardiogram showed no endocardial vegetations. QuantiFERON-TB Gold urine and stool cultures also tested negative. Several serological tests (via immunofluorescence or enzyme immunoassays) and molecular biology tests (via polymerase chain reaction) were performed on peripheral blood and bone marrow, and the following infectious agents were ruled out as active pathogens: Cytomegalovirus, Epstein–Barr virus, parvovirus B19, hepatitis B virus, hepatitis C virus, Leishmania spp., Rickettsia spp., Aspergillus spp., Bartonella spp., Borrelia burgdorferi, Brucella spp., Toxoplasma gondii, Plasmodium spp., human immunodeficiency virus 1-2. SARS-CoV-2 RNA was not detected on nasopharyngeal swabs.
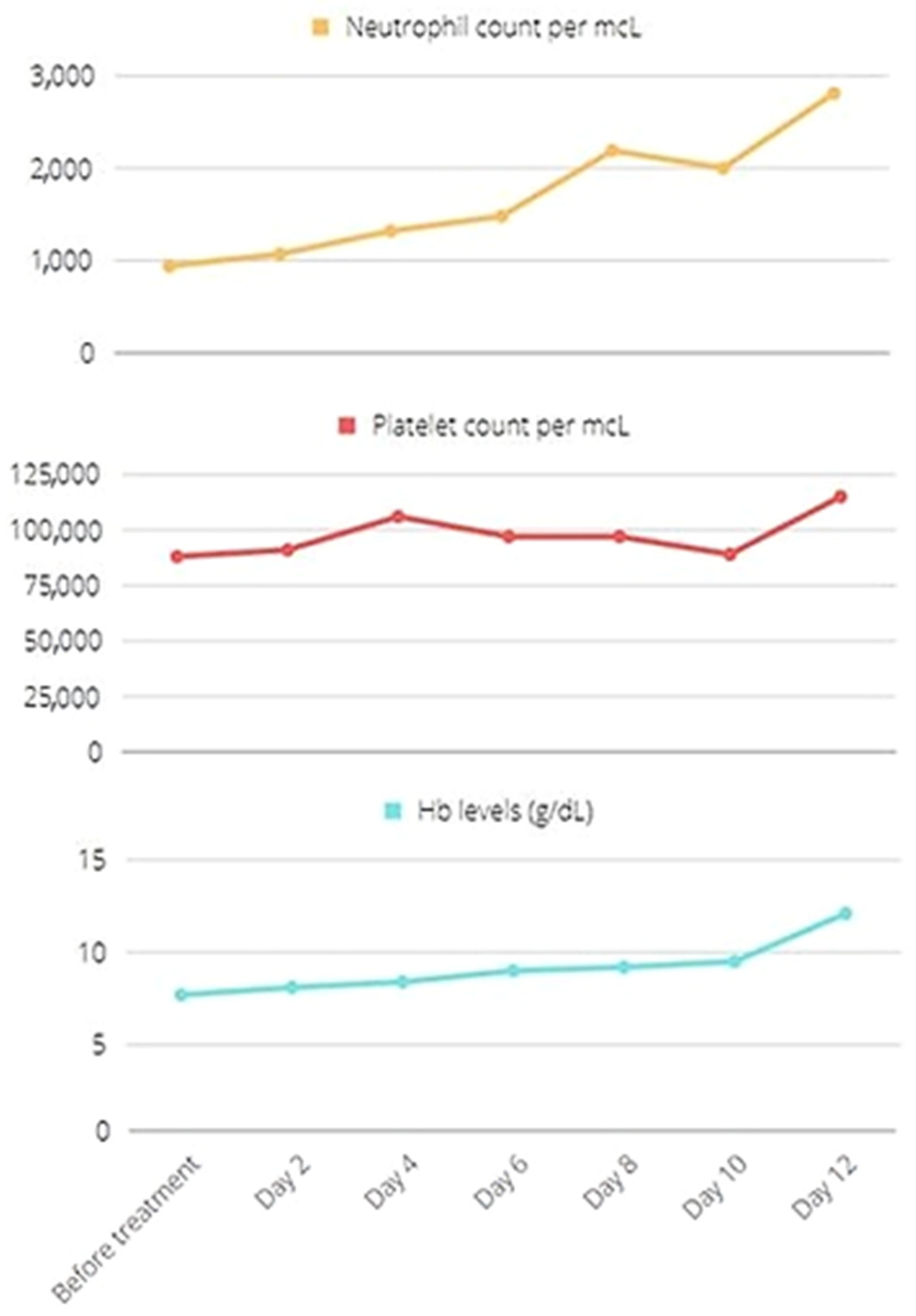
During her hospital stay, haemoglobin level, platelet and neutrophil counts dropped, respectively, to a minimum of 7.7 g/dL, 88 × 103/µL and 0.94 × 103/µL. The bone marrow examination showed a rich histiocytic infiltrate with interstitial distribution, haemophagocytosis and T-prevalent lymphoid infiltrate with interstitial distribution. Moreover, perforin and CD107a expression were tested, showing a normal intracytoplasmic perforin expression but a defective NK cells degranulation. With an H-score [1] of 203 points, defining an 88–93% probability of haemophagocytic syndrome, the patient fulfilled 6 of 8 diagnostic criteria according to the HLH-2004 protocol [2]: fever ≥ 38.5 °C, splenomegaly, peripheral blood trilinear cytopenia, haemophagocytosis in bone marrow, low NK cells activity and ferritin > 500 ng/mL, evaluated as a timing of fast and repeated increase after vaccination (727 ng/mL before vaccine; 927 ng/mL, 1590 ng/mL, 2247 ng/mL at 2, 3, 4 weeks later, respectively) in the presence of normal values of liver iron concentration assessed by magnetic resonance imaging (LIC-R2 3.3 mg/g dry tissue). Hypertriglyceridemia and hypofibrinogenemia were absent, and soluble CD25 was not tested. No genetic tests were performed to rule out hereditary HLH since family history was negative.
Therefore, as the clinical features were chronic by this stage, and the patient’s condition was stable, a steroid therapy with IV dexamethasone 10 mg sid was initiated. After a few days, the complete blood count recovered to normal, and the patient remained apyretic (Figure 1). The patient was treated with dexamethasone for a total of 6 weeks, during which a gradual tapering was performed. No additional supportive care was needed.
