
Analysis of Risk Determinants of Neonatal Mortality in the Last Decade: A Systematic Literature Review (2013–2023)

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Methodological Approach
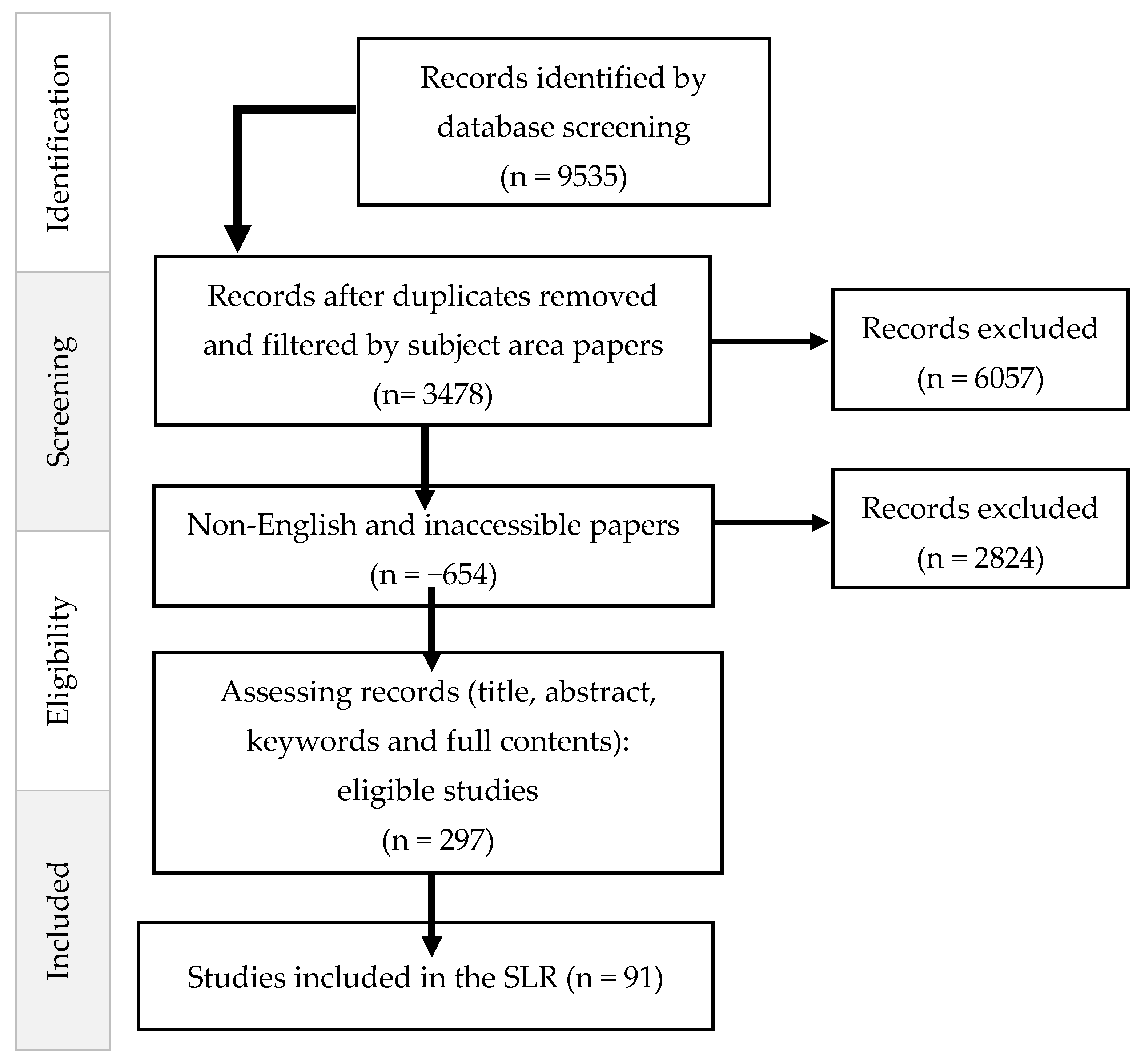
2.2. Data Selection
2.3. Data Analysis and Synthesis
3. Results
3.1. Bibliometric Analysis
3.1.1. Year of Publication
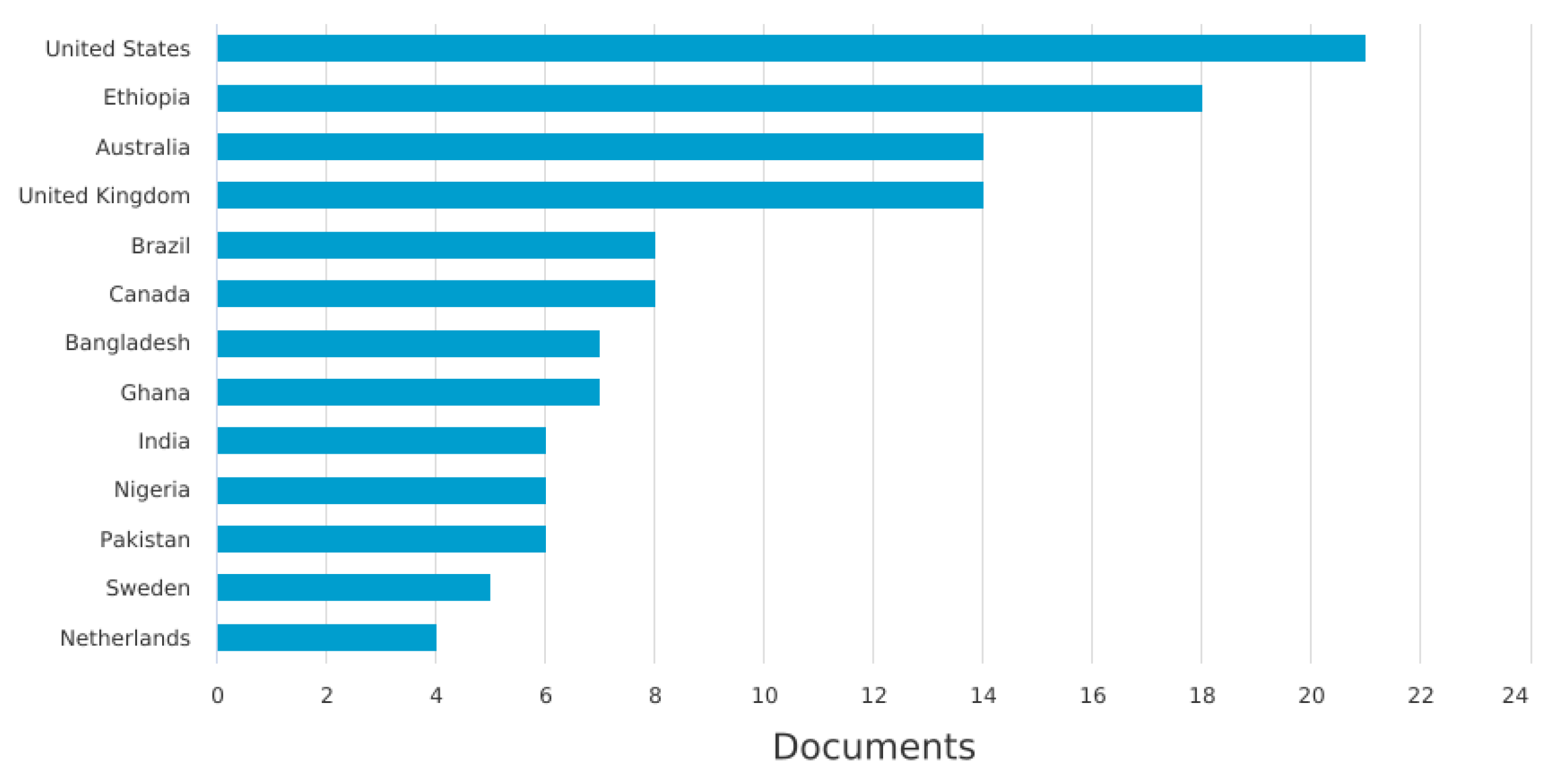
3.1.2. Documents by Country
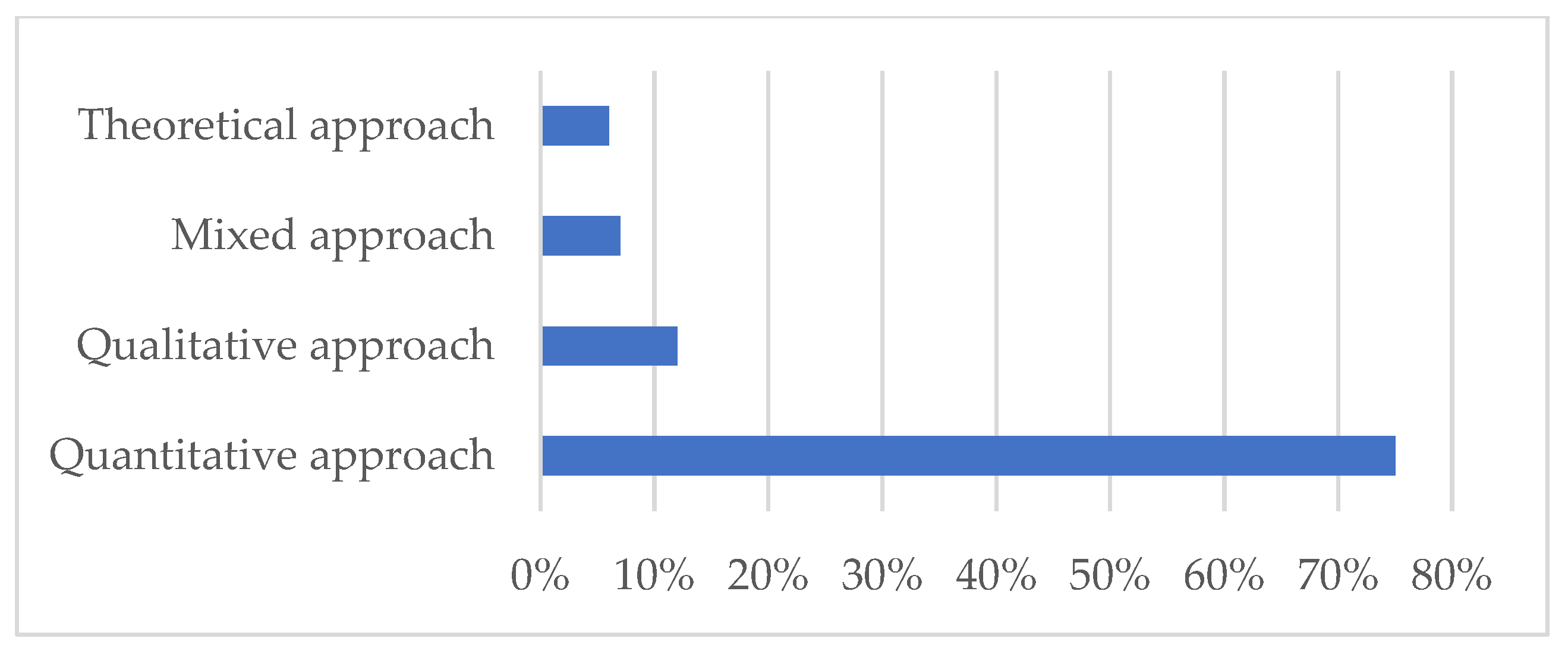
3.1.3. Methodologies Used and Research Fields
3.1.4. Documents by Type
3.1.5. Documents by Subject Area
3.2. Detailed Results
4. Discussion
5. Conclusions
5.1. Theoretical and Practical Implications
5.2. Research Limitations and Futures Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alkema, L.; Chou, D.; Hogan, D.; Zhang, S.; Moller, A.B.; Gemmill, A.; Fat, D.M.; Boerma, T.; Temmerman, P.M.; Mathers, C.; et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: A systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet 2016, 387, 462–474. [Google Scholar] [CrossRef]
- Liu, L.; Oza, S.; Hogan, D.; Perin, J.; Rudan, I.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet 2015, 385, 430–440. [Google Scholar] [CrossRef]
- OEzeh, O.K.; Agho, K.E.; Dibley, M.J.; Hall, J.; Page, A.N. Determinants of neonatal mortality in Nigeria: Evidence from the 2008 demographic and health survey. BMC Public Health 2014, 14, 521. [Google Scholar] [CrossRef]
- Mekonnen, Y.; Tensou, B.; Telake, D.S.; Degefie, T.; Bekele, A. Neonatal mortality in Ethiopia: Trends and determinants. BMC Public Health 2013, 13, 483. [Google Scholar] [CrossRef]
- Murad, W.; Abdullah, A.B.M.; Islam, M.; Alam, M.; Reaiche, C.; Boyle, S. Determinants of neonatal, infant and under-five mortalities: Evidence from a developing country, Bangladesh. J. Public Health Policy 2023, 44, 230–241. [Google Scholar] [CrossRef]
- Hazel, E.A.; Erchick, D.J.; Katz, J.; Lee, A.C.; Diaz, M.; Wu, L.S.; West, K.P., Jr.; Shamim, A.A.; Christian, P.; Ali, H.; et al. Neonatal mortality risk of vulnerable newborns: A descriptive analysis of subnational, population-based birth cohorts for 238 203 live births in low-and middle-income settings from 2000 to 2017. BJOG Int. J. Obstet. Gynaecol. 2023. ahead of print. [Google Scholar] [CrossRef]
- Hambisa, H.D.; Gedamu, S.; Birku, Z.; Emana, D.J. The top determinants and magnitude of preterm neonatal mortality in Ethiopia. Systematic review and meta-analysis. J. Neonatal Nurs. 2023, 29, 612–619. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 151, W-65–W-94. [Google Scholar]
- Zhu, J.; Liu, W. A tale of two databases: The use of Web of Science and Scopus in academic papers. Scientometrics 2020, 123, 321–335. [Google Scholar] [CrossRef]
- Page, M.J.; E McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Bettany-Saltikov, J. EBOOK: How to Do a Systematic Literature Review in Nursing: A Step-by-Step Guide; Open University Press: Berkshire, UK, 2016. [Google Scholar]
- Baloyi, W.T.H. Systematic review as a research method in postgraduate nursing education. Health Gesondheid 2016, 21, 120–128. [Google Scholar]
