Three-Way Translocation t(12;15;17) (p13;q24;q21) Found in Acute Promyelocytic Leukemia with Basophilic Differentiation

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
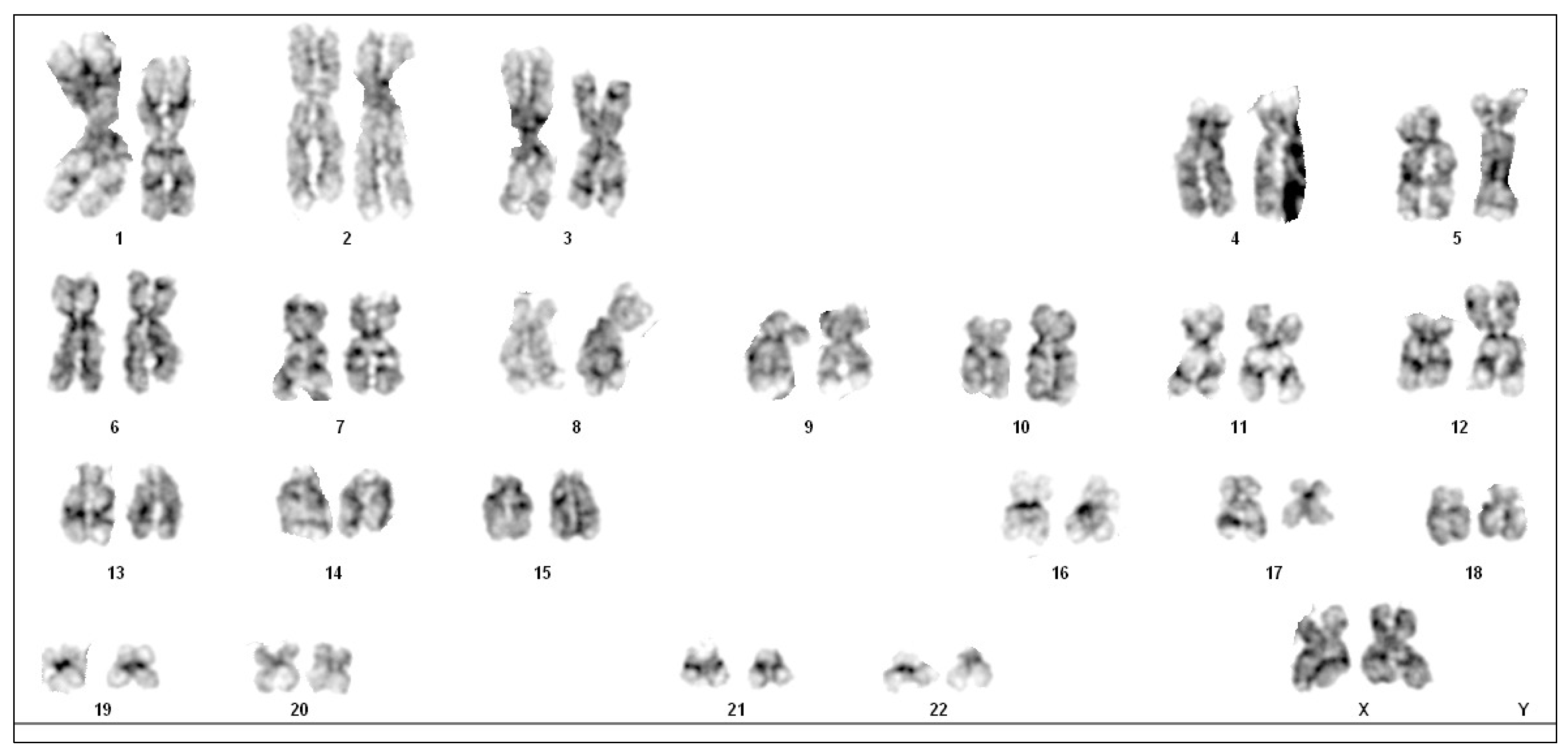
3. Case Presentation
4. Discussion
4.1. Cytogenic Alterations
4.2. t(12;17) Translocation in Acute Leukemia Has Been Described but t(12;15;17) Is Very Rare
4.3. Basophilic Differentiation in APL
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yilmaz, M.; Kantarjian, H.; Ravandi, F. Acute promyelocytic leukemia current treatment algorithms. Blood Cancer J. 2021, 11, 123. [Google Scholar] [CrossRef] [PubMed]
- Grimwade, D.; Coco, F.L. Acute promyelocytic leukemia: A model for the role of molecular diagnosis and residual disease monitoring in directing treatment approach in acute myeloid leukemia. Leukemia 2002, 16, 1959–1973. [Google Scholar] [CrossRef] [PubMed]
- Lo-Coco, F.; Ammatuna, E. The biology of acute promyelocytic leukemia and its impact on diagnosis and treatment. In ASH Education Program Book; ASH Pubblications: Washington, DC, USA, 2006; pp. 156–161. [Google Scholar]
- Guarnera, L.; Ottone, T.; Fabiani, E.; Divona, M.; Savi, A.; Travaglini, S.; Falconi, G.; Panetta, P.; Rapanotti, M.C.; Voso, M.T. Atypical Rearrangements in APL-Like Acute Myeloid Leukemias: Molecular Characterization and Prognosis. Front. Oncol. 2022, 12, 871590. [Google Scholar] [CrossRef] [PubMed]
- Geoffroy, M.C.; de Thé, H. Classic and Variants APLs, as Viewed from a Therapy Response. Cancers 2020, 12, 967. [Google Scholar] [CrossRef] [PubMed]
- Matarraz, S.; Leoz, P.; Fernández, C.; Colado, E.; Chillón, M.C.; Vidriales, M.B.; González, M.; Rivera, D.; Osuna, C.S.; Caballero-Velázquez, T.; et al. Basophil-lineage commitment in acute promyelocytic leukemia predicts for severe bleeding after starting therapy. Mod. Pathol. 2018, 31, 1318–1331. [Google Scholar] [CrossRef] [PubMed]
- Shameli, A.; Jamani, K. Acute promyelocytic leukemia presenting with atypical basophils. Clin. Case Rep. 2020, 8, 584–585. [Google Scholar] [CrossRef] [PubMed]
- Dubé, I.D.; Eaves, C.J.; Kalousek, D.K.; Eaves, A.C. A method for obtaining high quality chromosome preparations from single hemopoietic colonies on a routine basis. Cancer Genet. Cytogenet. 1981, 4, 157–168. [Google Scholar] [CrossRef]
