The Efficacy of Tofogliflozin on Metabolic Dysfunction-Associated Fatty Liver Disease

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Statistical Analysis
3. Result
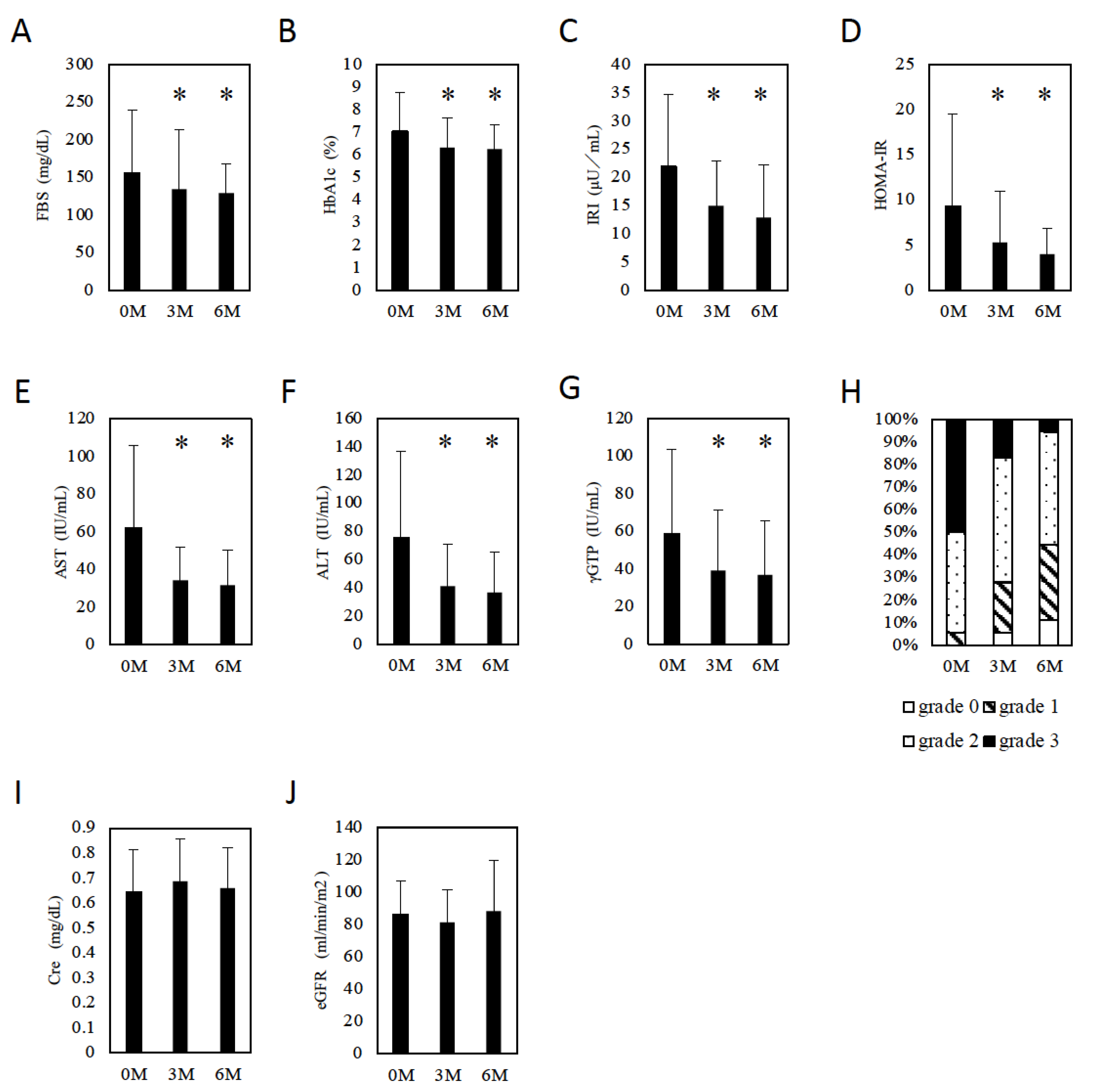
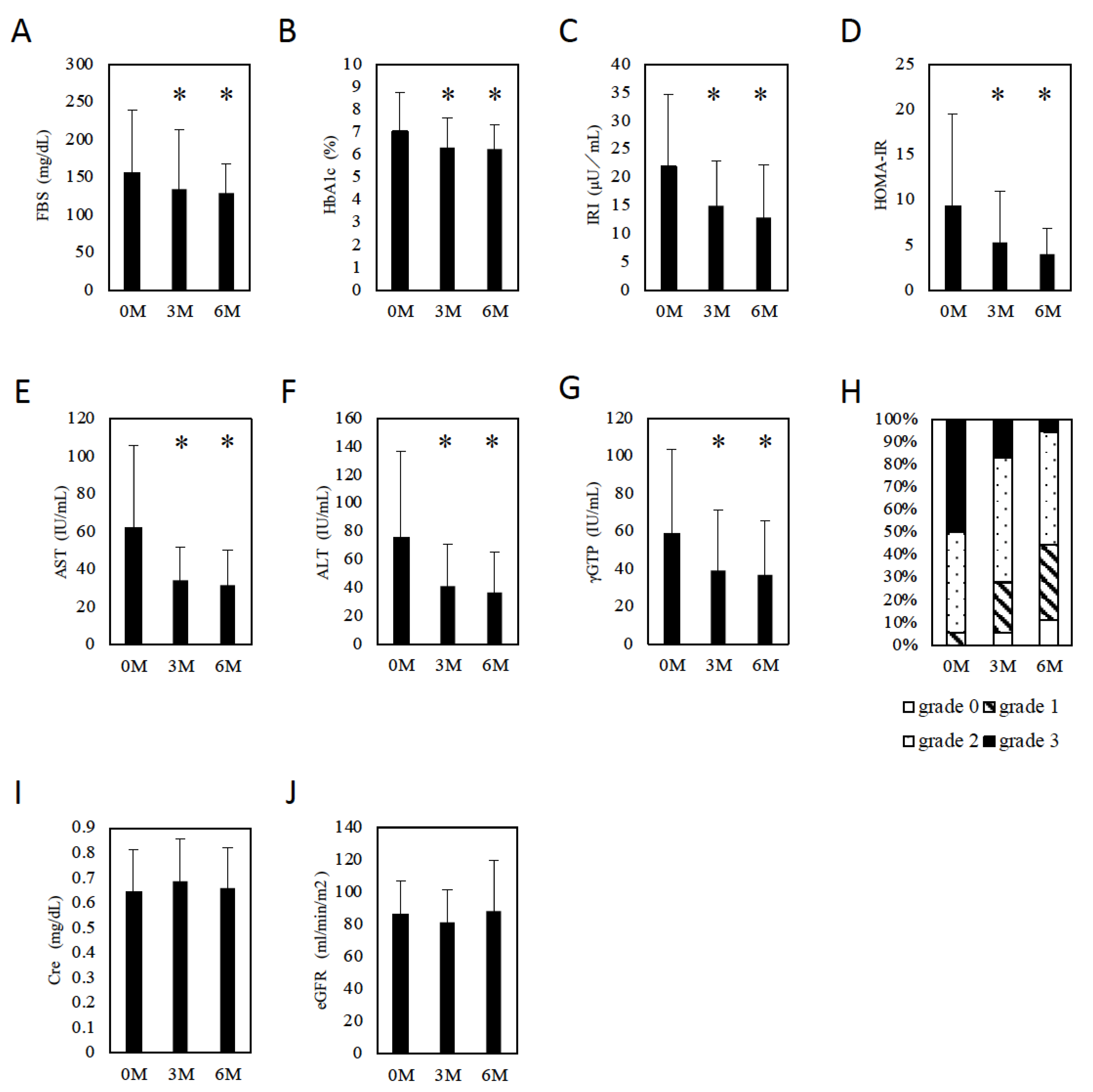
3.1. The Effect of Tofogliflozin on Glucose Metabolism and Hepatic Steatosis
3.2. The Effect of Tofogliflozin on Body Composition
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eslam, M.; Sanyal, A.J.; George, J. International Consensus Panel. MAFLD: A consensus-driven proposed nomenclature for met-abolic associated fatty liver disease. Gastroenterology 2020, 158, 1999–2014. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wong, V.W.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dys-function-associated fatty liver disease: An international expert consensus statement. J. Heptol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Saadeh, S.; Younossi, Z.M.; Remer, E.M.; Gramlich, T.; Ong, J.P.; Hurley, M.; Mullen, K.D.; Cooper, J.N.; Sheridan, M.J. The utility of radiological imaging in nonalcoholic fatty liver disease. Gastroenterology 2002, 123, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Ito, D.; Shimizu, S.; Inoue, K.; Saito, D.; Yanagisawa, M.; Inukai, K.; Akiyama, Y.; Morimoto, Y.; Noda, M.; Shimada, A. Comparison of Ipragliflozin and Pioglitazone Effects on Nonalcoholic Fatty Liver Disease in Patients With Type 2 Diabetes: A Randomized, 24-Week, Open-Label, Active-Controlled Trial. Diabetes Care 2017, 40, 1364–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibuya, T.; Fushimi, N.; Kawai, M.; Yoshida, Y.; Hachiya, H.; Ito, S.; Kawai, H.; Ohashi, N.; Mori, A. Luseogliflozin improves liver fat deposition compared to metformin in type 2 diabetes patients with non-alcoholic fatty liver disease: A prospective randomized controlled pilot study. Diabetes Obes. Metab. 