- Davies, A. Carrying out systematic literature reviews: An introduction. Br. J. Nurs. 2019, 28, 1008–1014. [Google Scholar] [CrossRef]
- Van Eck, N.; Waltman, L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010, 84, 523–538. [Google Scholar] [CrossRef]
- Kirkwood, B.R.; Manu, A.; Asbroek, A.H.T.; Soremekun, S.; Weobong, B.; Gyan, T.; Danso, S.; Amenga-Etego, S.; Tawiah-Agyemang, C.; Owusu-Agyei, S.; et al. Effect of the Newhints home-visits intervention on neonatal mortality rate and care practices in Ghana: A cluster randomised controlled trial. Lancet 2013, 381, 2184–2192. [Google Scholar] [CrossRef]
- Boccolini, C.S.; de Carvalho, M.L.; de Oliveira, M.I.C.; Pérez-Escamilla, R. Breastfeeding during the first hour of life and neonatal mortality. J. Pediatr. (Rio. J.) 2013, 89, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Iliodromiti, S.; Mackay, D.F.; Smith, G.C.S.; Pell, J.P.; Nelson, S.M. Apgar score and the risk of cause-specific infant mortality: A population-based cohort study. Lancet 2014, 384, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Grünebaum, A.; McCullough, L.B.; Sapra, K.J.; Brent, R.L.; Levene, M.I.; Arabin, B.; Chervenak, F.A. Early and total neonatal mortality in relation to birth setting in the United States, 2006–2009. Am. J. Obstet. Gynecol. 2014, 211, 390.e1–390.e7. [Google Scholar] [CrossRef]
- Fernandes, Q.F.; Wagenaar, B.H.; Anselmi, L.; Pfeiffer, J.; Gloyd, S.; Sherr, K. Effects of health-system strengthening on under-5, infant, and neonatal mortality: 11-year provincial-level time-series analyses in Mozambique. Lancet Glob. Health 2014, 2, e468–e477. [Google Scholar] [CrossRef]
- Yego, F.; D’este, C.; Byles, J.; Williams, J.S.; Nyongesa, P. Risk factors for maternal mortality in a Tertiary Hospital in Kenya: A case control study. BMC Pregnancy Childbirth 2014, 14, 38. [Google Scholar] [CrossRef]
- Batista, C.B.; de Carvalho, M.L.; Vasconcelos, A.G.G. Access to and use of health services as factors associated with neonatal mortality in the North, Northeast, and Vale do Jequitinhonha regions, Brazil. J. Pediatr. (Rio. J.) 2018, 94, 293–299. [Google Scholar] [CrossRef]
- Ahmed, I.; Ali, S.M.; Amenga-Etego, S.; Ariff, S.; Bahl, R.; Baqui, A.H.; Begum, N.; Bhandari, N.; Bhatia, K.; A Bhutta, Z.; et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: A multi-country prospective cohort study. Lancet Glob. Health 2018, 6, e1297–e1308. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.P.; Fernandes, C.M.; Traebert, J. Risk factors for neonatal death in the capital city with the lowest infant mortality rate in Brazil. J. Pediatr. (Rio. J.) 2019, 95, 194–200. [Google Scholar] [CrossRef]
- de Souza, S.; Duim, E.; Nampo, F.K. Determinants of neonatal mortality in the largest international border of Brazil: A case-control study. BMC Public Health 2019, 19, 1304. [Google Scholar] [CrossRef] [PubMed]
- Ferraz, A.; Nunes, F.; Resende, C.; Almeida, M.C.; Taborda, A. Short-term neonatal outcomes of vacuum-assisted delivery. A case–control study. An. Pediatría (Engl. Ed.) 2019, 91, 378–385. [Google Scholar] [CrossRef]