- Howe, B.; Umrigar, A.; Tsien, F. Chromosome Preparation From Cultured Cells. J. Vis. Exp. 2014, 83, e50203. [Google Scholar]
- Simons, A.; Shaffer, L.G.; Hastings, R.J. Cytogenetic Nomenclature: Changes in the ISCN 2013 Compared to the 2009 Edition. Cytogenet. Genome Res. 2013, 141, 1–6. [Google Scholar] [CrossRef]
- Gabert, J.; Beillard, E.; van der Velden, V.H.J.; Bi, W.; Grimwade, D.; Pallisgaard, N.; Barbany, G.; Cazzaniga, G.; Cayuela, J.M.; Cavé, H.; et al. Standardization and quality control studies of ‘real-time’ quantitative reverse transcriptase polymerase chain reaction of fusion gene transcripts for residual disease detection in leukemia—A Europe Against Cancer program. Leukemia 2003, 17, 2318–2357. [Google Scholar] [CrossRef]
- Lemons, R.S.; Eilender, D.; Waldmann, R.A.; Rebentisch, M.; Frej, A.; Ledbetter, D.H.; Willman, C.; McConnell, T.; O’Connell, P. Cloning and Characterization of the t(15;17) translocation breakpoint region in acute promyelocytic leukemia. Genes Chromosomes Cancer 1990, 87, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Alcalay, M.; Zangrilli, D.; Pandolfi, P.P.; Longo, L.; Mencarelli, A.; Giacomucci, A.; Rocchi, M.; Biondi, A.; Rambaldi, A.; Coco, F.L. Translocation breakpoint of acute promyelocytic leukemia lies within the retinoic acid receptor a locus. Proc. Natl. Acad. Sci. USA 1991, 88, 1977–1981. [Google Scholar] [CrossRef] [PubMed]
- Borrow, J.; Goddard, A.D.; Sheer, D. Molecular Analysis of Acute Promyelocytic Leukemia Breakpoint Cluster Region on Chromosome 17. Science 1990, 249, 1577–1580. [Google Scholar] [CrossRef] [PubMed]
- Bennour, A.; Tabka, I.; Ben Youssef, Y.; Zaier, M.; Hizem, S.; Khelif, A.; Saad, A.; Sennana, H. A PML/RARA chimeric gene on chromosome 12 in a patient with acute promyelocytic leukemia (M4) associated with a new variant translocation: T(12;15;17) (q24;q24;q11). Med. Oncol. 2013, 30, 409. [Google Scholar] [CrossRef] [PubMed]
- Saiki, Y.; Sakai, H.; Uchida, A.; Uemura, Y.; Matsunawa, M.; Isobe, Y.; Kato, M.; Tomita, N.; Miura, I.; Arai, A. Leukemic cell kinetics of APL with a novel complex variant t (12;17;15) (p13;q21;q22). Rinsho. Ketsueki. 2020, 61, 103–109. [Google Scholar] [PubMed]
- Kaneko, Y.; Rowley, J.D.; Variakojis, D.; Chilcote, R.R.; Check, I.; Sakurai, M. Correlation of karyotype with clinical features in acute lymphoblastic leukemia. Cancer Res. 1982, 42, 2918–2929. [Google Scholar] [PubMed]
