
Monocyte to HDL and Neutrophil to HDL Ratios as Potential Ischemic Stroke Prognostic Biomarkers

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Data Analysis
3. Results
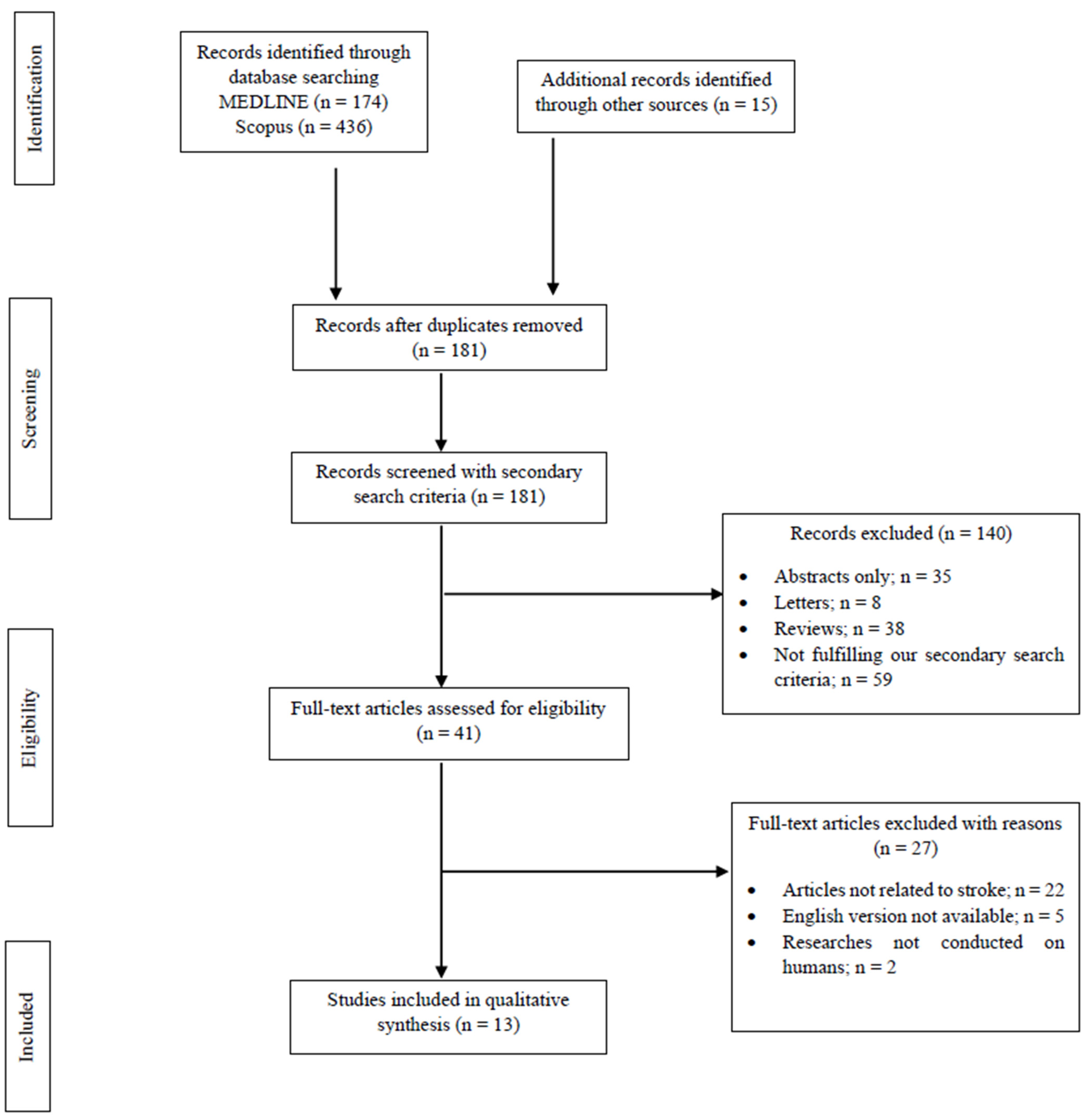
3.1. Database Searches
3.2. Study Characteristics
3.3. Study Design
3.4. Stroke Patients Group
3.5. Reference Groups
3.6. Demographic and Clinical Profiles
3.7. Time of Blood Sampling
3.8. Scales of Stroke Severity and Prognosis/Clinical Outcome
4. Discussion
4.1. Neutrophils-to-HDL-Ratio (NHR)
4.2. Monocyte-to-HDL Ratio (MHR)
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Donkor, E.S. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res. Treat. 2018, 2018, 3238165. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef]
- De Marchis, G.M.; Dittrich, T.D. Blood Biomarkers in the Diagnosis of Acute Stroke. In Precision Medicine in Stroke; Fonseca, A.C., Ferro, J.M., Eds.; Springer: Cham, Switzerland, 2021; pp. 163–189. [Google Scholar]
- Grefkes, C.; Fink, G.R. Recovery from stroke: Current concepts and future perspectives. Neurol. Res. Pract. 2020, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- Gkantzios, A.; Tsiptsios, D.; Karatzetzou, S.; Kitmeridou, S.; Karapepera, V.; Giannakou, E.; Vlotinou, P.; Aggelousis, N.; Vadikolias, K. Stroke and Emerging Blood Biomarkers: A Clinical Prospective. Neurol. Int. 2022, 14, 784–803. [Google Scholar] [CrossRef] [PubMed]
- Saver, J.L. Time is brain—Quantified. Stroke 2006, 37, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Sousanidou, A.; Tsiptsios, D.; Christidi, F.; Karatzetzou, S.; Kokkotis, C.; Gkantzios, A.; Bairaktaris, C.; Karapepera, V.; Bebeletsi, P.; Karagiannakidou, I.; et al. Exploring the Impact of Cerebral Microbleeds on Stroke Management. Neurol. Int. 2023, 15, 188–224. [Google Scholar] [CrossRef]
- Karatzetzou, S.; Tsiptsios, D.; Sousanidou, A.; Fotiadou, S.; Christidi, F.; Kokkotis, C.; Gkantzios, A.; Stefas, E.; Vlotinou, P.; Kaltsatou, A.; et al. Copeptin Implementation on Stroke Prognosis. Neurol. Int. 2023, 15, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Christidi, F.; Tsiptsios, D.; Fotiadou, A.; Kitmeridou, S.; Karatzetzou, S.; Tsamakis, K.; Sousanidou, A.; Psatha, E.A.; Karavasilis, E.; Seimenis, I.; et al. Diffusion Tensor Imaging as a Prognostic Tool for Recovery in Acute and Hyperacute Stroke. Neurol. Int. 2022, 14, 841–874. [Google Scholar] [CrossRef]
- Quinn, T.J.; Singh, S.; Lees, K.R.; Bath, P.M.; Myint, P.K.; VISTA Collaborators. Validating and comparing stroke prognosis scales. Neurology 2017, 89, 997–1002. [Google Scholar] [CrossRef]
- Karatzetzou, S.; Tsiptsios, D.; Terzoudi, A.; Aggeloussis, N.; Vadikolias, K. Transcranial magnetic stimulation implementation on stroke prognosis. Neurol. Sci. 2022, 43, 873–888. [Google Scholar] [CrossRef] [PubMed]
- Gkantzios, A.; Kokkotis, C.; Tsiptsios, D.; Moustakidis, S.; Gkartzonika, E.; Avramidis, T.; Aggelousis, N.; Vadikolias, K. Evaluation of Blood Biomarkers and Parameters for the Prediction of Stroke Survivors’ Functional Outcome upon Discharge Utilizing Explainable Machine Learning. Diagnostics 2023, 13, 532. [Google Scholar] [CrossRef] [PubMed]
