
Clinical Outcomes After Endoscopic Retrograde Cholangiopancreatography Using Balloon-Assisted Enteroscopy for Benign Anastomotic Stricture of Choledochojejunostomy: A Retrospective Study
 , and
, and
Abstract
1. Introduction
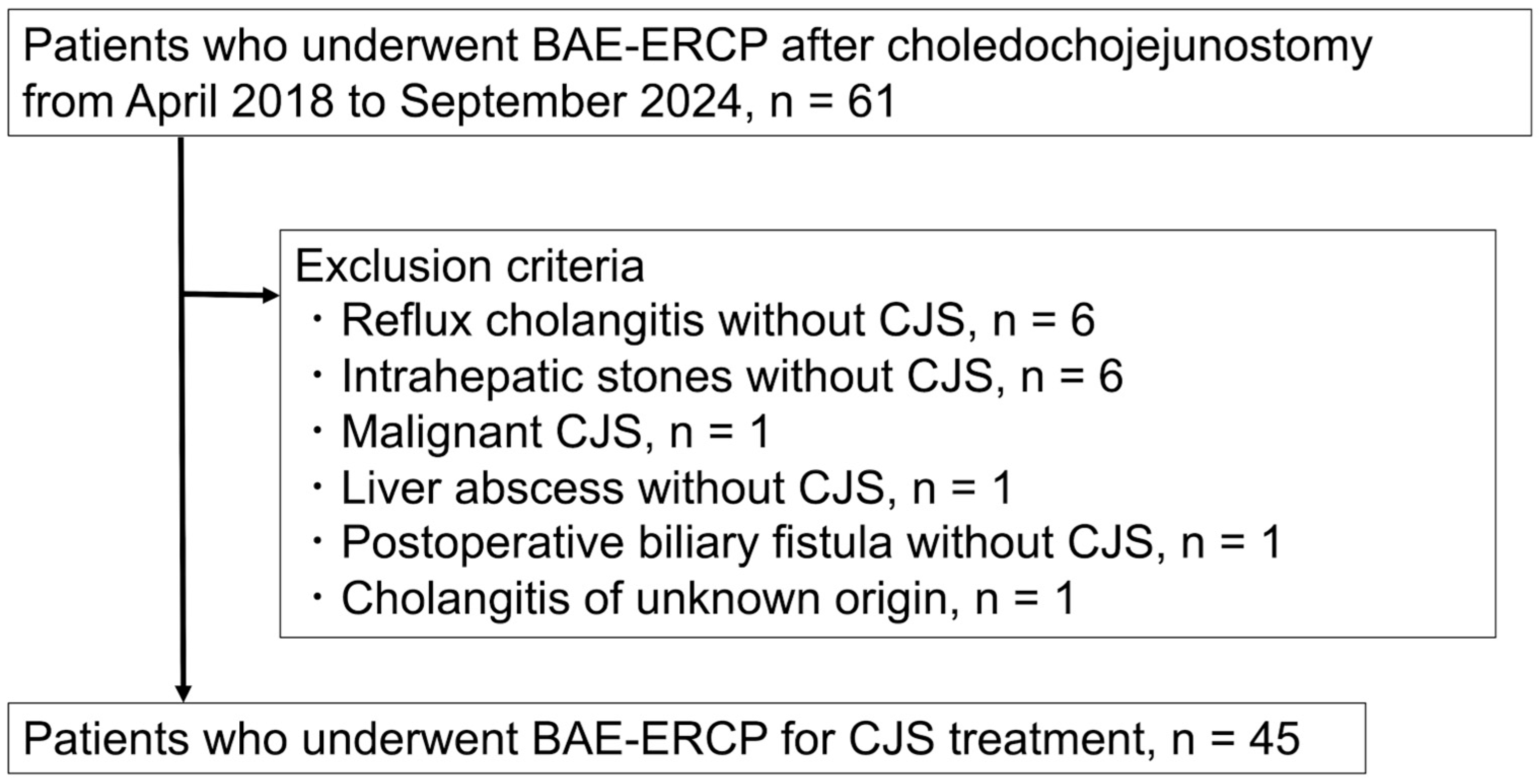
2. Materials and Methods
2.1. Study Design
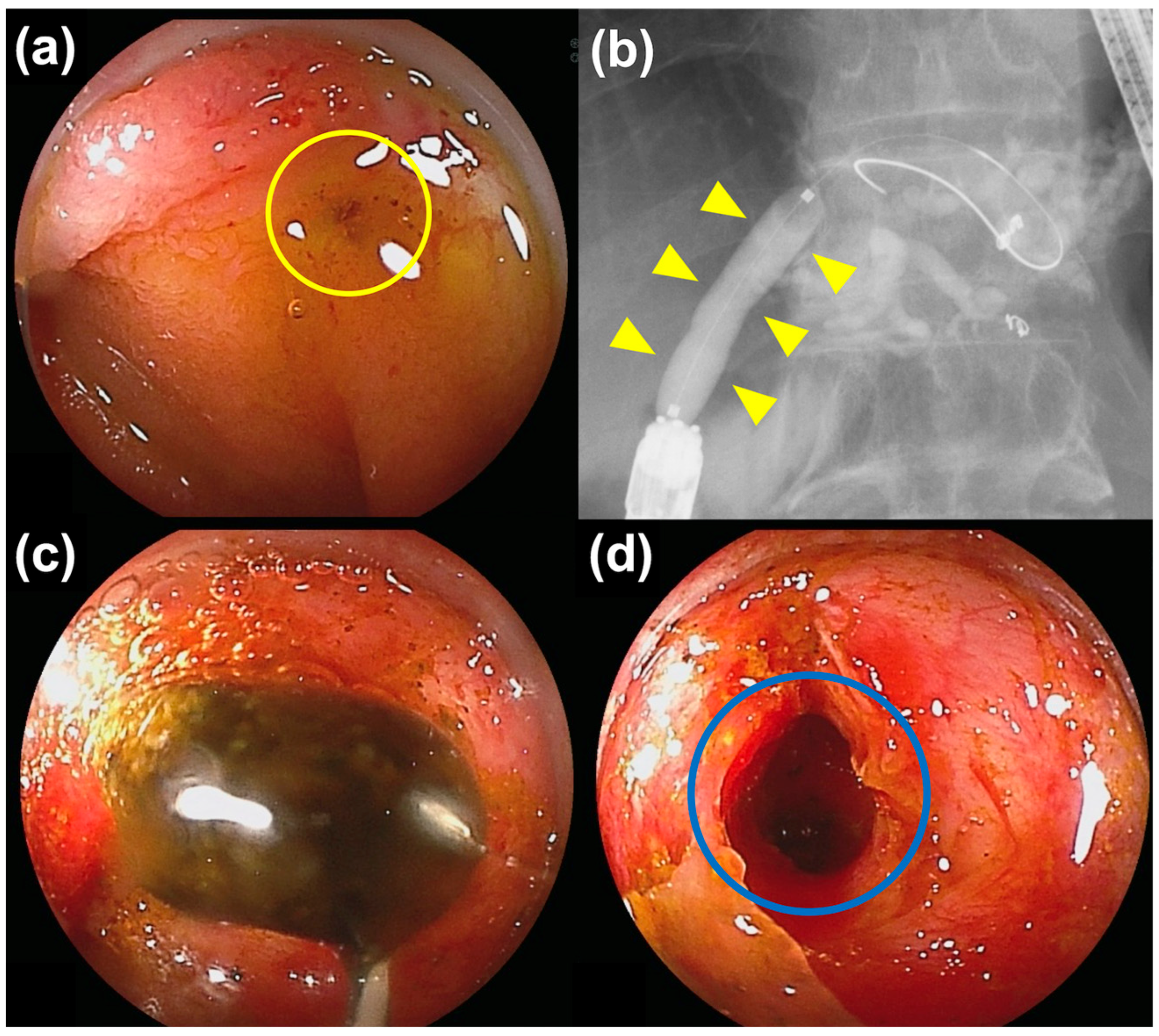
2.2. ERCP
2.3. Outcomes and Definition
2.4. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Procedural Details and AEs
3.3. Potential Factors Affecting Procedural Success
3.4. Recurrence of CJS
3.5. Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dimou, F.M.; Adhikari, D.; Mehta, H.B.; Olino, K.; Riall, T.S.; Brown, K.M. Incidence of hepaticojejunostomy stricture after hepaticojejunostomy. Surgery 2016, 160, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Booij, K.A.C.; Coelen, R.J.; de Reuver, P.R.; Besselink, M.G.; van Delden, O.M.; Rauws, E.A.; Busch, O.R.; van Gulik, T.M.; Gouma, D.J. Long-term follow-up and risk factors for strictures after hepaticojejunostomy for bile duct injury: An analysis of surgical and percutaneous treatment in a tertiary center. Surgery 2018, 163, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- House, M.G.; Cameron, J.L.; Schulick, R.D.; Campbell, K.A.; Sauter, P.K.; Coleman, J.; Lillemoe, K.D.; Yeo, C.J. Incidence and outcome of biliary strictures after pancreaticoduodenectomy. Ann. Surg. 2006, 243, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Tanisaka, Y.; Ryozawa, S.; Itoi, T.; Yamauchi, H.; Katanuma, A.; Okabe, Y.; Irisawa, A.; Nakahara, K.; Iwasaki, E.; Ishii, K.; et al. Efficacy and factors affecting procedure results of short-type single-balloon enteroscopy–assisted ERCP for altered anatomy: A multicenter cohort in Japan. Gastrointest. Endosc. 2022, 95, 310–318.e1. [Google Scholar] [CrossRef] [PubMed]
- Shimatani, M.; Matsushita, M.; Takaoka, M.; Koyabu, M.; Ikeura, T.; Kato, K.; Fukui, T.; Uchida, K.; Okazaki, K. Effective short double-balloon enteroscope for diagnostic and therapeutic ERCP in patients with altered gastrointestinal anatomy: A large case series. Endoscopy 2009, 41, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Yamada, A.; Kogure, H.; Nakai, Y.; Takahara, N.; Mizuno, S.; Tada, M.; Koike, K. Performance of a new short-type double-balloon endoscope with advanced force transmission and adaptive bending for pancreaticobiliary intervention in patients with surgically altered anatomy: A propensity-matched analysis. Dig. Endosc. 