- Barquiel, B.; Herranz, L.; Martínez-Sánchez, N.; Montes, C.; Hillman, N.; Bartha, J.L. Increased risk of neonatal complications or death among neonates born small for gestational age to mothers with gestational diabetes. Diabetes Res. Clin. Pract. 2020, 159, 107971. [Google Scholar] [CrossRef]
- Grünebaum, A.; McCullough, L.B.; Orosz, B.; Chervenak, F.A. Neonatal mortality in the United States is related to location of birth (hospital versus home) rather than the type of birth attendant. Am. J. Obstet. Gynecol. 2020, 223, 254.e1–254.e8. [Google Scholar] [CrossRef]
- Guinsburg, R.; Sanudo, A.; Kiffer, C.R.V.; Marinonio, A.S.S.; Costa-Nobre, D.T.; Areco, K.N.; Kawakami, M.D.; Miyoshi, M.H.; Bandiera-Paiva, P.; de Cássia X Balda, R.; et al. Annual trend of neonatal mortality and its underlying causes: Population-based study–São Paulo State, Brazil, 2004–2013. BMC Pediatr. 2021, 21, 54. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-S.; Liang, F.-W.; Lin, Y.-J.; Lu, T.-H.; Lin, C.-H. Neonatal and infant mortality of very-low-birth-weight infants in Taiwan: Does the level of delivery hospital matter? Pediatr. Neonatol. 2021, 62, 419–427. [Google Scholar] [CrossRef]
- Islam, M.A.; Biswas, B. Socio-economic factors associated with increased neonatal mortality: A mixed-method study of Bangladesh and 20 other developing countries based on demographic and health survey data. Clin. Epidemiol. Glob. Health 2021, 11, 100801. [Google Scholar] [CrossRef]
- Eyeberu, A.; Shore, H.; Getachew, T.; Atnafe, G.; Dheresa, M. Neonatal mortality among neonates admitted to NICU of Hiwot Fana specialized university hospital, eastern Ethiopia, 2020: A cross-sectional study design. BMC Pediatr. 2021, 21, 125. [Google Scholar] [CrossRef]
- Alabi, Q.K.; Oyedeji, A.S.; Kayode, O.O.; Kajewole-Alabi, D.I. Impact of COVID-19 pandemic on mother and child health in Sub-Saharan Africa—A review. Pediatr. Res. 2023, 94, 1278–1283. [Google Scholar] [CrossRef] [PubMed]
- Sampurna, M.T.A.; Handayani, K.D.; Utomo, M.T.; Angelika, D.; Etika, R.; Harianto, A.; Mahindra, M.P.; Efendi, F.; Kaban, R.K.; Rohsiswatmo, R.; et al. Determinants of neonatal deaths in Indonesia: A national survey data analysis of 10,838 newborns. Heliyon 2023, 9, e12980. [Google Scholar] [CrossRef] [PubMed]
- Seale, A.C.; Blencowe, H.; Manu, A.A.; Nair, H.; Bahl, R.; Qazi, S.A.; Zaidi, A.K.; Berkley, J.A.; Cousens, P.S.N.; Lawn, P.J.E.; et al. Estimates of possible severe bacterial infection in neonates in sub-Saharan Africa, south Asia, and Latin America for 2012: A systematic review and meta-analysis. Lancet Infect. Dis. 2014, 14, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Blondel, B.; Bréart, G. Mortinatalité et mortalité néonatale. EMC-Pédiatrie 2004, 1, 97–108. [Google Scholar] [CrossRef]
- Christina, N.; Ioanna, P.; George, L.; Konstantinos, T.; Georgios, S. Risk factors for nosocomial infections in neonatal intensive care units (NICU). Health Sci. J. 2015, 9, 1–6. [Google Scholar]