- Colombo, P.E.; Quenet, F.; Alric, P.; Mourregot, A.; Neron, M.; Portales, F.; Rouanet, P.; Carrier, G. Distal Pancreatectomy with Celiac Axis Resection (Modified Appleby Procedure) and Arterial Reconstruction for Locally Advanced Pancreatic Adenocarcinoma After FOLFIRINOX Chemotherapy and Chemoradiation Therapy. Ann. Surg. Oncol. 2021, 28, 1106–1108. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S. Biomarkers of cardiovascular disease: Molecular basis and practical considerations. Circulation 2006, 113, 2335–2362. [Google Scholar] [CrossRef]
- Makris, K.; Haliassos, A.; Chondrogianni, M.; Tsivgoulis, G. Blood biomarkers in ischemic stroke: Potential role and challenges in clinical practice and research. Crit. Rev. Clin. Lab. Sci. 2018, 55, 294–328. [Google Scholar] [CrossRef]
- Andone, S.; Bajko, Z.; Motataianu, A.; Mosora, O.; Balasa, R. The Role of Biomarkers in Atherothrombotic Stroke—A Systematic Review. Int. J. Mol. Sci. 2021, 22, 9032. [Google Scholar] [CrossRef]
- Garcia-Bonilla, L.; Moore, J.M.; Racchumi, G.; Zhou, P.; Butler, J.M.; Iadecola, C.; Anrather, J. Inducible nitric oxide synthase in neutrophils and endothelium contributes to ischemic brain injury in mice. J. Immunol. 2014, 193, 2531–2537. [Google Scholar] [CrossRef]
- Fassbender, K.; Rossol, S.; Kammer, T.; Daffertshofer, M.; Wirth, S.; Dollman, M.; Hennerici, M. Proinflammatory cytokines in serum of patients with acute cerebral ischemia: Kinetics of secretion and relation to the extent of brain damage and outcome of disease. J. Neurol. Sci. 1994, 122, 135–139. [Google Scholar] [CrossRef]
- Chamorro, A.; Hallenbeck, J. The harms and benefits of inflammatory and immune responses in vascular disease. Stroke 2006, 37, 291–293. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, J.; Chang, J.Y.; Kim, S.H.; Lee, J.E. Inflammation after Ischemic Stroke: The Role of Leukocytes and Glial Cells. Exp. Neurobiol. 2016, 25, 241–251. [Google Scholar] [CrossRef]
- Fu, Y.; Liu, Q.; Anrather, J.; Shi, F.D. Immune interventions in stroke. Nat. Rev. Neurol. 2015, 11, 524–535. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.-B.; Lu, Z.-X.; Zhu, F.; Jiang, C.-Q.; Zhang, W.-S.; Pan, J.; Jin, Y.-L.; Xu, L.; Thomas, G.N.; Cheng, K.; et al. Higher total white blood cell and neutrophil counts are associated with an increased risk of fatal stroke occurrence: The Guangzhou biobank cohort study. BMC Neurol. 2021, 21, 470. [Google Scholar] [CrossRef] [PubMed]
- Kazmierski, R.; Guzik, P.; Ambrosius, W.; Ciesielska, A.; Moskal, J.; Kozubski, W. Predictive value of white blood cell count on admission for in-hospital mortality in acute stroke patients. Clin. Neurol. Neurosurg. 2004, 107, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Algin, A.; Inan, I. The role of radiologic, clinical and biochemical parameters in prediction of stroke mortality. Neurosciences 2019, 24, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.; Shi, J.; Cao, Y.; Zhang, M.; Xu, J. Prognostic Value of White Blood Cell Counts and C-reactive Protein in Acute Ischemic Stroke Patients After Intravenous Thrombolysis. Curr. Neurovascular Res. 2018, 15, 10–17. [Google Scholar] [CrossRef]