2019, 31, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Tomoda, T.; Kato, H.; Ueki, T.; Ogawa, T.; Hirao, K.; Akimoto, Y.; Matsumoto, K.; Horiguchi, S.; Tsutsumi, K.; Okada, H. Efficacy of double-balloon enteroscopy-assisted endoscopic balloon dilatation combined with stent deployment for hepaticojejunostomy anastomotic stricture. Dig. Endosc. 2022, 34, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Iwasa, Y.; Iwashita, T.; Iwata, K.; Okuno, M.; Shimojo, K.; Uemura, S.; Tezuka, R.; Senju, A.; Iwata, S.; Shimizu, M. Safety and efficacy of covered self-expandable metallic stent for choledochojejunal anastomotic stricture: A multi-center retrospective cohort study. Dig. Dis. Sci. 2024, 69, 3481–3487. [Google Scholar] [CrossRef] [PubMed]
- Dell’Anna, G.; Nunziata, R.; Delogu, C.; Porta, P.; Grassini, M.V.; Dhar, J.; Barà, R.; Bencardino, S.; Fanizza, J.; Mandarino, F.V.; et al. The role of therapeutic endoscopic ultrasound in management of malignant double obstruction (biliary and gastric outlet): A comprehensive review with clinical scenarios. J. Clin. Med. 2024, 13, 7731. [Google Scholar] [CrossRef] [PubMed]
- Iwashita, T.; Uemura, S.; Tezuka, R.; Senju, A.; Yasuda, I.; Shimizu, M. Current status of endoscopic ultrasound-guided antegrade intervention for biliary diseases in patients with surgically altered anatomy. Dig. Endosc. 2023, 35, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Nagai, K.; Mukai, S.; Abe, M.; Sofuni, A.; Tsuchiya, T.; Tanaka, R.; Tonozuka, R.; Yamamoto, K.; Matsunami, Y.; Kojima, H.; et al. Long-term outcomes after EUS-guided antegrade intervention for benign bilioenteric anastomotic stricture. Gastrointest. Endosc. 2024, 99, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Iwasa, Y.; Iwashita, T.; Iwata, K.; Uemura, S.; Okuno, M.; Tezuka, R.; Senju, A.; Mukai, T.; Shimizu, M. Long- and short-term outcomes of balloon dilation for benign choledochojejunal anastomotic stricture using balloon endoscopy-assisted ERCP: A multi-center retrospective cohort study. BMC Gastroenterol. 2023, 23, 191. [Google Scholar] [CrossRef] [PubMed]