- Grammatico, S.; Vitale, A.; La Starza, R.; Gorello, P.; Angelosanto, N.; Negulici, A.D.; De Propris, M.S.; Nanni, M.; Meloni, G.; Mecucci, C.; et al. Lineage switch from pro-B acute lymphoid leukemia to acute myeloid leukemia in a case with t(12;17) (p13;q11)/ TAF15- ZNF384 rearrangement. Leuk. Lymphoma 2013, 54, 1802–1805. [Google Scholar] [CrossRef]
- Yamamoto, K.; Kawamoto, S.; Mizutani, Y.; Yakushijin, K.; Yamashita, T.; Nakamachi, Y.; Kawano, S.; Hayashi, Y.; Matsuoka, H.; Minami, H. Mixed phenotype acute leukemia with t(12;17) (p13;q21)/TAF15-ZNF384 and other chromosome abnormalities. Cytogenet. Genome Res. 2016, 149, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.W.; Wan, S.K.; Ching, L.M.; Liang, R.; Chan, L.C. Translocation (12;17) (p11-12;q11-12): A recurrent primary rearrangement in acute leukemia. Cancer Genet. Cytogenet. 1992, 64, 27–29. [Google Scholar] [CrossRef]
- Georgakopoulos, N.; Diamantopoulos, P.; Micci, F.; Giannakopoulos, N.; Zervakis, K.; Dimitrakopoulou, A.; Viniou, N.A. An Adult Patient with Early Pre-B Acute Lymphoblastic Leukemia with t(12;17) (p13;q21)/ZNF384-TAF15. Vivo 2018, 32, 1241–1245. [Google Scholar] [CrossRef]
- Sreedharanunni, S.; Kumar, N.; Prakash, G. Basophilia and megakaryoblastic differentiation in a case of acute myeloid leukemia: An unusual morphological combination. Hematol. Oncol. Stem Cell Ther. 2016, 9, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Tallman, M.S.; Hakimian, D.; Snower, D.; Rubin, C.M.; Reisel, H.; Variakojis, D. Basophilic differentiation in acute promyelocytic leukemia. Leukemia 1993, 7, 521–526. [Google Scholar] [PubMed]
- Zhang, J.; Li, M.; He, Y. Acute promyelocytic leukaemia with increased basophils. Br. J. Haematol. 2019, 185, 7. [Google Scholar] [CrossRef] [PubMed]
- Lebecque, B.; Lechevalier, N. B & B: Basophils and bleeding, an atypical case of acute promyelocytic leukemia. Blood 2018, 132, 2107. [Google Scholar]
- Shimamoto, Y.; Suga, K.; Yamaguchi, M.; Kuriyama, K.; Tomonaga, M. Prophylaxis of symptoms of hyperhistaminemia after the treatment of acute promyelocytic leukemia with all-trans retinoic acid. Acta Haematol. 1994, 92, 109–112. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cytogenetic Abnormality | Fusion Gene | Incidence |
|---|---|---|
| t(15;17) (q22;q21) | PML::RARA | 98% |