- Ho, W.-M.; Lin, J.-R.; Wang, H.-H.; Liou, C.-W.; Chang, K.-C.; Lee, J.-D.; Peng, T.-Y.; Yang, J.-T.; Chang, Y.-J.; Chang, C.-H.; et al. Prediction of in-hospital stroke mortality in critical care unit. Springerplus 2016, 5, 1051. [Google Scholar] [CrossRef]
- Soehnlein, O. Multiple roles for neutrophils in atherosclerosis. Circ. Res. 2012, 110, 875–888. [Google Scholar] [CrossRef]
- Herz, J.; Sabellek, P.; Lane, T.E.; Gunzer, M.; Hermann, D.M.; Doeppner, T.R. Role of Neutrophils in Exacerbation of Brain Injury After Focal Cerebral Ischemia in Hyperlipidemic Mice. Stroke 2015, 46, 2916–2925. [Google Scholar] [CrossRef]
- Al-Mufti, F.; Amuluru, K.; Damodara, N.; Dodson, V.; Roh, D.; Agarwal, S.; Meyers, P.M.; Connolly, E.S.; Schmidt, M.J.; Claassen, J.; et al. Admission neutrophil-lymphocyte ratio predicts delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage. J. NeuroInterv. Surg. 2019, 11, 1135–1140. [Google Scholar] [CrossRef]
- Otxoa-de-Amezaga, A.; Gallizioli, M.; Pedragosa, J.; Justicia, C.; Miró-Mur, F.; Salas-Perdomo, A.; Díaz-Marugan, L.; Gunzer, M.; Planas, A.M. Location of Neutrophils in Different Compartments of the Damaged Mouse Brain After Severe Ischemia/Reperfusion. Stroke 2019, 50, 1548–1557. [Google Scholar] [CrossRef]
- Hansson, G.K.; Libby, P.; Schönbeck, U.; Yan, Z.Q. Innate and adaptive immunity in the pathogenesis of atherosclerosis. Circ. Res. 2002, 91, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Hilgendorf, I.; Swirski, F.K.; Robbins, C.S. Monocyte fate in atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Shantsila, E.; Caligiuri, G.; Guzik, T.; Heine, G.H.; Hoefer, I.E.; Monaco, C.; Peter, K.; Rainger, E.; Siegbahn, A.; Steffens, S.; et al. Role and analysis of monocyte subsets in cardiovascular disease. Joint consensus document of the European Society of Cardiology (ESC) Working Groups “Atherosclerosis & Vascular Biology” and “Thrombosis”. Thromb. Haemost. 2016, 116, 626–637. [Google Scholar] [CrossRef]
- Xue, J.; Huang, W.; Chen, X.; Li, Q.; Cai, Z.; Yu, T.; Shao, B. Neutrophil-to-Lymphocyte Ratio Is a Prognostic Marker in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 650–657. [Google Scholar] [CrossRef]
- Cagdas, M.; Karakoyun, S.; Yesin, M.; Rencuzogullari, I.; Karabag, Y.; Uluganyan, M.; Ozan Gursoy, M.; Artac, I.; Ilis, D.; Atalay, E.; et al. The association between monocyte HDL-C ratio and SYNTAX score and SYNTAX score II in STEMI patients treated with primary PCI. Acta Cardiol. Sin. 2018, 34, 23–30. [Google Scholar] [CrossRef]
- Assmann, G.; Gotto, A.M., Jr. HDL cholesterol and protective factors in atherosclerosis. Criculation 2004, 109, III-8–III-14. [Google Scholar] [CrossRef]
- Hafiane, A.; Genest, J. High density lipoproteins: Measurement techniques and potential biomarkers of cardiovascular risk. BBA Clin. 2015, 3, 175–188. [Google Scholar] [CrossRef]
- Kanbay, M.; Solak, Y.; Unal, H.U.; Kurt, Y.G.; Gok, M.; Cetinkaya, H.; Karaman, M.; Oguz, Y.; Eyileten, T.; Vural, A.; et al. Monocyte count/HDL cholesterol ratio and cardiovascular events in patients with chronic kidney disease. Int. Urol. Nephrol. 2014, 46, 1619–1625. [Google Scholar] [CrossRef]