2017, 20, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Farooqui, K.J.; Singh, M.K.; Wasir, J.S.; Bansal, B.; Kaur, P.; Jevalikar, G.; Gill, H.K.; et al. Effect of Empagliflozin on Liver Fat in Patients With Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes Care 2018, 41, 1801–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksson, J.W.; Lundkvist, P.; Jansson, P.A.; Johansson, L.; Kvarnström, M.; Moris, L.; Miliotis, T.; Forsberg, G.B.; Risérus, U.; Lind, L.; et al. Effects of dapagliflozin and n-3 carboxylic acids on non-alcoholic fatty liver disease in people with type 2 diabetes: A double-blind randomised place-bo-controlled study. Diabetologia 2018, 61, 1923–1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, M.; Suzuki, K.; Kato, K.; Jojima, T.; Iijima, T.; Murohisa, T.; Iijima, M.; Takekawa, H.; Usui, I.; Hiraishi, H.; et al. Evaluation of the effects of dapagliflozin, a sodium-glucose co-transporter-2 inhibitor, on hepatic steatosis and fibrosis using transient elastography in patients with type 2 diabetes and non-alcoholic fatty liver disease. Diabetes Obes. Metab. 2018, 21, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Chrysavgis, L.; Papatheodorididi, A.M.; Chatzigeorgiou, A.; Cholongitas, E. The impact of sodium glucose co-transporter 2 inhibitors on non-alcoholic fatty liver disease. JGH 2021, 36, 893–909. [Google Scholar] [CrossRef] [PubMed]
- Koo, B.K.; Kim, D.; Joo, S.K.; Kim, J.H.; Chang, M.S.; Kim, B.G.; Lee, K.L.; Kim, W. Sarcopenia is an independent risk factor for non-alcoholic steatohepatitis and significant fibrosis. J. Hepatol. 2016, 66, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Umegaki, H. Sarcopenia and frailty in older patients with diabetes mellitus. Geriatr. Gerontol. Int. 2016, 16, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Kim, S.U.; Song, K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Lee, B.W.; Kang, E.S.; Cha, B.S.; Han, K.H. Sarcopenia is associated with significant liver fibrosis inde-pendently of obesity and insulin resistance