- Sano, I.; Katanuma, A.; Kuwatani, M.; Kawakami, H.; Kato, H.; Itoi, T.; Ono, M.; Irisawa, A.; Okabe, Y.; Iwashita, T.; et al. Long-term outcomes after therapeutic endoscopic retrograde cholangiopancreatography using balloon-assisted enteroscopy for anastomotic stenosis of choledochojejunostomy/pancreaticojejunostomy. J. Gastroenterol. Hepatol. 2019, 34, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Weng, H.; Fan, Q.Q.; Gu, J.; Weng, M.Z.; Zhang, W.J.; Xu, L.M.; Zhang, Y.; Shu, Y.J.; Wang, X.F. Efficacy and long-term outcomes of single-balloon enteroscopy-assisted treatment for biliary obstruction after choledochojejunostomy. Surg. Endosc. 2024, 38, 6282–6293. [Google Scholar] [CrossRef] [PubMed]
- Kiriyama, S.; Kozaka, K.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Gabata, T.; Hata, J.; Liau, K.H.; Miura, F.; Horiguchi, A.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholangitis (with videos). J. Hepato-Bil. Pancreat. Sci. 2018, 25, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Cotton, P.B.; Eisen, G.M.; Aabakken, L.; Baron, T.H.; Hutter, M.M.; Jacobson, B.C.; Mergener, K.; Nemcek, A.; Petersen, B.T.; Petrini, J.L.; et al. A lexicon for endoscopic adverse events: Report of an ASGE workshop. Gastrointest. Endosc. 2010, 71, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Tomoda, T.; Kato, H.; Miyamoto, K.; Saragai, Y.; Mizukawa, S.; Yabe, S.; Takata, S.; Muro, S.; Uchida, D.; Matsumoto, K.; et al. Comparison between endoscopic biliary stenting combined with balloon dilation and balloon dilation alone for the treatment of benign hepaticojejunostomy anastomotic stricture. J. Gastrointest. Surg. 2020, 24, 1352–1358. [Google Scholar] [CrossRef] [PubMed]
- Shimatani, M.; Mitsuyama, T.; Tokuhara, M.; Masuda, M.; Miyamoto, S.; Ito, T.; Nakamaru, K.; Ikeura, T.; Takaoka, M.; Naganuma, M.; et al. Recent advances of endoscopic retrograde cholangiopancreatography using balloon assisted endoscopy for pancreaticobiliary diseases in patients with surgically altered anatomy: Therapeutic strategy and management of difficult cases. Dig. Endosc. 2021, 33, 912–923. [Google Scholar] [CrossRef] [PubMed]
- Shimatani, M.; Mitsuyama, T.; Yamashina, T.; Takeo, M.; Horitani, S.; Saito, N.; Matsumoto, H.; Orino, M.; Kano, M.; Yuba, T.; et al. Advanced technical tips and recent insights in ERCP using balloon-assisted endoscopy. DEN Open 2024, 4, e301. [Google Scholar] [CrossRef] [PubMed]