- Chen, T.; Chen, H.; Xiao, H.; Tang, H.; Xiang, Z.; Wang, X.; Wang, X.; Zou, H. Comparison of the value of neutrophil to high-density lipoprotein cholesterol ratio and lymphocyte to high-density lipoprotein cholesterol ratio for predicting metabolic syndrome among a population in the southern coast of China. Diabetes, Metab. Syndr. Obes. 2020, 13, 597–605. [Google Scholar] [CrossRef]
- Sercelik, A.; Besnili, A.F. Increased monocyte to high-density lipoprotein cholesterol ratio is associated with TIMI risk score in patients with ST segment elevation myocardial infarction. Rev. Port. Cardiol. 2018, 37, 217–223. [Google Scholar] [CrossRef]
- Cetin, E.H.O.; Cetin, M.S.; Canpolat, U.; Aydin, S.; Topaloglu, S.; Aras, D.; Aydogdu, S. Monocyte/HDL-cholesterol ratio predicts the definite stent thrombosis after primary percutaneous coronary intervention for STsegment elevation myocardial infarction. Biomark. Med. 2015, 9, 967–977. [Google Scholar] [CrossRef]
- Chen, G.; Yang, N.; Ren, J.; He, Y.; Huang, H.; Hu, X.; Shen, J.; Yang, C.; Zeng, T.; Hu, J.; et al. Neutrophil Counts to High-Density Lipoprotein Cholesterol Ratio: A Potential Predictor of Prognosis in Acute Ischemic Stroke Patients after Intravenous Thrombolysis. Neurotox. Res. 2020, 38, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Sun, J.; Zou, H.; Li, M.; Su, Z.; Sun, W.; Kong, X. Prognostic Role of Neutrophil to High-Density Lipoprotein Cholesterol Ratio for All-Cause and Cardiovascular Mortality in the General Population. Front. Cardiovasc. Med. 2022, 9, 807339. [Google Scholar] [CrossRef] [PubMed]
- Bolayir, A.; Gokce, S.F.; Cigdem, B.; Bolayir, H.A.; Yildiz, O.K.; Bolayir, E.; Topaktas, S.A. Monocyte/high-density lipoprotein ratio predicts the mortality in ischemic stroke patients. Neurol. Neurochir. Polska 2018, 52, 150–155. [Google Scholar] [CrossRef]
- Liu, H.; Zhan, F.; Wang, Y. Evaluation of monocyte-to-high-density lipoprotein cholesterol ratio and monocyte-to-lymphocyte ratio in ischemic stroke. J. Int. Med Res. 2020, 48, 300060520933806. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Liu, K.; Pei, L.; Gao, Y.; Zhao, L.; Sun, S.; Wu, J.; Li, Y.; Fang, H.; Song, B.; et al. Monocyte-to-High-Density Lipoprotein Ratio Predicts the Outcome of Acute Ischemic Stroke. J. Atheroscler. Thromb. 2020, 27, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.Y.; Shi, W.R.; Yi, X.; Zhou, Y.P.; Wang, Z.Q.; Sun, Y.X. Assessing the performance of monocyte to high-density lipoprotein ratio for predicting ischemic stroke: Insights from a population-based Chinese cohort. Lipids Health Dis. 2019, 18, 127. [Google Scholar] [CrossRef]
- Oh, S.W.; Yi, H.J.; Lee, D.H.; Sung, J.H. Prognostic Significance of Various Inflammation-Based Scores in Patients with Mechanical Thrombectomy for Acute Ischemic Stroke. World Neurosurg. 2020, 141, e710–e717. [Google Scholar] [CrossRef]