in nonalcoholic fatty liver disease: Nationwide surveys (KNHANES 2008–2011). Hepatology 2016, 63, 776–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komiya, C.; Tsuchiya, K.; Shiba, K.; Miyachi, Y.; Furuke, S.; Shimazu, N.; Yamaguchi, S.; Kanno, K.; Ogawa, Y. Ipragliflozin Improves Hepatic Steatosis in Obese Mice and Liver Dysfunction in Type 2 Diabetic Patients Irrespective of Body Weight Reduction. PLoS ONE 2016, 11, e0151511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodine, S.C.; Stitt, T.N.; Gonzalez, M.; Kline, W.O.; Stover, G.L.; Bauerlein, R.; Zlotchenko, E.; Scrimgeour, A.; Lawrence, J.C.; Glass, D.J.; et al. Akt/mTOR pathway is a crucial regulator of skeletal muscle hypertrophy and can prevent muscle atrophy in vivo. Nat. Cell Biol. 2001, 3, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, B.T.; Lee, K.Y.; Klaus, K.; Softic, S.; Krumpoch, M.T.; Fentz, J.; Stanford, K.I.; Robinson, M.M.; Cai, W.; Kleinridders, A.; et al. Insulin and IGF-1 receptors regulate FoxO-mediated signaling in muscle proteostasis. J. Clin. Investig. 2016, 126, 3433–3446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaiswal, N.; Gavin, M.; Loro, E.; Sostre-Colón, J.; Roberson, P.A.; Uehara, K.; Rivera-Fuentes, N.; Neinast, M.; Arany, Z.; Kimball, S.R.; et al. AKT controls protein synthesis and oxidative metabolism via combined mTORC1 and FOXO1 signalling to govern muscle physiology. J. Cachex-Sarcopenia Muscle 2021. [Google Scholar] [CrossRef] [PubMed]
- Sakuma, K.; Yamaguchi, A. Sarcopenic Obesity and Endocrinal Adaptation with Age. Int. J. Endocrinol. 2013, 2013, 204164. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Factor | n = 18 |
|---|---|
| Age (y.o.) | 61.5 (48–71) |
| Gender (M/F) | 8/10 |
| BH (cm) | 160 (153–166) |
| BW (kg) | 68.0 (60.7–76.0) |
| BMI | 26.8 (23.7–29.9) |
| Disease duration of T2DM (year) | 1 (1–1.25) |
| Plt (/mL) | 21.1 (16.8–29.1) |
| Alb (g/dL) | 4.3 (4.1–4.5) |
| T-Bil (mg/dL) | 0.9 (0.6–1.1) |
