
The Psychosocial Impact of the COVID-19 Pandemic on Italian Families: The Perception of Quality of Life and Screening of Psychological Symptoms



Abstract
1. Introduction
Aims
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Instruments
2.3.1. Sociodemographic Questionnaire
2.3.2. Revised Children’s Manifest Anxiety Scale—Second Edition
2.3.3. ChIA
2.3.4. PedsQoL 3.0 Multidimensional Fatigue Scale
2.4. Plan of Statistical Analyses
3. Results
3.1. Perceptions of Anxiety, Anger, and Quality of Life of Children and Adolescents Compared to Norms
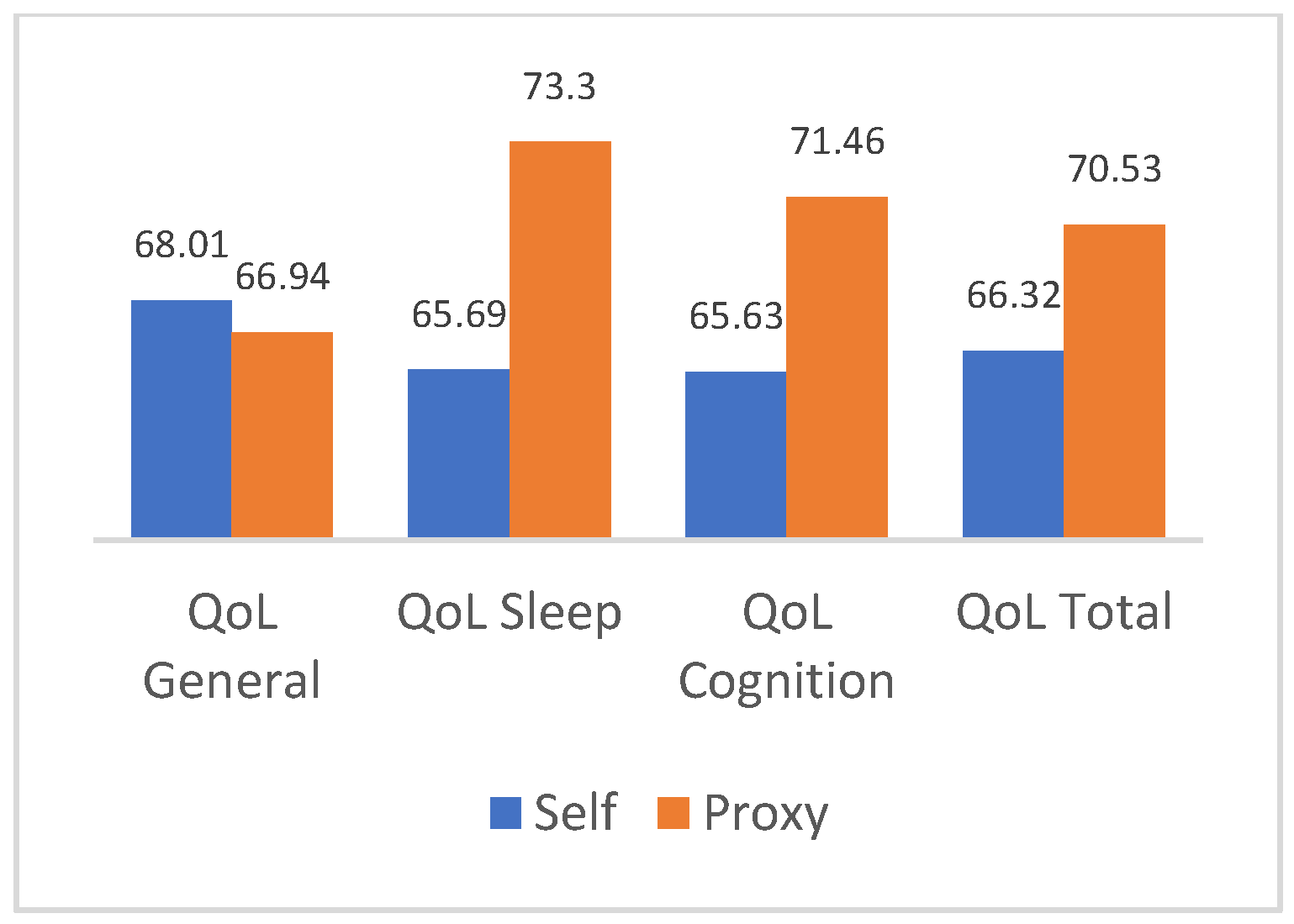
3.2. Comparison of Quality of Life Scores between Parents and Children
3.3. What Are the Factors That Influence Anxiety Symptoms in Children and Adolescents?
3.4. What Are the Factors That Influence the Perceived Quality of Life of Children and Adolescents?
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Balenzano, C.; Moro, G.; Girardi, S. Families in the pandemic between challenges and opportunities: An empirical study of parents with preschool and school-age children. Ital. Sociol. Rev. 2020, 10, 777–800. [Google Scholar]
- Petts, R.J.; Carlson, D.L.; Pepin, J.R. A gendered pandemic: Childcare, homeschooling, and parents’ employment during COVID-19. Gend. Work Organ. 2020, 28, 515–534. [Google Scholar] [CrossRef]
- Johnson, M.S.; Skjerdingstad, N.; Ebrahimi, O.V.; Hoffart, A.; Johnson, S.U. Parenting in a pandemic: Parental stress, anxiety and depression among parents during the government-initiated physical distancing measures following the first wave of COVID-19. Stress Health 2022, 38, 637–652. [Google Scholar] [CrossRef] [PubMed]
- Yamamura, E.; Tsustsui, Y. The impact of closing schools on working from home during the COVID-19 pandemic: Evidence using panel data from Japan. Rev. Econ. Househ. 2021, 19, 41–60. [Google Scholar] [CrossRef]
- Spinelli, M.; Lionetti, F.; Pastore, M.; Fasolo, M. Parents’ stress and children’s psychological problems in families facing the COVID-19 outbreak in Italy. Front. Psychol. 2020, 11, 1713. [Google Scholar] [CrossRef]
- Cerniglia, L.; Cimino, S.; Ammaniti, M. L’impatto del periodo di isolamento legato al COVID-19 nello sviluppo psicologico infantile. Psicol. Clin. Dello Svilupp. 2020, 24, 187–190. [Google Scholar]
- Ravens-Sieberer, U.; Erhart, M.; Devine, J.; Gilbert, M.; Reiss, F.; Barkmann, C.; Kaman, A. Child and adolescent mental health during the COVID-19 pandemic: Results of the three-wave longitudinal COPSY study. J. Adolesc. Health 2022, 71, 570–578. [Google Scholar] [CrossRef]
- Arnett, J.J. The Oxford Handbook of Emerging Adulthood, 3rd ed.; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Orben, A.; Tomova, L.; Blakemore, S.J. The effects of social deprivation on adolescent development and mental health. Lancet Child Adolesc. Health 2020, 4, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Orban, E.; Li, L.Y.; Gilbert, M.; Napp, A.K.; Kaman, A.; Topf, S.; Boecker, M.; Devine, J.; Reiß, F.; Wendel, F.; et al. Mental health and quality of life in children and adolescents during the COVID-19 pandemic: A systematic review of longitudinal studies. Front. Public Health 2024, 11, 1275917. [Google Scholar] [CrossRef]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: A meta-analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef]