- Zingg, W.; Hopkins, S.; Gayet-Ageron, A.; Holmes, A.; Sharland, M.; Suetens, C.; Almeida, M.; Asembergiene, J.; Borg, M.A.; Budimir, A.; et al. Health-care-associated infections in neonates, children, and adolescents: An analysis of paediatric data from the European Centre for Disease Prevention and Control point-prevalence survey. Lancet Infect. Dis. 2017, 17, 381–389. [Google Scholar] [CrossRef]
- Almudeer, A.H.; Alibrahim, M.A.; Gosadi, I.M. Epidemiology and risk factors associated with early onset neonatal sepsis in the south of KSA. J. Taibah Univ. Med. Sci. 2020, 15, 509–514. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion criteria | Document type | Literature review article, empirical research article, meta-analysis, systematic literature review, and conference article. |
| Objectives | All studies that address risk factors of neonatal mortality. | |
| Language | Articles published in English on the topics of neonatal mortality. | |
| Exclusion criteria | Type of document | Thesis and dissertations. |
| Objectives | Any article that does not focus on neonatal mortality in the broad sense. | |
| Keywords | “Infant mortality”, “neonatal mortality”, “neonatal mortality and risk factors”, “health services”, “prematurity”, “pregnancy”, “delivery” | |
| Scanned items | Article title, abstract, keywords. | |
| Database | Scopus, Web of Science (WoS), PubMed, Springer, Science Direct, and JSTOR, | |
| Documents | Frequency | % |
|---|---|---|
| Article | 78 | 86% |
| Review | 8 | 9% |
| Book chapter | 2 | 2% |
| Conference paper | 1 | 1% |
| Short Survey | 1 | 1% |
| Letter | 1 | 1% |
| 91 | 100% |
| Subject Area | Documents | Frequency (%) |
|---|---|---|
| Medicine | 59 | 65% |
| Multidisciplinary | 7 | 8% |
| Biochemistry, Genetics, and Molecular Biology | 4 | 4% |
| Social Sciences | 3 | 3% |
| Immunology and Microbiology | 2 | 2% |
| Environmental Science | 1 | 1% |
| Agricultural and Biological Sciences | 1 | 1% |
| Nursing | 1 | 1% |
| Pharmacology, Toxicology, and Pharmaceutics | 1 | 1% |
| 91 | 100% |
| Author | Country | Method Study Population | Sample | Results: Validated Factors | Perspectives: Variables Reducing Neonatal Mortality |
|---|---|---|---|---|---|
| Kirkwood et al. [16] | Ghana, the Brong Ahafo region | Cluster randomized controlled trial/pregnancies that ended in live birth or stillbirth between November 2008 and December 2009 from 98 new hint areas. | 15,200 live births | Home visits to perform necessary care can reduce the risk of neonatal mortality. | Home visits for promoting essential newborn care practices and treating or referral of sick babies can reduce neonatal mortality rates. |
| Boccolini et al. [17] | 67 countries in all continents | Ecological panel study on 67/ live births from 67 countries. This study used secondary data from 67 countries obtained from Demographic and Health Surveys. | N = 1000 | - Delayed breastfeeding initiation. - Poor delivery and birth care conditions. - Complications of prematurity. - Birth asphyxia. | Helping mothers to initiate breastfeeding in this sensitive period, with mother and newborn on the alert. |