| AST (IU/L) | 45 (34–93) |
| ALT (IU/L) | 53 (30–121) |
| g-GTP (IU/L) | 37 (24–113) |
| ALP (IU/L) | 222 (191–306) |
| CHE (IU/L) | 364 (334–460) |
| T-Chol (mg/dL) | 204 (157–225) |
| TG (mg/dL) | 115 (90–156) |
| HDL-C (mg/dL) | 50.5 (43.3–55.8) |
| LDL-C (mg/dL) | 124 (90–142) |
| FBS (mg/dL) | 120 (116–163) |
| HbA1c (%) | 6.4 (5.9–7.4) |
| IRI (IU/L) | 19.6 (12.1–31.8) |
| HOMA-IR | 6.0 (3.7–11.3) |
| Cre (mg/dL) | 0.66 (0.49–0.77) |
| eGFR (mL/min/m2) | 81.5 (71.8–100.3) |
| Comorbidity | |
| HBV | 3 |
| HCV | 1 |
| AIH | 0 |
| PBC | 1 |
| Treatment | |
| Sulfonylurea | 1 |
| Biguanide | 1 |
| DPP4 inhibitor | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goya, T.; Imoto, K.; Tashiro, S.; Aoyagi, T.; Takahashi, M.; Kurokawa, M.; Suzuki, H.; Tanaka, M.; Kato, M.; Kohjima, M.; et al. The Efficacy of Tofogliflozin on Metabolic Dysfunction-Associated Fatty Liver Disease. Gastroenterol. Insights 2022, 13, 20-26. https://doi.org/10.3390/gastroent13010003
Goya T, Imoto K, Tashiro S, Aoyagi T, Takahashi M, Kurokawa M, Suzuki H, Tanaka M, Kato M, Kohjima M, et al. The Efficacy of Tofogliflozin on Metabolic Dysfunction-Associated Fatty Liver Disease. Gastroenterology Insights. 2022; 13(1):20-26. https://doi.org/10.3390/gastroent13010003
Chicago/Turabian StyleGoya, Takeshi, Koji Imoto, Shigeki Tashiro, Tomomi Aoyagi, Motoi Takahashi, Miho Kurokawa, Hideo Suzuki, Masatake Tanaka, Masaki Kato, Motoyuki Kohjima, and et al. 2022. "The Efficacy of Tofogliflozin on Metabolic Dysfunction-Associated Fatty Liver Disease" Gastroenterology Insights 13, no. 1: 20-26. https://doi.org/10.3390/gastroent13010003
APA StyleGoya, T., Imoto, K., Tashiro, S., Aoyagi, T., Takahashi, M., Kurokawa, M., Suzuki, H., Tanaka, M., Kato, M., Kohjima, M., & Ogawa, Y. (2022). The Efficacy of Tofogliflozin on Metabolic Dysfunction-Associated Fatty Liver Disease. Gastroenterology Insights, 13(1), 20-26. https://doi.org/10.3390/gastroent13010003