- Bi, X.; Liu, X.; Cheng, J. Monocyte to High-Density Lipoprotein Ratio Is Associated With Early Neurological Deterioration in Acute Isolated Pontine Infarction. Front. Neurol. 2021, 12, 678884. [Google Scholar] [CrossRef]
- Sun, Y.; Lu, J.; Zheng, D.; Qian, J.; Zhang, H.; Xing, D.; Rong, F.; Cao, Y.; Liu, C.F.; You, S. Predictive value of monocyte to HDL cholesterol ratio for stroke-associated pneumonia in patients with acute ischemic stroke. Acta Neurol. Belg. 2021, 121, 1575–1581. [Google Scholar] [CrossRef]
- Li, X.; Wu, F.; Jiang, C.; Feng, X.; Wang, R.; Song, Z.; Zhang, J.; Hong, G. Novel peripheral blood cell ratios: Effective 3-month post-mechanical thrombectomy prognostic biomarkers for acute ischemic stroke patients. J. Clin. Neurosci. 2021, 89, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Chen, D.; Sun, L.; Chen, Z.; Quan, W. Monocyte/High-Density Lipoprotein Ratio Predicts the Prognosis of Large Artery Atherosclerosis Ischemic Stroke. Front. Neurol. 2021, 12, 769217. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Xu, T.; Zhan, Z.; Wu, Y.; Xu, Y.; Cao, Y.; Han, Z. High ratio of monocytes to high-density lipoprotein is associated with hemorrhagic transformation in acute ischemic stroke patients on intravenous thrombolysis. Front. Aging Neurosci. 2022, 14, 977332. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cheng, Y.; Song, Q.; Wei, C.; Liu, J.; Wu, B.; Liu, M. The association between monocyte to high-density lipoprotein ratio and hemorrhagic transformation in patients with acute ischemic stroke. Aging 2020, 12, 2498–2506. [Google Scholar] [CrossRef]
- Enciu, A.M.; Gherghiceanu, M.; Popescu, B.O. Triggers and effectors of oxidative stress at blood-brain barrier level: Relevance for brain ageing and neurodegeneration. Oxidat. Med. Cell. Longev. 2013, 2013, 297512. [Google Scholar] [CrossRef]
- Jin, R.; Yang, G.; Li, G. Inflammatory mechanisms in ischemic stroke: Role of inflammatory cells. J. Leukoc. Biol. 2010, 87, 779–789. [Google Scholar] [CrossRef]
- Jickling, G.C.; Liu, D.; Stamova, B.; Ander, B.P.; Zhan, X.; Lu, A.; Sharp, F.R. Hemorrhagic transformation after ischemic stroke in animals and humans. J. Cereb. Blood Flow Metab. 2014, 34, 185–199. [Google Scholar] [CrossRef]
- Park, T.H.; Lee, J.-K.; Park, M.-S.; Park, S.-S.; Hong, K.-S.; Ryu, W.-S.; Kim, D.-E.; Park, M.S.; Choi, K.-H.; Kim, J.-T.; et al. Neurologic deterioration in patients with acute ischemic stroke or transient ischemic attack. Neurology 2020, 95, e2178–e2191. [Google Scholar] [CrossRef]
- Saver, J.L.; Altman, H. Relationship between neurologic deficit severity and final functional outcome shifts and strengthens during first hours after onset. Stroke 2012, 43, 1537–1541. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- Banerjee, C.; Chimowitz, M.I. Stroke caused by atherosclerosis of the major intracranial arteries. Circ. Res. 2017, 120, 502–513. [Google Scholar] [CrossRef] [PubMed]
- Rexrode, K.M.; Madsen, T.E.; Yu, A.Y.; Carcel, C.; Lichtman, J.H.; Miller, E.C. The Impact of Sex and Gender on Stroke. Circ. Res. 2022, 130, 512–528. [Google Scholar] [CrossRef] [PubMed]