| Iliodromiti et al. [18] | Royaume-Uni (Ecosse) | Population-based cohort study/ singleton live births in women with a gestational age at delivery between 22 and 44 weeks. | N = 2307 cases | A low Apgar score at 5 min was strongly associated with the risk of neonatal and infant death due to anoxia or infection, with an additional association with hyaline membrane disease in preterm infants. | The authors did not suggest any recommendations. |
| Grünebaum et al. [19] | United States | Retrospective study/infant births and deaths linked to the Centers for Disease Control and Prevention in the United States from 2006 to 2009. | 4 million births in the United States each year | - Home deliveries by a midwife were associated with a considerably greater risk of total infant death than hospital midwife births. - The rate of total and early neonatal mortality for home births remained higher, as did the risks for women of 41 weeks or more and women with a first birth. - Deliveries outside of hospitals greatly raised the chance of infant mortality. | Physicians and other health care providers have a professional responsibility to understand, identify, and address the underlying cause of patients’ desire to give birth outside of the hospital by providing evidence-based compassionate hospital care, improving the hospital setting, treating obstetrical interventions, and providing excellent hospital care. |
| Fernandes et al. [20] | Mozambique | Longitudinal subnational study ((Demographic and Health Survey (2003 and 2011) and Multiple Indicator Cluster Survey (2008)) data /children under 5 and newborns. | 26,464 children in 2000, 20,936 children in 2005, and 10,697 children in 2010 | -Facility-based birth assistance. -The overall density of the public sector health workforce and the density of maternal and child health nurses and coverage of facility-based birth assistance were strongly associated with reduced neonatal mortality. | Improving public sector health human resources and increasing coverage of institutional births, as well as increasing public spending on health. |
| Yego et al. [21] | Kenya | Retrospective case-control study/fetal deaths and live births. | Cases were early fetal and neonatal deaths (n = 200) and controls were newborns alive immediately before and after the cases (n = 400) | - Birth attendant qualifications; gestational age; and number of prenatal visits. - Maternal complications at birth (hemorrhage and dystocia). - Congenital malformations and low five-minute Apgar scores. | - Education of mothers on prenatal consultation, screening, monitoring, and management of maternal conditions during the prenatal period should be strengthened. - The presence of a physician at every delivery and emergency admission is critical to ensuring early infant survival and avoiding potential risk factors for mortality. - The development of protocols for the management of newborns and regular audits based on criteria to prevent early neonatal mortality. |