- Feng, Z.; Xu, L.; Cheng, P.; Zhang, L.; Li, L.-J.; Li, W.-H. The psychological impact of COVID-19 on the families of first-line rescuers. Indian J. Psychiatry 2020, 62 (Suppl. 3), S438–S444. [Google Scholar] [PubMed]
- Ferreira, L.N.; Pereira, L.N.; da Fé Brás, M.; Ilchuk, K. Quality of life under the COVID-19 quarantine. Qual. Life Res. 2021, 30, 1389–1405. [Google Scholar] [CrossRef] [PubMed]
- Eiser, C.; Varni, J.W. Health-related quality of life and symptom reporting: Similarities and differences between children and their parents. Eur. J. Pediatr. 2013, 172, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Khanna, D.; Khadka, J.; Mpundu-Kaambwa, C.; Lay, K.; Russo, R.; Ratcliffe, J. Are we agreed? Self-versus proxy-reporting of pediatric health-related quality of life (HRQoL) using generic preference-based measures: A systematic review and meta-analysis. Pharmacoeconomics 2022, 40, 1043–1067. [Google Scholar] [CrossRef] [PubMed]
- Matza, L.S.; Patrick, D.L.; Riley, A.W.; Alexander, J.J.; Rajmil, L.; Pleil, A.M.; Bullinger, M. Pediatric patient-reported outcome instruments for research to support medical product labeling: Report of the ISPOR PRO good research practices for the assessment of children and adolescents task force. Value Health 2013, 16, 461–479. [Google Scholar] [CrossRef] [PubMed]
- Roddenberry, A.; Renk, K. Quality of life in pediatric cancer patients: The relationships among parents’ characteristics, children’s characteristics, and informant concordance. J. Child Fam. Stud. 2008, 17, 402–426. [Google Scholar] [CrossRef]
- Otero, S.; Eiser, C.; Wright, N.; Butler, G. Implications of parent and child quality of life assessments for decisions about growth hormone treatment in eligible children. Child Care Health Dev. 2013, 39, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Brazier, J.; Ratcliffe, J.; Saloman, J.; Tsuchiya, A. Measuring and Valuing Health Benefits for Economic Evaluation, 2nd ed.; University Press: Oxford, UK, 2016. [Google Scholar]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2022, 31, 879–889. [Google Scholar] [CrossRef] [PubMed]
- De Bles, N.J.; Ottenheim, N.R.; van Hemert, A.M.; Pütz, L.E.; van der Does, A.W.; Penninx, B.W.; Giltay, E.J. Trait anger and anger attacks in relation to depressive and anxiety disorders. J. Affect. Disord. 2019, 259, 259–265. [Google Scholar] [CrossRef]
- Cox, D.E.; Harrison, D.W. Models of anger: Contributions from psychophysiology, neuropsychology and the cognitive behavioral perspective. Brain Struct. Funct. 2008, 212, 371–385. [Google Scholar] [CrossRef]