| t(11;17) (q23;q21) | ZBTB16::RARA | 1% |
| t(X;17) (p11;q21) | BCoR::RARA | 2 cases |
| t(X;17) (p28;q12) | X::RARA | 1 case |
| t(4;17) (q12;q21) | FIP1L1::RARA | 4 cases |
| t(3;17) (q26;q21) | TBLR1::RARA | 4 cases |
| t(3;17) (q26;q21) | FNDC3B::RARA | 1 case |
| t(7;17) (q11;q21) | 6TF2I::RARA | 1 case |
| t(1;17) (q42;q21) | IRF2BP2::RARA | 6 cases |
| t(2;17) (q32;q21) | OBFC2A::RARA | 1 case |
| t(5;17) (q35;q21) | NPM1::RARA | 11 cases |
| t(11;17) (q13;q21) | NuMA::RARA | 1 case |
| del(17) (q21q24) | PRKAR1A::RARA | 1 case |
| t(17;17) (q21;q21) | STAT5b::RARA | 17 cases |
| t(17;17) (q21;q21) | STAT3::RARA | 2 cases |
| t(17;17) (q21;q24) | PRKAR1A::RARA | 2 cases |
| t(14;17) (q11;q21) | HNRNPC::RARA | 1 case |
| t(3;14;17) (q12;q11;q21) | TFG::RARA | 1 case |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frazzetto, S.; Gullo, L.; Sapuppo, G.; Fazio, M.; Lo Faro, C.; Giunta, G.; Caravotta, I.; Mauro, E.; Parisi, M.S.; Triolo, A.M.; et al. Three-Way Translocation t(12;15;17) (p13;q24;q21) Found in Acute Promyelocytic Leukemia with Basophilic Differentiation. Hematol. Rep. 2024, 16, 367-374. https://doi.org/10.3390/hematolrep16020037
Frazzetto S, Gullo L, Sapuppo G, Fazio M, Lo Faro C, Giunta G, Caravotta I, Mauro E, Parisi MS, Triolo AM, et al. Three-Way Translocation t(12;15;17) (p13;q24;q21) Found in Acute Promyelocytic Leukemia with Basophilic Differentiation. Hematology Reports. 2024; 16(2):367-374. https://doi.org/10.3390/hematolrep16020037
Chicago/Turabian StyleFrazzetto, Sara, Lara Gullo, Gabriele Sapuppo, Manlio Fazio, Cristina Lo Faro, Giuliana Giunta, Ignazio Caravotta, Elisa Mauro, Marina Silvia Parisi, Anna Maria Triolo, and et al. 2024. "Three-Way Translocation t(12;15;17) (p13;q24;q21) Found in Acute Promyelocytic Leukemia with Basophilic Differentiation" Hematology Reports 16, no. 2: 367-374. https://doi.org/10.3390/hematolrep16020037
APA StyleFrazzetto, S., Gullo, L., Sapuppo, G., Fazio, M., Lo Faro, C., Giunta, G., Caravotta, I., Mauro, E., Parisi, M. S., Triolo, A. M., Parrinello, N. L., Consoli, M. L., També, L., Cambria, D., Marino, S., Scuderi, G., & Di Raimondo, F. (2024). Three-Way Translocation t(12;15;17) (p13;q24;q21) Found in Acute Promyelocytic Leukemia with Basophilic Differentiation. Hematology Reports, 16(2), 367-374. https://doi.org/10.3390/hematolrep16020037