| Batista et al. [22] | Brazil | Case control study/ population of live births in 2008. | 1772 controls for 412 cases | - Socioeconomic level. - Mother with a history of fetal loss. - Time to find health services before delivery. - Absence of a health care professional at the time of delivery. - Congenital malformations. - Prematurity. - Regional and intra-national inequality. | - Adequate and high-quality prenatal care, guaranteed access to a maternity hospital before birth, timely care for the parturient woman, and competent hospital care for the mother and baby. - Investment in health-care organization, such as expanding the number of beds in critical care units and neonatal intensive care units. |
| Ahmed et al. [23] | South Asia/Sub-Saharan Africa | Multi-country prospective cohort study from 2012 to 2016/women of reproductive age (15–49 years) in Sub-Saharan Africa and South Asia. | 278,186 pregnancies and 263,563 births | - Perinatal asphyxia. - Severe neonatal infections. - Complications of prematurity. | -Programs in sub-Saharan Africa and South Asia should intensify efforts to reduce mortality rates. -Access to high-quality, standardized, population-based prospective studies to quantify the burden, causes, and timing of deaths, including neonatal deaths. Training and advocacy workshops. |
| Garcia et al. [24] | Brazil | Cohort study: The study was based on a historical cohort of live births, developed as part of the epidemiological surveillance activities of the Municipal Health Secretariat in 2016 in Brazil/live births. | 15,879 live births | -Risk factors related to behavior and health service use (number of prenatal visits, type of health service, and type of delivery). -Apgar score and biological risk factors (sex, identified malformation, birth weight, weeks of pregnancy, identified malformation, type of pregnancy, maternal age). | The authors did not suggest any recommendations. |
| de Souza et al. [25] | Brazil | Case-control study/ neonatal deaths in Foz do Iguassu (Brazil) from 2012 to 2016. | 25,563 births | -Factors associated with neonatal death were congenital fetal anomalies; low birth weight, first minute Apgar score less than 7, and prematurity. | The implications for practice that can be drawn from the study include the following: - Prenatal surveillance should be increased, and hospital treatment for pregnant women and newborns should be prioritized. - Future studies on the quality of prenatal, delivery, and early postpartum care, preterm risk factors, the influence of cross-border patients on birthing indicators, and the epidemiology of birth anomalies on the international border are needed. |
| Ferraz et al. [26] | Portugal | Retrospective case-control study/medical records of all vaginal deliveries between January 2012 and December 2016. | Two control groups including 1802 spontaneous deliveries and 909 forceps-assisted deliveries | -The risk of soft tissue trauma, cephalohematoma, jaundice, intensive phototherapy, and transitory brachial plexus injury. | The authors did not suggest any recommendations. |