- Yane, K.; Katanuma, A.; Maguchi, H.; Takahashi, K.; Kin, T.; Ikarashi, S.; Sano, I.; Yamazaki, H.; Kitagawa, K.; Yokoyama, K.; et al. Short-type single-balloon enteroscope-assisted ERCP in postsurgical altered anatomy: Potential factors affecting procedural failure. Endoscopy 2017, 49, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Kogure, H.; Nakai, Y.; Ishigaki, K.; Hakuta, R.; Saito, K.; Saito, T.; Takahara, N.; Hamada, T.; Mizuno, S.; et al. Double-balloon endoscopy-assisted treatment of hepaticojejunostomy anastomotic strictures and predictive factors for treatment success. Surg. Endosc. 2020, 34, 1612–1620. [Google Scholar] [CrossRef] [PubMed]
- Hosono, K.; Sato, T.; Hasegawa, S.; Kurita, Y.; Yagi, S.; Iwasaki, A.; Fujita, Y.; Sekino, Y.; Tanida, E.; Kessoku, T.; et al. Learning curve of endoscopic retrograde cholangiopancreatography using single-balloon enteroscopy. Dig. Dis. Sci. 2022, 67, 2882–2890. [Google Scholar] [CrossRef] [PubMed]
- Uchida, D.; Tsutsumi, K.; Kato, H.; Matsumi, A.; Saragai, Y.; Tomoda, T.; Matsumoto, K.; Horiguchi, S.; Okada, H. Potential factors affecting results of short-type double-balloon endoscope-assisted endoscopic retrograde cholangiopancreatography. Dig. Dis. Sci. 2020, 65, 1460–1470. [Google Scholar] [CrossRef] [PubMed]
- Tanisaka, Y.; Mizuide, M.; Fujita, A.; Jinushi, R.; Ogawa, T.; Katsuda, H.; Saito, Y.; Miyaguchi, K.; Mashimo, Y.; Ryozawa, S. Competence development of trainees performing short-type single-balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy. J. Hepato-Bil. Pancreat. Sci. 2022, 29, 1316–1326. [Google Scholar] [CrossRef] [PubMed]
- Grobmyer, S.R.; Pieracci, F.M.; Allen, P.J.; Brennan, M.F.; Jaques, D.P. Defining morbidity after pancreaticoduodenectomy: Use of a prospective complication grading system. J. Am. Coll. Surg. 2007, 204, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Kanno, A.; Masamune, A.; Hanada, K.; Maguchi, H.; Shimizu, Y.; Ueki, T.; Hasebe, O.; Ohtsuka, T.; Nakamura, M.; Takenaka, M.; et al. Multicenter study of early pancreatic cancer in Japan. Pancreatology 2018, 18, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Nakachi, K.; Ikeda, M.; Konishi, M.; Nomura, S.; Katayama, H.; Kataoka, T.; Todaka, A.; Yanagimoto, H.; Morinaga, S.; Kobayashi, S.; et al. Adjuvant S-1 compared with observation in resected biliary tract cancer (JCOG1202, Ascot): A multicentre, open-label, randomised, controlled, phase 3 trial. Lancet 2023, 401, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Uesaka, K.; Boku, N.; Fukutomi, A.; Okamura, Y.; Konishi, M.; Matsumoto, I.; Kaneoka, Y.; Shimizu, Y.; Nakamori, S.; Sakamoto, H.; et al. Adjuvant chemotherapy of S-1 versus gemcitabine for resected pancreatic cancer: A phase 3, open-label, randomised, non-inferiority trial (JASPAC 01). Lancet 2016, 388, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Nagai, M.; Nakagawa, K.; Nishiwada, S.; Terai, T.; Hokuto, D.; Yasuda, S.; Matsuo, Y.; Doi, S.; Akahori, T.; Sho, M. Clinically relevant late-onset biliary complications after pancreatoduodenectomy. World J. Surg. 2022, 46, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, K.; Mitoro, A.; Suzuki, H.; Tomooka, F.; Asada, S.; Hanatani, J.I.; Motokawa, Y.; Iwata, T.; Osaki, Y.; Takeda, M.; et al. Role of liquid-based cytology in the endoscopic diagnosis of pancreatic ductal adenocarcinoma. J. Clin. Med. 2024, 13, 6148. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, K.; Mitoro, A.; Tomooka, F.; Asada, S.; Fujinaga, Y.; Nishimura, N.; Kaji, K.; Kawaratani, H.; Akahane, T.; Ozutsumi, T.; et al. Diagnostic yield of liquid-based cytology in serial pancreatic juice aspiration cytological examination. DEN Open 2023, 3, e177. [Google Scholar] [CrossRef] [PubMed]
- Sagami, R.; Nakahodo, J.; Minami, R.; Yamao, K.; Yoshida, A.; Nishikiori, H.; Takenaka, M.; Mizukami, K.; Murakami, K. True diagnostic ability of EUS-guided fine-needle aspiration/biopsy sampling for small pancreatic lesions ≤10 mm and salvage diagnosis by pancreatic juice cytology: A multicenter study. Gastrointest. Endosc. 2024, 99, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Hanada, K.; Shimizu, A.; Kurihara, K.; Ikeda, M.; Yamamoto, T.; Okuda, Y.; Tazuma, S. Endoscopic approach in the diagnosis of high-grade pancreatic intraepithelial neoplasia. Dig. Endosc. 2022, 34, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Iiboshi, T.; Hanada, K.; Fukuda, T.; Yonehara, S.; Sasaki, T.; Chayama, K. Value of cytodiagnosis using endoscopic nasopancreatic drainage for early diagnosis of pancreatic cancer: Establishing a new method for the early detection of pancreatic carcinoma in situ. Pancreas 2012, 41, 523–529. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| All Participants, n = 45 | ||
|---|---|---|
| Age, median, years (range) | 73 (47–88) | |
| Sex, n (%) | Male | 27 (60) |
| Female | 18 (40) | |
| WHO performance status, n (%) | 0 | 34 (75.6) |