- Bozzola, E.; Ferrara, P.; Spina, G.; Villani, A.; Roversi, M.; Raponi, M.; Corsello, G.; Staiano, A. The pandemic within the pandemic: The surge of neuropsychological disorders in Italian children during the COVID-19 era. Ital. J. Pediatr. 2022, 48, 126. [Google Scholar] [CrossRef] [PubMed]
- Ludwig-Walz, H.; Dannheim, I.; Pfadenhauer, L.M.; Fegert, J.M.; Bujard, M. Anxiety among children and adolescents during the COVID-19 pandemic in Europe: A systematic review protocol. Syst. Rev. 2023, 12, 64. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, D.; Fontanesi, L.; Mazza, C.; Di Giandomenico, S.; Roma, P.; Verrocchio, M.C. Parenting-related exhaustion during the Italian COVID-19 lockdown. J. Pediatr. Psychol. 2020, 45, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Polizzi, C.; Burgio, S.; Lavanco, G.; Alesi, M. Parental Distress and Perception of Children’s Executive Functioning after the First COVID-19 Lockdown in Italy. J. Clin. Med. 2021, 10, 4170. [Google Scholar] [CrossRef] [PubMed]
- Mocho, H.; Martins, C.; dos Santos, R.; Nunes, C. Parental Involvement and Stress in Children’s Quality of Life: A Longitudinal Study with Portuguese Parents during the COVID-19 Pandemic Period. Children 2024, 11, 440. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.R.; Richmond, B.O. Revised Children’s Manifest Anxiety Scale: Second Edition (RCMAS-2); WPS Online Evaluation System: Los Angeles, CA, USA, 2008. [Google Scholar]
- Filce, H.G.; LaVergne, L. Absenteeism, educational plans, and anxiety among children with incontinence and their parents. J. Sch. Health 2015, 85, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Nelson, W.M.; Finch, A.J. Children’s Inventory of Anger (ChIA); Western Psychological Services: Los Angeles, CA, USA, 2000. [Google Scholar]
- Varni, J.W.; Burwinkle, T.M.; Katz, E.R.; Meeske, K.; Dickinson, P. The PedsQL™ in pediatric cancer: Reliability and validity of the pediatric quality of life inventory™ generic core scales, multidimensional fatigue scale, and cancer module. Cancer 2002, 94, 2090–2106. [Google Scholar] [CrossRef]
- Reid, J.A.; Chenneville, T.; Gardy, S.M.; Baglivio, M.T. An exploratory study of COVID-19′s impact on psychological distress and antisocial behavior among justice-involved youth. Crime Delinq. 2022, 68, 1271–1291. [Google Scholar] [CrossRef]
- Walsh, L.M.; Benjamin Wolk, C.; Becker-Haimes, E.M.; Jensen-Doss, A.; Beidas, R.S. The relationship between anger and anxiety symptoms in youth with anxiety disorders. J. Child Adolesc. Couns. 2018, 4, 117–133. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Cisler, J.M.; Tolin, D.F. Quality of life in the anxiety disorders: A meta-analytic review. Clin. Psychol. Rev. 2007, 27, 572–581. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Statistics | Frequencies | ||||||
|---|---|---|---|---|---|---|---|
| Min | Max | M | SD | ||||
| Children’s Age | 6 | 16 | 12.44 | 2.74 | |||
| Children’s Gender | Male Female | 60 71 | 45.8% 54.2% | ||||
| Children’s School Level | Primary School Secondary School, 1st Secondary School, 2nd | 35 50 46 | 26.7% 38.2% 35.1% | ||||