| Barquiel et al. [27] | Spain | Retrospective observational study/newborns of women with gestational diabetes. | Neonates born to 3413 women with gestational diabetes | -Factors associated with gestational diabetes mellitus (severity of hyperglycemia at diagnosis, glycemic control, and gestational weight gain). -Weight of the newborn. -Gestational weight gain of the mother was a factor for neonates born small for gestational age (SGA). | -The prevalence of SGA should be added to the rate of LGSs and cesarean sections in future studies of DG-related complications. - Diabetes screening methods for mothers whose fetuses are growing slowly should be developed. - Once GDM is identified, dietary changes and obstetric care should be followed to lower the risk of SGA complications. |
| Grünebaum et al. [28] | United States | Retrospective study/ infant births and deaths for 2010 to 2017. | CDC10-related infant birth and death records for 2010 to 2017 | -The location of the birth. -The nature of the birth attendant. | -Neonatal mortality can be significantly optimized by planning hospital births. |
| Guinsburg et al. [29] | Brazil | Retrospective study/ population of live births and deaths from 0 to 27 days in 2004–2013 in the region of Sao Paulo. | All children born in the state of São Paulo to mothers residing in the state in 2004–2013 were included | - Respiratory disorders. - Congenital malformations. - Infections. - Perinatal asphyxia. - Birth year, mother education level, marital status, maternal age, and multiple pregnancies. - Prenatal/delivery care. - Delay in obtaining appropriate care. | - Access to skilled health care should be prioritized to minimize newborn mortality in São Paulo. |
| Chang et al. [30] | Taiwan | Retrospective cohort study/ all live-born infants of a single birth, with a birth weight between 500 and 1499 g and a gestational age of 22 completed weeks, born between 2011 and 2014. | 4560 very low birth weight infants (VLBW) | Gender, low birth weight, gestational age of the infant, and maternal age. Non-medical assistance and hospitalization of an early birth (of gestational age infants). Birth in a non-tertiary hospital and postnatal transfer. Intrapartum transfer of pregnant women. Lack of coordination between obstetric and neonatal services. | -Tertiary facility birth may reduce neonatal mortality rates. -A policy of delivering low body weight infants in medical centers could potentially further reduce neonatal and infant mortality. Avoiding the transfer of women during the intrapartum period. - Avoiding transfer of infants at gestational age. - Provide neonatal intensive care units in rural areas. |
| Islam and Biswas [31] | Bangladesh | Mixed study (cross-sectional and meta-analysis)/ | Sample of 21 developing countries including Bangladesh | -Micro: biological/demographic factors, socioeconomic status, health care system, cultural practices, and technologies were key determinants of neonatal death and the interactions among its variables. -Macro: the socioeconomic condition of a country, the effectiveness. and efficiency of health care systems. | -Higher education for parents. -Improving the economic status of parents. -Superior birth rank. -Delivery at an age above 19 years. -Care during the neonatal period can all reduce neonatal mortality. |