| 1 | 11 (24.4) | |
| Indication for surgery, n (%) | Pancreatic cancer | 17 (37.8) |
| IPMN | 6 (13.3) | |
| Congenital biliary dilation | 5 (11.1) | |
| Postsurgical biliary injury/leak | 4 (8.9) | |
| Duodenal cancer | 4 (8.9) | |
| Bile duct cancer | 1 (2.2) | |
| Gastric cancer | 1 (2.2) | |
| Other neoplasms | 5 (11.1) | |
| Other benign diseases | 2 (4.4) | |
| Type of surgery, n (%) | PD and modified Child’s method reconstruction | 32 (71.1) |
| Bile duct/hepatic resection and R-Y reconstruction | 13 (28.9) | |
| Coexistence of intrahepatic stones, n (%) | 28 (62.2) | |
| Time from surgery to ERCP, median (range), days | 1057 (116–12,807) | |
| Severity of cholangitis * before ERCP, n (%) | Mild | 20 (44.4) |
| Moderate | 25 (55.6) | |
| Timing of ERCP §, n (%) | Induction phase | 18 (40) |
| Proficiency phase | 27 (60) | |
| Technical Success for Each Patient, n/N (%) | 36/45 (80%) |
| Median time to insert the scope to the target site, min (range) | 7 (3–48) |
| Total median procedure time, min (range) | 38 (19–136) |
| Balloon diameter, 4–6/8–12 mm, n (%) | 4/32 (11.1/88.9) |
| PS placement, n (%) | 20 (55.6) |
| Number of PS, 1/2, n | 2/18 |
| Diameter of PS, 7-Fr/8.5-Fr | 19/1 |
| Median stent-demanding time, days (range) | 154 (34–1259) |
| Recurrence of CJS following successful ERCP, n/N (%) | 8/36 (22.2%) |
| Adverse Events of all 98 ERCP Procedures, n/N (%) | |
| PS migration (mild) | 3/98 (3.1) |
| Portal vein thrombosis at the tip of the PS (mild) | 1/98 (1.0) |
| Intestinal perforation (severe) | 1/98 (1.0) |
| Variable | Procedural Success (n = 36) | Procedural Failure (n = 9) | p |
|---|---|---|---|
| Age (≥75 years), yes/no, n | 20/16 | 2/7 | 0.135 |
| Sex, male/female, n | 23/13 | 4/5 | 0.449 |
| Primary disease, benign/malignant, n | 15/21 | 7/2 | 0.071 |
| Recurrence of malignant tumor, yes/no, n | 31/5 | 7/2 | 0.614 |
| Reconstruction method, PD/R-Y, n | 28/8 | 4/5 | 0.095 |
| Time from surgery to onset of CJS (≥400 days), yes/no, n | 10/26 | 2/7 | 1 |
| EBD before surgery, yes/no, n | 32/4 | 6/3 | 0.131 |
| Timing of ERCP, induction phase/proficiency phase | 11/25 | 7/2 | 0.019 |
| Facility where the surgery was performed, our hospital/other hospitals, n | 34/2 | 5/4 | 0.010 |
| Univariate Analysis | ||
|---|---|---|
| Hazard Ratio (95% CI) | p | |
| Age (≥75 years) | 0.771 (0.192–3.098) | 0.714 |