| Parental Age | 30 | 66 | 46.46 | 6.02 | |||
| Parent’s Gender | Male Female | 26 105 | 19.8% 80.2% | ||||
| Parental Schooling Years | 5 | 20 | 13.82 | 3.42 | |||
| Parental Civil Status | Single Parent Two Parents | 10 121 | 7.6% 92.4% | ||||
| Parental Perceived Economic Condition | Low Medium High | 23 72 36 | 16.6% 55.0% 27.5% | ||||
| QoL General | QoL Sleep | QoL Cognition | Total QoL Total | |||||
|---|---|---|---|---|---|---|---|---|
| Freq. | Perc. | Freq. | Perc. | Freq. | Perc. | Freq. | Perc. | |
| Very Low QOL | 1 | 0.8% | 6 | 4.6% | 6 | 4.6% | 0 | 0% |
| Low Quality of Life | 21 | 16% | 19 | 14.5% | 21 | 16% | 14 | 10.7% |
| Moderate QoL | 72 | 55% | 75 | 57.3% | 65 | 49.6% | 88 | 67.2% |
| Good QoL | 37 | 28.2% | 31 | 23.7% | 39 | 29.8% | 29 | 22.1% |
| Total | 131 | 100% | 131 | 100% | 131 | 100% | 131 | 100% |
| QoL General | QoL Sleep | QoL Cognition QoL Total | ||||||
|---|---|---|---|---|---|---|---|---|
| Freq. | Perc. | Freq. | Perc. | Freq. | Perc. | Freq. | Perc. | |
| Very Low QOL | 8 | 6.1% | 0 | 0% | 4 | 3.1% | 1 | 0.8% |
| Low QoL | 36 | 27.5% | 16 | 12.2% | 30 | 22.9% | 25 | 19.1% |
| Moderate QoL | 66 | 50.4% | 67 | 51.1% | 50 | 38.2% | 76 | 58% |
| Good QoL | 21 | 16% | 48 | 36.6% | 47 | 35.9% | 29 | 22.1% |
| Total | 131 | 100% | 131 | 100% | 131 | 100% | 131 | 100% |
| Model | Anova a | Coefficients a | |||||
|---|---|---|---|---|---|---|---|
| R-Square | Df | F | p | Beta | T | P | |
| Model | 0.15 | 3 | 7.6 | 0.0001 b | |||
| Sex | 0.22 | 2.68 | 0.008 * | ||||
| Parents of PEDS TOT Self-Report | −0.197 | −2.40 | 0.018 * | ||||
| Total Anger | 0.24 | 2.93 | 0.004 * | ||||
| Model | Anova a | Coefficients a | |||||
|---|---|---|---|---|---|---|---|
| R-Square | Df | F | p | Beta | T | P | |
| Model | 0.33 | 2 | 31.67 | 0.0001 b | |||
| Physiological Anxiety | −0.34 | −4.12 | 0.0001 * | ||||
| Social Anxiety | −0.32 | −3.90 | 0.0001 * | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Incardona, R.M.; Tremolada, M. The Psychosocial Impact of the COVID-19 Pandemic on Italian Families: The Perception of Quality of Life and Screening of Psychological Symptoms. Pediatr. Rep. 2024, 16, 519-529. https://doi.org/10.3390/pediatric16020043
Incardona RM, Tremolada M. The Psychosocial Impact of the COVID-19 Pandemic on Italian Families: The Perception of Quality of Life and Screening of Psychological Symptoms. Pediatric Reports. 2024; 16(2):519-529. https://doi.org/10.3390/pediatric16020043
Chicago/Turabian StyleIncardona, Roberta Maria, and Marta Tremolada. 2024. "The Psychosocial Impact of the COVID-19 Pandemic on Italian Families: The Perception of Quality of Life and Screening of Psychological Symptoms" Pediatric Reports 16, no. 2: 519-529. https://doi.org/10.3390/pediatric16020043
APA StyleIncardona, R. M., & Tremolada, M. (2024). The Psychosocial Impact of the COVID-19 Pandemic on Italian Families: The Perception of Quality of Life and Screening of Psychological Symptoms. Pediatric Reports, 16(2), 519-529. https://doi.org/10.3390/pediatric16020043