- Cuadrado-Godia, E.; Jiménez-Conde, J.; Ois, A.; Rodríguez-Campello, A.; García-Ramallo, E.; Roquer, J. Sex differences in the prognostic value of the lipid profile after the first ischemic stroke. J. Neurol. 2009, 256, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Sato, Y.; Falcone-Juengert, J.; Kurisu, K.; Shi, J.; Yenari, M.A. Sexual dimorphism in immune cell responses following stroke. Neurobiol. Dis. 2022, 172, 105836. [Google Scholar] [CrossRef]
- Banerjee, A.; McCullough, L.D. Sex-Specific Immune Responses in Stroke. Stroke 2022, 53, 1449–1459. [Google Scholar] [CrossRef]


{kind=link}
| Authors, Year of Publication | Biomarker | Type of Study | Type of Stroke | Number of Participants/ Mean Age | Time of Blood Sampling | Scale of Stroke Severity and Prognosis/Clinical Outcome | Cut-Off Values; (Specificity); [Sensitivity] | Main Results |
|---|---|---|---|---|---|---|---|---|
| 1. Chen et al., 2020 [43] | NHR | Retrospective | IS | 160 patients, 160 healthy controls/patients: 67.67 ± 12.08, healthy controls: 67.62 ± 10.38 | Within 24 h of admission | NIHSS, mRS | NHR > 5.66; (79.6%); [51.6%] | The NHR was strongly connected with neurological impairment and 3-month outcomes in AIS patients |
| 2. Jiang et al., 2022 [44] | NHR | Prospective | IS (as part of cardiovascular events in general) | 34,335/49.6 ± 18.2 | Not mentioned | None | Not mentioned | In the general population, NHR was independently correlated with cardiovascular and all-cause death |
| 3. Bolayir et al., 2017 [45] | MHR | Retrospective | IS | 466 IS patients, 408 controls/IS patients: 77.09 ± 6.7, controls: 77.35 ± 9.6 | Within 24 h of admission | None | MHR > 17.52; (84.8%); [94.4%] | In IS patients, a high MHR value at admission may be a reliable indicator of 30-day mortality |
| 4. Algin et al., 2019 [25] | MHR | Retrospective | IS | 75 patients/73.23 ± 11.49 | On admission | GCS, NIHSS | 0.191; (90%); [52.3%] | Short-term mortality was highly correlated with MHR |
| 5. Liu et al., 2020 [46] | MHR | Retrospective | IS | 253 patients, 211 healthy Subjects/Patients:67, healthy controls:66 years | Within 24 h of admission | NIHSS | 0.28 with an area under the curve: 0.777; (77.25%); [66.01%] | MHR is characterized as a distinct risk factor for the development of IS. Together, MHR and MLR showed increased sensitivity for the IS diagnosis |
| 6. Liu et al., 2020 [47] | MHR | Prospective | IS | 1090 patients/ Patients with good outcome: 59.32 ± 12.64, patients with poor outcome: 64.13 ± 12.21 | Within 24 h of admission | mRS | 0.51; (66.5%); [62.3%] | In AIS patients, MHR may be a substantial and independent indicator of poor functional prognosis |
| 7. Wang et al., 2020 [48] | MHR | Retrospective | IS | 974 patients/69 (IQR: 58–78) | Within 24 h of admission | NIHSS | Not mentioned | In individuals with IS, reduced MHR was independently linked to an increased risk of HT and symptomatic HT |
| 8. Oh et al., 2020 [49] | MHR and LMR | Retrospective | IS (patients with LAO treated with MT) | 411/68.6 | On admission, before MT | mRS, NIHSS | MHR cutoff: 1.4; N.A. | Higher MHR and NLR, and lower LMR values were detected after MT in patients who had a poor outcome. Scores based on inflammation, such as the MHR, NLR and LMR might be independent factors of patients’ clinical outcome and prognosis after MT |