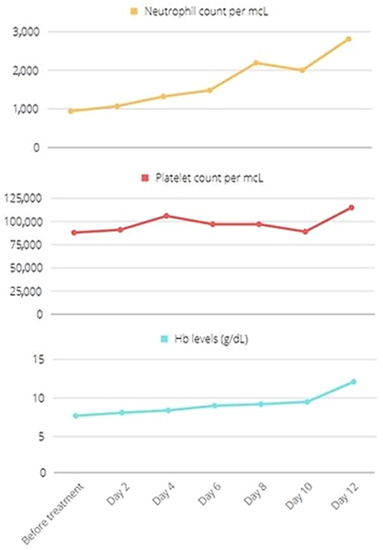
Figure 1.
Resolution of pancytopenia with dexamethasone. Hb: haemoglobin.
3. Discussion
Given the close temporal correlation between the administration of the booster dose of anti-SARS-CoV-2 vaccine and the onset of fever and the worsening of anaemia with subsequent neutropenia and thrombocytopenia, the clinical presentation compatible with HLH was likely triggered by vaccination. Since the patient was admitted to our unit about a month after the onset of symptoms, useful laboratory data that could have been collected in the acute phase were lacking. The timing of the fast and repeated increase in serum ferritin levels associated with normal values of LIC, after vaccination, may be related to the inflammatory state of HLH rather than to iron overloading.
Fortunately, the disease did not have a rapid and ominous course as in most cases. This made it possible to exclude other potential causes of secondary HLH and to attempt a treatment with glucocorticoids only, avoiding classic therapeutic schemes that involve the combination of dexamethasone and etoposide for eight weeks of induction [3,4].
To our knowledge, there are no data concerning the management of HLH in patients with thalassemia, and this is the first case report of a patient with HLH occurring after anti-SARS-CoV-2 booster dose. Other authors have recently described similar cases associated with the first doses of m-RNA or virus-vectored vaccines: some of them were successfully treated with corticosteroid therapy alone, obtaining a rapid remission of symptoms and improvement in blood counts [5,6,7,8]. Some recovered with support therapy alone [9], while others required etoposide or stronger combined therapies with steroids, IVIG and IL-1 receptor antagonists [8,10,11,12]. To date, unfortunately, there are no management guidelines for patients who develop HLH after anti-SARS-CoV-2 vaccination.
4. Conclusions
The immune stimulation caused by vaccines can sometimes lead to systemic hyperinflammatory diseases. The relationship between the immune response to anti-SARS-CoV-2 vaccines and HLH requires further study, but HLH should be considered in patients who present with long-lasting fever after vaccination in the absence of any other potential causes, even after the administration of first doses without adverse reactions.