| Eyeberu et al. [32] | Ethiopia | A cross-sectional study/ newborns. | 834 neonates | -Antepartum hemorrhage, pregnancy-induced hypertension, and type of pregnancy. - Low birth weight, perinatal asphyxia, and early onset neonatal sepsis. | - Improve care for all newborns, with a specific emphasis on high-risk neonates, and focus on factors that affect neonatal survival to minimize neonatal death. |
| Hambisa et al. (2023) [7] | Ethiopia | Systematic review and meta-analysis of studies delineating preterm mortality and associated factors. | 17 studies | Preterm mortality associated with neonatal sepsis, respiratory distress syndrome, and perinatal asphyxia. Kangaroo Mother Care significantly reduced mortality. | Kangaroo Mother Care; improving preterm neonatal healthcare system; and community-based healthcare strategies. |
| Alabi et al. [33] | Sub-Saharan Africa | Literature review of the impact of COVID-19 on maternal and child health. | Not specified | The COVID-19 pandemic increased maternal and child mortality, highlighting the importance of antenatal care and preparedness for health crises. | Prioritizing women’s antenatal care and developing policies for health crises and emerging diseases. |
| Sampurna et al. [34] | Indonesia | National survey data analysis of 10,838 live-born infants from singleton pregnancies in 2017. | 10,838 live-born infants | Lack of postnatal care and delivery complications (other than prolonged labor) associated with increased neonatal death; low birth weight infants at higher risk. | Improving quality and services of public hospitals and equitable distribution of healthcare services. |
| Categories of Factros | Factors |
|---|---|
| Socioeconomic factors |
|
| Clinical factors |
|
| Healthcare access and quality |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nabila, M.; Baidani, A.; Mourajid, Y.; Chebabe, M.; Abderraouf, H. Analysis of Risk Determinants of Neonatal Mortality in the Last Decade: A Systematic Literature Review (2013–2023). Pediatr. Rep. 2024, 16, 696-716. https://doi.org/10.3390/pediatric16030059
Nabila M, Baidani A, Mourajid Y, Chebabe M, Abderraouf H. Analysis of Risk Determinants of Neonatal Mortality in the Last Decade: A Systematic Literature Review (2013–2023). Pediatric Reports. 2024; 16(3):696-716. https://doi.org/10.3390/pediatric16030059
Chicago/Turabian StyleNabila, Msatfa, Aziz Baidani, Yassmine Mourajid, Milouda Chebabe, and Hilali Abderraouf. 2024. "Analysis of Risk Determinants of Neonatal Mortality in the Last Decade: A Systematic Literature Review (2013–2023)" Pediatric Reports 16, no. 3: 696-716. https://doi.org/10.3390/pediatric16030059
APA StyleNabila, M., Baidani, A., Mourajid, Y., Chebabe, M., & Abderraouf, H. (2024). Analysis of Risk Determinants of Neonatal Mortality in the Last Decade: A Systematic Literature Review (2013–2023). Pediatric Reports, 16(3), 696-716. https://doi.org/10.3390/pediatric16030059