| 9. Bi et al., 2021 [50] | MHR | Retrospective | IS | 212 patients/68.27 ± 11.57 | Within 24 h of admission | NIHSS | MHR cutoff 0.51; (76.6%); [65.5%] | As a biomarker of END in individuals with isolated pontine infarction, elevated MHR may be useful, and the higher MHR was independently linked to the END |
| 10. Sun et al., 2021 [51] | MHR | Retrospective | IS | 803 patients/69 ± 12.3 | Within 24 h of admission | NIHSS, mRS | Not mentioned | In patients with AIS, elevated MHR and MC on admission are both linked to SAP, but not to all-cause mortality at 3 months |
| 11. Li et al., 2021 [52] | MHR | Retrospective | IS | 316 patients/64.66 ± 12.24 | Within 24 h of admission | mRS | Not mentioned | They proposed that poor 3-month functional outcomes in LAA IS were dependently associated with greater MHR values |
| 12. Li et al., 2021 [53] | MHR | Retrospective | IS | 286 patients/70.00 (IQR: 63.00–77.00) | All blood tests were performed before MT | NIHSS, mRS | 0.368; (56.8%); [67.4%] | In patients with AIS who received MT, higher RPR, MHR, and NLR may be independent risk factors for predicting a poor outcome at three months |
| 13. Xia et al., 2022 [54] | MHR | Retrospective | IS | 340 patients/69.5 ± 13.5 | At 24 h after thrombolytic treatment | NIHSS | 0.46; (57.1%); [70.6%] | In patients with acute ischemic stroke receiving intravenous thrombolysis, elevated MHR may be independently linked to a greater risk of HT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkantzios, A.; Tsiptsios, D.; Karapepera, V.; Karatzetzou, S.; Kiamelidis, S.; Vlotinou, P.; Giannakou, E.; Karampina, E.; Paschalidou, K.; Kourkoutsakis, N.; et al. Monocyte to HDL and Neutrophil to HDL Ratios as Potential Ischemic Stroke Prognostic Biomarkers. Neurol. Int. 2023, 15, 301-317. https://doi.org/10.3390/neurolint15010019
Gkantzios A, Tsiptsios D, Karapepera V, Karatzetzou S, Kiamelidis S, Vlotinou P, Giannakou E, Karampina E, Paschalidou K, Kourkoutsakis N, et al. Monocyte to HDL and Neutrophil to HDL Ratios as Potential Ischemic Stroke Prognostic Biomarkers. Neurology International. 2023; 15(1):301-317. https://doi.org/10.3390/neurolint15010019
Chicago/Turabian StyleGkantzios, Aimilios, Dimitrios Tsiptsios, Vaia Karapepera, Stella Karatzetzou, Stratis Kiamelidis, Pinelopi Vlotinou, Erasmia Giannakou, Evangeli Karampina, Katerina Paschalidou, Nikolaos Kourkoutsakis, and et al. 2023. "Monocyte to HDL and Neutrophil to HDL Ratios as Potential Ischemic Stroke Prognostic Biomarkers" Neurology International 15, no. 1: 301-317. https://doi.org/10.3390/neurolint15010019
APA StyleGkantzios, A., Tsiptsios, D., Karapepera, V., Karatzetzou, S., Kiamelidis, S., Vlotinou, P., Giannakou, E., Karampina, E., Paschalidou, K., Kourkoutsakis, N., Papanas, N., Aggelousis, N., & Vadikolias, K. (2023). Monocyte to HDL and Neutrophil to HDL Ratios as Potential Ischemic Stroke Prognostic Biomarkers. Neurology International, 15(1), 301-317. https://doi.org/10.3390/neurolint15010019