Author Contributions
Case management, G.C., D.R., S.R., M.G., A.M. and M.C.; data analysis and interpretation, G.C., D.R., A.M., V.L.L. and F.D.; writing—original draft preparation, M.C.; Writing—review and editing, A.M., F.D., A.C. and M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data can be made available upon request to the corresponding author.
Acknowledgments
The authors thank the Foundation Franco and Piera Cutino for the support to conduct research on thalassemia. The help of Eurobloodnet (ERN) in spreading the research on rare diseases is also fully appreciated.
Conflicts of Interest
Aurelio Maggio has been or is a member of advisory boards for Novartis, Celgene Corp (Bristol Meyers Squibb), Vertex and Bluebird Bio. The remaining authors have no conflicts of interest to disclose.
References
- Debaugnies, F.; Mahadeb, B.; Ferster, A.; Meuleman, N.; Rozen, L.; Demulder, A.; Corazza, F. Performances of the H-Score for Diagnosis of Hemophagocytic Lymphohistiocytosis in Adult and Pediatric Patients. Am. J. Clin. Pathol. 2016, 145, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Henter, J.I.; Horne, A.; Aricò, M.; Egeler, R.M.; Filipovich, A.H.; Imashuku, S.; Ladisch, S.; McClain, K.; Webb, D.; Winiarski, J.; et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer 2007, 48, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Henter, J.I.; Aricò, M.; Egeler, R.M.; Elinder, G.; Favara, B.E.; Filipovich, A.H.; Gadner, H.; Imashuku, S.; Janka-Schaub, G.; Komp, D.; et al. HLH-94: A treatment protocol for hemophagocytic lymphohistiocytosis. HLH study Group of the Histiocyte Society. Med. Pediatr. Oncol. 1997, 28, 342–347. [Google Scholar] [CrossRef]
- La Rosée, P.; Horne, A.C.; Hines, M.; von Bahr Greenwood, T.; Machowicz, R.; Berliner, N.; Birndt, S.; Gil-Herrera, J.; Girschikofsky, M.; Jordan, M.B.; et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood 2019, 133, 2465–2477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, L.V.; Hu, Y. Hemophagocytic lymphohistiocytosis after COVID-19 vaccination. J. Hematol. Oncol. 2021, 14, 87. [Google Scholar] [CrossRef] [PubMed]
- Caocci, G.; Fanni, D.; Porru, M.; Greco, M.; Nemolato, S.; Firinu, D.; Faa, G.; Scuteri, A.; La Nasa, G. Kikuchi-Fujimoto disease associated with hemophagocytic lymphohistiocytosis following the BNT162b2 mRNA COVID-19 vaccination. Haematologica 2022, 107, 1222–1225. [Google Scholar] [CrossRef] [PubMed]
- Baek, D.W.; Hwang, S.; Kim, J.; Lee, J.M.; Cho, H.J.; Moon, J.H.; Hwang, N.; Jeong, J.Y.; Lee, S.W.; Sohn, S.K. Patients presenting high fever with lymphadenopathy after COVID-19 vaccination were diagnosed with hemophagocytic lymphohistiocytosis. Infect. Dis. 2022, 54, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Attwell, L.; Zaw, T.; McCormick, J.; Marks, J.; McCarthy, H. Haemophagocytic lymphohistiocytosis after ChAdOx1 nCoV-19 vaccination. J. Clin. Pathol. 2022, 75, 282–284. [Google Scholar] [CrossRef] [PubMed]
- Ai, S.; Awford, A.; Roncolato, F. Hemophagocytic lymphohistiocytosis following ChAdOx1 nCov-19 vaccination. J. Med. Virol. 2022, 94, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Rocco, J.M.; Mallarino-Haeger, C.; Randolph, A.H.; Ray, S.M.; Schechter, M.C.; Zerbe, C.S.; Holland, S.M.; Sereti, I. Hyperinflammatory syndromes after SARS-CoV-2 mRNA vaccination in individuals with underlying immune dysregulation. Clin. Infect. Dis. 2021, ciab1024. [Google Scholar] [CrossRef] [PubMed]
- Hieber, M.L.; Sprute, R.; Eichenauer, D.A.; Hallek, M.; Jachimowicz, R.D. Hemophagocytic lymphohistiocytosis after SARS-CoV-2 vaccination. Infection 2022, 26, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.; Lopez, C.A.; Hines, A.M.; Barrientos, J.C. Haemophagocytic lymphohistiocytosis following COVID-19 mRNA vaccination. BMJ Case Rep. 2022, 15, e247022. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).