| Sex (female) | 0.823 (0.165–4.097) | 0.812 |
| Malignant primary disease | 0.295 (0.058–1.485) | 0.139 |
| Recurrence of the malignant tumor | 1.000 (0.811–1.233) | 0.998 |
| R-Y reconstruction | 2.246 (0.501–10.07) | 0.290 |
| Time from surgery to the onset of CJS < 400 days | 4.651 (1.102–19.63) | 0.036 |
| EBD before surgery | 1.000 (0.744–1.344) | 0.999 |
| Timing of ERCP (proficiency phase) | 2.535 (0.48–13.39) | 0.273 |
| Coexistence of intrahepatic stones | 0.368 (0.082–1.65) | 0.192 |
| PS placement for CJS | 0.359 (0.070–1.853) | 0.221 |
| Balloon dilation with waist disappearance | 0.826 (0.195–3.502) | 0.795 |
| Deaths during follow-up, n (%) | 5 (11.1%) |
| Cause of mortality | |
| Recurrence of pancreatic cancer, n (%) | 4 (8.9%) |
| Liver abscess, n (%) | 1 (2.2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitagawa, K.; Asada, S.; Hanatani, J.-i.; Motokawa, Y.; Osaki, Y.; Iwata, T.; Kaji, K.; Mitoro, A.; Yoshiji, H. Clinical Outcomes After Endoscopic Retrograde Cholangiopancreatography Using Balloon-Assisted Enteroscopy for Benign Anastomotic Stricture of Choledochojejunostomy: A Retrospective Study. Surg. Tech. Dev. 2025, 14, 24. https://doi.org/10.3390/std14030024
Kitagawa K, Asada S, Hanatani J-i, Motokawa Y, Osaki Y, Iwata T, Kaji K, Mitoro A, Yoshiji H. Clinical Outcomes After Endoscopic Retrograde Cholangiopancreatography Using Balloon-Assisted Enteroscopy for Benign Anastomotic Stricture of Choledochojejunostomy: A Retrospective Study. Surgical Techniques Development. 2025; 14(3):24. https://doi.org/10.3390/std14030024
Chicago/Turabian StyleKitagawa, Koh, Shohei Asada, Jun-ichi Hanatani, Yuki Motokawa, Yui Osaki, Tomihiro Iwata, Kosuke Kaji, Akira Mitoro, and Hitoshi Yoshiji. 2025. "Clinical Outcomes After Endoscopic Retrograde Cholangiopancreatography Using Balloon-Assisted Enteroscopy for Benign Anastomotic Stricture of Choledochojejunostomy: A Retrospective Study" Surgical Techniques Development 14, no. 3: 24. https://doi.org/10.3390/std14030024
APA StyleKitagawa, K., Asada, S., Hanatani, J.-i., Motokawa, Y., Osaki, Y., Iwata, T., Kaji, K., Mitoro, A., & Yoshiji, H. (2025). Clinical Outcomes After Endoscopic Retrograde Cholangiopancreatography Using Balloon-Assisted Enteroscopy for Benign Anastomotic Stricture of Choledochojejunostomy: A Retrospective Study. Surgical Techniques Development, 14(3), 24. https://doi.org/10.3390/std14030024